Exploring the Health Information Management System of Kuwait: Lessons and Opportunities


Abstract
:1. Introduction
- Evaluate the existing condition of medical records in Kuwait’s healthcare centers;
- Establish whether medical records policies, procedures, and filing systems have been appropriately implemented and followed;
- Assess the disparity of the medical record system among the hospitals being studied;
- Assess the level of top management support for the management of medical records.
2. Materials and Methods
2.1. Study Population
2.2. Data Collection Instrument
2.3. Conducting the Survey
- Delays in sending the original invitations from the health district headquarters to targeted hospitals.
- Rejection to participate in the study by certain sites without receiving the original invitations.
- Delays in returning the completed surveys, which were self-administered by the respondents.
- The process of data collection was interrupted for four months due to the government shutdown in Kuwait during the peak of the coronavirus disease (COVID-19) pandemic (February–June 2020).
2.4. Statistical Analysis
3. Results
3.1. Response Rate
3.2. Demographics of the Survey Participants
3.3. Charectaristics of the Medical Records Management System
3.4. Policies and Procedures of the Medical Records Management Department
3.5. Storage, Retention, and Disposition of the Medical Records
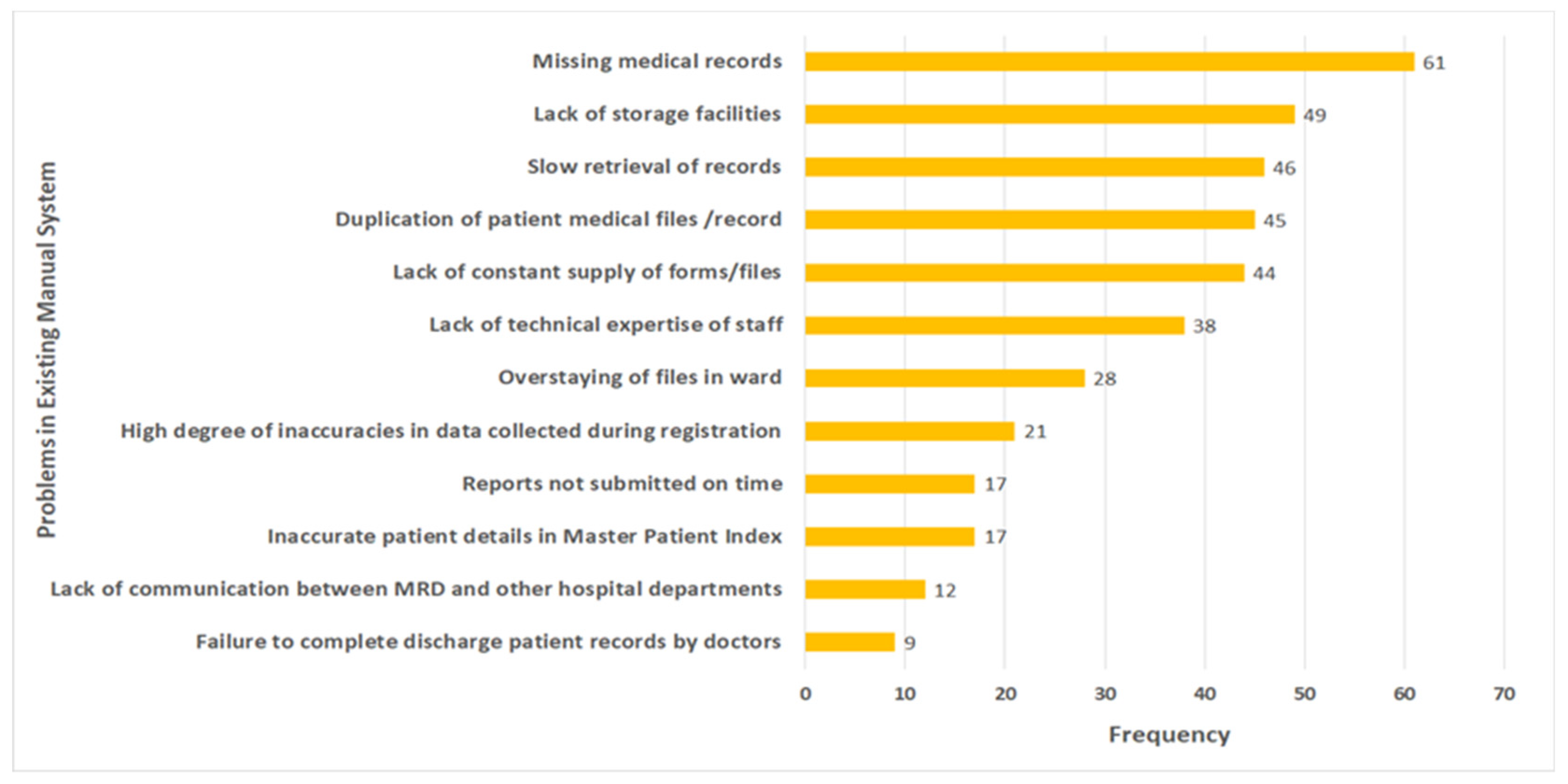
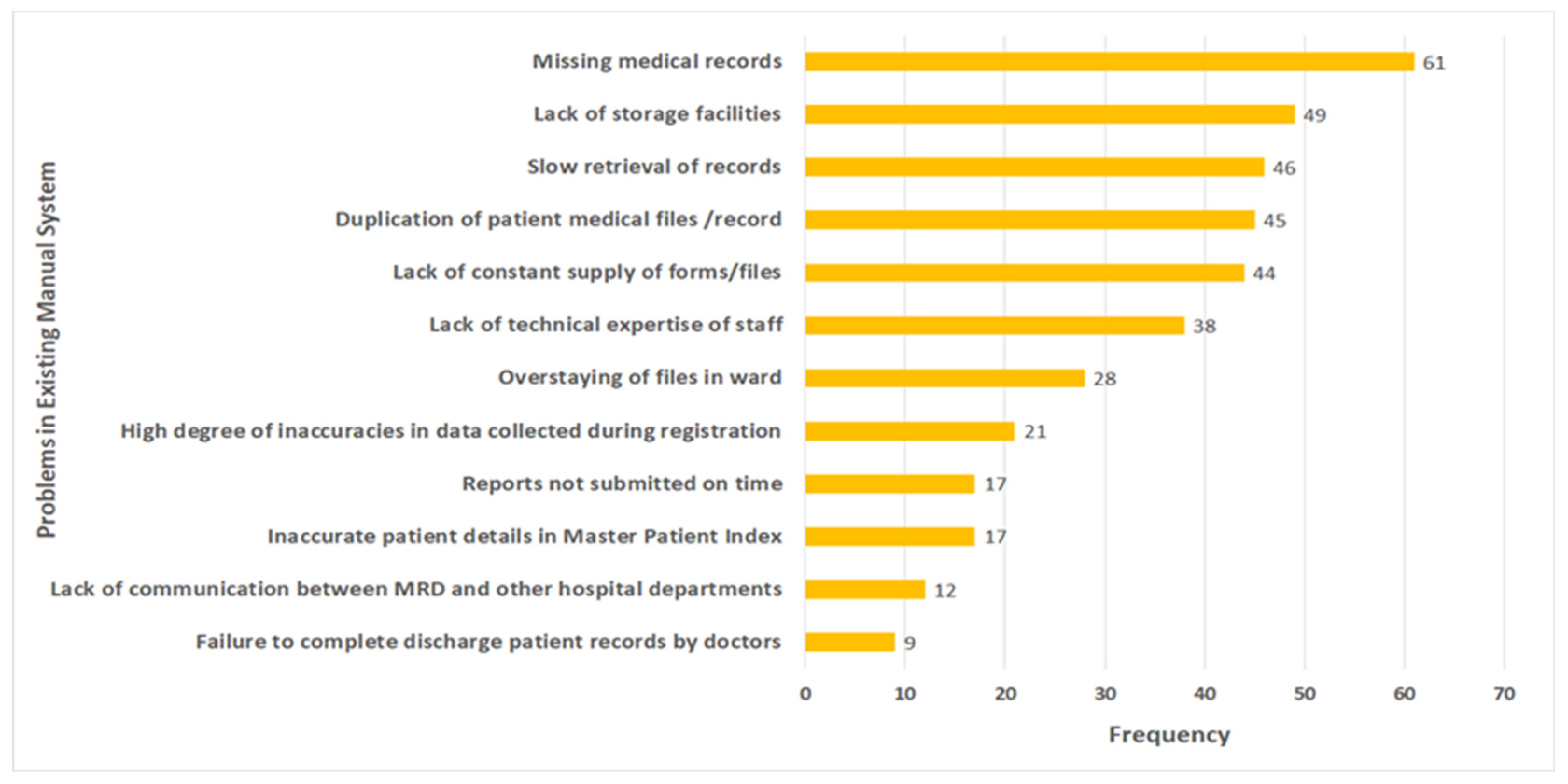
3.6. Problems in the Existing Medical Records Management Systems
3.7. Correlation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mathioudakis, A.; Rousalova, I.; Gagnat, A.A.; Saad, N.; Hardavella, G. How to keep good clinical records. Breathe 2016, 12, 369–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, J. Medical records and issues in negligence. Indian J. Urol. 2009, 25, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Gillum, R.F. From Papyrus to the Electronic Tablet: A Brief History of the Clinical Medical Record with Lessons for the Digital Age. Am. J. Med. 2013, 126, 853–857. [Google Scholar] [CrossRef] [PubMed]
- Abdelrahman, W.; Abdelmageed, A. Medical record keeping: Clarity, accuracy, and timeliness are essential. BMJ 2014, 348, f7716. [Google Scholar] [CrossRef]
- McFall, W.J., Jr.; Bader, J.D.; Rozier, R.G.; Ramsey, D. Presence of Periodontal Data in Patient Records of General Practitioners. J. Periodontol. 1988, 59, 445–449. [Google Scholar] [CrossRef]
- Brown, L.F.; Keily, P.A.; Spencer, A.J. Hygienist employment and the presence of periodontal notations in general dental practice patient records. Aust. Dent. J. 1994, 39, 45–49. [Google Scholar] [CrossRef]
- WHO. Everybody Business—Strengthening Health Systems to Improve Health Outcomes: WHO’s Framework for Action; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Mossialos, E.; Cheatley, J.; Reka, H.; Alsabah, A.; Patel, N. Kuwait Health System Review; London School of Economics and Political Science: London, UK, 2018. [Google Scholar]
- Chun, S.; Salman, A. Policy Paper for the Health Pillar: Overview of Gaps, Challenges, and Way Forward in Kuwait National Development Plan 2015–2020; Kuwait Public Policy Center, General Secretariat of the Supreme Council for Planning and Development: Kuwait City, Kuwait, 2019.
- Medical Records Working Party. Medical Records in Kuwait; Ministry of Public Health: Kuwait City, Kuwait, 1985.
- Mogli, G.D. Medical Records Role in Healthcare Delivery in 21st Century. Acta Inform. Med. 2009, 17, 209–212. [Google Scholar]
- Salman, A.; Al-Hemoud, A.; Fakhraldeen, S.; Al-Nashmi, M.; AlFadhli, S.; Chun, S. Research and Development as a Moderating Variable for Sustainable Economic Performance: The Asian, European, and Kuwaiti Models. Sustainability 2020, 12, 7525. [Google Scholar] [CrossRef]
- Salman, A.; Fakhraldeen, S.; Chun, S.; Jamil, K.; Gasana, J.; Al-Hunayan, A. Enhancing Research and Development in the Health Sciences as a Strategy to Establish a Knowledge-Based Economy in the State of Kuwait: A Call for Action. Healthcare 2020, 8, 264. [Google Scholar] [CrossRef]
- National Sustainable Development Goals Implementation Committee in Kuwait. Kuwait Voluntary National Review 2019: Report on the Implementation of the 2030 Agenda to the UN High-Level Political Forum on Sustainable Development; General Secretariat of the Supreme Council for Planning and Development: Kuwait City, Kuwait, 2019.
- Salman, A.; Tolma, E.; Chun, S.; Sigodo, K.; Al-Hunayan, A. Health Promotion Programs to Reduce Noncommunicable Diseases: A Call for Action in Kuwait. Healthcare 2020, 8, 251. [Google Scholar] [CrossRef]
- Chun, S.; Salman, A. Research Agenda for the Health Pillar; Kuwait Public Policy Center, General Secretariat of the Supreme Council for Planning and Development: Kuwait City, Kuwait, 2019. [CrossRef]
- Chun, S.; Salman, A. White Paper for the Health Pillar National Health Policy Framework: Ensuring Healthy Lives and Wellbeing; Kuwait Public Policy Center, General Secretariat of the Supreme Council for Planning and Development: Kuwait City, Kuwait, 2019. [CrossRef]
- Almutairi, B. A Strategic Roadmap for Achieving the Potential Benefits of Electronic Health Record System in the State of Kuwait. Ph.D. Thesis, University College London, London, UK, 2011. [Google Scholar]
- Al-Jafar, E. Exploring patient satisfaction before and after electronic health record (EHR) implementation: The Kuwait experience. Perspect. Health Inf. Manag. 2013, 10, 1c. [Google Scholar] [PubMed]
- Johar, S.; Patagundi, B. Analysis of Health Record Management System in Private Hospitals. Ph.D. Thesis, Cambridge Institute of Technology, Ranchi, India, 2021. [Google Scholar]
- Ajlouni, M. Assessment of Medical Records Services at Ministry of Health Hospitals in Jordan; Abt Associates Inc.: Bethesda, MD, USA, 2006. [Google Scholar]
- Ahmed, H.A.A.; El-Salami, R.M.; Ayad, K.M.; El-Deeb, A.E.-A.F. Assessment of Medical Records Documentation in Secondary Health Care Facilities in Kafr El-Sheikh and El-Mahalla El-Kubra Cities. Med. J. Cairo Univ. 2019, 87, 183–194. [Google Scholar]
- Moghaddasi, H.; Hosseini, A.; Sheikhtaheri, A. A new model for the organizational structure of medical record departments in hospitals in Iran. Perspect. Health Inf. Manag. 2006, 3, 4. [Google Scholar]
- Hajavi, A.; Haqani, H.; Akhlaqi, F.; Pur, U.M. Evaluating the Performance of the Medical Records Departments of Mashhad medical University teaching hospital (1381). J. Health Adm. 2005, 7, 7–13. [Google Scholar]
- Ngidi, T. Management of Medical Records: A Study at Princes Marina Hospital, Gaborone, Botswana. Master’s Thesis, University of Botswana, Gaborone, Botswana, 2016. [Google Scholar]
- Alhuwail, D. Understanding health information management practices in public hospitals in Kuwait. Health Inf. Manag. J. 2019, 49, 127–136. [Google Scholar] [CrossRef]
- Fricker, R.D.J.; Schonlau, M. Advantages and Disadvantages of Internet Research Surveys: Evidence from the Literature; SAGE Internet Research Methods: London, UK, 2012. [Google Scholar]
- Weber, A.S.; Turjoman, R.; Shaheen, Y.; Al Sayyed, F.; Hwang, M.J.; Malick, F. Systematic thematic review of e-health research in the Gulf Cooperation Council (Arabian Gulf): Bahrain, Kuwait, Oman, Qatar, Saudi Arabia and United Arab Emirates. J. Telemed. Telecare 2016, 23, 452–459. [Google Scholar] [CrossRef]
- LaTour, K.M.; Maki, S.E. Health Information Management: Concepts, Principles, and Practice, 5th ed.; American Health Information Management Association: Chicago, IL, USA, 2010. [Google Scholar]
- Abdelhak, M.; Hanken, M.A. Health Information, 5th ed.; Elsevier: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Kruk, M.E.; Freedman, L.P. Assessing health system performance in developing countries: A review of the literature. Health Policy 2008, 85, 263–276. [Google Scholar] [CrossRef]
- Gupta, A.; Jain, K.; Bhoi, S. Evaluation of patients record and its implications in the management of trauma patients. J. Emerg. Trauma Shock 2020, 13, 257. [Google Scholar] [CrossRef]
- Tavakoli, N.; Jahanbakhsh, M. Investigation of retention and destruction process of medical records in the hospitals and codifying appropriate guidelines. J. Educ. Health Promot. 2013, 2, 17. [Google Scholar] [CrossRef]
- Al-Shorbaji, N. Improving Healthcare Access through Digital Health: The Use of Information and Communication Technologies. In Healthcare Access; IntechOpen: London, UK, 2021. [Google Scholar]
- Salman, A.; Sigodo, K.; Al-Ghadban, F.; Al-Lahou, B.; Alnashmi, M.; Hermassi, S.; Chun, S. Effects of COVID-19 Lockdown on Physical Activity and Dietary Behaviors in Kuwait: A Cross-Sectional Study. Nutrients 2021, 13, 2252. [Google Scholar] [CrossRef]
- Salman, A.; Al-Ghadban, F.; Sigodo, K.; Taher, A.; Chun, S. The Psychological and Social Impacts of Curfew during the COVID-19 Outbreak in Kuwait: A Cross-Sectional Study. Sustainability 2021, 13, 8464. [Google Scholar] [CrossRef]
- McAlearney, A.S.; Robbins, J.; Kowalczyk, N.; Chisolm, D.J.; Song, P.H. The role of cognitive and learning theories in supporting successful EHR system implementation training: A qualitative study. Med. Care Res. Rev. 2012, 69, 294–315. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.G.; Lyle, D. Lean Integration: An Integration Factory Approach to Business Agility; Addison-Wesley Professional: Boston, MA, USA, 2010. [Google Scholar]
{kind=link}
| Demographics | Hospital Type | ||||||
|---|---|---|---|---|---|---|---|
| Government General Hospital | Government Tertiary Hospital | Total Government Hospitals | Private Hospitals | Oil Sector Hospital | Total | ||
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | ||
| Gender | Male | 1 (2.6) | 4 (10.5) | 5 (6.6) | 10 (58.8) | 1 (20.0) | 16 (16.3) |
| Female | 37 (97.4) | 34 (89.5) | 71 (93.4) | 7 (41.2) | 4 (80.0) | 82 (83.7) | |
| Nationality | Kuwaiti | 37 (97.4) | 37 (97.4) | 74 (97.4) | 0 (0.0) | 5 (100.0) | 79 (80.6) |
| Non-Kuwaiti | 1 (2.6) | 1 (2.6) | 2 (2.6) | 17 (100) | 0 (0.0) | 19 (19.4) | |
| Qualification | Elementary | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Intermediate | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Secondary | 3 (7.9) | 3 (7.9) | 6 (7.9) | 2 (11.8) | 0 (0.0) | 8 (8.2) | |
| Special courses | 7 (18.4) | 2 (5.3) | 9 (11.8) | 1 (5.9) | 0 (0.0) | 10 (10.2) | |
| Diploma | 9 (23.7) | 15 (39.5) | 24 (31.6) | 7 (41.2) | 0 (0.0) | 31 (31.6) | |
| Bachelor | 17 (44.7) | 14 (36.8) | 31 (40.8) | 6 (35.3) | 3 (60.0) | 40 (40.8) | |
| Master | 2 (5.3) | 4 (10.5) | 6 (7.9) | 1 (5.9) | 2 (40.0) | 9 (9.2) | |
| PhD | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Position | MRD Director | 5 (13.2) | 16 (42.1) | 21 (27.6) | 1 (5.9) | 0 (0.0) | 22 (22.4) |
| MRD Deputy director | 6 (15.8) | 6 (15.8) | 12 (15.8) | 0 (0.0) | 3 (60.0) | 15 (15.3) | |
| MRD Supervisor | 27 (71.1) | 16 (42.1) | 43 (56.6) | 16 (94.1) | 2 (40.0) | 61 (62.2) | |
| Years of Service | Less than 4 | 2 (5.3) | 6 (15.8) | 8 (10.5) | 2 (11.8) | 0 (0.0) | 10 (10.2) |
| from 5 to 9 | 12 (31.6) | 7 (18.4) | 19 (25.0) | 5 (29.4) | 2 (40.0) | 26 (26.5) | |
| from 10 to 19 | 8 (21.1) | 14 (36.8) | 22 (28.9) | 9 (52.9) | 3 (60.0) | 34 (34.7) | |
| 20+ | 16 (42.1) | 11 (28.9) | 27 (35.5) | 1 (5.9) | 0 (0.0) | 28 (28.6) | |
| Characteristics of Medical Records Management System | Hospital Type | |||||
|---|---|---|---|---|---|---|
| Government General Hospital | Government Tertiary Hospital | Private Hospitals | Oil Sector Hospital | Total | ||
| n (%) | n (%) | n (%) | n (%) | n (%) | ||
| Patient Records media | Paper only | 0 (0.0) | 11 (57.9) | 2 (50.0) | 0 (0.0) | 13 (43.3) |
| Paper & Electronic | 6 (100.0) | 8 (42.1) | 2 (50.0) | 0 (0.0) | 16 (53.3) | |
| Paper, Electronic, & DIMS | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (100.0) | 1 (3.3) | |
| Type of Records System Used | Manual Record System | 0 (0.0) | 5 (26.3) | 1 (25.0) | 0 (0.0) | 6 (20.0) |
| HIS | 0 (0.0) | 2 (10.5) | 0 (0.0) | 1 (100.0) | 3 (10.0) | |
| Hybrid (manual & HIS) | 6 (100.0) | 12 (63.2) | 3 (75) | 0 (0.0) | 21 (70.0) | |
| Filing System | Serial | 0 (0.0) | 4 (21.1) | 2 (50.0) | 0 (0.0) | 6 (20.0) |
| Terminal Digit | 6 (100.0) | 15 (78.9) | 2 (50.0) | 0 (0.0) | 23 (76.7) | |
| Other | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (100.0) | 1 (3.3) | |
| Patient records are kept in (multiple choice) | Filing Room | 6 (100) | 16 (84.2) | 4 (100) | 0 (0.0) | 26 (86.7) |
| Wards | 0 (0.0) | 1 (5.3) | 0 (0.0) | 0 (0.0) | 1 (3.3) | |
| Filing Room & Wards | 0 (0.0) | 3 (15.8) | 0 (0.0) | 0 (0.0) | 3 (10.0) | |
| With patients | 1 (16.7) | 1 (5.3) | 0 (0.0) | 0 (0.0) | 2 (6.7) | |
| Emergency room | 0 (0.0) | 1 (5.3) | 0 (0.0) | 0 (0.0) | 1 (3.3) | |
| Other | 1 (16.7) | 1 (5.3) | 0 (0.0) | 1 (100.0) | 3 (10.0) | |
| Medical Records Policies | Yes n (%) | No n (%) | I Don‘t Know n (%) | Total n (%) | |
| Is the medical records policy and procedure? | Available | 93 (94.9) | 5 (5.1) | 0 (0.0) | 98 (100.0) |
| Reviewed | 89 (90.8) | 6 (6.1) | 3 (3.1) | 98 (100.0) | |
| If yes, how frequently do you review MR policies & procedures? | Yearly | Every 2 years | Other | I don‘t know | Total |
| 50 (51.0%) | 25 (25.5) | 14 (14.3) | 9 (9.2) | 98 (100.0) | |
| Medical Records Policies Awareness | Yes n (%) | No n (%) | I Don‘t know n (%) | Total n (%) | |
| Is the medical records staff aware of the policies & procedures? | 94 (95.9) | 1 (1.0) | 3 (3.1) | 98 (100.0) | |
| Is the medical records staff aware of their roles & responsibilities? | 97 (99.0) | 1 (1.0) | 0 (0.0) | 98 (100.0) | |
| Does MR staff receive copy of their roles & responsibilities? | 83 (84.7) | 15 (15.3) | 0 (0.0) | 98 (100.0) | |
| How are the medical records staff made aware of department policy and procedures? | Orientation | 77 (78.6) | 21 (21.4) | 0 (0.0) | 98 (100.0) |
| Meetings | 54 (55.1) | 44 (44.9) | 0 (0.0) | 98 (100.0) | |
| Circulars | 49 (50.0) | 49 (50.0) | 0 (0.0) | 98 (100.0) | |
| Internet | 2 (2.0) | 96 (98.0) | 0 (0.0) | 98 (100.0) | |
| 16 (16.3) | 82 (83.7) | 0 (0.0) | 98 (100.0) | ||
| Other | 12 (12.2) | 86 (87.8) | 0 (0.0) | 98 (100.0) | |
| Storage, Retention, and Disposal of Medical Records | Hospital Type | |||||
|---|---|---|---|---|---|---|
| Government General Hospital | Government Tertiary Hospital | Private Hospitals | Oil Sector Hospital | Total | ||
| n (%) | n (%) | n (%) | n (%) | n (%) | ||
| How long were inactive Kuwaiti patients‘ records kept in the department? | 2 years | 0 (0.0) | 1 (5.3) | 0 (0.0) | 0 (0.0) | 1 (3.3) |
| 5 years | 1 (16.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (3.3) | |
| 10 years | 5 (83.3) | 13 (68.4) | 4 (100.0) | 0 (0.0) | 22 (73.3) | |
| More than 10 years | 0 (0.0) | 5 (26.3) | 0 (0.0) | 0 (0.0) | 5 (16.7) | |
| NA | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (100.0) | 1 (3.3) | |
| How long were in-active Non-Kuwaiti patients‘ records kept in the department? | 2 years | 1 (16.7) | 1 (5.3) | 0(0.0) | 0 (0.0) | 2 (6.7) |
| 5 years | 5 (83.3) | 15 (78.9) | 4 (100.0) | 0 (0.0) | 24 (80.0) | |
| 10 years | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0(0.0) | |
| More than 10 years | 0 (0.0) | 3 (15.8) | 0 (0.0) | 0 (0.0) | 3 (10.0) | |
| NA | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (100.0) | 1 (3.3) | |
| Do you have enough storage facilities | Yes | 0 (0.0) | 4 (21.1) | 2 (50.0) | 1 (100.0) | 7 (23.3) |
| No | 6 (100.0) | 15 (78.9) | 2 (50.0) | 0 (0.0) | 23 (76.7) | |
| Method of Disposal of patient in-active records | Burned then disposed | 1 (16.7) | 2 (10.5) | 0 (0.0) | 0 (0.0) | 3 (10.0) |
| Archived then burned & disposed | 3 (50.0) | 0 (0.0) | 1 (25.0) | 0 (0.0) | 4 (13.3) | |
| Stacked then stored on-site | 2 (33.3) | 13 (68.4) | 0 (0.0) | 0 (0.0) | 15 (50.0) | |
| Stored off site facility | 2 (33.3) | 3 (15.8) | 1 (25.0) | 0 (0.0) | 6 (20.0) | |
| Other methods | 0 (0.0) | 2 (10.5) | 1 (25.0) | 1 (100.0) | 4 (13.3) | |
| NA | 0 (0.0) | 0 (0.0) | 1 (25.0) | 0 (0.0) | 1 (3.3) | |
| Availability of MR disposal policy | Ministry of Health policy | 4 (66.7) | 13 (68.4) | 4 (100.0) | 0 (0.0) | 21 (70.0) |
| Hospital policy | 2 (33.3) | 1 (5.3) | 1 (25.0) | 0 (0.0) | 4 (13.3) | |
| Department policy | 3 (50.0) | 5 (26.3) | 0 (0.0) | 0 (0.0) | 8 (26.7) | |
| v6-Years of Service | v11-Available | v14-Aware | ||
|---|---|---|---|---|
| v6-Years of Service | Pearson Correlation | 1 | 0.092 | −0.081 |
| Sig. (2-tailed) | 0.365 | 0.430 | ||
| N | 98 | 98 | 98 | |
| v11-Available | Pearson Correlation | 0.092 | 1 | 0.213 * |
| Sig. (2-tailed) | 0.365 | 0.035 | ||
| N | 98 | 98 | 98 | |
| v14-Aware | Pearson Correlation | −0.081 | 0.213 * | 1 |
| Sig. (2-tailed) | 0.430 | 0.035 | ||
| N | 98 | 98 | 98 | |
| Missing Medical Records | How Were the Records Filed? | Lack of Storage Facilities | |||||
|---|---|---|---|---|---|---|---|
| Missing medical records | Pearson Correlation | 1 | −0.025 | 0.095 | |||
| Sig. (1-tailed) | 0.448 | 0.309 | |||||
| N | 30 | 30 | 30 | ||||
| How were the records filed? | Pearson Correlation | −0.025 | 1 | −0.104 | |||
| Sig. (1-tailed) | 0.448 | 0.292 | |||||
| N | 30 | 30 | 30 | ||||
| Lack of storage facilities | Pearson Correlation | 0.095 | −0.104 | 1 | |||
| Sig. (1-tailed) | 0.309 | 0.292 | |||||
| N | 30 | 30 | 30 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alnashmi, M.; Salman, A.; AlHumaidi, H.; Yunis, M.; Al-Enezi, N. Exploring the Health Information Management System of Kuwait: Lessons and Opportunities. Appl. Syst. Innov. 2022, 5, 25. https://doi.org/10.3390/asi5010025
Alnashmi M, Salman A, AlHumaidi H, Yunis M, Al-Enezi N. Exploring the Health Information Management System of Kuwait: Lessons and Opportunities. Applied System Innovation. 2022; 5(1):25. https://doi.org/10.3390/asi5010025
Chicago/Turabian StyleAlnashmi, Maha, Ahmad Salman, Hanadi AlHumaidi, Maha Yunis, and Naser Al-Enezi. 2022. "Exploring the Health Information Management System of Kuwait: Lessons and Opportunities" Applied System Innovation 5, no. 1: 25. https://doi.org/10.3390/asi5010025
APA StyleAlnashmi, M., Salman, A., AlHumaidi, H., Yunis, M., & Al-Enezi, N. (2022). Exploring the Health Information Management System of Kuwait: Lessons and Opportunities. Applied System Innovation, 5(1), 25. https://doi.org/10.3390/asi5010025