Abstract
Patients undergoing definitive surgery or ablative techniques for nonmetastatic kidney cancer have varying degrees of risk of recurrent disease post procedure. The ultimate goal of “adjuvant therapy” is to reduce the incidence of recurrent disease, and to cure more patients. We summarize the current state of perioperative therapy for kidney cancer and explore future directions to develop optimal adjuvant strategies. We define risk and risk of recurrence post-definitive therapy, describe the controversies surrounding the trial landscape of adjuvant vascular endothelial growth factor receptor tyrosine kinase inhibitors and immune checkpoint inhibitors. We review data on neoadjuvant therapy before advanced kidney cancer resection. Radiologic, ethnic, economic, and geographic considerations with respect to adjuvant therapy are highlighted, as well as adjuvant therapy issues especially pertinent to patients, future directions in adjuvant trial design specifically targeted to biomarkers and patient selection, and sequencing of treatment after adjuvant therapy in those patients with recurrence.
Introduction
Patients undergoing definitive surgery or ablative techniques for nonmetastatic kidney cancer have varying degrees of risk for recurrent disease post-procedure. The ultimate goal of “adjuvant therapy” is to reduce the incidence of recurrent disease, and to cure more patients.
This review summarizes the current state of perioperative therapy for kidney cancer and explores future directions to develop optimal adjuvant strategies. We define risk and risk for recurrence post-definitive therapy and describe the adjuvant trials landscape of adjuvant vascular endothelial growth factor receptor tyrosine kinase inhibitor (VEGFRTKI) trials and immune checkpoint inhibitor (IO) trials. We review data on neoadjuvant therapy before advanced kidney cancer resection. Radiologic, ethnic, economic, and geographic considerations with regard to adjuvant therapy are highlighted. Also covered are adjuvant therapy issues especially pertinent to patients, future directions in adjuvant trial design specifically targeted to biomarkers and patient selection, and sequencing of treatment after adjuvant therapy in those patients with recurrence.
Defining Risk
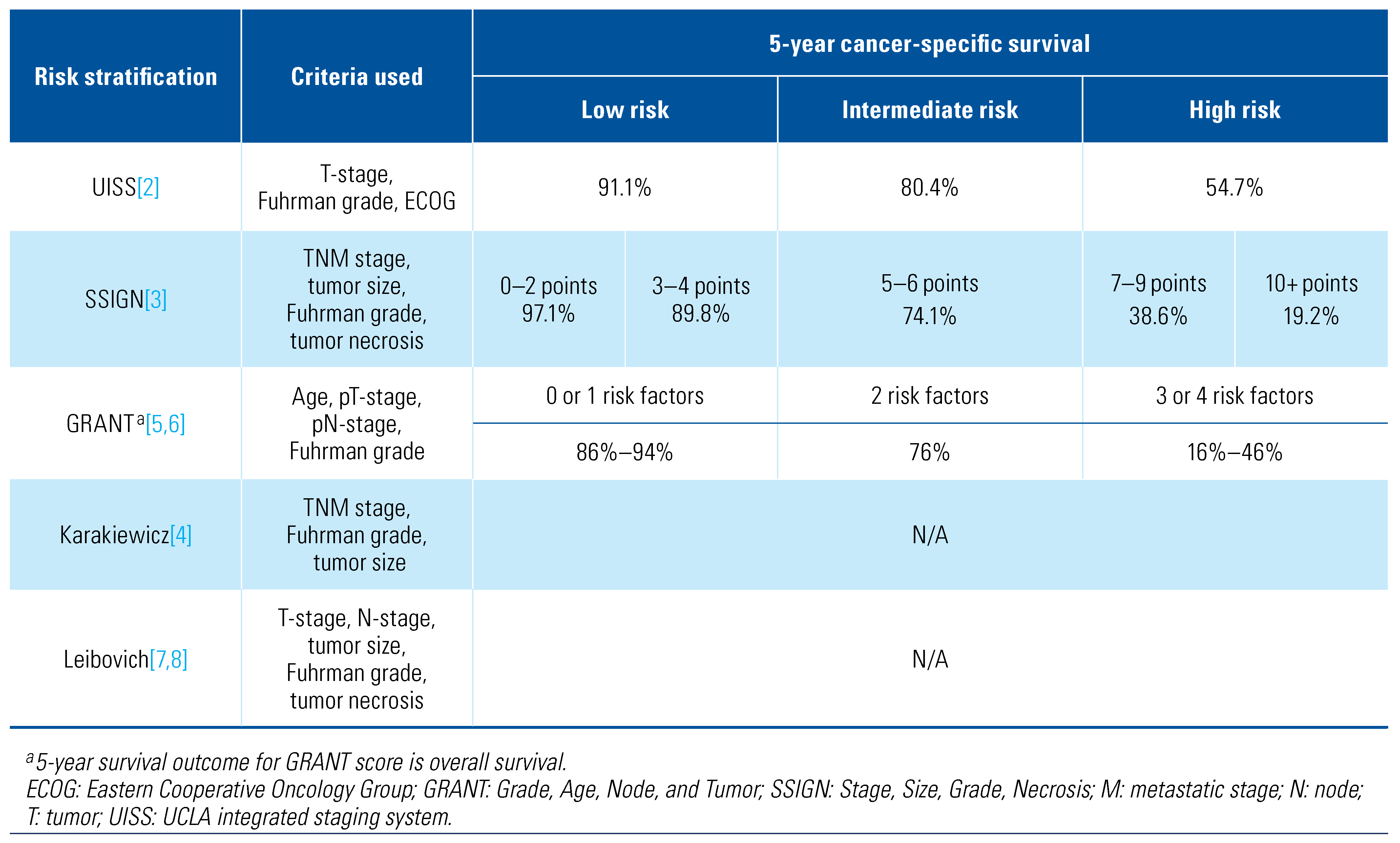
Risk for disease recurrence post-nephrectomy for renal cell cancer depends largely on the characteristics of the primary tumor. This risk can mainly be stratified based on stage and grade of the cancer. Patients with larger tumors and higher grade are at increased risk for recurrence after nephrectomy. Risk for recurrence for high-risk patients is greatest early (0–3 years) postnephrectomy and plateaus after 4 to 5 years[1].
Some predictive models that have been used for survival outcomes post-nephrectomy for renal cell carcinoma (RCC) including the UISS (University of California LA Integrated Staging System)[2], SSIGN (Stage, Size, Grade, Necrosis)[3], Karakiewicz nomogram[4], GRANT (Grade, Age, Node, and Tumor)[5,6], and Leibovich[7,8]. The criteria used to determine risk in these staging systems can be found in Table 1.

Table 1.
Predictive models for renal cell carcinoma recurrence and survival.
Based on these predictive models, in general, patients with resected stage T3 or higher, and high-grade tumors, are at the highest risk for recurrent disease, and are most likely to benefit from an adjuvant agent that would decrease their risk for recurrence and improve overall survival (OS). Patients at lower risk (T1 and T2A disease) receiving adjuvant therapy for the most part may be overtreated, as the risk for recurrence is less than 20%. The patient population that would likely benefit the most from adjuvant therapy are those with resected metastases, as demonstrated in KEYNOTE-564[9].
Unanswered questions in adjuvant therapy include its role in non-clear cell histology. Non-clear cell histologies can have higher risk for recurrence, but are often excluded in adjuvant trials, including the recent landmark KEYNOTE-564 adjuvant pembrolizumab trial, which required a clear cell component[9].
Adjuvant Therapy Trials in Renal Cell Carcinoma
Cytokine Era: Several adjuvant trials with cytokines or other biologics have been previously completed, and summarized elsewhere, and are outside the scope of this review[10].
Adjuvant Trials with Targeted Agents
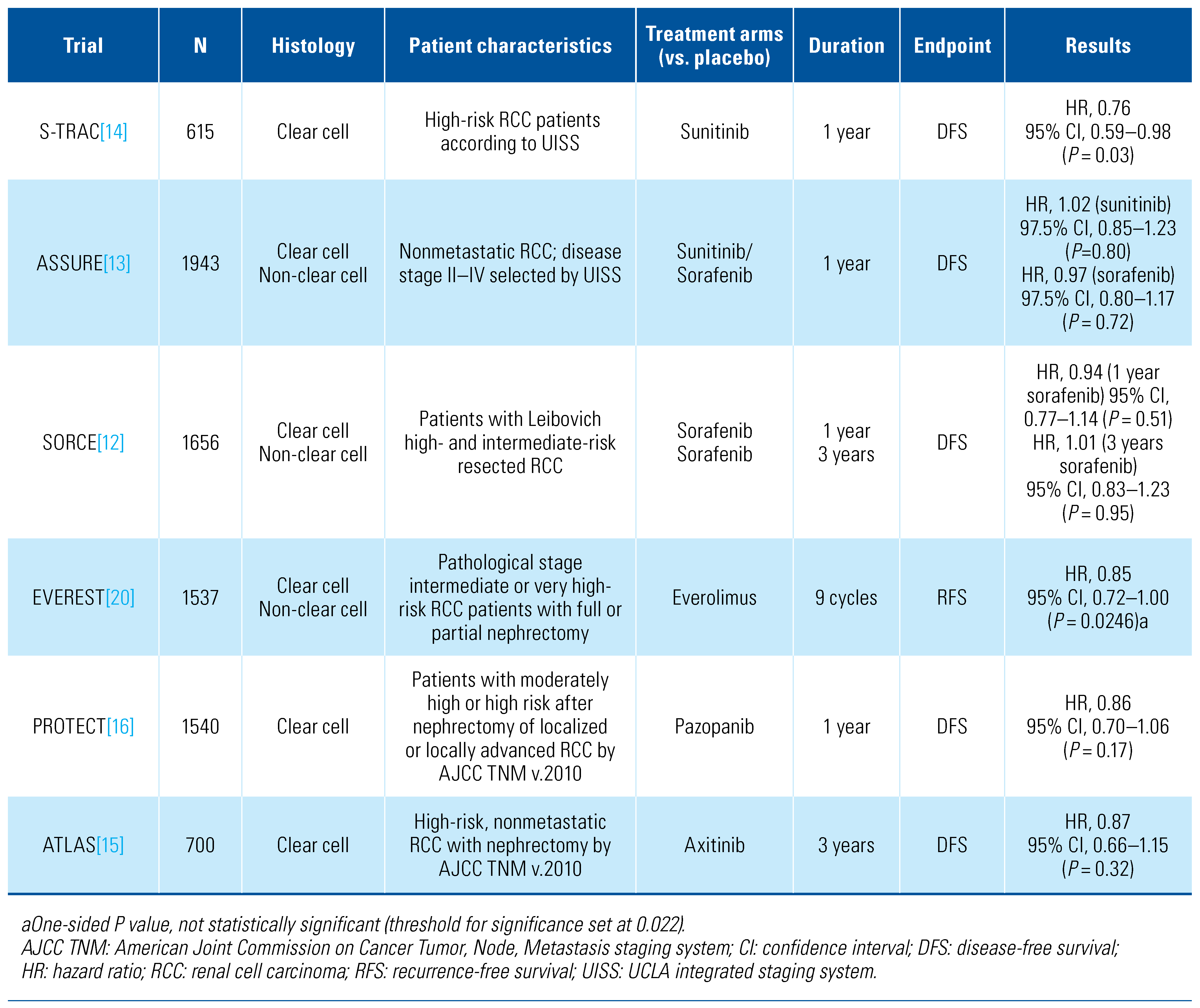
The rationale for testing agents targeting the angiogenic pathway in the adjuvant setting is based on multiple observations showing that vascular endothelial growth factor (VEGF) is involved in the pathogenesis of metastasis[11]. Five placebo-controlled, adjuvant, phase 3 studies investigated the benefit of targeted therapy with VEGFR-TKIs versus placebo (Table 2)[12,13,14,15,16]. The primary endpoint in all trials was disease-free survival (DFS); however, patient populations and study designs varied between the trials, with differing agents and duration of therapy.
Table 2.
Adjuvant trials with targeted agents in RCC.
Of these, only S-TRAC[14], which enrolled the highest risk group (pT3 and higher) demonstrated an improvement in DFS with sunitinib compared with placebo. Patients assigned to sunitinib had a significantly improved DFS (6.8 years; 95% CI, 5.8–not reached) when compared to patients in the placebo arm (5.6 years; 95% CI, 3.8–6.6), though in an updated analysis, there was no difference in OS[17]. Notably, the ASSURE[13] trial did not identify a significant difference between adjuvant sunitinib versus placebo with respect to DFS. The differences in patient population may have accounted for the differences in results between S-TRAC and ASSURE. Only patients with clear cell histology were eligible for S-TRAC, while clear cell histology accounted for only 80% of patients in ASSURE. Additionally, the higher risk (tumor stage 3 or higher) of patients in S-TRAC may have also led to differences in study outcomes. It should be noted, however, that in a post-hoc analysis of a subpopulation subject to the S-TRAC inclusion criteria, DFS was similar between all 3 arms[18]. While this analysis was underpowered to statistically detect a difference between sunitinib and placebo, there was no obvious trend in favor of active treatment. It is also possible that differences in trial conduct between S-TRAC and ASSURE, such as disease imaging intervals (earlier and more frequent in S-TRAC), may have contributed to the observed differences in DFS, but they would not have impact on OS.
While there were differences in outcome of the individual VEGFR-TKI studies, a meta-analysis of adjuvant VEGFR-TKI trials for patients with RCC did identify a DFS benefit (HR, 0.84; 95% CI, 0.76–0.93)[19]. However, the meta-analysis did not identify an OS benefit (nor have any of the individual trials), and due to the lack of a proven OS benefit, coupled with the high rates of unacceptable toxicity and dropout from the treatment arms of the VEGFR-TKI trials, adjuvant therapy with sunitinib has not achieved widespread adoption, even in countries where sunitinib is approved for adjuvant therapy in RCC.
EVEREST is a randomized, placebo-controlled, phase 3 trial of everolimus versus placebo for 54 weeks in patients with clear and non-clear cell RCC after nephrectomy or partial nephrectomy[20]. A total of 1545 patients with pathological stage intermediate- or high-risk status were enrolled. The primary endpoint of the trial was recurrence-free survival (RFS), and with median follow-up of 76 months, there was improvement in the everolimus arm that did not reach statistical significance (HR, 0.85; 95% CI, 0.72–1.00).
Adjuvant Trials with Immune Checkpoint Inhibitors
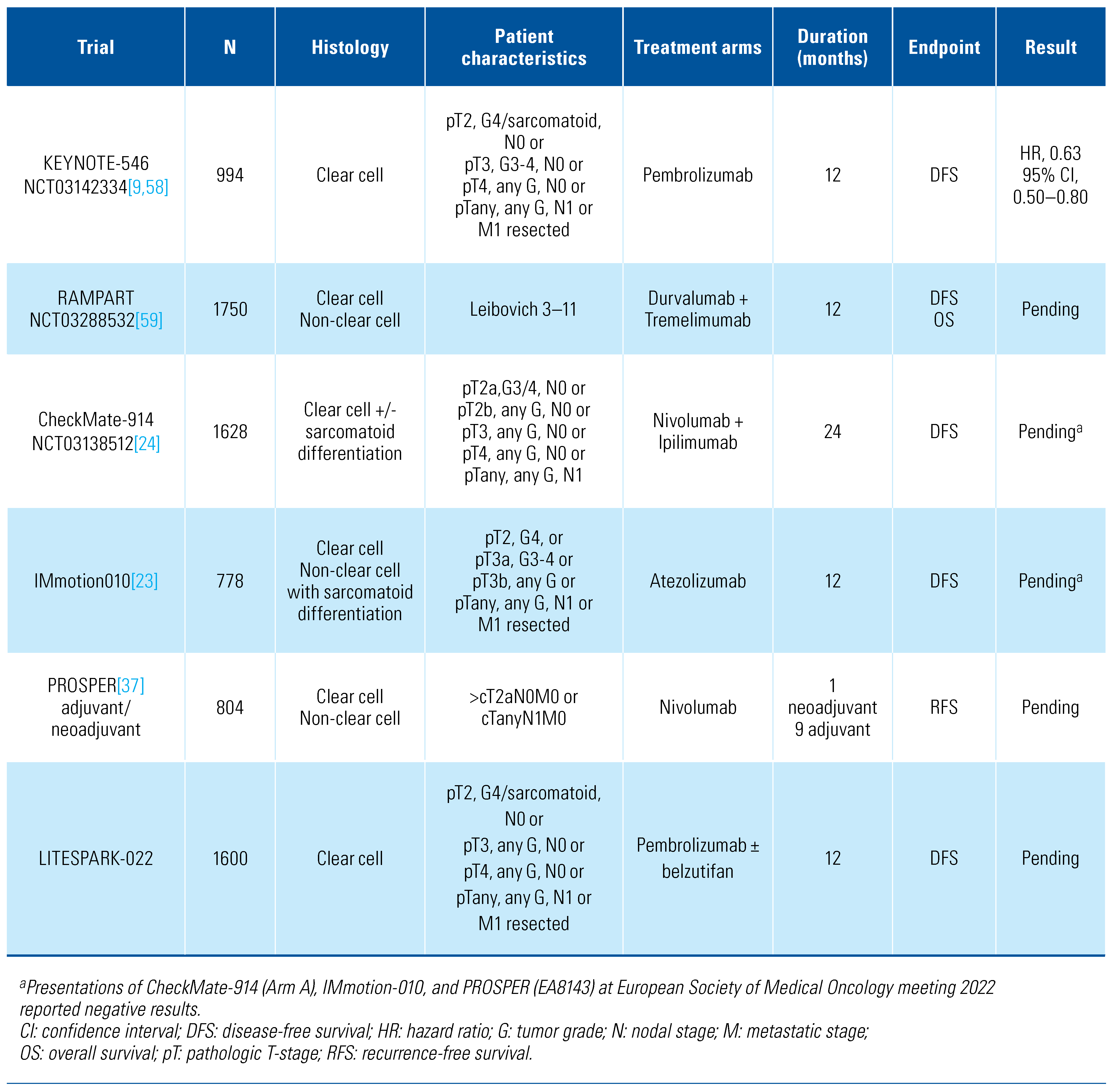
Immune checkpoint inhibitors (IOs) targeting the programmed cell death protein 1 (PD-1) pathway, or the cytotoxic T lymphocyte-associated protein 4 (CTLA-4) pathway have revolutionized the treatment of metastatic RCC. Their role in the adjuvant setting is currently under investigation in multiple clinical trials (Table 3), with one phase 3 trial—KEYNOTE-564—having published results so far.
Table 3.
Ongoing or completed adjuvant trials with immune checkpoint inhibitors in RCC.
KEYNOTE-564[9] is a randomized, double-blind, placebo-controlled, phase 3 trial testing the role of the PD-1 inhibitor pembrolizumab in patients with intermediate-high-risk, high-risk, or M1–no evidence of disease (NED) status including intermediate-risk (pT2, grade 4, N0M0 or pT3, any grade, N0, M0), high-risk (pT4, any grade, any N, M0 or any pT, any grade, N+, M0), and also patients who had undergone complete resection of metastasis (M1), within a year of primary surgery. Patients (n=994) were randomized to receive either pembrolizumab or placebo every 3 weeks for 1 year. The primary endpoint was investigator-assessed DFS, with OS as a secondary endpoint. After a median follow-up of 30.1 months, the DFS rate at 30 months was 75.2% and 65.5% for pembrolizumab and placebo, respectively (HR, 0.63; 95% CI, 0.50–0.80)[21]. OS data is not mature. The authors reported grades 3+4 treatment-related adverse events (AEs) for pembrolizumab and placebo in 18.9% and 1.2%, respectively, with no treatment-related deaths. In the pembrolizumab group, 22% of patients discontinued treatment due to AEs. Based on these findings, pembrolizumab has received United States Food and Drug Administration (FDA) and European Medicines Agency (EMA) approval as an adjuvant treatment in patients with RCC and high risk for relapse.
While data has not yet been presented, recent press releases indicate that adjuvant atezolizumab (IMmotion010) and ipilimumab and nivolumab combination therapy (CheckMate-914) have not demonstrated benefit in the adjuvant setting[22,23,24,25]. Once full results are published, comparisons in trial design and patient selection will need to be carefully examined to determine why the results are inconsistent with KEYNOTE-564. Additional trials evaluating the utility of adjuvant IOs are ongoing (Table 3).
Neoadjuvant Therapy in RCC
The standard-of-care management of nonmetastatic disease remains surgical resection. Just as combination TKI and immunotherapy combinations have come to dominate the frontline metastatic space, so too are investigators attempting to capitalize on the synergy of these agents in the neoadjuvant setting[26,27,28,29,30,31,32,33]. A summary of ongoing trials investigating immunotherapy in the preoperative setting is found in Table 4.
Table 4.
Ongoing clinical trials investigating neoadjuvant therapy (± adjuvant component) in locally advanced or metastatic (with planned cytoreductive nephrectomy) RCC.
Neoadjuvant therapy may have several potential advantages over adjuvant therapy: First, it may decrease tumor burden and improve surgical outcomes, allowing for nephron-sparing surgery in select cases, converting unresectable tumors to resectable, and decreasing venous involvement, thereby facilitating ease of surgery. Second, response of the primary tumor to therapy can predict long-term outcomes to a particular therapy, potentially allowing for adaptive adjuvant therapy trials. Also, neoadjuvant studies allow for collection of molecular correlative data from peripheral blood as well as paired biopsy and resection specimens to aid in response evaluation. Lastly, the in situ tumor may provide increased priming of the immune system compared with micrometastatic disease, leading to a more robust immune response[34,35].
The application of immunotherapy in the neoadjuvant setting is early. Two small phase 2 studies have demonstrated that neoadjuvant nivolumab prior to nephrectomy was safe and feasible, without delay to nephrectomy after receiving at least one dose of nivolumab[36,37]. The phase 3 study of neoadjuvant nivolumab, PROSPER RCC (NCT03055013), is the only phase 3 trial investigating preoperative immunotherapy versus observation, with results pending at the European Society Medical Oncology (ESMO)[38]. Perioperative durvalumab (anti–PD-L1) with or without tremelimumab (anti–CTLA-4) was investigated in a multicohort phase 1b trial evaluating combined IO[39]. There were no treatment-related delays or complications of surgery although the addition of tremelimumab was associated with excess immune-related AEs (irAEs) and the study was suspended.
Rare instances of irAEs delaying surgery, include at least one grade 4 AE, which underscores the need for biologic markers of patient susceptibility to irAEs [36,39,40,41,42]. Notably, there was no signal regarding surgical complications across the above studies of neoadjuvant immunotherapy. These data, combined with retrospective data, suggest that IO is safe to continue through surgery without interruption[43]. Additionally, while patients are less likely to have an AE with immunotherapy in the adjuvant setting, these AEs can be debilitating and permanent, requiring long-term immunosuppression, whereas the AEs seen with VEGFR inhibition typically resolve with drug cessation.
Regulatory Issues
Uptake of new therapies into routine clinical practice is based on published peer-reviewed evidence, influenced by international guidelines and recommendations, and tailored to the needs of each specific patient based on their circumstances and comorbidities. The “real-world” access to and uptake of new therapies is influenced primarily by what is approved and, more importantly, reimbursed in each region or available to those with financial resources. The impact of heterogeneous regulatory approval processes was clearly illustrated with sunitinib. While sunitinib was granted approval as adjuvant therapy for patients with risk for RCC recurrence by the United States FDA, counterparts in the European Union and United Kingdom did not grant approval for an adjuvant indication. Additionally, the Kidney Cancer Research Network of Canada issued a consensus statement that did not support the use of VEGFR-TKI in the adjuvant setting following a systematic review and meta-analysis of trials in this space[44].
In November 2021, the FDA approved adjuvant pembrolizumab for patients who are at intermediate-high or high risk for recurrence after surgery based on the KEYNOTE-564 study results using investigator-assessed DFS as the major efficacy outcome[9]. The review of the pembrolizumab submission was also conducted under Project Orbis, which facilitates concurrent review of oncology products among international partners, allowing for simultaneous decisions in all countries. The Australian Therapeutic Goods Administration, Health Canada, and Swissmedic participated in this review. The approval of pembrolizumab redemonstrated the FDA’s acceptance of DFS as a regulatory endpoint for adjuvant RCC trials. In the UK, the appraisal of pembrolizumab in the adjuvant setting has started, the EMA has approved, and publication of the results from the National Institute for Health and Care Excellence (NICE) are pending[45].
Issues Important to Patients
Adjuvant and Neoadjuvant Therapy
Adjuvant therapy given after curative intent therapy can be likened to life insurance: “a bet you do not want to win.” A life insurance policy is essentially saying to a company, “I bet I die,” and the company saying, “We bet you don’t.” A decision to undertake adjuvant therapy employs similar thinking. Patients with no apparent residual disease will be offered adjuvant therapy to reduce their theoretical risk for recurrence and death from cancer. Most patients who receive adjuvant therapy cannot benefit from it, and are therefore only exposed to possible harms, which is evident in the high discontinuation rate seen in the above adjuvant studies. However, it may be possible to increase the proportion of patients who may benefit through careful patient selection.
Conversely, neoadjuvant therapy is “a bet you want to win”—an investment in treatment now, while cancer is still detectable, to try to improve outcomes from definitive treatment such as surgery. Currently for patients with renal cell cancer, this approach is nearly always in the context of a clinical trial, as its benefit is unproven.
Patient Preferences
Clinicians and patients often have different goals for treatment and expectations of outcomes. A patient preference substudy in the SORCE clinical trial[12] used a validated questionnaire aiming to understand what degree of improvement in survival would be judged by participants and investigators as sufficient to justify their participation and potential side effects from treatment with sorafenib[46]. Investigators judged that larger survival benefits were required than their patients to make adjuvant treatment worthwhile[46,47]. Patients and clinicians also perceive and report adverse events differently. Clinician assessment through the NCI Common Terminology Criteria for Adverse Events (CTCAE) is not always concordant with patient-reported outcomes (PRO)[48]. Owing to the differences between patient and clinician perspectives, it is imperative to work with community partners in the design of adjuvant clinical trials in RCC to ensure the outcomes align with community expectations and needs[49].
Unmet Needs
The most obvious unmet need in the context of clinical trials for RCC is for effective therapies. None of the trials so far have demonstrated a survival advantage, including the data with pembrolizumab in KEYNOTE-564[9]. It is therefore reasonable to advise patients that the standard of care remains observation, with access to life-prolonging therapies in the event of relapse. Patients want better treatments and outcomes with quicker results[50,51,52,53], and they want trials that examine and report the patient experience. These are all considerations for future trial designs but also apply to everyday treatment decision-making.
Future Directions
Several issues need to be considered when designing clinical trials of adjuvant therapy in RCC.
Statistical Designs for the Trials
There is equipoise in arguments for randomized control trials (RCTs) versus multi-arm multistage (MAMS) designs for adjuvant trials. RCTs are preferred in industry and ask well-defined controlled questions. This approach gives confidence that the trial will be delivered in the projected timescale and the simple design is easy for patients and physicians to understand. MAMS trials are ideal for academic consortia and can ask multiple questions simultaneously and in sequence and adapt to new data. Rapid advancements in prostate cancer have been made using this approach via STAMPEDE and in kidney cancer via RAMPART. This model allows adaptions that include adding arms, dropping arms, and changing control arms in light of new data. Although initially less attractive for commercial support, this approach, which demonstrated speed and quality of data at low cost, could be compelling.
Trial Endpoints
The aim of adjuvant treatment is to improve the cure rate or at least to prolong healthy life. OS remains the gold standard but in event-driven trials, this will either take a long time (generally 3 to 4 years to accrue and 3 to 7 years for maturity) or will require very large numbers of patients. This massively increases costs and slows potential progress. Moreover, there is expenditure of patients who may not need therapy and perhaps undertreatment of very high-risk patients. Thus, DFS has become a de facto approach and was an accepted endpoint for S-TRAC and KEYNOTE-564. However, in a recent meta-analysis encompassing 13 studies and more than 6400 patients treated with adjuvant therapies for RCC, correlation between 5-year DFS and OS rates was modest, suggesting DFS is not a good surrogate marker of OS[54]. These results underline the difficulty of choosing the good primary objective in designing an adjuvant clinical trial in RCC.
Essential requirements for future trials include cost-effectiveness: need for innovation in therapies to reduce health care costs, including the medium (such as oral checkpoint inhibitors instead of intravenous), the duration of therapy, and access to care. Finally, quality of life remains underappreciated: the diarrhea and dysgeusia and fatigue experienced from VEGFR-TKIs continue to have poor remedy, and the autoimmune side effects from immunotherapy can be permanent. The risk/ benefit ratio for adjuvant therapy must outweigh that of reserving treatment only for metastatic disease.
Biomarkers Needed
Contemporary metastatic clear cell cancer trial designs have failed to address whether both IO and antiangiogenic therapy are necessary for individual patients. Both pure antiangiogenic trials and pure IO monotherapy trials have been applied to the adjuvant setting with continued uncertainty as to whom would benefit from adjuvant therapy or neoadjuvant therapy and for how long. With the availability of molecular signatures, which could improve prognostication, there is opportunity to design smarter trials. Transcriptomics, which appear to indicate sensitivity or resistance of some metastatic renal cancers to IO or antiangiogenic therapy[55], need validation and could be used to select treatments when indicated, or could be used in the development of adaptive, biomarker-driven basket trials similar to I-SPY2 in breast cancer (NCT01042379). The PROSPER trial is undergoing such analysis retrospectively. Specimens from the ASSURE trial are undergoing whole-exome RNA sequencing, which likely will provide further insight into which patients are more likely to relapse and have worse prognosis. Furthermore, analysis of kidney injury molecule-1 (KIM-1) from blood correlates with detection of recurrence[56] and plasma DNA methylation immunoprecipitation analysis are being retrospectively validated to predict recurrence in this population[57]. If validated, these tools could be applied to future trials to guide patient populations to be offered or spared adjuvant therapy.
Sequencing of Treatments Postadjuvant Therapy
The new approval and future use of IO adjuvant therapy in some patients affects the design of first-line metastatic renal cancer trials. The timing of relapse may be important, as it is untested whether patients who relapse while receiving adjuvant therapy might still benefit from VEGFR-TKI monotherapy or VEGFR-TKI /IO or IO/IO. Furthermore, should patients who relapse 6 months after IO therapy be considered differently than those who relapse later post-therapy? For now, these are unanswered questions. The application of molecular typing becomes essential in this era, and tools such as KIM-1, DNA methylation, or circulating tumor DNA (ctDNA) if sensitive enough, could be used for cancer screening, as is in process in GRAIL[58], to identify earlier cancers and thereby obviate the use of adjuvant therapy in many patients.
Conclusions
While IO shows promise for the adjuvant treatment of high-risk clear cell RCC, there is still much to learn from ongoing clinical trials and longer follow-up data in this space, and the lessons learned from adjuvant targeted therapy trials must now be applied to this era. We must await and properly weigh OS data from trials of adjuvant IO, and we should strive to identify readily scalable biomarkers that can be used to hone patient selection criteria in future prospective therapeutic trials.
Acknowledgments
- N. Haas: Participation on a data safety monitoring board or advisory board: Merck; Eisai, Exilexis, Aveo, Roche (all paid to me). Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid: Co-Chair Genitourinary Committee ECOG-ACRIN, Member NCI GU Steering Committee, ECOG-ACRIN representative to NCI Renal Task Force. Funding: DOD Kidney Cancer Consortium.
- J. Shevach: T32HG009495 funding support.
- I. Davis: Participation on a data safety monitoring board or advisory board: Ipsen; Eisai, BMS, Merck/ Pfizer avelumab, AztraZeneca IO (all advisory boards unpaid; honoraria paid directly to ANZUP). Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid: Director and Board Chair, ANZUP Cancer Trials Group (unpaid).
- Other financial or non-financial interests: Institutional payments to support kidney cancer trials: ANZUP Cancer Trials Group, MSD, AstraZeneca, Exelixis, Merck, Pfizer, Eisai.
- T. Eisen: Employment: AstraZeneca (to March 2020); Employment as VP Oncology Early Clinical Dev Roche (from March 2020); Employment as VP GU Oncology Late Clin Dev AstraZeneca Research support. Stock options AstraZeneca and Roche. Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid: Macmillan Cancer Support Trustee for 10 years to 2021; Cambridge University Health Partners non-executive director
- Travel Support to Genitourinary Symposiums ASCO 2020 Roche.
- M. Gross-Goupil: Participation on a data safety monitoring board or advisory board: MSD, BMS, Pfizer, Ipsen. Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid: Member of the GETUG. Support for attending meetings and/or travel: MSD, Ipsen, BMS, Pfizer.
- A. Kapoor: Participation on a data safety monitoring board or advisory board: Ipsen, Eisai, Merck, BMS, Janssen, Bayer, Abbvie (Advisory Boards). Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid: Chair, Kidney Cancer Research Network of Canada (KCRNC). Stock options: Verity Pharma.
- V. Master: Participation on a data safety monitoring board or advisory board: Merck, Pfizer, BMS, Exilexis.
- Support for attending meetings and/or travel: American College of Surgeons.
- C. Ryan: Grants or contracts from any entity: Ayala, Bristol Meyer Squibb, Daiichi-Sankyo, Deciphera, Exelixis, Genentech, Novartis, Karyopharm, Merck, Nektar, Pfizer, Xynomic, Shasqi, Monopar, Boehringer Ingelheim, PTC Therapeutics, Trillium Therapeutic (to my institution for all). Consulting Fees: Exelixis (all payments to me) Aveo, Daiichi, Sankyo, Synox, Bristol Meyer Squibb, Astra Zeneca, Janssen.
- M. Schmidinger: Consulting fees and honoraria: BMS, MSD, Ipsen, Exelixis, EISAI. Support for attending meetings and/or travel: MSD Ipsen BMS. Participation on a data safety monitoring board or advisory board: BMS MSD, Ipsen, EISAI.
Competing Interests
See ”Acknowledgments” for details.
Abbreviations
| DFS | disease-free survival |
| FDA | United States Food and Drug Administration |
| GRANT | Grade, Age, Node, and Tumor |
| IO | immune checkpoint inhibitor |
| irAEs | immune-related adverse events |
| OS | overall survival |
| RCC | renal cell carcinoma |
| RFS | recurrence-free survival |
| SSIGN | Stage, Size, Grade, Necrosis |
| UISS | University of California LA Integrated Staging System |
| VEGF | vascular endothelial growth factor |
| VEGFR-TKI | vascular endothelial growth factor receptor tyrosine kinase inhibitor |
References
- Chamie, K.; Donin, N.M.; Klöpfer, P.; Bevan, P.; Fall, B.; Wilhelm, O.; et al. Adjuvant Weekly Girentuximab Following Nephrectomy for High-Risk Renal Cell Carcinoma: The ARISER Randomized Clinical Trial. JAMA Oncol. 2017, 3, 913–920. [Google Scholar] [CrossRef]
- Zisman, A.; Pantuck, A.J.; Dorey, F.; Said, J.W.; Shvarts, O.; Quintana, D.; et al. Improved prognostication of renal cell carcinoma using an integrated staging system. J. Clin. Oncol. 2001, 19, 1649–1657. [Google Scholar] [CrossRef] [PubMed]
- Frank, I.; Blute, M.L.; Cheville, J.C.; Lohse, C.M.; Weaver, A.L.; Zincke, H. An outcome prediction model for patients with clear cell renal cell carcinoma treated with radical nephrectomy based on tumor stage, size, grade and necrosis: The SSIGN score. J. Urol. 2002, 168, 2395–2400. [Google Scholar] [CrossRef] [PubMed]
- Karakiewicz, P.I.; Briganti, A.; Chun, F.K.H.; Trinh, Q.-D.; Perrotte, P.; Ficarra, V.; et al. Multi-institutional validation of a new renal cancer–specific survival nomogram. J. Clin. Oncol. 2007, 25, 1316–1322. [Google Scholar] [CrossRef] [PubMed]
- Buti, S.; Puligandla, M.; Bersanelli, M.; DiPaola, R.S.; Manola, J.; Taguchi, S.; et al. Validation of a new prognostic model to easily predict outcome in renal cell carcinoma: The GRANT score applied to the ASSURE trial population. Ann. Oncol. 2017, 28, 2747–2753. [Google Scholar] [CrossRef] [PubMed]
- Buti, S.; Karakiewicz, P.I.; Bersanelli, M.; Capitanio, U.; Tian, Z.; Cortellini, A.; et al. Validation of the GRade, Age, Nodes and Tumor (GRANT) score within the Surveillance Epidemiology and End Results (SEER) database: A new tool to predict survival in surgically treated renal cell carcinoma patients. Sci. Rep. 2019, 9, 13218. [Google Scholar] [CrossRef] [PubMed]
- Leibovich, B.C.; Blute, M.L.; Cheville, J.C.; Lohse, C.M.; Frank, I.; Kwon, E.D.; et al. Prediction of progression after radical nephrectomy for patients with clear cell renal cell carcinoma: A stratification tool for prospective clinical trials. Cancer 2003, 97, 1663–1671. [Google Scholar] [CrossRef] [PubMed]
- Leibovich, B.C.; Cheville, J.C.; Lohse, C.M.; Zincke, H.; Frank, I.; Kwon, E.D.; et al. A scoring algorithm to predict survival for patients with metastatic clear cell renal cell carcinoma: A stratification tool for prospective clinical trials. J. Urol. 2005, 174, 1759–1763; discussion 1763. [Google Scholar] [CrossRef] [PubMed]
- Choueiri, T.K.; Tomczak, P.; Park, S.H.; Venugopal, B.; Ferguson, T.; Chang, Y.H.; et al. Adjuvant Pembrolizumab after Nephrectomy in Renal-Cell Carcinoma. N. Engl. J. Med. 2021, 385, 683–694. [Google Scholar] [CrossRef]
- Dizman, N.; Adashek, J.J.; Hsu, J.; Bergerot, P.G.; Bergerot, C.D.; Pal, S.K. Adjuvant treatment in renal cell carcinoma. Clin. Adv. Hematol. Oncol. 2018, 16, 555–563. [Google Scholar]
- Weis, S.; Cui, J.; Barnes, L.; Cheresh, D. Endothelial barrier disruption by VEGF-mediated Src activity potentiates tumor cell extravasation and metastasis. J. Cell Biol. 2004, 167, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Eisen, T.; Frangou, E.; Oza, B.; Ritchie, A.W.S.; Smith, B.; Kaplan, R.; et al. Adjuvant sorafenib for renal cell carcinoma at intermediate or high risk of relapse: Results from the SORCE Randomized Phase III Intergroup Trial. J. Clin. Oncol. 2020, 38, 4064–4075. [Google Scholar] [CrossRef] [PubMed]
- Haas, N.B.; Manola, J.; Uzzo, R.G.; Flaherty, K.T.; Wood, C.G.; Kane, C.; et al. Adjuvant sunitinib or sorafenib for high-risk, non-metastatic renal-cell carcinoma (ECOG-ACRIN E2805): A double-blind, placebo-controlled, randomised, phase 3 trial. Lancet 2016, 387, 2008–2016. [Google Scholar] [CrossRef] [PubMed]
- Ravaud, A.; Motzer, R.J.; Pandha, H.S.; George, D.J.; Pantuck, A.J.; Patel, A.; et al. Adjuvant sunitinib in high-risk renal-cell carcinoma after nephrectomy. N. Engl. J. Med. 2016, 375, 2246–2254. [Google Scholar] [CrossRef] [PubMed]
- Gross-Goupil, M.; Kwon, T.G.; Eto, M.; Ye, D.; Miyake, H.; Seo, S.I.; et al. Axitinib versus placebo as an adjuvant treatment of renal cell carcinoma: Results from the phase III, randomized ATLAS trial. Ann. Oncol. 2018, 29, 2371–2378. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Haas, N.B.; Donskov, F.; Gross-Goupil, M.; Varlamov, S.; Kopyltsov, E.; et al. Randomized phase III trial of adjuvant pazopanib versus placebo after nephrectomy in patients with localized or locally advanced renal cell carcinoma. J. Clin. Oncol. 2017, 35, 3916–3923. [Google Scholar] [CrossRef]
- Motzer, R.J.; Ravaud, A.; Patard, J.J.; Pandha, H.S.; George, D.J.; Patel, A.; et al. Adjuvant sunitinib for high-risk renal cell carcinoma after nephrectomy: Subgroup analyses and updated overall survival results. Eur. Urol. 2018, 73, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Haas, N.B.; Manola, J.; Dutcher, J.P.; Flaherty, K.T.; Uzzo, R.G.; Atkins, M.B.; et al. Adjuvant treatment for high-risk clear cell renal cancer: Updated results of a high-risk subset of the ASSURE randomized trial. JAMA Oncol. 2017, 3, 1249–1252. [Google Scholar] [CrossRef] [PubMed]
- Massari, F.; Di Nunno, V.; Mollica, V.; Graham, J.; Gatto, L.; Heng, D. Adjuvant tyrosine kinase inhibitors in treatment of renal cell carcinoma: A meta-analysis of available clinical trials. Clin. Genitourin. Cancer 2019, 17, e339–e44. [Google Scholar] [CrossRef]
- Ryan, C.W.; Tangen, C.; Heath, E.I.; Stein, M.N.; Meng, M.; Alva, A.S.; et al. EVEREST: Everolimus for renal cancer ensuing surgical therapy—A phase III study (SWOG S0931, NCT01120249). J. Clin. Oncol. 2022, 40 (Suppl. 17), LBA4500–LBA. [Google Scholar] [CrossRef]
- Powles, T.; Tomczak, P.; Park, S.H.; Venugopal, B.; Ferguson, T.; Symeonides, S.N.; et al. Pembrolizumab versus placebo as post-nephrectomy adjuvant therapy for clear cell renal cell carcinoma (KEYNOTE-564): 30-month follow-up analysis of a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2022, 23, 1133–1144. [Google Scholar] [CrossRef] [PubMed]
- Bristol Myers Squibb. Bristol Myers Squibb Provides Update on CheckMate -914 Trial Evaluating Opdivo (nivolumab) Plus Yervoy (ipilimumab) as Adjuvant Treatment of Localized Renal Cell Carcinoma [Press Release]. Available online: https://news.bms.com/news/ details/2022/Bristol-Myers-Squibb-Provides-Update-on-CheckMate--914-Trial-Evaluating-Opdivo-nivolumab-Plus-Yervoy-ipilimumab-as-Adjuvant-Treatment-of-Localized-Renal-Cell-Carcinoma/default.aspx (accessed on 29 July 2022).
- Uzzo, R.; Bex, A.; Rini, B.I.; Albiges, L.; Suarez, C.; Donaldson, F.; et al. A phase III study of atezolizumab (atezo) vs placebo as adjuvant therapy in renal cell carcinoma (RCC) patients (pts) at high risk of recurrence following resection (IMmotion010). J. Clin. Oncol. 2017, 35 (Suppl. 15), TPS4598-TPS. [Google Scholar] [CrossRef]
- Bex, A.; Russo, P.; Tomita, Y.; Grünwald, V.; Ramirez, L.-M.; McHenry, B.M.; et al. A phase III, randomized, placebo-controlled trial of nivolumab or nivolumab plus ipilimumab in patients with localized renal cell carcinoma at high-risk of relapse after radical or partial nephrectomy (CheckMate 914). J. Clin. Oncol. 2020, 38 (Suppl. 15), TPS5099–TPS. [Google Scholar] [CrossRef]
- Oza, B.; Frangou, E.; Smith, B.; Bryant, H.; Kaplan, R.; Choodari-Oskooei, B.; et al. RAMPART: A phase III multi-arm multi-stage trial of adjuvant checkpoint inhibitors in patients with resected primary renal cell carcinoma (RCC) at high or intermediate risk of relapse. Contemp. Clin. Trials. 2021, 108, 106482. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.; Choueiri, T.K. Lenvatinib plus pembrolizumab for renal cell carcinoma. Reply. N. Engl. J. Med. 2021, 385, 287. [Google Scholar] [PubMed]
- Rini, B.I.; Plimack, E.R.; Stus, V.; Gafanov, R.; Hawkins, R.; Nosov, D.; et al. Pembrolizumab (pembro) plus axitinib (axi) versus sunitinib as first-line therapy for metastatic renal cell carcinoma (mRCC): Outcomes in the combined IMDC intermediate/poor risk and sarcomatoid subgroups of the phase 3 KEYNOTE-426 study. J. Clin. Oncol. 2019, 37 (Suppl. 15), 4500. [Google Scholar] [CrossRef]
- Powles, T.; Plimack, E.R.; Soulières, D.; Waddell, T.; Stus, V.; Gafanov, R.; et al. Pembrolizumab plus axitinib versus sunitinib monotherapy as first-line treatment of advanced renal cell carcinoma (KEYNOTE-426): Extended follow-up from a randomised, open-label, phase 3 trial. Lancet Oncol. 2020, 21, 1563–1573. [Google Scholar] [CrossRef] [PubMed]
- Albiges, L.; Rini, B.I.; Haanen, J.B.A.G.; Motzer, R.J.; Kollmannsberger, C.K.; Negrier, S.; et al. 908PD - Primary renal tumour shrinkage in patients (pts) who did not undergo upfront cytoreductive nephrectomy (uCN): Subgroup analysis from the phase III JAVELIN Renal 101 trial of first-line avelumab + axitinib (A + Ax) vs sunitinib (S) for advanced renal cell carcinoma (aRCC). Ann. Oncol. 2019, 30, v359–v60. [Google Scholar]
- Choueiri, T.K.; Powles, T.; Burotto, M.; Escudier, B.; Bourlon, M.T.; Zurawski, B.; et al. Nivolumab plus Cabozantinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2021, 384, 829–841. [Google Scholar] [CrossRef]
- Motzer, R.J.; Penkov, K.; Haanen, J.; Rini, B.; Albiges, L.; Campbell, M.T.; et al. Avelumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1103–1115. [Google Scholar] [CrossRef]
- Dallos, M.; Aggen, D.H.; Ager, C.; Obradovic, A.; Easterlin, C.A.; Hawley, J.; et al. The SPARC-1 trial: A phase I study of neoadjuvant combination interleukin-1 beta and PD-1 blockade in localized clear cell renal cell carcinoma. J. Clin. Oncol. 2021, 39 (Suppl. 6), TPS373-TPS. [Google Scholar] [CrossRef]
- Wang, D.Y.; Salem, J.-E.; Cohen, J.V.; Chandra, S.; Menzer, C.; Ye, F.; et al. Fatal toxic effects associated with immune checkpoint inhibitors: A systematic review and meta-analysis. JAMA Oncol. 2018, 4, 1721–1728. [Google Scholar] [CrossRef] [PubMed]
- Topalian, S.L.; Taube, J.M.; Pardoll, D.M. Neoadjuvant checkpoint blockade for cancer immunotherapy. Science 2020, 367. [Google Scholar] [CrossRef] [PubMed]
- Krishnamoorthy, M.; Lenehan, J.G.; Maleki Vareki, S. Neoadjuvant Immunotherapy for High-Risk, Resectable Malignancies: Scientific Rationale and Clinical Challenges. J. Natl. Cancer Inst. 2021, 113, 823–832. [Google Scholar] [CrossRef]
- Gorin, M.A.; Patel, H.D.; Rowe, S.P.; Hahn, N.M.; Hammers, H.J.; Pons, A.; et al. Neoadjuvant nivolumab in patients with high-risk nonmetastatic renal cell carcinoma. Eur. Urol. Oncol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Carlo, M.I.; Attalla, K.; Mazaheri, Y.; Gupta, S.; Yildirim, O.; Murray, S.J.; et al. Phase II study of neoadjuvant nivolumab in patients with locally advanced clear cell renal cell carcinoma undergoing nephrectomy. Eur. Urol. 2022, 81, 570–573. [Google Scholar] [CrossRef] [PubMed]
- Harshman, L.C.; Puligandla, M.; Haas, N.B.; Allaf, M.; Drake, C.G.; McDermott, D.F.; et al. PROSPER: A phase III randomized study comparing perioperative nivolumab (nivo) versus observation in patients with localized renal cell carcinoma (RCC) undergoing nephrectomy (ECOG-ACRIN 8143). J Clin Oncol. 2019, 37 (Suppl. 7), TPS684-TPS. [Google Scholar] [CrossRef]
- Ornstein, M.C.; Zabell, J.; Wood, L.S.; Hobbs, B.; Devonshire, S.; Martin, A.; et al. A phase Ib trial of neoadjuvant/adjuvant durvalumab +/- tremelimumab in locally advanced renal cell carcinoma (RCC). J. Clin. Oncol. 2020, 38 (Suppl. 15), 5021. [Google Scholar] [CrossRef]
- Carlo, M.I.; Attalla, K.; Patil, S.; Murray, S.J.; Chen, Y.-B.; Kotecha, R.; et al. A pilot study of preoperative nivolumab in high-risk nonmetastatic renal cell carcinoma. J. Clin. Oncol. 2021, 39 (Suppl. 6), 323. [Google Scholar] [CrossRef]
- Forde, P.M.; Chaft, J.E.; Smith, K.N.; Anagnostou, V.; Cottrell, T.R.; Hellmann, M.D.; et al. Neoadjuvant PD-1 Blockade in Resectable Lung Cancer. N. Engl. J. Med. 2018, 378, 1976–1986. [Google Scholar] [CrossRef]
- Schmid, P.; Cortes, J.; Pusztai, L.; McArthur, H.; Kümmel, S.; Bergh, J.; et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N. Engl. J. Med. 2020, 382, 810–821. [Google Scholar] [CrossRef] [PubMed]
- Elias, A.W.; Kasi, P.M.; Stauffer, J.A.; Thiel, D.D.; Colibaseanu, D.T.; Mody, K.; et al. The Feasibility and Safety of Surgery in Patients Receiving Immune Checkpoint Inhibitors: A Retrospective Study. Front. Oncol. 2017, 7, 121. [Google Scholar] [CrossRef] [PubMed]
- Karakiewicz, P.I.; Zaffuto, E.; Kapoor, A.; Basappa, N.S.; Bjarnason, G.A.; Blais, N.; et al. Kidney Cancer Research Network of Canada consensus statement on the role of adjuvant therapy after nephrectomy for high-risk, non-metastatic renal cell carcinoma: A comprehensive analysis of the literature and meta-analysis of randomized controlled trials. Can. Urol. Assoc. J. 2018, 12, 173–180. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Pembrolizumab for adjuvant treatment of renal cell carcinoma [ID3810]. In development [GID-TA10693]. Expected publication date: September 28. 2022. Available online: https://www.nice.org.uk/guidance/indevelopment/ gid-ta10693 (accessed on 17 June 2022).
- Lawrence, N.J.; Martin, A.; Davis, I.D.; Troon, S.; Sengupta, S.; Hovey, E.; et al. What survival benefits are needed to make adjuvant sorafenib worthwhile after resection of intermediate- or high-risk renal cell carcinoma? clinical investigators‘ preferences in the SORCE Trial. Kidney Cancer 2018, 2, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Blinman, P.L.; Davis, I.D.; Martin, A.; Troon, S.; Sengupta, S.; Hovey, E.; et al. Patients‘ preferences for adjuvant sorafenib after resection of renal cell carcinoma in the SORCE trial: What makes it worthwhile? Ann. Oncol. 2018, 29, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, T.M.; Ryan, S.J.; Bennett, A.V.; Stover, A.M.; Saracino, R.M.; Rogak, L.J.; et al. The association between clinician-based common terminology criteria for adverse events (CTCAE) and patient-reported outcomes (PRO): A systematic review. Support. Care Cancer 2016, 24, 3669–3676. [Google Scholar] [CrossRef] [PubMed]
- Battle, D.; Jonasch, E.; Hammers, H.J.; Derweesh, I.; George, D.J.; Bex, A.; et al. Patients perspectives on adjuvant therapy in renal cell carcinoma. J. Clin. Oncol. 2018, 36 (Suppl. 6), 644. [Google Scholar] [CrossRef]
- Cruz Rivera, S.; McMullan, C.; Jones, L.; Kyte, D.; Slade, A.; Calvert, M. The impact of patient-reported outcome data from clinical trials: Perspectives from international stakeholders. J. Patient Rep. Outcomes 2020, 4, 51. [Google Scholar] [CrossRef] [PubMed]
- Kadam, R.A. Informed consent process: A step further towards making it meaningful! Perspect. Clin. Res. 2017, 8, 107–112. [Google Scholar] [CrossRef]
- Mercieca-Bebber, R.; King, M.T.; Calvert, M.J.; Stockler, M.R.; Friedlander, M. The importance of patient-reported outcomes in clinical trials and strategies for future optimization. Patient Relat. Outcome Meas. 2018, 9, 353–367. [Google Scholar] [CrossRef]
- Zeps, N.; Northcott, N.; Weekes, L. Opportunities for eConsent to enhance consumer engagement in clinical trials. Med. J. Aust. 2020, 213, 260–262. [Google Scholar] [CrossRef] [PubMed]
- Harshman, L.C.; Xie, W.; Moreira, R.B.; Bossé, D.; Ruiz Ares, G.J.; Sweeney, C.J.; et al. Evaluation of disease-free survival as an intermediate metric of overall survival in patients with localized renal cell carcinoma: A trial-level meta-analysis. Cancer 2018, 124, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Banchereau, R.; Hamidi, H.; Powles, T.; McDermott, D.; Atkins, M.B.; et al. Molecular Subsets in Renal Cancer Determine Outcome to Checkpoint and Angiogenesis Blockade. Cancer Cell. 2020, 38, 803–817. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Puligandla, M.; Halbert, B.; Haas, N.B.; Flaherty, K.T.; Uzzo, R.G.; et al. Plasma KIM-1 is associated with recurrence risk after nephrectomy for localized renal cell carcinoma: A trial of the ECOG-ACRIN Research Group (E2805). Clin. Cancer Res. 2021, 27, 3397–3403. [Google Scholar] [CrossRef] [PubMed]
- Nuzzo, P.V.; Berchuck, J.E.; Korthauer, K.; Spisak, S.; Nassar, A.H.; Abou Alaiwi, S.; et al. Detection of renal cell carcinoma using plasma and urine cell-free DNA methylomes. Nat. Med. 2020, 26, 1041–1043. [Google Scholar] [CrossRef]
- Liu, M.C.O.G.; Klein, E.A.; Swanton, C.; Seiden, M.V. Sensitive and specific multi-cancer detection and localization using methylation signatures in cell-free DNA. Ann. Oncol. 2020, 31, 745–759. [Google Scholar] [CrossRef]
This is an open access article under the terms of a license that permits non-commercial use, provided the original work is properly cited. © 2022 The Authors. Société Internationale d'Urologie Journal, published by the Société Internationale d'Urologie, Canada.