2022 WUOF/SIU International Consultation on Urological Diseases: Ablative Therapies for Localized Primary Renal Cell Carcinoma

Abstract
:Introduction
Thermal Ablation
Indications and Patient Selection
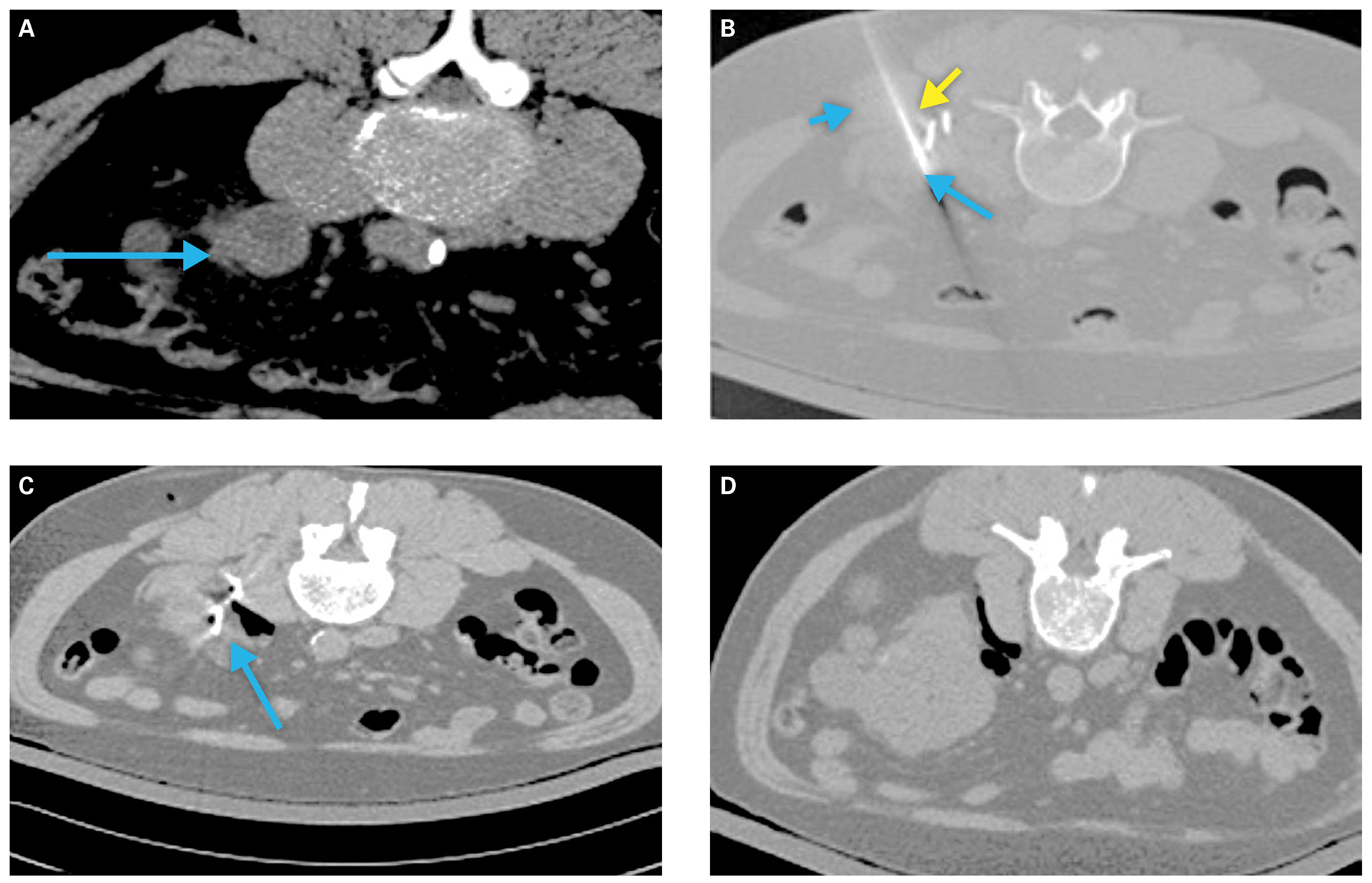
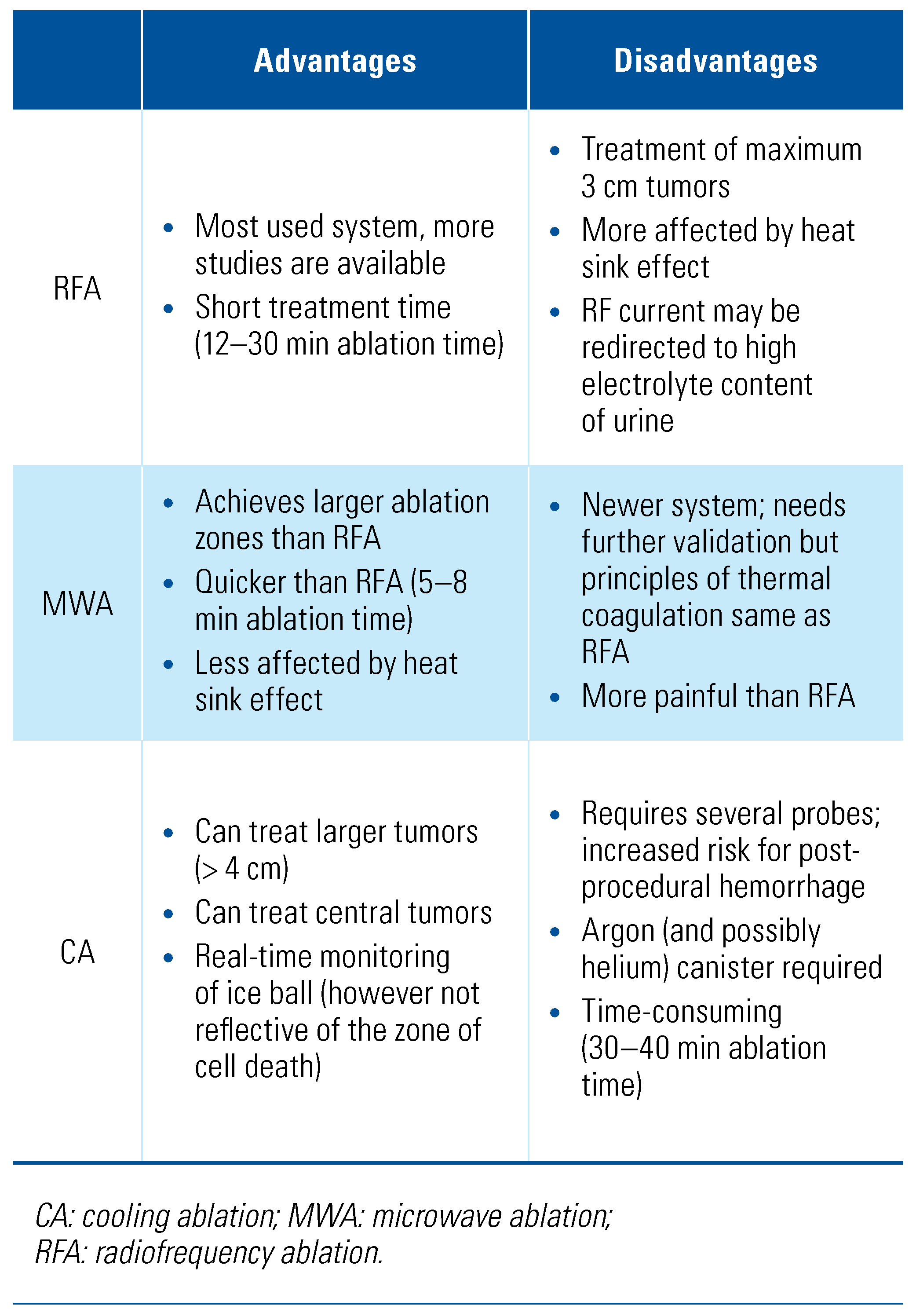
Technical Considerations
Preprocedural Planning
Peri- and Post-Procedural Complications
- Post-ablation syndrome: A transient and self-limiting constellation of symptoms experienced following TA characterized by fever, nausea, vomiting, and malaise. Larger volumes of necrosis may prolong symptoms. Fewer than 10% of patients experience the full spectrum of symptoms, while 60% report flu-like symptoms within the first 10 days following ablation[46].
- Hematuria: This is a rare side effect of TA (0.5–1%) that generally spontaneously resolves within 12 to 24 hours of treatment[43]. If hematuria persists, thermal damage to the pelvicalyceal system should be suspected. In the case of hydronephrosis due to clot obstruction, placement of a ureteric stent and/or manual irrigation of the bladder may be necessary.
- Ureteric/Collecting System Injury: This complication is associated with treatment of central tumors. Although rare (1%–3% of cases[43]), injury can result in ureteric strictures, urine leak, urinoma, or formation of a urinary fistula[40,43,47], which may present in a delayed fashion (weeks to months following treatment).
Evidence Synthesis
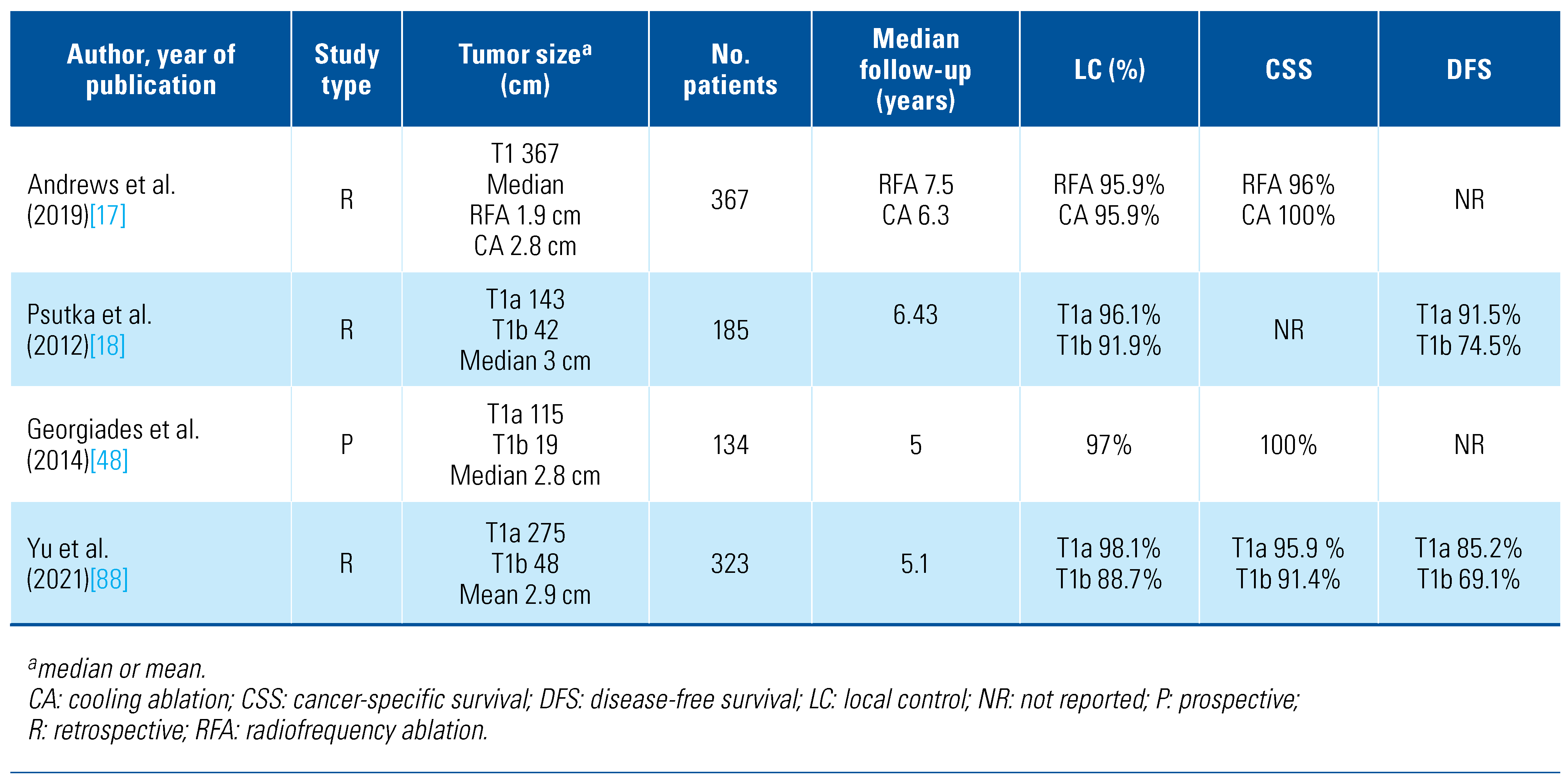
Local Tumor Control
Comparative Studies
Stereotactic Ablative Radiotherapy (SABR)
Patient Selection for SABR
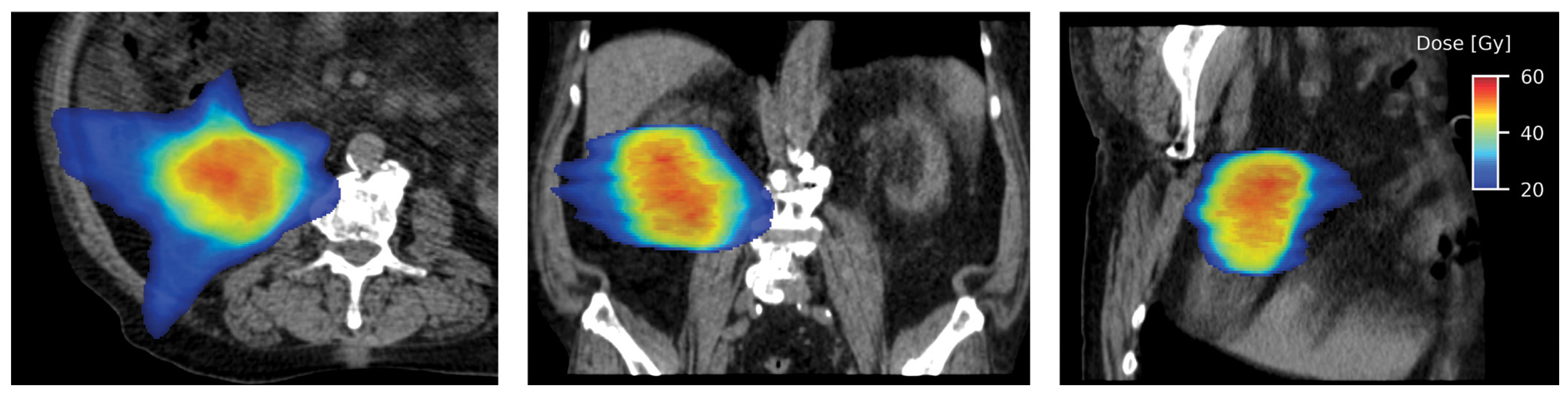
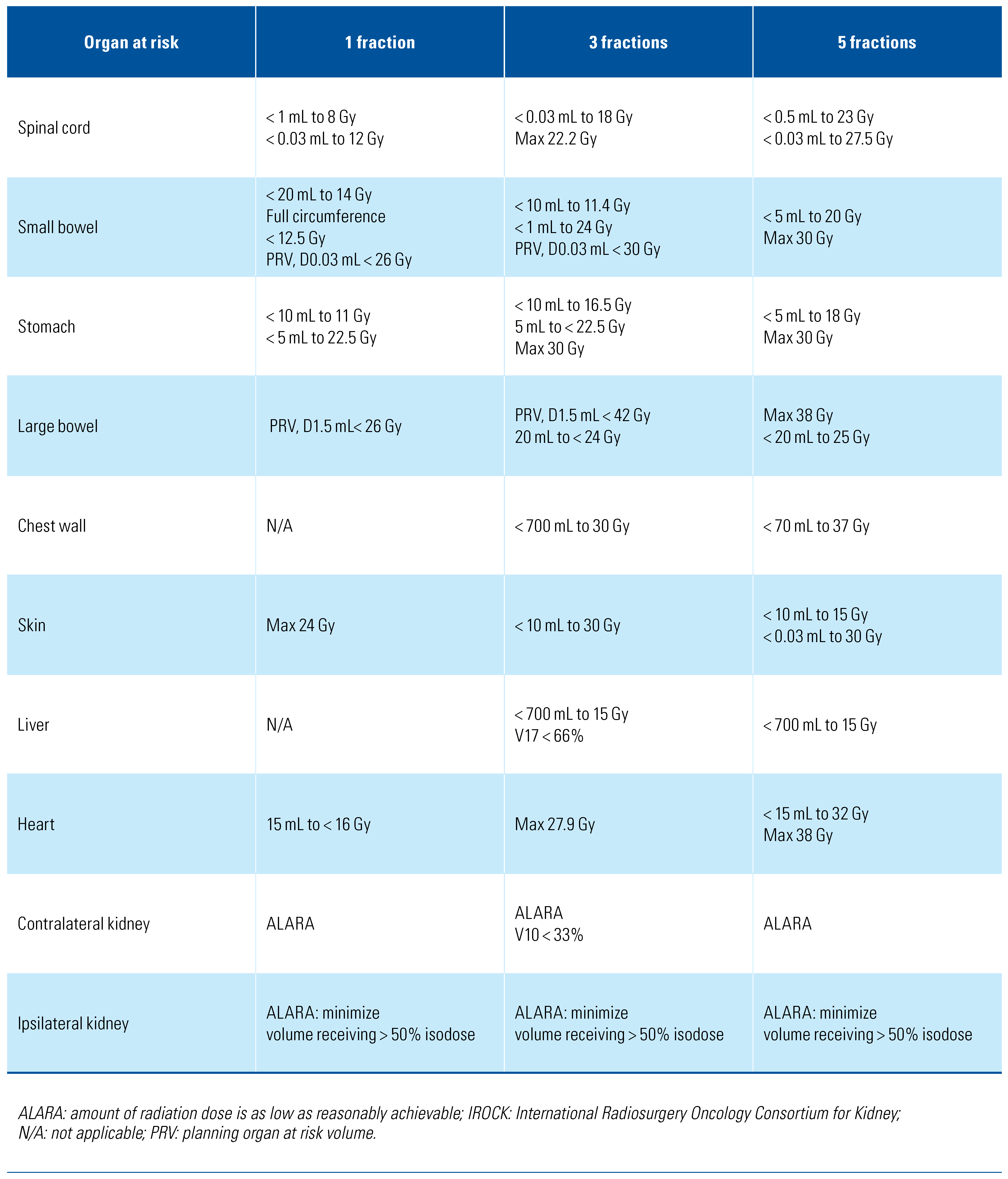
Technical Consideration
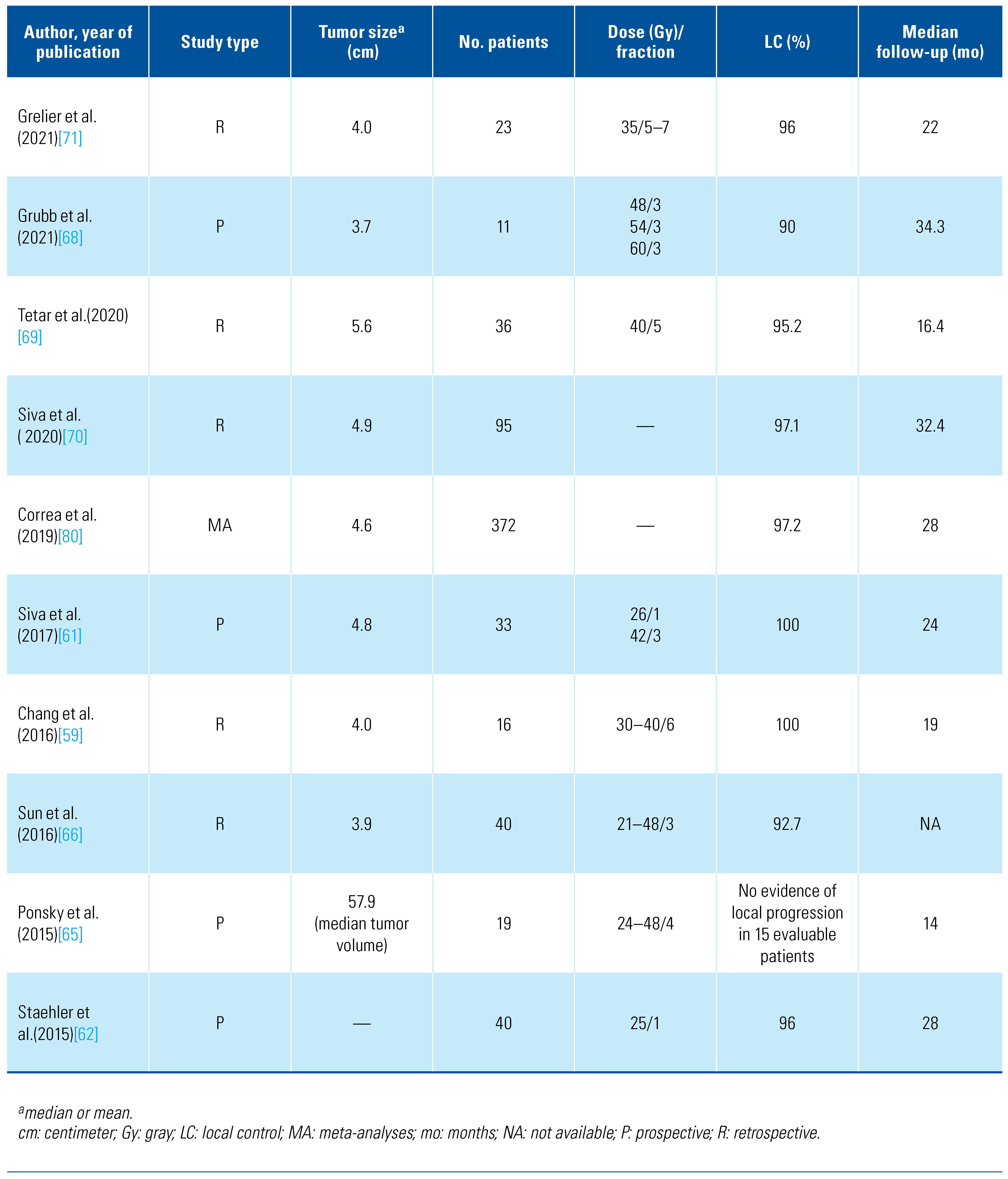
Clinical Evidence for SABR in Localized Primary RCC
Response Evaluation
Renal Function Post-SABR
Future Perspectives
Take-Home Messages
- Patients with a newly diagnosed, localized renal mass should undergo a detailed assessment, including history focusing on comorbidity burden, physical examination, renal function assessment, and appropriate comprehensive tumor staging imaging. In patients considering TA or SABR, renal mass biopsy is recommended to characterize the histology of the tumor.
- Each case should be discussed in a multidisciplinary team meeting consisting of a urologist, interventional radiologist, and radiation oncologist, including a central imaging review.
- Ablative treatments, including TA or SABR, can be considered in patients at high risk for adverse outcomes following surgery who decline surgery and in whom AS is not optimal. Local expertise should be considered for decision-making.
- SRMs less than 4 cm (ideally < 3 cm), predominantly exophytic and distant to the renal hilum, should be considered for TA preferentially to SABR.
- Tumors measuring more than 4 cm (ideally > 3 cm), predominantly endophytic and centrally located, could be considered preferentially for SABR over TA.
- Ongoing imaging at regular specified intervals is essential to monitor the treatment outcome.
Acknowledgments
Competing Interests
Abbreviations
| AS | active surveillance |
| CA | cooling ablation |
| CKD | chronic kidney disease |
| CSS | cancer-specific survival |
| CT | computed tomography |
| IROCK | International Radiosurgery Oncology Consortium for Kidney |
| MRI | magnetic resonance imaging |
| MWA | microwave ablation |
| PN | partial nephrectomy |
| RCC | renal cell carcinoma |
| RFA | radiofrequency ablation |
| RN | radical nephrectomy |
| SABR | stereotactic ablative radiotherapy |
| SMRs | small renal masses |
| TA | thermal ablation |
References
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2013. CA Cancer J. Clin. 2013, 63, 11–30. [Google Scholar] [CrossRef] [PubMed]
- Demirjian, S.; Lane, B.R.; Derweesh, I.H.; Takagi, T.; Fergany, A.; Campbell, S.C. Chronic kidney disease due to surgical removal of nephrons: Relative rates of progression and survival. J. Urol. 2014, 192, 1057–1062. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.P.; Thompson, R.H.; Boorjian, S.A.; Weight, C.J.; Han, L.C.; Murad, M.H.; et al. Comparative effectiveness for survival and renal function of partial and radical nephrectomy for localized renal tumors: A systematic review and meta-analysis. J. Urol. 2012, 188, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.C.; Uzzo, R.G.; Karam, J.A.; Chang, S.S.; Clark, P.E.; Souter, L. Renal mass and localized renal cancer: Evaluation, management, and follow-up: AUA Guideline: Part II. J. Urol. 2021, 206, 209–218. [Google Scholar] [CrossRef] [PubMed]
- European Assocation of Urology (EAU). Guidelines on Renal Cell Cacrcinoma. Available online: https://uroweb.org/guideline/renal-cellcarcinoma/#7 (accessed on 20 August 2022).
- Escudier, B.; Porta, C.; Schmidinger, M.; Rioux-Leclercq, N.; Bex, A.; Khoo, V.; et al. Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann. Oncol. 2019, 30, 706–720. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Kidney Cancer (Version 2. 2022). Available online: https://www.nccn.org/professionals/physician_gls/pdf/kidney.pdf (accessed on 20 August 2022).
- Ahmed, M.; Solbiati, L.; Brace, C.L.; Breen, D.J.; Callstrom, M.R.; Charboneau, J.W.; et al. Image-guided tumor ablation: Standardization of terminology and reporting criteria--a 10-year update. J. Vasc. Interv. Radiol. 2014, 25, 1691–1705. [Google Scholar] [CrossRef] [PubMed]
- Breen, D.J.; Railton, N.J. Minimally invasive treatment of small renal tumors: Trends in renal cancer diagnosis and management. Cardiovasc. Intervent Radiol. 2010, 33, 896–908. [Google Scholar] [CrossRef]
- Campbell, S.; Uzzo, R.G.; Allaf, M.E.; Bass, E.B.; Cadeddu, J.A.; Chang, A.; et al. Renal mass and localized renal cancer: AUA Guideline. J. Urol. 2017, 198, 520–529. [Google Scholar] [CrossRef] [PubMed]
- Finelli, A.; Ismaila, N.; Bro, B.; Durack, J.; Eggener, S.; Evans, A.; et al. Management of small renal masses: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2017, 35, 668–680. [Google Scholar] [CrossRef]
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bensalah, K.; Dabestani, S.; Fernández-Pello, S.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2019 update. Eur Urol. 2019, 75, 799–810. [Google Scholar] [CrossRef]
- Ginzburg, S.; Uzzo, R.; Walton, J.; Miller, C.; Kurz, D.; Li, T.; et al. Residual parenchymal volume, not warm ischemia time, predicts ultimate renal functional outcomes in patients undergoing partial nephrectomy. Urology 2015, 86, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Song, C.; Bang, J.K.; Park, H.K.; Ahn, H. Factors influencing renal function reduction after partial nephrectomy. J. Urol. 2009, 181, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Katsanos, K.; Mailli, L.; Krokidis, M.; McGrath, A.; Sabharwal, T.; Adam, A. Systematic review and meta-analysis of thermal ablation versus surgical nephrectomy for small renal tumours. Cardiovasc. Intervent Radiol. 2014, 37, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Acosta Ruiz, V.; Batelsson, S.; Onkamo, E.; Wernroth, L.; Nilsson, T.; Lonnemark, M.; et al. Split renal function after treatment of small renal masses: Comparison between radiofrequency ablation and laparoscopic partial nephrectomy. Acta Radiol. 2020, 284185120956281. [Google Scholar] [CrossRef] [PubMed]
- Andrews, J.R.; Atwell, T.; Schmit, G.; Lohse, C.M.; Kurup, A.N.; Weisbrod, A.; et al. Oncologic outcomes following partial nephrectomy and percutaneous ablation for cT1 renal masses. Eur. Urol. 2019, 76, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Psutka, S.P.; Feldman, A.S.; McDougal, W.S.; McGovern, F.J.; Mueller, P.; Gervais, D.A. Long-term oncologic outcomes after radiofrequency ablation for T1 renal cell carcinoma. Eur. Urol. 2013, 63, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Gervais, D.A.; McGovern, F.J.; Arellano, R.S.; McDougal, W.S.; Mueller, P.R. Radiofrequency ablation of renal cell carcinoma: Part 1, Indications, results, and role in patient management over a 6-year period and ablation of 100 tumors. AJR Am. J. Roentgenol. 2005, 185, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Wah, T.M.; Irving, H.C.; Gregory, W.; Cartledge, J.; Joyce, A.D.; Selby, P.J. Radiofrequency ablation (RFA) of renal cell carcinoma (RCC): Experience in 200 tumours. BJU Int. 2014, 113, 416–428. [Google Scholar] [CrossRef]
- Aarts, B.M.; Prevoo, W.; Meier, M.A.J.; Bex, A.; Beets-Tan, R.G.H.; Klompenhouwer, E.G.; et al. Percutaneous microwave ablation of histologically proven T1 renal cell carcinoma. Cardiovasc. Intervent Radiol. 2020, 43, 1025–1033. [Google Scholar] [CrossRef]
- Zagoria, R.J.; Traver, M.A.; Werle, D.M.; Perini, M.; Hayasaka, S.; Clark, P.E. Oncologic efficacy of CT-guided percutaneous radiofrequency ablation of renal cell carcinomas. AJR Am. J. Roentgenol. 2007, 189, 429–436. [Google Scholar] [CrossRef]
- Yu, J.; Wang, H.; Cheng, Z.G.; Liu, F.Y.; Li, Q.Y.; He, G.Z.; et al. A multicenter 10-year oncologic outcome of ultrasound-guided percutaneous microwave ablation of clinical T1 renal cell carcinoma: Will it stand the test of time? Eur. Radiol. 2022, 32, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Atwell, T.D.; Vlaminck, J.J.; Boorjian, S.A.; Kurup, A.N.; Callstrom, M.R.; Weisbrod, A.J.; et al. Percutaneous cryoablation of stage T1b renal cell carcinoma: Technique considerations, safety, and local tumor control. J. Vasc. Interv. Radiol. 2015, 26, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wu, X.; Zhou, J.; Zhang, J.; Huang, J.; Huang, Y.; et al. Thermal ablation assisted laparoscopic partial nephrectomy for clinical T1b renal tumors. Minim. Invasive Ther. Allied Technol. 2022, 31, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Atwell, T.D.; Farrell, M.A.; Leibovich, B.C.; Callstrom, M.R.; Chow, G.K.; Blute, M.L.; et al. Percutaneous renal cryoablation: Experience treating 115 tumors. J. Urol. 2008, 179, 2136–2140. [Google Scholar] [CrossRef] [PubMed]
- Breen, D.J.; Bryant, T.J.; Abbas, A.; Shepherd, B.; McGill, N.; Anderson, J.A.; et al. Percutaneous cryoablation of renal tumours: Outcomes from 171 tumours in 147 patients. BJU Int. 2013, 112, 758–765. [Google Scholar] [CrossRef] [PubMed]
- Acosta Ruiz, V.; Lonnemark, M.; Brekkan, E.; Dahlman, P.; Wernroth, L.; Magnusson, A. Predictive factors for complete renal tumor ablation using RFA. Acta Radiol. 2016, 57, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Hinshaw, J.L.; Lubner, M.G.; Ziemlewicz, T.J.; Fred, T.; Lee, J.; Brace, CL. Percutaneous tumor ablation tools: Microwave, radiofrequency, or cryoablation–what should you use and why? RadioGraphics. 2014, 34, 1344–1362. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, M.D.; Kim, C.Y.; Tsivian, M.; Suberlak, M.N.; Sopko, D.R.; Polascik, T.J.; et al. Percutaneous cryoablation of renal lesions with radiographic ice ball involvement of the renal sinus: Analysis of hemorrhagic and collecting system complications. AJR Am. J. Roentgenol. 2011, 196, 935–939. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.B.; Saboorian, M.H.; Duchene, D.A.; Ogan, K.; Cadeddu, J.A. Nephrectomy after radiofrequency ablation-induced ureteropelvic junction obstruction: Potential complication and long-term assessment of ablation adequacy. Urology 2003, 62, 351–352. [Google Scholar] [CrossRef]
- Johnson, D.B.; Solomon, S.B.; Su, L.M.; Matsumoto, E.D.; Kavoussi, L.R.; Nakada, S.Y.; et al. Defining the complications of cryoablation and radio frequency ablation of small renal tumors: A multi-institutional review. J. Urol. 2004, 172, 874–877. [Google Scholar] [CrossRef]
- Warlick, C.A.; Lima, G.C.; Allaf, M.E.; Varkarakis, I.; Permpongkosol, S.; Schaeffer, E.M.; et al. Clinical sequelae of radiographic iceball involvement of collecting system during computed tomography-guided percutaneous renal tumor cryoablation. Urology 2006, 67, 918–922. [Google Scholar] [CrossRef] [PubMed]
- Schmit, G.D.; Kurup, A.N.; Weisbrod, A.J.; Thompson, R.H.; Boorjian, S.A.; Wass, C.T.; et al. ABLATE: A renal ablation planning algorithm. AJR Am. J. Roentgenol. 2014, 202, 894–903. [Google Scholar] [CrossRef] [PubMed]
- Tsivian, M.; Lyne, J.C.; Mayes, J.M.; Mouraviev, V.; Kimura, M.; Polascik, T.J. Tumor size and endophytic growth pattern affect recurrence rates after laparoscopic renal cryoablation. Urology 2010, 75, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Kutikov, A.; Uzzo, R.G. The R. E. N. A. L. nephrometry score: A comprehensive standardized system for quantitating renal tumor size, location and depth. J. Urol. 2009, 182, 844–853. [Google Scholar] [CrossRef] [PubMed]
- Gahan, J.C.; Richter, M.D.; Seideman, C.A.; Trimmer, C.; Chan, D.; Weaver, M.; et al. The Performance of a modified RENAL nephrometry score in predicting renal mass radiofrequency ablation success. Urology 2015, 85, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Higgins, L.J.; Hong, K. Renal Ablation Techniques: State of the Art. AJR Am. J. Roentgenol. 2015, 205, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Finley, D.S.; Beck, S.; Box, G.; Chu, W.; Deane, L.; Vajgrt, D.J.; et al. Percutaneous and laparoscopic cryoablation of small renal masses. J. Urol. 2008, 180, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Hui, G.C.; Tuncali, K.; Tatli, S.; Morrison, P.R.; Silverman, S.G. Comparison of percutaneous and surgical approaches to renal tumor ablation: Metaanalysis of effectiveness and complication rates. J. Vasc. Interv. Radiol. 2008, 19, 1311–1320. [Google Scholar] [CrossRef]
- Acosta Ruiz, V.; Ladjevardi, S.; Brekkan, E.; Haggman, M.; Lonnemark, M.; Wernroth, L.; et al. Periprocedural outcome after laparoscopic partial nephrectomy versus radiofrequency ablation for T1 renal tumors: A modified R. E. N. A. L nephrometry score adjusted comparison. Acta Radiol. 2019, 60, 260–268. [Google Scholar] [CrossRef]
- Ahmed, M.; Solbiati, L.; Brace, C.L.; Breen, D.J.; Callstrom, M.R.; Charboneau, J.W.; et al. Image-guided tumor ablation: Standardization of terminology and reporting criteria-a 10-year update. J. Vasc. Interv. Radiol. 2014, 25, 1691–1705. [Google Scholar] [CrossRef]
- Krokidis, M.E.; Orsi, F.; Katsanos, K.; Helmberger, T.; Adam, A. CIRSE guidelines on percutaneous ablation of small renal cell carcinoma. Cardiovasc. Intervent Radiol. 2017, 40, 177–191. [Google Scholar] [CrossRef]
- Andersson, M.; Hashimi, F.; Lyrdal, D.; Lundstam, S.; Hellstrom, M. Improved outcome with combined US/CT guidance as compared to US guidance in percutaneous radiofrequency ablation of small renal masses. Acta Radiol. 2015, 56, 1519–1526. [Google Scholar] [CrossRef]
- Dai, Y.; Covarrubias, D.; Uppot, R.; Arellano, R.S. Image-guided percutaneous radiofrequency ablation of central renal cell carcinoma: Assessment of clinical efficacy and safety in 31 tumors. J. Vasc. Interv. Radiol. 2017, 28, 1643–1650. [Google Scholar] [CrossRef] [PubMed]
- Zhong, J.; Bambrook, J.; Bhambra, B.; Smith, J.; Cartledge, J.; Ralph, C.; et al. Incidence of post-ablation syndrome following image-guided percutaneous cryoablation of renal cell carcinoma: A prospective study. Cardiovasc. Interv. Radiol. 2018, 41, 270–276. [Google Scholar] [CrossRef]
- Atwell, T.D.; Carter, R.E.; Schmit, G.D.; Carr, C.M.; Boorjian, S.A.; Curry, T.B.; et al. Complications following 573 percutaneous renal radiofrequency and cryoablation procedures. J. Vasc. Interv. Radiol. 2012, 23, 48–54. [Google Scholar] [CrossRef]
- Georgiades, C.S.; Rodriguez, R. Efficacy and safety of percutaneous cryoablation for stage 1A/B renal cell carcinoma: Results of a prospective, single-arm, 5-year study. Cardiovasc. Intervent Radiol. 2014, 37, 1494–1499. [Google Scholar] [CrossRef]
- Crawford, D.; vanSonnenberg, E.; Kang, P. Infectious outcomes from renal tumor ablation: Prophylactic antibiotics or not? Cardiovasc. Intervent Radiol. 2018, 41, 1573–1578. [Google Scholar] [CrossRef] [PubMed]
- Pierorazio, P.M.; Johnson, M.H.; Patel, H.D.; Sozio, S.M.; Sharma, R.; Iyoha, E.; et al. Management of renal masses and localized renal cancer: Systematic review and meta-analysis. J. Urol. 2016, 196, 989–999. [Google Scholar] [CrossRef] [PubMed]
- Castle, S.M.; Gorbatiy, V.; Avallone, M.A.; Eldefrawy, A.; Caulton, D.E.; Leveillee, R.J. Cost comparison of nephron-sparing treatments for cT1a renal masses. Urol. Oncol. Semin. Orig. Investig. 2013, 31, 1327–1332. [Google Scholar] [CrossRef]
- Larcher, A.; Sun, M.; Dell’Oglio, P.; Trudeau, V.; Boehm, K.; Schiffmann, J.; et al. Mortality, morbidity and healthcare expenditures after local tumour ablation or partial nephrectomy for T1A kidney cancer. Eur. J. Surg. Oncol. 2017, 43, 815–822. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, Y.W.; Leow, J.J.; Levy, A.C.; Chang, S.L.; Gelpi, F.H. Cost-effectiveness of management options for small renal mass: A systematic review. Am. J. Clin. Oncol. 2016, 39, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Pandharipande, P.V.; Gervais, D.A.; Mueller, P.R.; Hur, C.; Gazelle, G.S. Radiofrequency ablation versus nephron-sparing surgery for small unilateral renal cell carcinoma: Cost-effectiveness analysis. Radiology 2008, 248, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Ning, S.; Trisler, K.; Wessels, B.W.; Knox, S.J. Radiobiologic studies of radioimmunotherapy and external beam radiotherapy in vitro and in vivo in human renal cell carcinoma xenografts. Cancer 1997, 80 (Suppl. 12), 2519–2528. [Google Scholar] [CrossRef]
- Walsh, L.; Stanfield, J.L.; Cho, L.C.; Chang, C.H.; Forster, K.; Kabbani, W.; et al. Efficacy of ablative high-dose-per-fraction radiation for implanted human renal cell cancer in a nude mouse model. Eur. Urol. 2006, 50, 795–800. [Google Scholar] [CrossRef] [PubMed]
- Kothari, G.; Foroudi, F.; Gill, S.; Corcoran, N.M.; Siva, S. Outcomes of stereotactic radiotherapy for cranial and extracranial metastatic renal cell carcinoma: A systematic review. Acta Oncol. 2015, 54, 148–157. [Google Scholar] [CrossRef] [PubMed]
- Svedman, C.; Karlsson, K.; Rutkowska, E.; Sandström, P.; Blomgren, H.; Lax, I.; et al. Stereotactic body radiotherapy of primary and metastatic renal lesions for patients with only one functioning kidney. Acta Oncol. 2008, 47, 1578–1583. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.H.; Cheung, P.; Erler, D.; Sonier, M.; Korol, R.; Chu, W. Stereotactic ablative body radiotherapy for primary renal cell carcinoma in non-surgical candidates: Initial clinical experience. Clin. Oncol. (R Coll Radiol.) 2016, 28, e109–e114. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.H.; Huang, W.Y.; Chao, H.L.; Lin, K.T.; Jen, Y.M. Novel application of stereotactic ablative radiotherapy using CyberKnife® for early-stage renal cell carcinoma in patients with pre-existing chronic kidney disease: Initial clinical experiences. Oncol. Lett. 2014, 8, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Siva, S.; Pham, D.; Kron, T.; Bressel, M.; Lam, J.; Tan, T.H.; et al. Stereotactic ablative body radiotherapy for inoperable primary kidney cancer: A prospective clinical trial. BJU Int. 2017, 120, 623–630. [Google Scholar] [CrossRef]
- Staehler, M.; Bader, M.; Schlenker, B.; Casuscelli, J.; Karl, A.; Roosen, A.; et al. Single fraction radiosurgery for the treatment of renal tumors. J. Urol. 2015, 193, 771–775. [Google Scholar] [CrossRef]
- Svedman, C.; Sandström, P.; Pisa, P.; Blomgren, H.; Lax, I.; Kälkner, K.M.; et al. A prospective phase II trial of using extracranial stereotactic radiotherapy in primary and metastatic renal cell carcinoma. Acta Oncol. 2006, 45, 870–875. [Google Scholar] [CrossRef] [PubMed]
- Pham, D.; Thompson, A.; Kron, T.; Foroudi, F.; Kolsky, M.S.; Devereux, T.; et al. Stereotactic ablative body radiation therapy for primary kidney cancer: A 3-dimensional conformal technique associated with low rates of early toxicity. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 1061–1068. [Google Scholar] [CrossRef] [PubMed]
- Ponsky, L.; Lo, S.S.; Zhang, Y.; Schluchter, M.; Liu, Y.; Patel, R.; et al. Phase I dose-escalation study of stereotactic body radiotherapy (SBRT) for poor surgical candidates with localized renal cell carcinoma. Radiother. Oncol. 2015, 117, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.R.; Brook, A.; Powell, M.F.; Kaliannan, K.; Wagner, A.A.; Kaplan, I.D.; et al. Effect of Stereotactic Body Radiotherapy on the Growth Kinetics and Enhancement Pattern of Primary Renal Tumors. AJR Am. J. Roentgenol. 2016, 206, 544–553. [Google Scholar] [CrossRef] [PubMed]
- Kaidar-Person, O.; Price, A.; Schreiber, E.; Zagar, T.M.; Chen, R.C. Stereotactic body radiotherapy for large primary renal cell carcinoma. Clin. Genitourin. Cancer. 2017, 15, e851–e854. [Google Scholar] [CrossRef] [PubMed]
- Grubb, W.R.; Ponsky, L.; Lo, S.S.; Kharouta, M.; Traughber, B.; Sandstrom, K.; et al. Final results of a dose escalation protocol of stereotactic body radiotherapy for poor surgical candidates with localized renal cell carcinoma. Radiother. Oncol. 2021, 155, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Tetar, S.U.; Bohoudi, O.; Senan, S.; Palacios, M.A.; Oei, S.S.; Wel, A.M.V.; et al. The role of daily adaptive stereotactic mr-guided radiotherapy for renal cell cancer. Cancers 2020, 12, 2763. [Google Scholar] [CrossRef] [PubMed]
- Siva, S.; Correa, R.J.M.; Warner, A.; Staehler, M.; Ellis, R.J.; Ponsky, L.; et al. Stereotactic ablative radiotherapy for ≥t1b primary renal cell carcinoma: A report from the International Radiosurgery Oncology Consortium for Kidney (IROCK). Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Grelier, L.; Baboudjian, M.; Gondran-Tellier, B.; Couderc, A.L.; McManus, R.; Deville, J.L.; et al. Stereotactic Body radiotherapy for frail patients with primary renal cell carcinoma: Preliminary results after 4 years of experience. Cancers 2021, 13, 3129. [Google Scholar] [CrossRef] [PubMed]
- Senger, C.; Conti, A.; Kluge, A.; Pasemann, D.; Kufeld, M.; Acker, G.; et al. Robotic stereotactic ablative radiotherapy for renal cell carcinoma in patients with impaired renal function. BMC Urol. 2019, 19, 96. [Google Scholar] [CrossRef]
- Nomiya, T.; Tsuji, H.; Hirasawa, N.; Kato, H.; Kamada, T.; Mizoe, J.; et al. Carbon ion radiation therapy for primary renal cell carcinoma: Initial clinical experience. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 828–833. [Google Scholar] [CrossRef]
- Swaminath, A.; Cheung, P.; Glicksman, R.M.; Donovan, E.K.; Niglas, M.; Vesprini, D.; et al. Patient-reported quality of life following stereotactic body radiation therapy for primary kidney cancer—Results from a prospective cohort study. Clin. Oncol. (R Coll Radiol.) 2021, 33, 468–475. [Google Scholar] [CrossRef]
- Correa, R.J.M.; Louie, A.V.; Staehler, M.; Warner, A.; Gandhidasan, S.; Ponsky, L.; et al. Stereotactic radiotherapy as a treatment option for renal tumors in the solitary kidney: A multicenter analysis from the IROCK. J. Urol. 2019, 201, 1097–1104. [Google Scholar] [CrossRef] [PubMed]
- Siva, S.; Pham, D.; Gill, S.; Bressel, M.; Dang, K.; Devereux, T.; et al. An analysis of respiratory induced kidney motion on four-dimensional computed tomography and its implications for stereotactic kidney radiotherapy. Radiat. Oncol. 2013, 8, 248. [Google Scholar] [CrossRef]
- Wilke, L.; Andratschke, N.; Blanck, O.; Brunner, T.B.; Combs, S.E.; Grosu, A.L.; et al. ICRU report 91 on prescribing, recording, and reporting of stereotactic treatments with small photon beams : Statement from the DEGRO/DGMP working group stereotactic radiotherapy and radiosurgery. Strahlenther. Onkol. 2019, 195, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Siva, S.; Ellis, R.J.; Ponsky, L.; Teh, B.S.; Mahadevan, A.; Muacevic, A.; et al. Consensus statement from the International Radiosurgery Oncology Consortium for Kidney for primary renal cell carcinoma. Future Oncol. 2016, 12, 637–645. [Google Scholar] [CrossRef]
- Siva, S.; Louie, A.V.; Warner, A.; Muacevic, A.; Gandhidasan, S.; Ponsky, L.; et al. Pooled analysis of stereotactic ablative radiotherapy for primary renal cell carcinoma: A report from the International Radiosurgery Oncology Consortium for Kidney (IROCK). Cancer. 2018, 124, 934–942. [Google Scholar] [CrossRef]
- Correa, R.J.M.; Louie, A.V.; Zaorsky, N.G.; Lehrer, E.J.; Ellis, R.; Ponsky, L.; et al. The emerging role of stereotactic ablative radiotherapy for primary renal cell carcinoma: A systematic review and meta-analysis. Eur. Urol. Focus. 2019, 5, 958–969. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, I.; Redrosa, I.; Martin, C.; Collins, C.; Wagner, A. Results of a phase I dose escalation study of stereotactic radiosurgery for primary renal tumors. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, S191. [Google Scholar] [CrossRef]
- McBride, S.; Wagner, A.; Kaplan, I. A phase 1 dose-escalation study of robotic radiosurgery in inoperable primary renal cell carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, S84. [Google Scholar] [CrossRef]
- Siva, S.; Chesson, B.; Bressel, M.; Pryor, D.; Higgs, B.; Reynolds, H.M.; et al. TROG 15. 03 phase II clinical trial of Focal Ablative STereotactic Radiosurgery for Cancers of the Kidney-FASTRACK II. BMC Cancer 2018, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, H.M.; Parameswaran, B.K.; Finnegan, M.E.; Roettger, D.; Lau, E.; Kron, T.; et al. Diffusion weighted and dynamic contrast enhanced MRI as an imaging biomarker for stereotactic ablative body radiotherapy (SABR) of primary renal cell carcinoma. PLoS ONE 2018, 13, e0202387. [Google Scholar] [CrossRef] [PubMed]
- Blitzer, G.C.; Wojcieszynski, A.; Abel, E.J.; Best, S.; Lee, F.T., Jr.; Hinshaw, J.L.; et al. Combining stereotactic body radiotherapy and microwave ablation appears safe and feasible for renal cell carcinoma in an early series. Clin. Genitourin. Cancer 2021, 19, e313–e318. [Google Scholar] [CrossRef] [PubMed]
- Chow, J.; Hoffend, N.C.; Abrams, S.I.; Schwaab, T.; Singh, A.K.; Muhitch, J.B. Radiation induces dynamic changes to the T cell repertoire in renal cell carcinoma patients. Proc. Natl. Acad. Sci. USA 2020, 117, 23721–23729. [Google Scholar] [CrossRef]
- Chu, K.F.; Dupuy, D.E. Thermal ablation of tumours: Biological mechanisms and advances in therapy. Nat. Rev. Cancer. 2014, 14, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Wang, H.; Cheng, Z.G.; Liu, F.Y.; Li, Q.Y.; He, G.Z.; et al. A multicenter 10-year oncologic outcome of ultrasound-guided percutaneous microwave ablation of clinical T1 renal cell carcinoma: Will it stand the test of time? Eur. Radiol. 2021. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
This is an open access article under the terms of a license that permits non-commercial use, provided the original work is properly cited. © 2022 The Authors. Société Internationale d'Urologie Journal, published by the Société Internationale d'Urologie, Canada.
Share and Cite
Ali, M.; Ruiz, V.A.; Psutka, S.P.; Liu, D.; Siva, S. 2022 WUOF/SIU International Consultation on Urological Diseases: Ablative Therapies for Localized Primary Renal Cell Carcinoma. Soc. Int. Urol. J. 2022, 3, 437-449. https://doi.org/10.48083/UEML5802
Ali M, Ruiz VA, Psutka SP, Liu D, Siva S. 2022 WUOF/SIU International Consultation on Urological Diseases: Ablative Therapies for Localized Primary Renal Cell Carcinoma. Société Internationale d’Urologie Journal. 2022; 3(6):437-449. https://doi.org/10.48083/UEML5802
Chicago/Turabian StyleAli, Muhammad, Vanessa Acosta Ruiz, Sarah P. Psutka, David Liu, and Shankar Siva. 2022. "2022 WUOF/SIU International Consultation on Urological Diseases: Ablative Therapies for Localized Primary Renal Cell Carcinoma" Société Internationale d’Urologie Journal 3, no. 6: 437-449. https://doi.org/10.48083/UEML5802
APA StyleAli, M., Ruiz, V. A., Psutka, S. P., Liu, D., & Siva, S. (2022). 2022 WUOF/SIU International Consultation on Urological Diseases: Ablative Therapies for Localized Primary Renal Cell Carcinoma. Société Internationale d’Urologie Journal, 3(6), 437-449. https://doi.org/10.48083/UEML5802