Comparison of the Changes in the Structure of the Transverse Arch of the Normal and Hallux Valgus Feet under Different Loading Positions

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Experimental Design and Set-Up
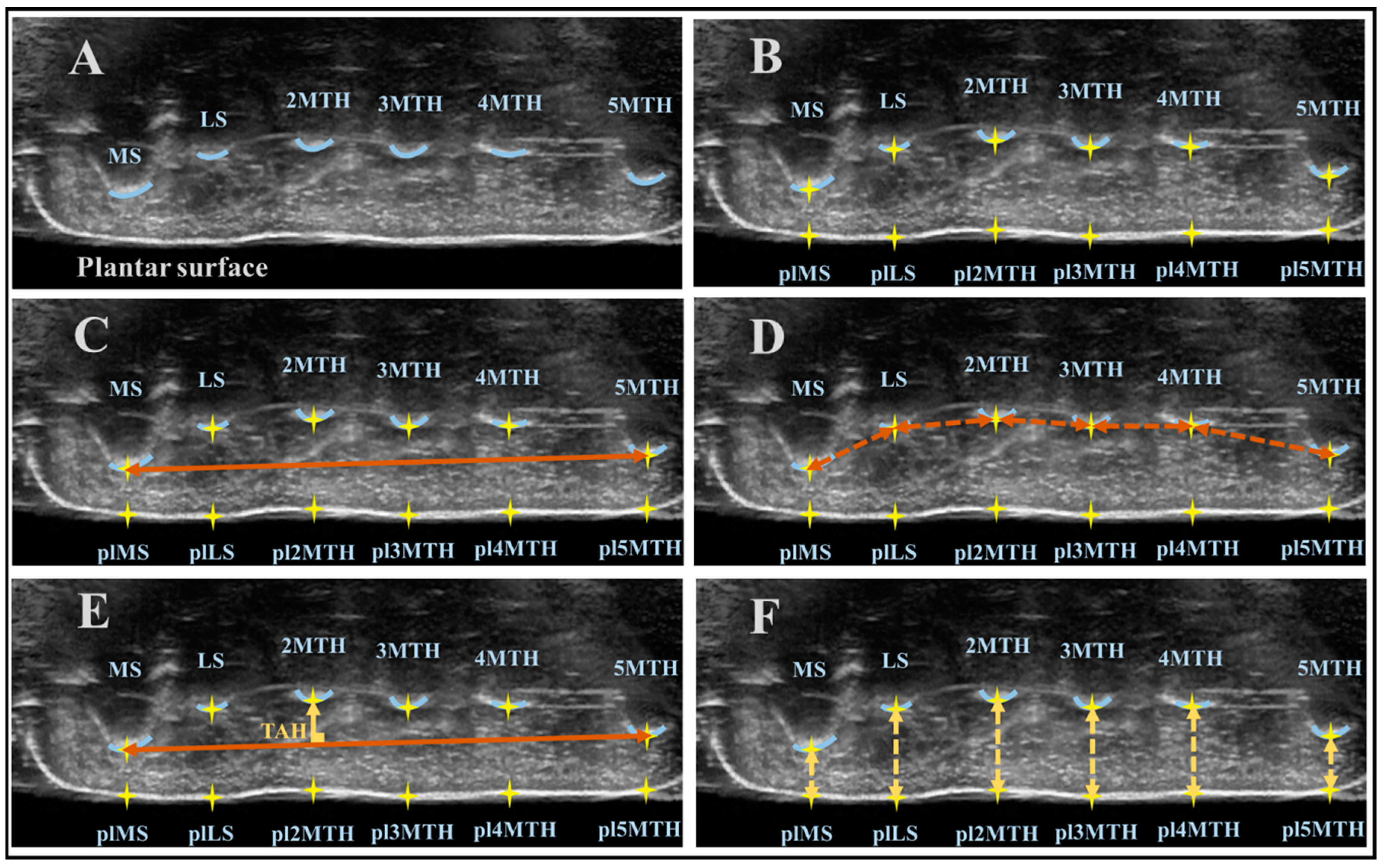
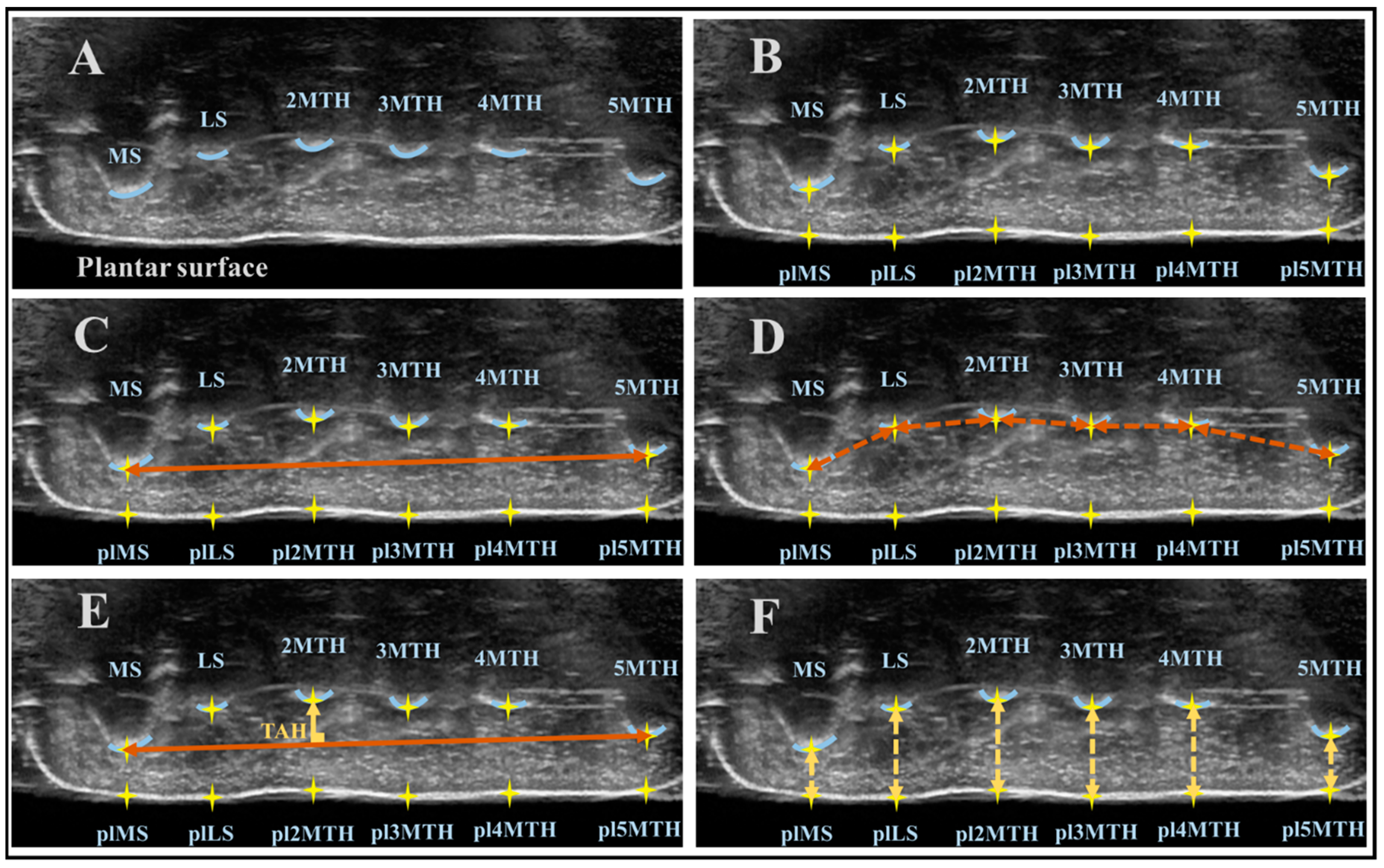
2.3. US Data Analysis
2.4. Statistical Analysis
3. Results
3.1. TAL
3.2. TAH
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Glasoe, W.M.; Nuckley, D.J.; Ludewig, P.M. Hallux valgus and the first metatarsal arch segment: A theoretical biomechanical perspective. Phys. Ther. 2010, 90, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Perera, A.M.; Mason, L.; Stephens, M.M. The pathogenesis of hallux valgus. J. Bone Joint Surg. 2011, 93, 1650–1661. [Google Scholar] [CrossRef] [PubMed]
- Menz, H.B.; Roddy, E.; Marshall, M.; Thomas, M.J.; Rathod, T.; Peat, G.M.; Croft, P.R. Epidemiology of shoe wearing patterns over time in older women: Associations with foot pain and hallux valgus. J. Gerontol. A Biol. Med. Sci. 2016, 71, 1682–1687. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, U.S.; Hillstrom, H.J.; Li, W.; Dufoury, A.B.; Kielyz, D.P.; Procter-Grayk, E.; Gagnony, M.M.; Hannanyz, M.T. Factors associated with hallux valgus in a population-based study of older women and men: The mobilize Boston study. Osteoarthr. Cartil. 2010, 18, 41–46. [Google Scholar] [CrossRef]
- Nix, S.E.; Vicenzino, B.T.; Collins, N.J.; Smith, M.D. Gait parameters associated with hallux valgus: A systematic review. J. Foot Ankle Res. 2013, 6, 9. [Google Scholar] [CrossRef] [PubMed]
- Kavlak, Y. The Relation of hallux valgus severity with foot function and balance in older men. Turk. J. Physiother. Rehabil. 2015, 26, 93–99. [Google Scholar] [CrossRef]
- Kokubo, T.; Hashimoto, T.; Suda, Y.; Waseda, A.; Ikezawa, H. Radiographic shape of foot with second metatarsophalangeal joint dislocation associated with hallux valgus. Foot Ankle Int. 2017, 38, 1374–1379. [Google Scholar] [CrossRef] [PubMed]
- Webster, J.; Murphy, D. Atlas of Orthoses and Assistive Devices, 5th ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 216–225. ISBN 9780323483230. [Google Scholar]
- Nakayama, Y.; Tashiro, Y.; Suzuki, Y.; Kajiwara, Y.; Zeidan, H.; Kawagoe, M.; Yokota, Y.; Sonoda, T.; Shimoura, K.; Tatsumi, M.; et al. Relationship between transverse arch height and foot muscles evaluated by ultrasound imaging device. J. Phys. Ther. Sci. 2018, 30, 630–635. [Google Scholar] [CrossRef] [Green Version]
- Perry, J. Gait Analysis: Normal and Pathological Function; SLACK Incorporated: Thorofare, NJ, USA, 1992; ISBN 9781556427664. [Google Scholar]
- Hing, W.W.; Rome, K.; Cameron, A.F.M. Reliability of measuring abductor hallucis muscle parameters using two different diagnosis ultrasound machines. J. Foot Ankle Res. 2009, 2, 33. [Google Scholar] [CrossRef]
- Nwawka, K.; Endo, Y. Ultrasound-guided interventions in the midfoot and forefoot. Semin. Musculoskelet. Radiol. 2016, 20, 214–223. [Google Scholar]
- Crofts, G.; Angin, S.; Mickle, K.J.; Hill, S.; Nester, C.J. Reliability of ultrasound for measurement of selected foot structures. Gait Posture 2014, 39, 35–39. [Google Scholar] [CrossRef]
- Matsubara, K.; Matsushita, T.; Tashiro, Y.; Tasaka, S.; Sonoda, T.; Nakayama, Y.; Yokota, Y.; Suzuki, Y.; Kawagoe, M.; Aoyama, T. Repeatability and agreement of ultrasonography with computed tomography for evaluating forefoot structure in the coronal plane. J. Foot Ankle Res. 2017, 10, 17. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, A.; Kato, K.; Fukuda, A.; Nakazora, S.; Yamada, T.; Uchida, A.; Sudo, A. Prevalence of hallux valgus and risk factors among Japanese community dwellers. J. Orthop. Sci. 2014, 19, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, K.; Tasaka, S.; Fukumoto, T.; Nishiguchi, S.; Fukutani, N.; Tashiro, Y.; Shirooka, H.; Nozaki, Y.; Hirata, H.; Yamaguchi, M.; et al. Weak TGS correlates with hallux valgus in 10-12 year old girls: A cross-sectional study. Clin. Res. Foot Ankle 2016, 4, 189. [Google Scholar] [CrossRef]
- Kilmartin, T.E. The Orthotic Treatment of Juvenile Hallux Valgus. Ph.D. Thesis, University of Nottingham, Nottingham, UK, 1994. [Google Scholar]
- Uritani, D.; Fukumoto, T.; Matsumoto, D.; Shima, M. Associations between toe grip strength and hallux valgus, toe curl ability, and foot arch height in Japanese adults aged 20 to 79 years: A cross-sectional study. J. Foot Ankle Res. 2015, 8, 18. [Google Scholar] [CrossRef] [PubMed]
- Matsushita, T.; Tashiro, Y.; Suzuki, Y.; Tasaka, S.; Matsubara, K.; Kawagoe, M.; Yokota, U.; Sonoda, T.; Nakayama, Y.; Fukumoto, T.; et al. Association between height of the forefoot transverse arch and kinetics or kinematics of ankle joint during gait. Clin. Res. Foot Ankle 2017, 5, 227. [Google Scholar] [CrossRef]
- Abdalbary, S.A.; Elshaarawy, E.A.A.; Khalid, B.E.A. Tensile properties of the deep transverse metatarsal ligament in hallux valgus: A CONSORT-compliant article. Medicine 2016, 95, 1–5. [Google Scholar] [CrossRef]
- Kim, Y.; Kim, J.S.; Young, K.W.; Naraghi, R.; Cho, H.K.; Lee, S.Y. A new measure of tibial sesamoid position in hallux valgus in relation to the coronal rotation of the first metatarsal in CT scans. Foot Ankle Int. 2015, 36, 944–952. [Google Scholar] [CrossRef]
- Gu, Y.D.; Rong, M.; Li, Z.Y.; Lake, M.J.; Ruan, G.Q. Finite element analysis of deep transverse metatarsal ligaments mechanical response during landing. Adv. Mat. Res. 2012, 472, 2558–2561. [Google Scholar] [CrossRef]
- Wang, B.; Guss, A.; Chalayon, O.; Bachus, K.N.; Barg, A.; Saltzman, C.L. Deep transverse metatarsal ligament and static stability of lesser metatarsophalangeal joints: A cadaveric study. Foot Ankle Int. 2015, 36, 573–578. [Google Scholar] [CrossRef]
- Kelly, L.A.; Cresswell, A.G.; Racinais, S.; Whiteley, R.; Lichtwark, G. Intrinsic foot muscles have the capacity to control deformation of the longitudinal arch. J. R. Soc. Interface 2014, 11, 20131188. [Google Scholar] [CrossRef] [PubMed]
- Ker, R.F.; Bennett, M.B.; Bibby, S.R.; Kester, R.C.; Alexander, R. McN. The spring in the arch of the foot. Nature 1987, 325, 147–149. [Google Scholar] [CrossRef] [PubMed]
- Erdemir, A.; Hamel, A.J.; Fauth, A.R.; Piazza, S.J.; Sharkey, N.A. Dynamic loading of the plantar aponeurosis in walking. J. Bone Joint Surg. 2004, 86, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Cameron, A.F.M.; Rome, K.; Hing, W.A. Ultrasound evaluation of the abductor hallucis muscle: Reliability study. J. Foot Ankle Res. 2008, 1, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mickle, K.J.; Nester, C.J. Size of the Abductor Hallucis Muscle in Older Women with Hallux Valgus. J. Foot Ankle Res. 2014, 7 (Suppl. 1), A57. [Google Scholar] [CrossRef]
- Glasoe, W. Treatment of progressive first metatarsophalangeal hallux valgus deformity: A biomechanically based muscle-strengthening approach. J. Orthop. Sports Phys. Ther. 2016, 46, 596–606. [Google Scholar] [CrossRef] [PubMed]
- Kelly, L.A.; Kuitunen, S.; Racinais, S.; Cresswell, A.G. Recruitment of the plantar intrinsic foot muscles with increasing postural demand. Clin. Biomech. 2012, 27, 46–51. [Google Scholar] [CrossRef]
- Caravaggi, P.; Pataky, T.; Gunther, M.; Savage, R.; Crompton, R. Dynamics of longitudinal arch support in relation to walking speed: Contribution of the plantar aponeurosis. J. Anat. 2010, 217, 254–261. [Google Scholar] [CrossRef]
- Bates, K.T.; Collins, D.; Savage, R.; McClymont, J.; Webster, E.; Pataky, T.C.; D’Aout, C.; Sellers, W.E.; Bennett, M.R.; Crompton, R.H. The evolution of compliance in the human lateral mid-foot. Proc. Biol. Sci. 2013, 280, 1–7. [Google Scholar] [CrossRef]
- Geng, X.; Zhang, C.; Ma, X.; Wang, X.; Huang, J.; Xu, J.; Wang, C. Lateral sesamoid position relative to the second metatarsal in feet with and without hallux valgus: A prospective study. J. Foot Ankle Surg. 2016, 55, 136–139. [Google Scholar] [CrossRef]
- Schneider, W. Distal soft tissue procedure in hallux valgus surgery: Biomechanical background and technique. Int. Orthop. 2013, 37, 1669–1675. [Google Scholar] [CrossRef] [PubMed]
- Katsui, R.; Samoto, N.; Taniguchi, A.; Akahane, M.; Isomoto, S.; Sugimoto, K.; Tanaka, Y. Relationship between displacement and degenerative changes of the sesamoids in hallux valgus. Foot Ankle Int. 2016, 37, 1303–1309. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W.C.; Sugiarto, T.; Chen, J.W.; Lin, Y.J. The Design and Application of Simplified Insole-Based Prototypes with Plantar Pressure Measurement for Fast Screening of Flat-Foot. Sensors 2018, 18, 3617. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Without-HV (n = 260) | With-HV (n = 118) | p-Value | |
|---|---|---|---|
| HV Angle (°) | 9.4 ± 5.0 | 29.6 ± 9.4 | <0.0001 * |
| Age (years) | 68.9 ± 9.3 | 69.6 ± 8.7 | 0.454 |
| Height (cm) | 153.7 ± 6.0 | 154.7 ± 6.0 | 0.146 |
| Weight (kg) | 52.8 ± 10.2 | 51.5 ± 7.7 | 0.161 |
| Without-HV (n = 260) | With-HV (n = 118) | |||||
|---|---|---|---|---|---|---|
| Sitting | Standing | 90% W.S. | Sitting | Standing | 90% W.S. | |
| TAL (mm) | 67.8 ± 3.9 | 69.2 ± 4.4 † | 69.8 ± 4.4 † | 69.5 ± 4.0 § | 71.4 ± 4.2 §* | 71.4 ± 4.2 §* |
| MS~LS Length (mm) | 12.2 ± 1.8 | 12.6 ± 2.1 | 12.6 ± 2.1 | 12.1 ± 2.0 | 12.2 ± 1.8 | 12.3 ± 2.0 |
| LS~2MTH Length (mm) | 14.0 ± 2.4 | 14.0 ± 2.6 | 14.3 ± 2.5 | 14.4 ± 2.7 | 14.9 § ± 2.8 | 14.6 ± 2.5 |
| 2~3MTH Length (mm) | 12.7 ± 1.7 | 13.2 ± 1.9 † | 13.2 ± 1.9 † | 13.6 ± 1.7 § | 14.3 ± 2.2 §* | 14.4 ± 1.9 §* |
| 3~4MTH Length (mm) | 13.3 ± 1.8 | 13.8 ± 1.9 † | 13.8 ± 2.1 † | 13.9 ± 1.6 § | 14.1 ± 2.0 | 14.2 ± 2.2 |
| 4~5MTH Length (mm) | 16.6 ± 2.1 | 16.8 ± 2.2 | 17.0 ± 2.0 | 16.6 ± 1.9 | 17.2 ± 2.2 | 17.3 ± 2.1 * |
| Without-HV (n = 260) | With-HV (n = 118) | |||||
|---|---|---|---|---|---|---|
| Sitting | Standing | 90% W.S. | Sitting | Standing | 90% W.S. | |
| TAH (mm) | 4.0 ± 2.4 | 4.0 ± 2.4 | 3.9 ± 2.4 | 4.4 ± 2.5 | 4.3 ± 2.5 | 3.9 ± 2.3 |
| TAH Ratio (%) | 6.0 ± 3.5 | 5.8 ± 3.6 | 5.6 ± 3.4 | 6.4 ± 3.6 | 6.0 ± 3.5 | 5.5 ± 3.4 |
| MS Height (mm) | 6.3 ± 1.4 | 6.0 ± 1.2 † | 6.0 ± 1.2 | 5.9 ± 1.2 § | 5.6 ± 1.2 § | 5.9 ± 1.3 |
| LS Height (mm) | 8.1 ± 1.4 | 8.6 ± 1.4 † | 8.6 ± 1.5 † | 9.0 ± 1.5 § | 9.3 ± 1.6 § | 9.6 ± 1.7 §* |
| 2MTH Height (mm) | 10.1 ± 2.3 | 10.1 ± 2.3 | 10.0 ± 2.2 | 10.2 ± 2.3 | 10.1 ± 2.2 | 9.9 ± 2.2 |
| 3MTH Height (mm) | 9.0 ± 1.8 | 9.1 ± 1.6 | 9.1 ± 1.6 | 9.0 ± 1.7 | 8.9 ± 1.6 | 8.9 ± 1.7 |
| 4MTH Height (mm) | 8.4 ± 1.4 | 8.5 ± 1.4 | 8.7 ± 1.4 † | 8.4 ± 1.5 | 8.4 ± 1.5 | 8.5 ± 1.5 |
| 5MTH Height (mm) | 6.7 ± 1.2 | 6.4 ± 1.1 † | 6.4 ± 1.2 † | 6.8 ± 1.2 | 6.3 ± 1.2* | 6.3 ± 1.3 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeidan, H.; Suzuki, Y.; Kajiwara, Y.; Nakai, K.; Shimoura, K.; Yoshimi, S.; Tatsumi, M.; Nishida, Y.; Bito, T.; Aoyama, T. Comparison of the Changes in the Structure of the Transverse Arch of the Normal and Hallux Valgus Feet under Different Loading Positions. Appl. Syst. Innov. 2019, 2, 3. https://doi.org/10.3390/asi2010003
Zeidan H, Suzuki Y, Kajiwara Y, Nakai K, Shimoura K, Yoshimi S, Tatsumi M, Nishida Y, Bito T, Aoyama T. Comparison of the Changes in the Structure of the Transverse Arch of the Normal and Hallux Valgus Feet under Different Loading Positions. Applied System Innovation. 2019; 2(1):3. https://doi.org/10.3390/asi2010003
Chicago/Turabian StyleZeidan, Hala, Yusuke Suzuki, Yuu Kajiwara, Kengo Nakai, Kanako Shimoura, Soyoka Yoshimi, Masataka Tatsumi, Yuichi Nishida, Tsubasa Bito, and Tomoki Aoyama. 2019. "Comparison of the Changes in the Structure of the Transverse Arch of the Normal and Hallux Valgus Feet under Different Loading Positions" Applied System Innovation 2, no. 1: 3. https://doi.org/10.3390/asi2010003
APA StyleZeidan, H., Suzuki, Y., Kajiwara, Y., Nakai, K., Shimoura, K., Yoshimi, S., Tatsumi, M., Nishida, Y., Bito, T., & Aoyama, T. (2019). Comparison of the Changes in the Structure of the Transverse Arch of the Normal and Hallux Valgus Feet under Different Loading Positions. Applied System Innovation, 2(1), 3. https://doi.org/10.3390/asi2010003