Protocol for the RoboSling Trial: A Randomised Study Assessing Urinary Continence Following Robotic Radical Prostatectomy with or without an Intraoperative Retropubic Vascularised Fascial Sling (RoboSling)

 , ,
, ,
Abstract
1. Introduction
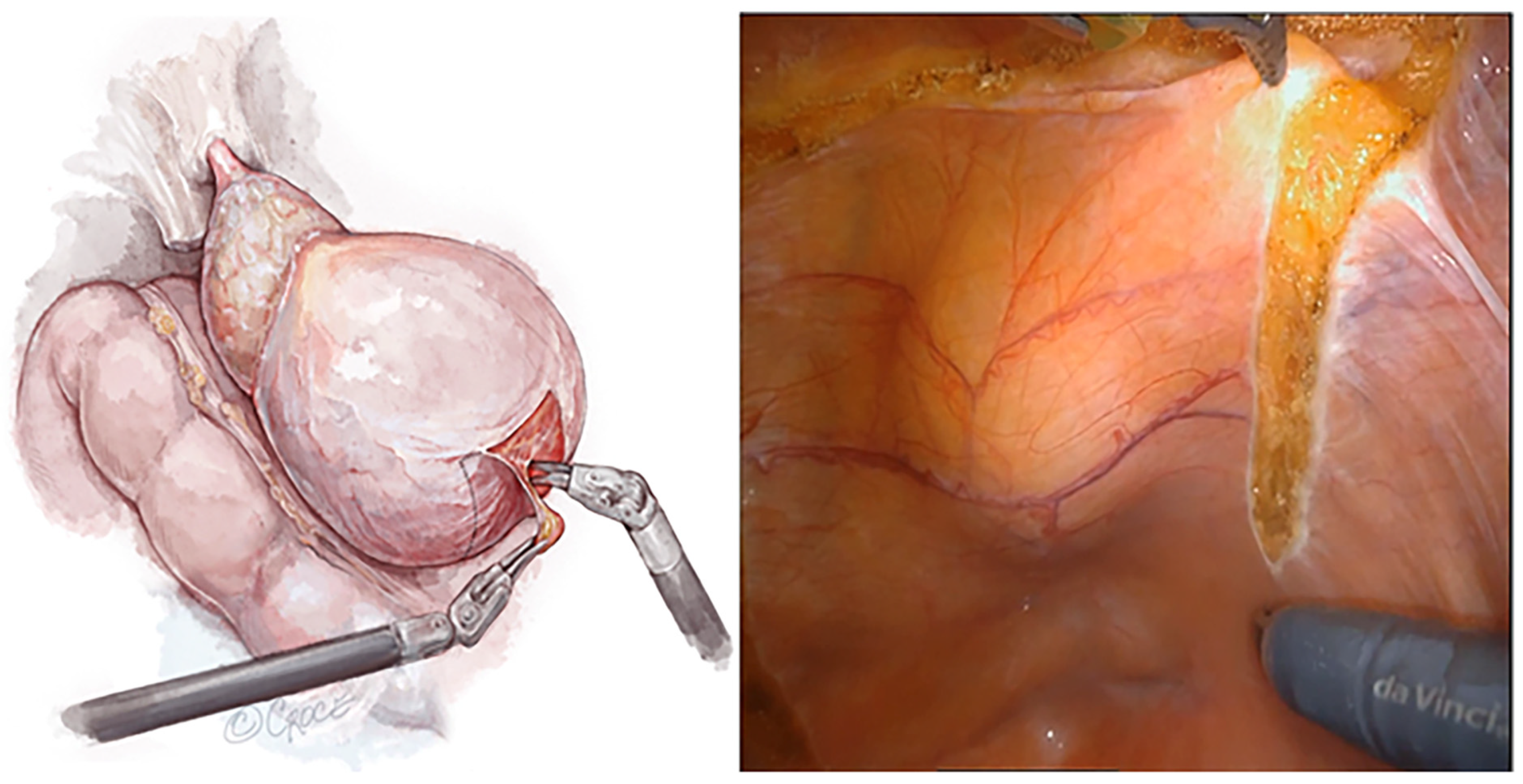
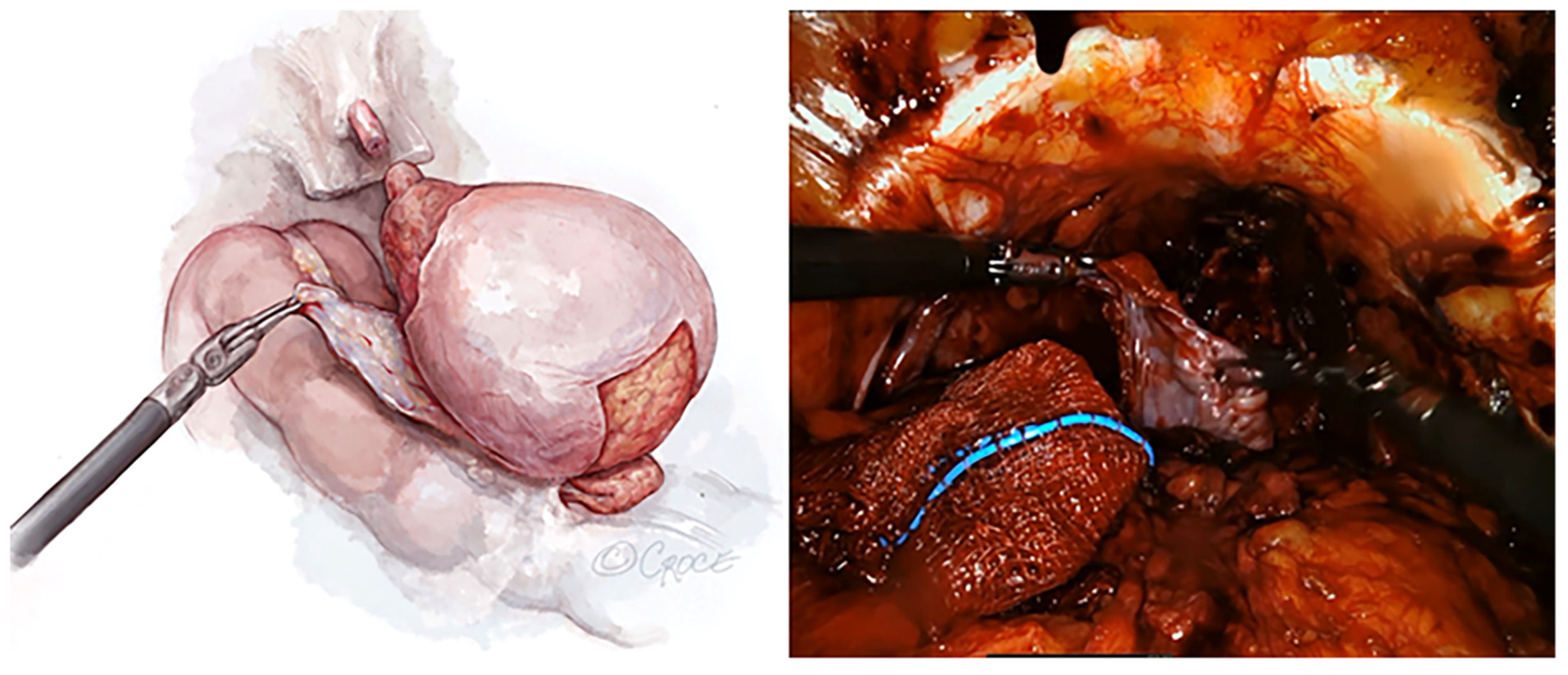
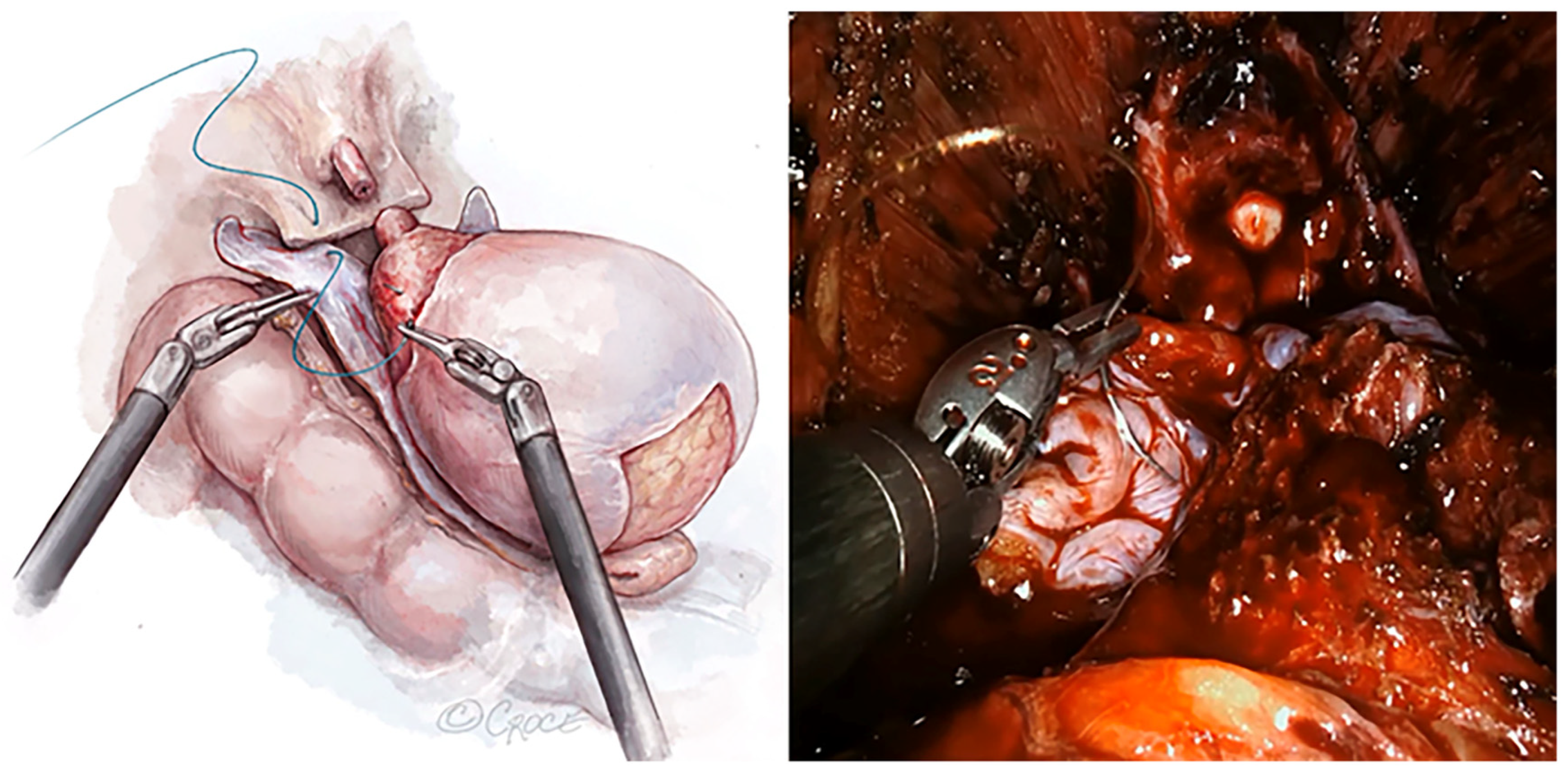
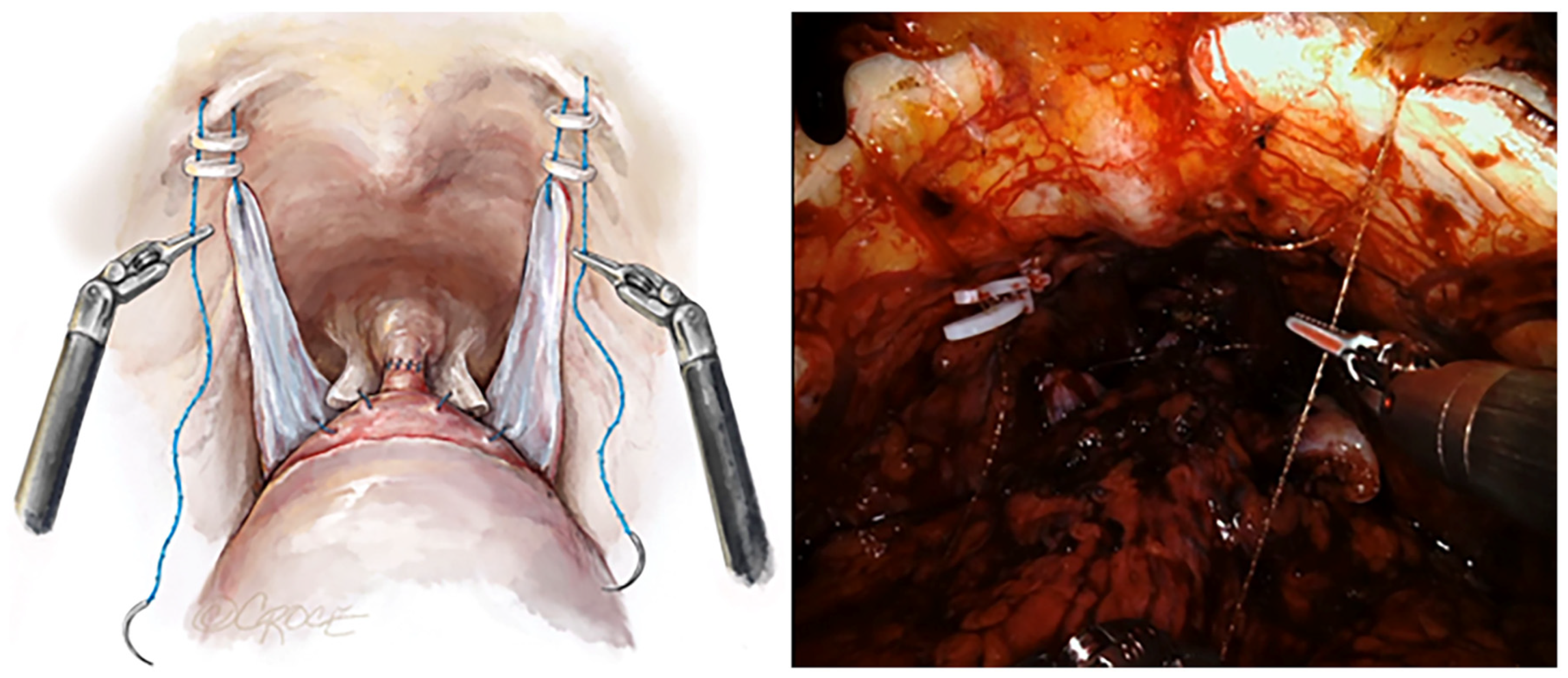
RoboSling Technique
2. Materials and Methods
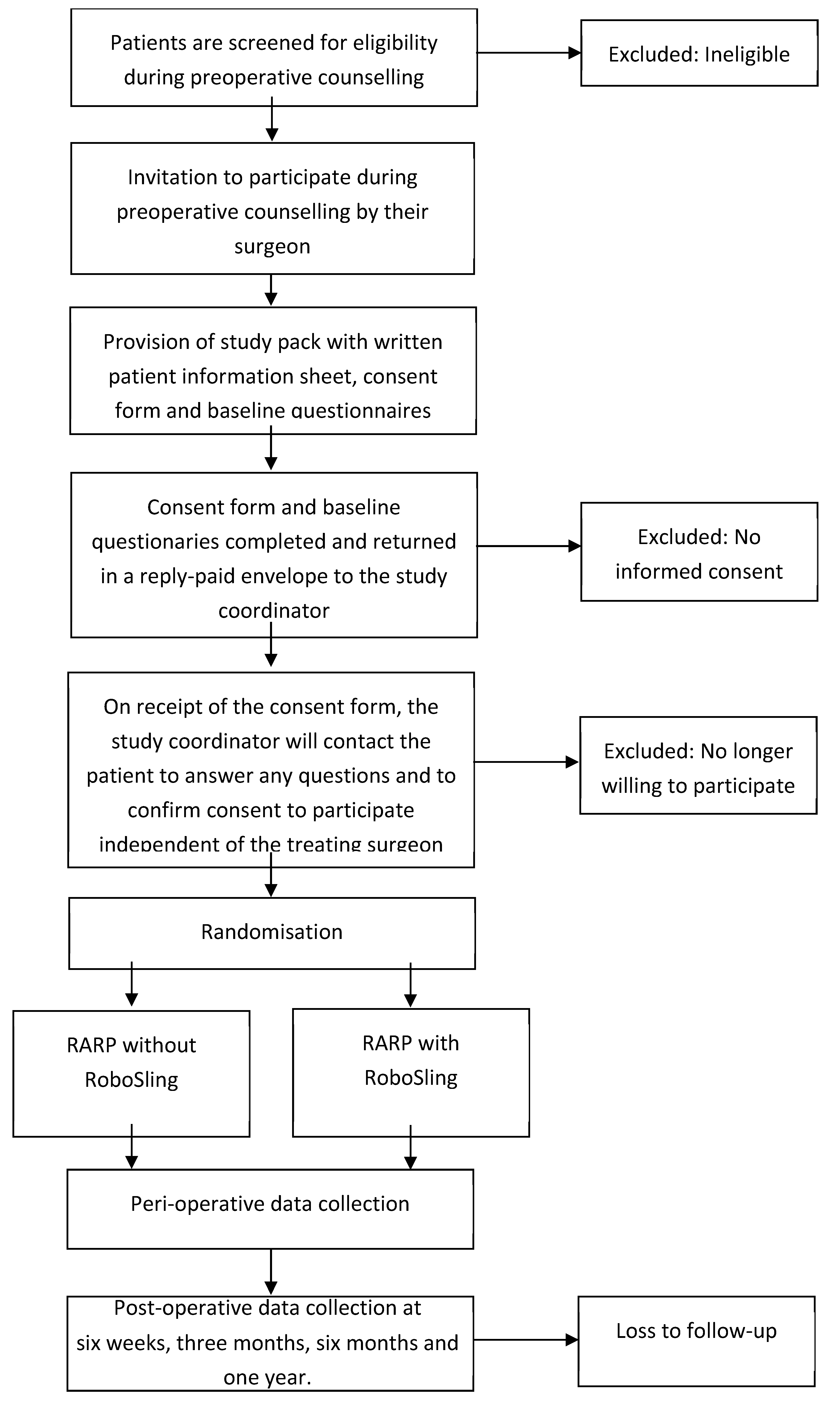
2.1. Study Design
2.2. Patient Recruitment
2.3. Intervention Randomisation
2.4. Sample Size Determination
2.5. Methods of Data Collection
- Urodynamics (to study bladder storage function, voiding function, and continence).
- Pelvic floor ultrasound (to assess pelvic floor contraction and urethral mobility and measure urethral sphincter length).
- Uroflow assessment (to assess bladder and sphincter function and to determine urine obstructions).
3. Results
3.1. Outcome Measures
3.2. Analysis Plan
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Australian Institute of Health and Welfare. Cancer Data in Australia [Internet]; Australian Institute of Health and Welfare: Canberra, Australia, 2022. Available online: https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia (accessed on 26 May 2023).
- Katz, G.; Rodriguez, R. Changes in continence and health-related quality of life after curative treatment and watchful waiting of prostate cancer. Urology 2007, 69, 1157–1160. [Google Scholar] [CrossRef]
- Ficarra, V.; Novara, G.; Artibani, W.; Cestari, A.; Galfano, A.; Graefen, M.; Guazzoni, G.; Guillonneau, B.; Menon, M.; Montorsi, F.; et al. Retropubic, laparoscopic, and robot-assisted radical prostatectomy: A systematic review and cumulative analysis of comparative studies. Eur. Urol. 2009, 55, 1037–1063. [Google Scholar] [CrossRef]
- Rocco, B.; Gregori, A.; Stener, S.; Santoro, L.; Bozzola, A.; Galli, S.; Knez, R.; Scieri, F.; Scaburri, A.; Gaboardi, F. Posterior reconstruction of the rhabdosphincter allows a rapid recovery of continence after transperitoneal videolaparoscopic radical prostatectomy. Eur. Urol. 2007, 51, 996–1003. [Google Scholar] [CrossRef]
- Zorn, K.C.; Wille, M.A.; Thong, A.E.; Katz, M.H.; Shikanov, S.A.; Razmaria, A.; Gofrit, O.N.; Zagaja, G.P.; Shalhav, A.L. Continued improvement of perioperative, pathological and continence outcomes during 700 robot-assisted radical prostatectomies. Can. J. Urol. 2009, 16, 4742–4749; discussion 4749. [Google Scholar]
- Patel, V.R.; Coelho, R.F.; Palmer, K.J.; Rocco, B. Periurethral suspension stitch during robot-assisted laparoscopic radical prostatec-tomy: Description of the technique and continence outcomes. Eur. Urol. 2009, 56, 472–478. [Google Scholar] [CrossRef]
- Cestari, A.; Ferrari, M.; Ghezzi, M.; Sangalli, M.; Zanoni, M.; Fabbri, F.; Sozzi, F.; Lolli, C.; Dell, V.; Rigatti, P. Retropubic Intracorporeal Placement of a Suburethral Autologous Sling During Ro-bot-Assisted Radical Prostatectomy to Improve Early Urinary Continence Recovery: Preliminary Data. J. Endourol. 2015, 29, 1379–1385. [Google Scholar] [CrossRef]
- Takenaka, A.; Tewari, A.K.; Leung, R.A.; Bigelow, K.; El-Tabey, N.; Murakami, G.; Fujisawa, M. Preservation of the puboprostatic collar and puboperineoplasty for early recovery of urinary continence after robotic prostatectomy: Anatomic basis and preliminary outcomes. Eur. Urol. 2007, 51, 433–440. [Google Scholar] [CrossRef]
- Ficarra, V.; Novara, G.; Rosen, R.C.; Artibani, W.; Carroll, P.R.; Costello, A.; Menon, M.; Montorsi, F.; Patel, V.R.; Stolzenburg, J.-U.; et al. Systematic review and meta-analysis of studies reporting urinary continence recovery after robot-assisted radical prostatectomy. Eur. Urol. 2012, 62, 405–417. [Google Scholar] [CrossRef]
- Nguyen, H.G.; Punnen, S.; Cowan, J.E.; Leapman, M.; Cary, C.; Welty, C.; Weinberg, V.; Cooperberg, M.R.; Meng, M.V.; Greene, K.L.; et al. A Randomized Study of Intraoperative Autologous Retropubic Urethral Sling on Urinary Control after Robotic Assisted Radical Prostatectomy. J. Urol. 2017, 197, 369–375. [Google Scholar] [CrossRef]
- Bahler, C.D.; Sundaram, C.P.; Kella, N.; Lucas, S.M.; Boger, M.A.; Gardner, T.A.; Koch, M.O. A Parallel Randomized Clinical Trial Examining the Return of Urinary Continence after Robot-Assisted Radical Prostatectomy with or without a Small Intestinal Submucosa Bladder Neck Sling. J. Urol. 2016, 196, 179–184. [Google Scholar] [CrossRef]
- Leslie, S.; Jackson, S.; Broe, M.; van Diepen, D.C.; Stanislaus, C.; Steffens, D.; McClintock, G.; Kim, S.; Jeffery, N.; Fallot, J.; et al. Improved early and late continence following robot-assisted radical prostatectomy with concurrent bladder neck fascial sling (RoboSling). BJUI Compass 2023, 4, 597–604. [Google Scholar] [CrossRef]
- Menon, M.; Muhletaler, F.; Campos, M.; Peabody, J.O. Assessment of early continence after reconstruction of the periprostatic tissues in patients undergoing computer assisted (robotic) prostatectomy: Results of a 2 group parallel randomized controlled trial. J. Urol. 2008, 180, 1018–1023. [Google Scholar] [CrossRef]
- Ahlering, T.E.; Gordon, A.; Morales, B.; Skarecky, D.W. Preserving continence during robotic prostatectomy. Curr. Urol. Rep. 2013, 14, 52–58. [Google Scholar] [CrossRef]
- Lee, S.R.; Kim, H.W.; Lee, J.W.; Jeong, W.J.; Rha, K.H.; Kim, J.H. Discrepancies in perception of urinary incontinence between patient and physician after robotic radical prostatectomy. Yonsei Med. J. 2010, 51, 883–887. [Google Scholar] [CrossRef]
- Kundu, S.D.; Roehl, K.A.; Eggener, S.E.; Antenor, J.A.; Han, M.; Catalona, W.J. Potency, continence and complications in 3477 con-secutive radical retropubic prostatectomies. J. Urol. 2004, 172, 2227–2231. [Google Scholar] [CrossRef]
- Coakley, F.V.; Eberhardt, S.; Kattan, M.W.; Wei, D.C.; Scardino, P.T.; Hricak, H. Urinary continence after radical retropubic prosta-tectomy: Relationship with membranous urethral length on preoperative endorectal magnetic resonance imaging. J. Urol. 2002, 168, 1032–1035. [Google Scholar] [CrossRef]
- Link, B.A.; Nelson, R.; Josephson, D.Y.; Yoshida, J.S.; Crocitto, L.E.; Kawachi, M.H.; Wilson, T.G. The impact of prostate gland weight in robot assisted laparoscopic radical prostatectomy. J. Urol. 2008, 180, 928–932. [Google Scholar] [CrossRef]
- Boczko, J.; Erturk, E.; Golijanin, D.; Madeb, R.; Patel, H.; Joseph, J.V. Impact of prostate size in robot-assisted radical prostatectomy. J. Endourol. 2007, 21, 184–188. [Google Scholar] [CrossRef]
- Chang, J.I.; Lam, V.; Patel, M.I. Preoperative Pelvic Floor Muscle Exercise and Postprostatectomy Incontinence: A Systematic Review and Meta-analysis. Eur. Urol. 2016, 69, 460–467. [Google Scholar] [CrossRef]
- Trinh, Q.-D.; Bjartell, A.; Freedland, S.J.; Hollenbeck, B.K.; Hu, J.C.; Shariat, S.F.; Sun, M.; Vickers, A.J. A systematic review of the volume–outcome relationship for radical prostatectomy. Eur. Urol. 2013, 64, 786–798. [Google Scholar] [CrossRef]
- Samadi, D.B.; Muntner, P.; Nabizada-Pace, F.; Brajtbord, J.S.; Carlucci, J.; Lavery, H.J. Improvements in robot-assisted prostatectomy: The effect of surgeon experience and technical changes on oncologic and functional outcomes. J. Endourol. 2010, 24, 1105–1110. [Google Scholar] [CrossRef] [PubMed]
- Yaxley, J.W.; Coughlin, G.D.; Chambers, S.K.; Occhipinti, S.; Samaratunga, H.; Zajdlewicz, L.; Dunglison, N.; Carter, R.; Williams, S.; Payton, D.J.; et al. Robot-assisted laparoscopic prostatectomy versus open radical retropubic prostatectomy: Early outcomes from a randomised controlled phase 3 study. Lancet 2016, 388, 1057–1066. [Google Scholar] [CrossRef] [PubMed]
- Coughlin, G.D.; Yaxley, J.W.; Chambers, S.K.; Occhipinti, S.; Samaratunga, H.; Zajdlewicz, L.; Teloken, P.; Dunglison, N.; Williams, S.; Lavin, M.F.; et al. Robot-assisted laparoscopic prostatectomy versus open radical retropubic prostatectomy: 24-month outcomes from a randomised controlled study. Lancet Oncol. 2018, 19, 1051–1060. [Google Scholar] [CrossRef] [PubMed]
- Stolzenburg, J.-U.; Holze, S.; Neuhaus, P.; Kyriazis, I.; Do, H.M.; Dietel, A.; Truss, M.C.; Grzella, C.I.; Teber, D.; Hohenfellner, M.; et al. Robotic-assisted Versus Laparoscopic Surgery: Outcomes from the First Multicentre, Randomised, Patient-blinded Controlled Trial in Radical Prostatectomy (LAP-01). Eur. Urol. 2021, 79, 750–759. [Google Scholar] [CrossRef]
- Stolzenburg, J.-U.; Holze, S.; Arthanareeswaran, V.-K.; Neuhaus, P.; Do, H.M.; Haney, C.M.; Dietel, A.; Truss, M.C.; Stützel, K.D.; Teber, D.; et al. Robotic-assisted Versus Laparoscopic Radical Prostatectomy: 12-month Outcomes of the Multicentre Randomised Controlled LAP-01 Trial. Eur. Urol. Focus 2022, 8, 1583–1590. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primary Endpoint |
| To determine if incorporating the RoboSling procedure with RARP improves early (three months) and late (one year) post-operative urinary continence compared to RARP alone. |
| Secondary Endpoints |
| To identify urinary functional parameters (using uroflow, urodynamics, and dynamic 3D pelvic floor ultrasound), which may differ between the RoboSling group and the control group. |
| To identify differences in perioperative complications. |
| To identify anatomic features on pre-op imaging (MRI scan/3D pelvic floor ultrasound scan), which may result in poorer post-operative functional outcome post RARP (prostate volume; pelvic volume; urethral length; BMI). |
To prospectively assess the following:
|
| Inclusion Criteria |
| Adult men aged 18 years and over |
| Undergoing prostatectomy for prostate cancer at RPA hospital |
| Clinically suitable for robotic prostatectomy |
| Cognitively able to provide written informed consent for participation |
| Elective procedure |
| Exclusion Criteria |
| The patient lacks the ability to consent for themselves |
| Patient or tumour factors precluding robotic surgery |
| The lack of available tissue behind the bladder to create the vascularised flap |
| Measurement | Timepoint | |||||
|---|---|---|---|---|---|---|
| Pre-Op | Peri-Op | Post-Operative | ||||
| Six W | Three M | Six M | One Y | |||
| Demographic and Clinical Factors | ||||||
| Age (years) | x | |||||
| Body Mass Index (BMI) | x | |||||
| American Society of Anaesthesiologists (ASA) Grade | x | |||||
| Prostate-specific antigen1 (PSA) level | x | x | x | x | x | |
| Multiparametric MRI (mpMRI)/CT | x | |||||
| Pelvic Cavity Index (PCI) | x | |||||
| Prostate Volume: Pelvic Cavity Index (PCI) ratio | x | |||||
| Tumour Characteristics | ||||||
| Clinical stage | x | |||||
| Biopsy Gleason Score | x | |||||
| Prostate Volume | x | |||||
| Procedure Details | ||||||
| Surgical access (robotic or open) | x | |||||
| Operative time/console time, minutes | x | |||||
| Conversions to non-robotic procedure, number | x | |||||
| Patient Reported Outcomes | ||||||
| International Index of erectile Function (IIEF) | x | x | x | x | x | |
| International Prostate Symptom Score (I-PSS) | x | x | ||||
| SF-36v2 Quality of Life | x | x | x | x | ||
| Decision Regret Scale | x | x | x | |||
| Expanded Prostate Cancer Index Composite (EPIC) | x | x | x | x | x | |
| International Consultation on Incontinence Questionnaire Urinary Incontinence (ICIQ-UI) | x | x | x | x | x | |
| Clinical (Functional) Outcomes | ||||||
| Pad weight and number/24 h | x | x | x | x | x | |
| Urodynamics assessment * | x | x | ||||
| Uro-flow/pelvic floor ultrasound assessment * | x | x | x | x | x | |
| Clinical (Operative) Outcomes | ||||||
| Complications, number | x | |||||
| Complications (Clavien–Dindo), classification I-V | x | |||||
| Blood loss, mL | x | |||||
| Transfusions, mL | x | |||||
| Numerical Pain Rating Scores (NPRS), score 0–10 | x | x | x | x | ||
| Length of hospital stay, days | ||||||
| Death: date, cause | x | x | x | x | x | |
| Pathology Outcomes | ||||||
| Weight of resected tissue | x | |||||
| Extracapsular extension | x | |||||
| Seminal vesical Invasion | x | |||||
| Lymph node involvement/yield | x | |||||
| Margin involvement | x | |||||
| Adjuvant treatment | x | |||||
| Economic Evaluation | ||||||
| Hospital discharge data | ||||||
| Work and care responsibilities | x | x | x | x | ||
| Assistance at home | x | x | x | |||
| Financial issues | x | x | x | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Virk, A.; Treacy, P.-J.; Zhong, W.; Jackson, S.R.; Ahmadi, N.; Jeffery, N.N.; Chan, L.; Sved, P.; Vasilaras, A.; Thanigasalam, R.; et al. Protocol for the RoboSling Trial: A Randomised Study Assessing Urinary Continence Following Robotic Radical Prostatectomy with or without an Intraoperative Retropubic Vascularised Fascial Sling (RoboSling). Soc. Int. Urol. J. 2024, 5, 148-159. https://doi.org/10.3390/siuj5020024
Virk A, Treacy P-J, Zhong W, Jackson SR, Ahmadi N, Jeffery NN, Chan L, Sved P, Vasilaras A, Thanigasalam R, et al. Protocol for the RoboSling Trial: A Randomised Study Assessing Urinary Continence Following Robotic Radical Prostatectomy with or without an Intraoperative Retropubic Vascularised Fascial Sling (RoboSling). Société Internationale d’Urologie Journal. 2024; 5(2):148-159. https://doi.org/10.3390/siuj5020024
Chicago/Turabian StyleVirk, Amandeep, Patrick-Julien Treacy, Wenjie Zhong, Stuart Robert Jackson, Nariman Ahmadi, Nicola Nadia Jeffery, Lewis Chan, Paul Sved, Arthur Vasilaras, Ruban Thanigasalam, and et al. 2024. "Protocol for the RoboSling Trial: A Randomised Study Assessing Urinary Continence Following Robotic Radical Prostatectomy with or without an Intraoperative Retropubic Vascularised Fascial Sling (RoboSling)" Société Internationale d’Urologie Journal 5, no. 2: 148-159. https://doi.org/10.3390/siuj5020024
APA StyleVirk, A., Treacy, P.-J., Zhong, W., Jackson, S. R., Ahmadi, N., Jeffery, N. N., Chan, L., Sved, P., Vasilaras, A., Thanigasalam, R., & Leslie, S. (2024). Protocol for the RoboSling Trial: A Randomised Study Assessing Urinary Continence Following Robotic Radical Prostatectomy with or without an Intraoperative Retropubic Vascularised Fascial Sling (RoboSling). Société Internationale d’Urologie Journal, 5(2), 148-159. https://doi.org/10.3390/siuj5020024