Urogenital Malignancy and Cannabis Use: A Narrative Review

Abstract
:1. Introduction
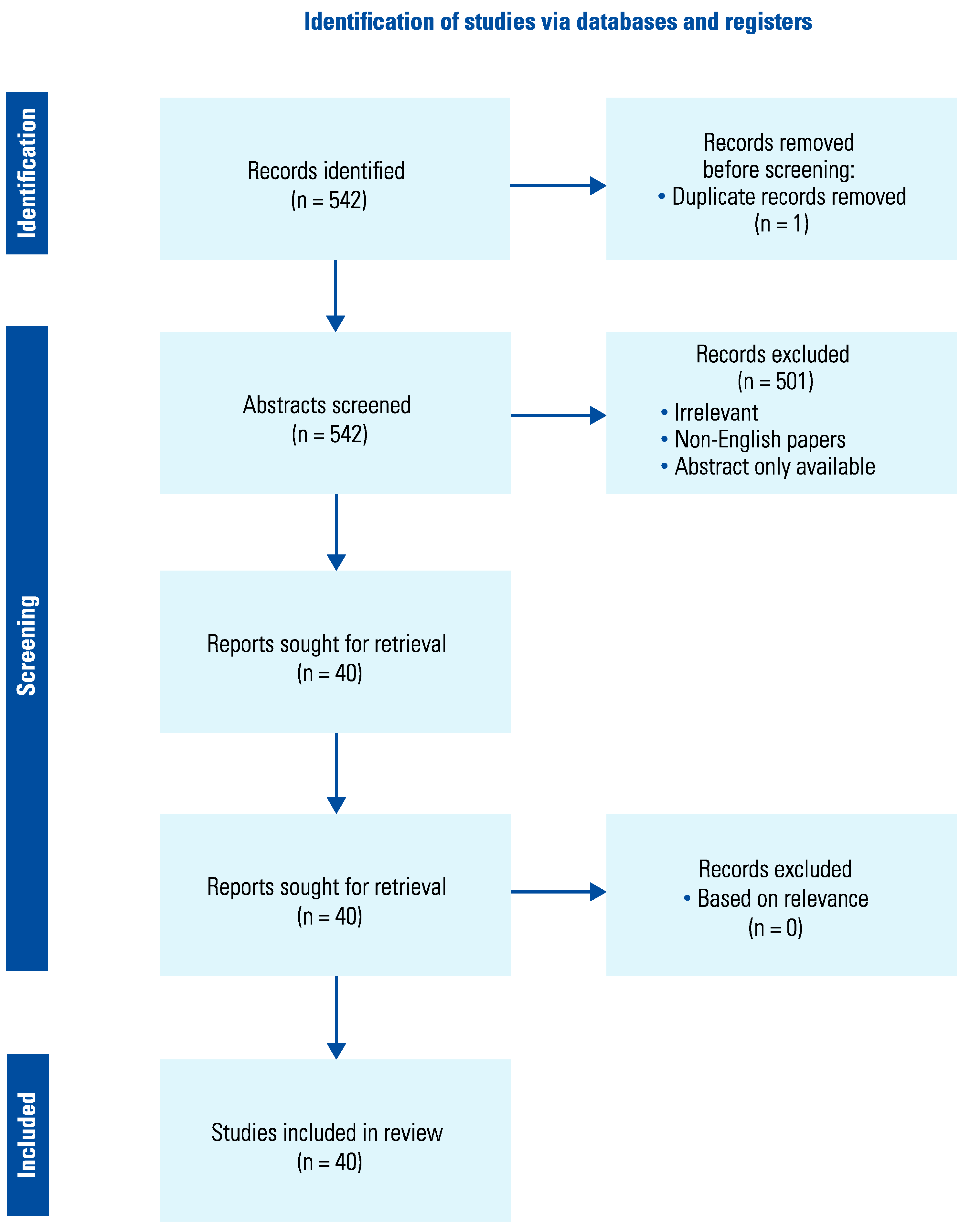
2. Methods
2.1. Search strategy
2.2. Data extraction and screening
3. Results
4. Discussion
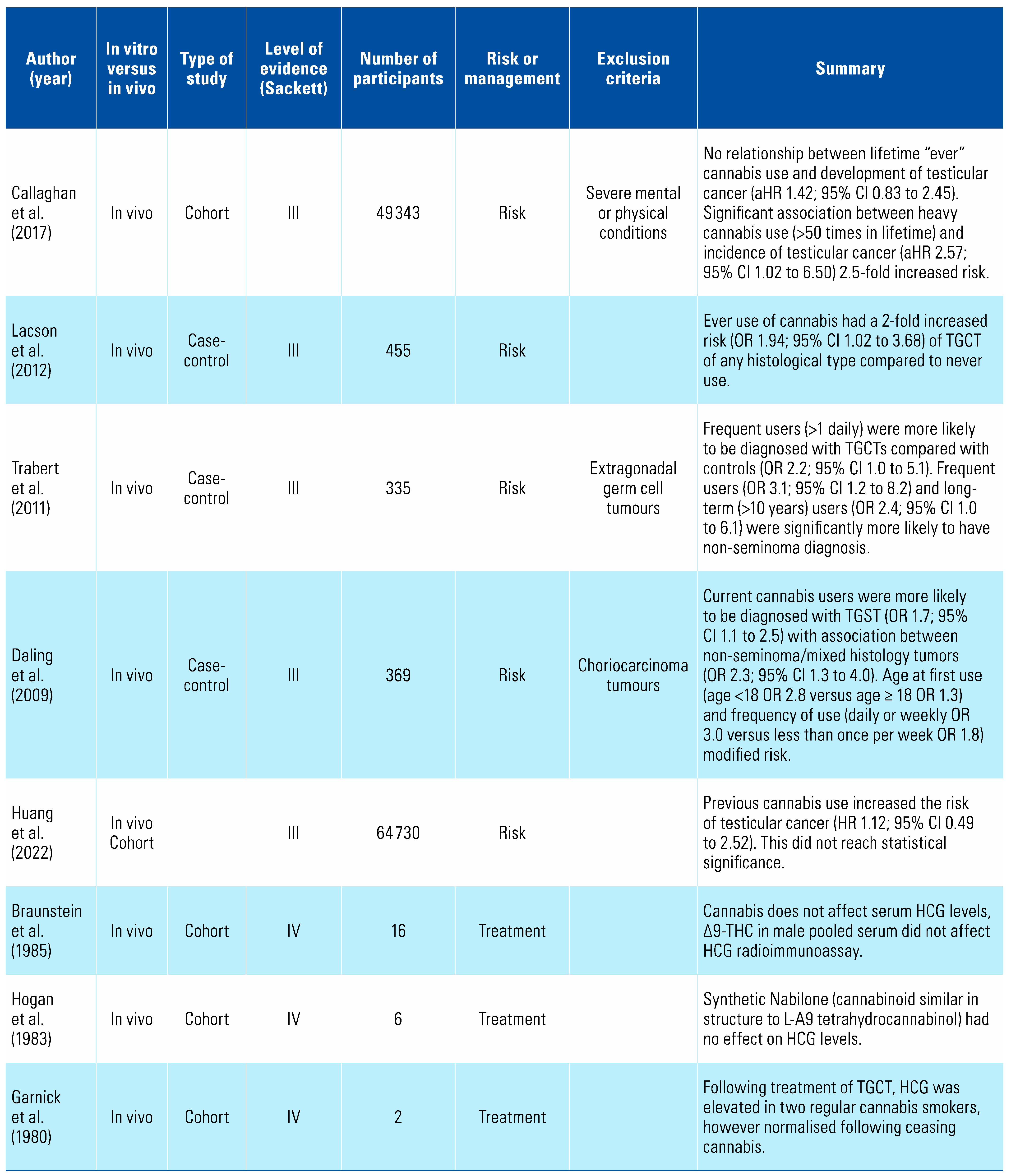
4.1. Testicular Cancer
4.2. Penile Cancer
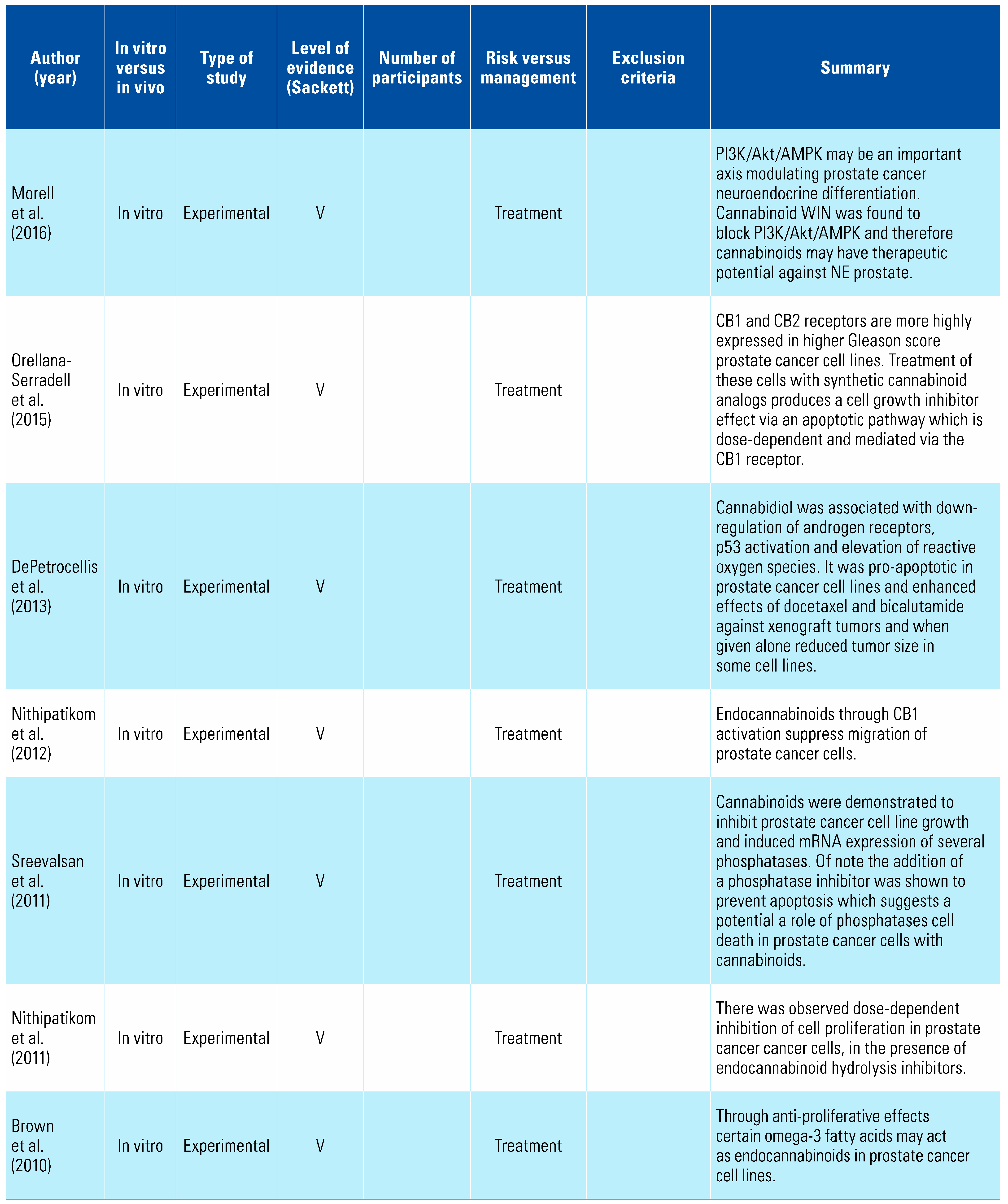
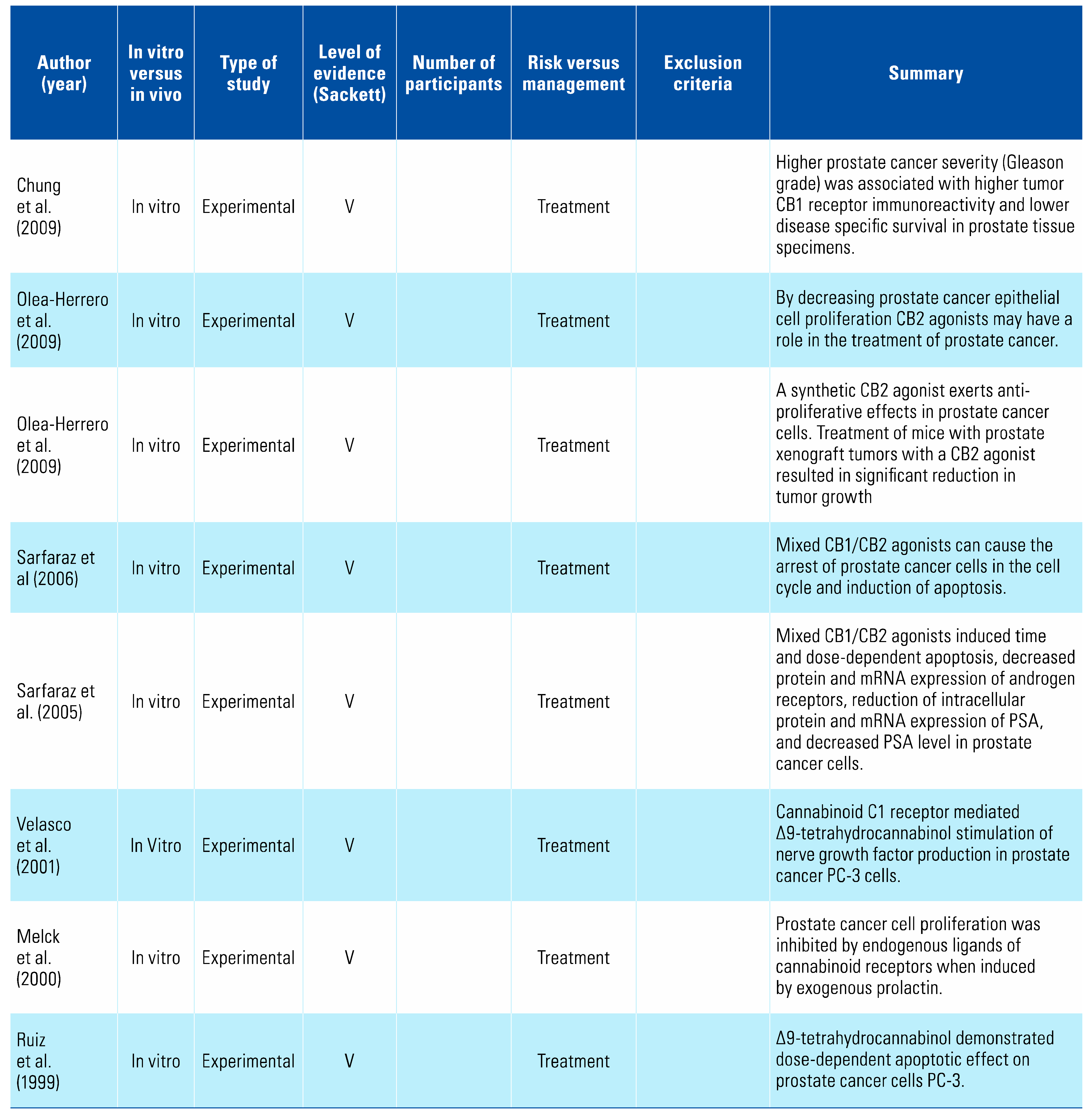
4.3. Prostate Cancer
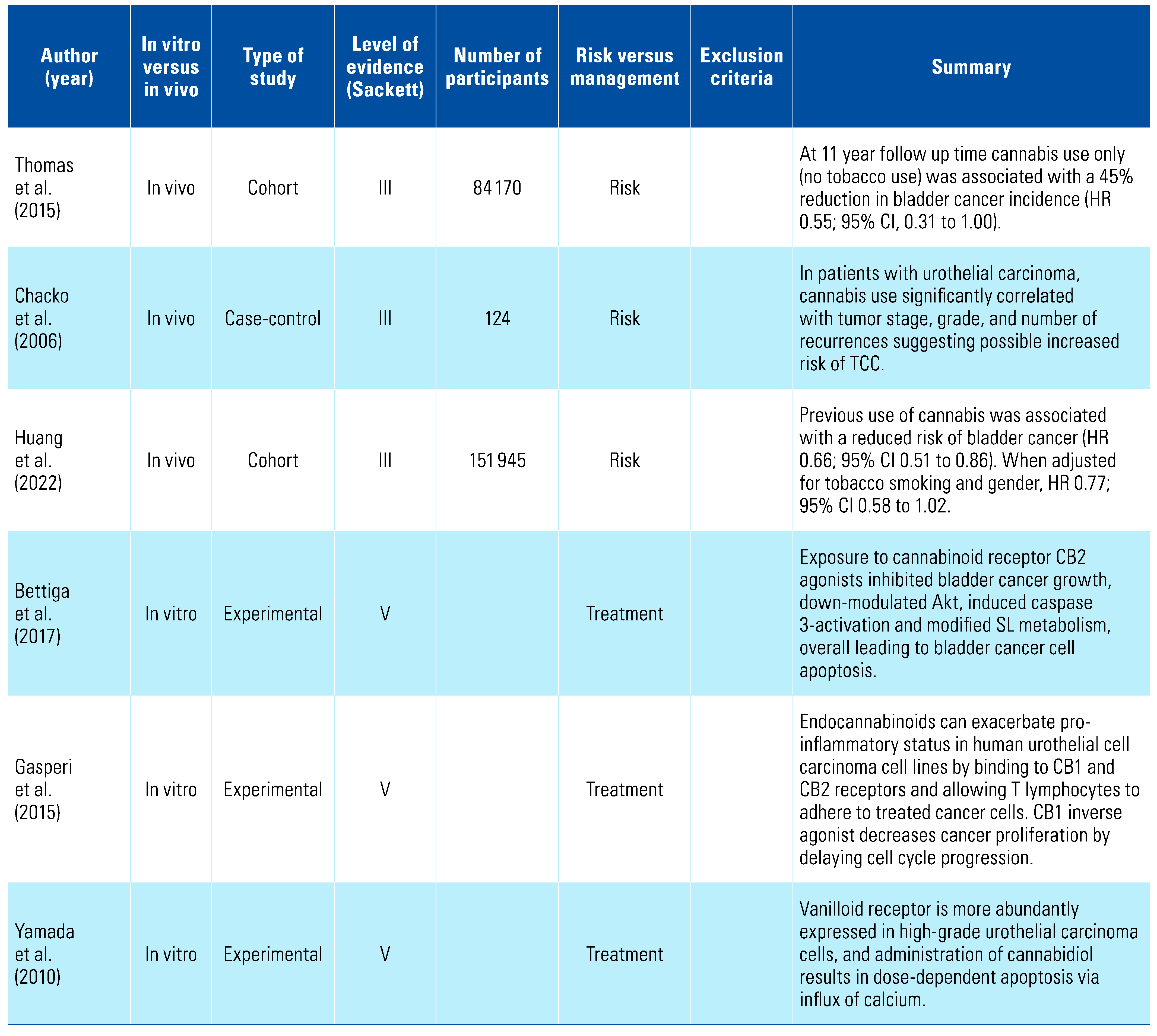
4.4. Bladder Cancer
4.5. Renal Cancer
4.6. Confounding effect of tobacco
4.7. Effect of THC delivery
4.8. Limitations
4.9. Future directions
5. Conclusion
Conflicts of Interest
Abbreviations
| CB | cannabinoid receptor |
| hCG | human chorionic gonadotropin |
| RCC | renal cell carcinoma |
| TGCT | testicular germ cell tumours |
| THC | tetrahydrocannabinol |
| UC | urothelial carcinoma |
References
- United Nation Office on Drugs and Crime. World Drug Report 2021: Cannabis and opioids [Internet]. 2021. Available online: https://www.unodc.org/res/wdr2021/field/WDR21_Booklet_4.pdf https://www.unodc.org/res/wdr2021/field/WDR21_Booklet_3.pdf (accessed on 09 December 2022).
- Rossato, M.; Pagano, C.; Vettor, R. The cannabinoid system and male reproductive functions. J Neuroendocrinol. 2008, 20 (Suppl. 1), 90–93. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. National Drug Strategy Household Survey 2019. Canberra; 2020.
- Zi, H.; He, S.H.; Leng, X.Y.; Xu, X.F.; Huang, Q.; Weng, H.; et al. Global, regional, and national burden of kidney, bladder, and prostate cancers and their attributable risk factors, 1990–2019. Mil Med Res. 2021, 8, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Daling, J.R.; Doody, D.R.; Sun, X.; Trabert, B.L.; Weiss, N.S.; Chen, C.; et al. Association of marijuana use and the incidence of testicular germ cell tumors. Cancer. 2009, 115, 1215–1223. [Google Scholar] [CrossRef] [PubMed]
- Lacson, J.C.A.; Carroll, J.D.; Tuazon, E.; Castelao, E.J.; Bernstein, L.; Cortessis, V.K. Population-based case-control study of recreational drug use and testis cancer risk confirms an association between marijuana use and nonseminoma risk. Cancer. 2012, 118, 5374–5383. [Google Scholar] [CrossRef] [PubMed]
- Trabert, B.; Sigurdson, A.J.; Sweeney, A.M.; Strom, S.S.; Mcglynn, K.A. Marijuana use and testicular germ cell tumors. Cancer. 2011, 117, 848–853. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Huang, D.; Ruan, X.; Huang, J.; Xu, D.; Heavey, S.; et al. Association between cannabis use with urological cancers: a population-based cohort study and a mendelian randomization study in the UK biobank. Cancer Med. 2022. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Garnick, M.B. Spurious rise in human chorionic gonadotropin induced by marihuana in patients with testicular cancer. N Engl J Med. 1980, 303, 1177. [Google Scholar]
- Braustein, G.; Thompson, R.; Gross, S.; Soares, J. Marijuana use does not spuriously elevate serum human chorionic gonadotropin levels. Urology. 1985, 25. [Google Scholar]
- Sidney, S.; Quesenberry, C.P.; Friedman, G.D.; Tekawa, I.S. Marijuana use and cancer incidence (California, United States). Cancer Causes Control. 1997, 8, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Roberto, D.; Klotz, L.H.; Venkateswaran, V. Cannabinoid WIN 55,212-2 induces cell cycle arrest and apoptosis, and inhibits proliferation, migration, invasion, and tumor growth in prostate cancer in a cannabinoid-receptor 2 dependent manner. Prostate. 2019, 79, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Morales, P.; Vara, D.; Goméz-Cañas, M.; Zúñiga, M.C.; Olea-Azar, C.; Goya, P.; et al. Synthetic cannabinoid quinones: Preparation, in vitro antiproliferative effects and in vivo prostate antitumor activity. Eur J Med Chem. 2013, 70, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Brown, I.; Cascio, M.G.; Wahle, K.W.J.; Smoum, R.; Mechoulam, R.; Ross, R.A.; et al. Cannabinoid receptor-dependent and -independent anti-proliferative effects of omega-3 ethanolamides in androgen receptor-positive and -negative prostate cancer cell lines. Carcinogenesis 2010, 31, 1584–1591. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.C.; Hammarsten, P.; Josefsson, A.; Stattin, P.; Granfors, T.; Egevad, L.; et al. A high cannabinoid CB1 receptor immunoreactivity is associated with disease severity and outcome in prostate cancer. Eur J Cancer. 2009, 45, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Olea-Herrero, N.; Vara, D.; Malagarie-Cazenave, S.; Díaz-Laviada, I. Inhibition of human tumour prostate PC-3 cell growth by cannabinoids R()-Methanandamide and JWH-015: Involvement of CB 2. Br J Cancer. 2009, 101, 940–950. [Google Scholar] [CrossRef] [PubMed]
- Olea-Herrero, N.; Vara, D.; Malagarie-Cazenave, S.; Díaz-Laviada, I. The cannabinoid R()methanandamide induces IL-6 secretion by prostate cancer PC3 cells. J Immunotoxicol. 2009, 6, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Sarfaraz, S.; Afaq, F.; Adhami, V.M.; Mukhtar, H. Cannabinoid receptor as a novel target for the treatment of prostate cancer. Cancer Res. 2005, 65, 1635–1641. [Google Scholar] [CrossRef] [PubMed]
- Sarfaraz, S.; Afaq, F.; Adhami, V.M.; Malik, A.; Mukhtar, H. Cannabinoid receptor agonist-induced apoptosis of human prostate cancer cells LNCaP proceeds through sustained activation of ERK1/2 leading to G 1 cell cycle arrest. J Biol Chem. 2006, 281, 39480–36491. [Google Scholar] [CrossRef] [PubMed]
- Velasco, L.; Ruiz, L.; Sánchez, M.G.; Díaz-Laviada, I. Δ9-tetrahydrocannabinol increases nerve growth factor production by prostate PC-3 cells: Involvement of CB1 cannabinoid receptor and Raf-1. Eur J Biochem. 2001, 268, 531–535. [Google Scholar] [CrossRef] [PubMed]
- Melck, D.; De Petrocellis, L.; Orlando, P.; Bisogno, T.; Laezza, C.; Bifulco, M.; et al. Suppression of nerve growth factor Trk receptors and prolactin receptors by endocannabinoids leads to inhibition of human breast and prostate cancer cell proliferation. Endocrinology. 2000, 141, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, L.; Miguel, A.; Díaz-Laviada, I. Δ9-Tetrahydrocannabinol induces apoptosis in human prostate PC-3 cells via a receptor-independent mechanism. FEBS Lett. 1999, 458, 400–404. [Google Scholar] [CrossRef] [PubMed]
- Pietrovito, L.; Iozzo, M.; Bacci, M.; Giannoni, E.; Chiarugi, P. Treatment with cannabinoids as a promising approach for impairing fibroblast activation and prostate cancer progression. Int J Mol Sci. 2020, 21, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Baram, L.; Peled, E.; Berman, P.; Yellin, B.; Besser, E.; Benami, M.; et al. The heterogeneity and complexity of Cannabis extracts as antitumor agents. Oncotarget. 2019, 10, 4091–4106. [Google Scholar] [CrossRef] [PubMed]
- Kosgodage, U.S.; Mould, R.; Henley, A.B.; Nunn, A.V.; Guy, G.W.; Thomas, E.L. Cannabidiol (CBD) is a novel inhibitor for exosome and microvesicle (EMV) release in cancer. Front Pharmacol. 2018, 9, 1–17. [Google Scholar] [CrossRef]
- Morell, C.; Bort, A.; Vara, D.; Ramos-Torres, A.; Rodríguez-Henche, N.; Díaz-Laviada, I. The cannabinoid WIN 55,212-2 prevents neuroendocrine differentiation of LNCaP prostate cancer cells. Prostate Cancer Prostatic Dis. 2016, 19, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Orellana-Serradell, O.; Poblete, C.E.; Sanchez, C.; Castellón, E.A.; Gallegos, I.; Huidobro, C.; et al. Proapoptotic effect of endocannabinoids in prostate cancer cells. Oncol Rep. 2015, 33, 1599–1608. [Google Scholar] [CrossRef] [PubMed]
- De Petrocellis, L.; Ligresti, A.; Schiano Moriello, A.; Iappelli, M.; Verde, R.; Stott, C.G.; et al. Non-THC cannabinoids inhibit prostate carcinoma growth in vitro and in vivo: pro-apoptotic effects and underlying mechanisms. Br J Pharmacol. 2013, 168, 79–102. [Google Scholar] [CrossRef] [PubMed]
- Nithipatikom, K.; Gomez-Granados, A.D.; Tang, A.T.; Pfeiffer, A.W.; Williams, C.L.; Campbell, W.B. Cannabinoid receptor type 1 (CB1) activation inhibits small GTPase RhoA activity and regulates motility of prostate carcinoma cells. Endocrinology. 2012, 153, 29–41. [Google Scholar] [CrossRef] [PubMed]
- Sreevalsan, S.; Joseph, S.; Jutooru, I.; Chadalapaka, G.; Safe, S.H. Induction of apoptosis by cannabinoids in prostate and colon cancer cells is phosphatase dependent. Anticancer Res. 2011, 31, 3799–3807. [Google Scholar] [PubMed]
- Thomas, A.A.; Wallner, L.P.; Quinn, V.P.; Slezak, J.; Van Den Eeden, S.K.; Chien, G.W.; et al. Association between cannabis use and the risk of bladder cancer: results from the California men’s health study. Urology. 2015, 85, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Chacko, J.A.; Heiner, J.G.; Siu, W.; Macy, M.; Terris, M.K. Association between marijuana use and transitional cell carcinoma. Urology. 2006, 67, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Bettiga, A.; Aureli, M.; Colciago, G.; Murdica, V.; Moschini, M.; Lucianò, R.; et al. Bladder cancer cell growth and motility implicate cannabinoid 2 receptor-mediated modifications of sphingolipids metabolism. Sci Rep. 2017, 7, 1–11. [Google Scholar] [CrossRef]
- Gasperi, V.; Evangelista, D.; Oddi, S.; Florenzano, F.; Chiurchiù, V.; Avigliano, L.; et al. Regulation of inflammation and proliferation of human bladder carcinoma cells by type-1 and type-2 cannabinoid receptors. Life Sci. 2015; 138, 41–51. [Google Scholar] [CrossRef]
- Yamada, T.; Ueda, T.; Shibata, Y.; Ikegami, Y.; Saito, M.; Ishida, Y.; et al. TRPV2 activation induces apoptotic cell death in human T24 bladder cancer cells: a potential therapeutic target for bladder cancer. Urology. 2010, 76, 509.e1–509.e7. [Google Scholar] [CrossRef] [PubMed]
- Maden, C.; Sherman, K.J.; Beckmann, A.M.; Hislop, T.G.; Teh, C.Z.; Ashley, R.L.; et al. History of circumcision, medical conditions, and sexual activity and risk of penile cancer. J Natl Cancer Inst. 1993, 85, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Woythal, N.; Arsenic, R.; Kempkensteffen, C.; Miller, K.; Janssen, J.C.; Huang, K.; et al. Immunohistochemical validation of PSMA expression measured by 68 Ga-PSMA PET/CT in primary prostate cancer. J Nucl Med. 2018, 59, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Taha, T.; Meiri, D.; Talhamy, S.; Wollner, M.; Peer, A.; Bar-Sela, G. Cannabis impacts tumor response rate to nivolumab in patients with advanced malignancies. Oncologist. 2019, 24, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Xu, Y.; Zhu, L.; Zou, Y.; Kong, W.; Dong, B.; et al. Cannabinoid receptor 2 as a novel target for promotion of renal cell carcinoma prognosis and progression. J Cancer Res Clin Oncol. 2018, 144, 39–52. [Google Scholar] [CrossRef]
- Larrinaga, G.; Sanz, B.; Blanco, L.; Perez, I.; Candenas, M.L.; Pinto, F.M.; et al. Cannabinoid CB1 receptor is expressed in chromophobe renal cell carcinoma and renal oncocytoma. Clin Biochem 2013, 46, 638–641. [Google Scholar] [CrossRef] [PubMed]
- Larrinaga, G.; Varona, A.; Perez, I.; Sanz, B.; Ufalde, A.; Candenas, M.L.; et al. Expression of cannabinoid receptors in human kidney. Histol Histopathol. 2010, 25, 1133–1138. [Google Scholar]
- Choi, W.H.; Park HDo Baek, S.H.; Chu, J.P.; Kang, M.H.; Mi, Y.J. Cannabidiol induces cytotoxicity and cell death via apoptotic pathway in cancer cell lines. Biomol Ther. 2008, 16, 87–94. [Google Scholar]
- EAU Renal Cell Cancer Guidelines. 2021. Available online: https://uroweb.org/guidelines (accessed on 20 December 2022).
- Gurney, J.; Shaw, C.; Stanley, J.; Signal, V.; Sarfati, D. Cannabis exposure and risk of testicular cancer: A systematic review and meta-analysis. BMC Cancer. 2015, 15. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, R.C.; Allebeck, P.; Akre, O.; McGlynn, K.A.; Sidorchuk, A. Cannabis use and incidence of testicular cancer: a 42-year follow-up of Swedish men between 1970 and 2011. Cancer Epidemiol Biomarkers Prev. 2017, 26, 1644–1652. [Google Scholar] [CrossRef] [PubMed]
- Hogan, P.; Sharpe, M.; Smedley, H.; Sikora, K. Cannabinoids and hCG levels in patients with testicular cancer. Lancet. 1983, 1144. [Google Scholar] [CrossRef] [PubMed]
- Gandini, S.; Botteri, E.; Iodice, S.; Boniol, M.; Lowenfels, A.B.; Maisonneuve, P.; et al. Tobacco smoking and cancer: a meta-analysis. Int J Cancer. 2008, 122, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.; Budney, A.J.; Lynskey, M.T. The co-occurring use and misuse of cannabis and tobacco: A review. Addiction. 2012, 107, 1221–1233. [Google Scholar] [CrossRef] [PubMed]
- Dryburgh, L.M.; Bolan, N.S.; Grof, C.P.L.; Galettis, P.; Schneider, J.; Lucas, C.J.; et al. Cannabis contaminants: sources, distribution, human toxicity and pharmacologic effects. Br J Clin Pharmacol. 2018, 84, 2468–2476. [Google Scholar] [CrossRef]

{kind=link}
 |
   |
 |
 |
 |
This is an open access article under the terms of a license that permits non-commercial use, provided the original work is properly cited. © 2023 The Authors. Société Internationale d'Urologie Journal, published by the Société Internationale d'Urologie, Canada.
Share and Cite
Thomson, A.; McVey, A.; Timm, B.; Bolton, D. Urogenital Malignancy and Cannabis Use: A Narrative Review. Soc. Int. Urol. J. 2023, 4, 51-64. https://doi.org/10.48083/NDOJ8638
Thomson A, McVey A, Timm B, Bolton D. Urogenital Malignancy and Cannabis Use: A Narrative Review. Société Internationale d’Urologie Journal. 2023; 4(1):51-64. https://doi.org/10.48083/NDOJ8638
Chicago/Turabian StyleThomson, Alice, Aoife McVey, Brennan Timm, and Damien Bolton. 2023. "Urogenital Malignancy and Cannabis Use: A Narrative Review" Société Internationale d’Urologie Journal 4, no. 1: 51-64. https://doi.org/10.48083/NDOJ8638
APA StyleThomson, A., McVey, A., Timm, B., & Bolton, D. (2023). Urogenital Malignancy and Cannabis Use: A Narrative Review. Société Internationale d’Urologie Journal, 4(1), 51-64. https://doi.org/10.48083/NDOJ8638