
Vertical and Side-Alternating Whole Body Vibration Platform Parameters Influence Lower Extremity Blood Flow and Muscle Oxygenation

 ,
, 
Abstract
:1. Introduction
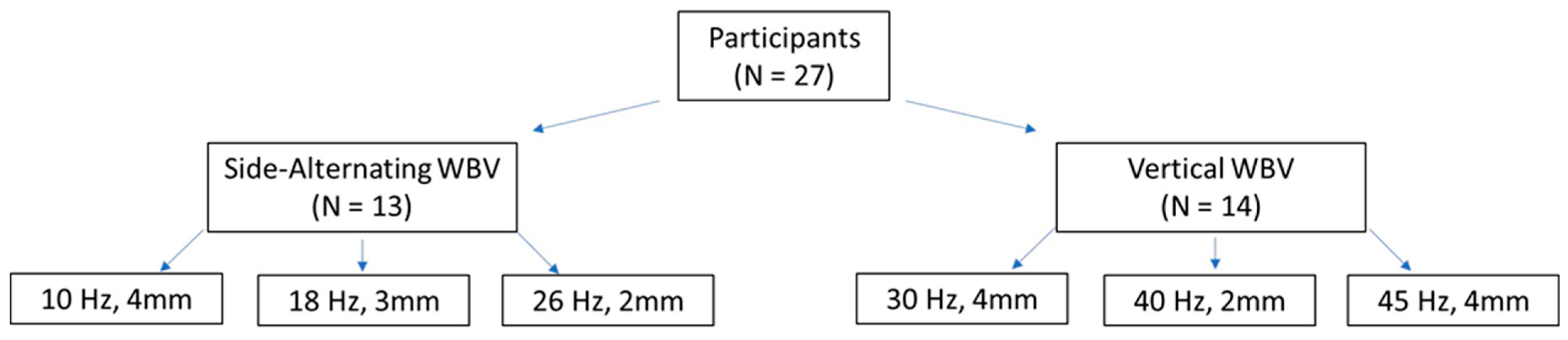
2. Materials and Methods
3. Results
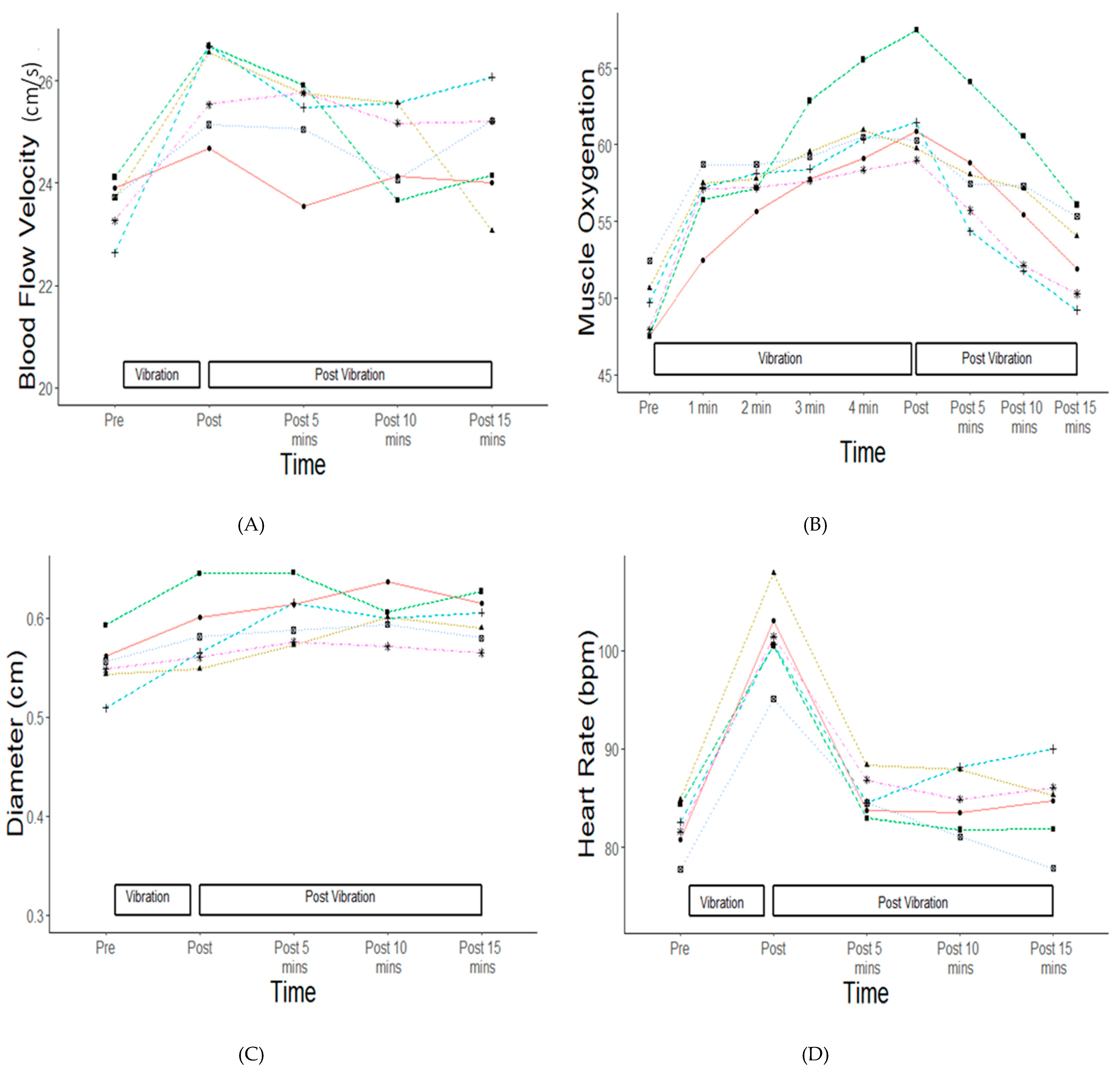
3.1. Heart Rate, Blood Flow Velocity, Popliteal Diameter, and Skin Temperature
3.2. Muscle Oxygenation
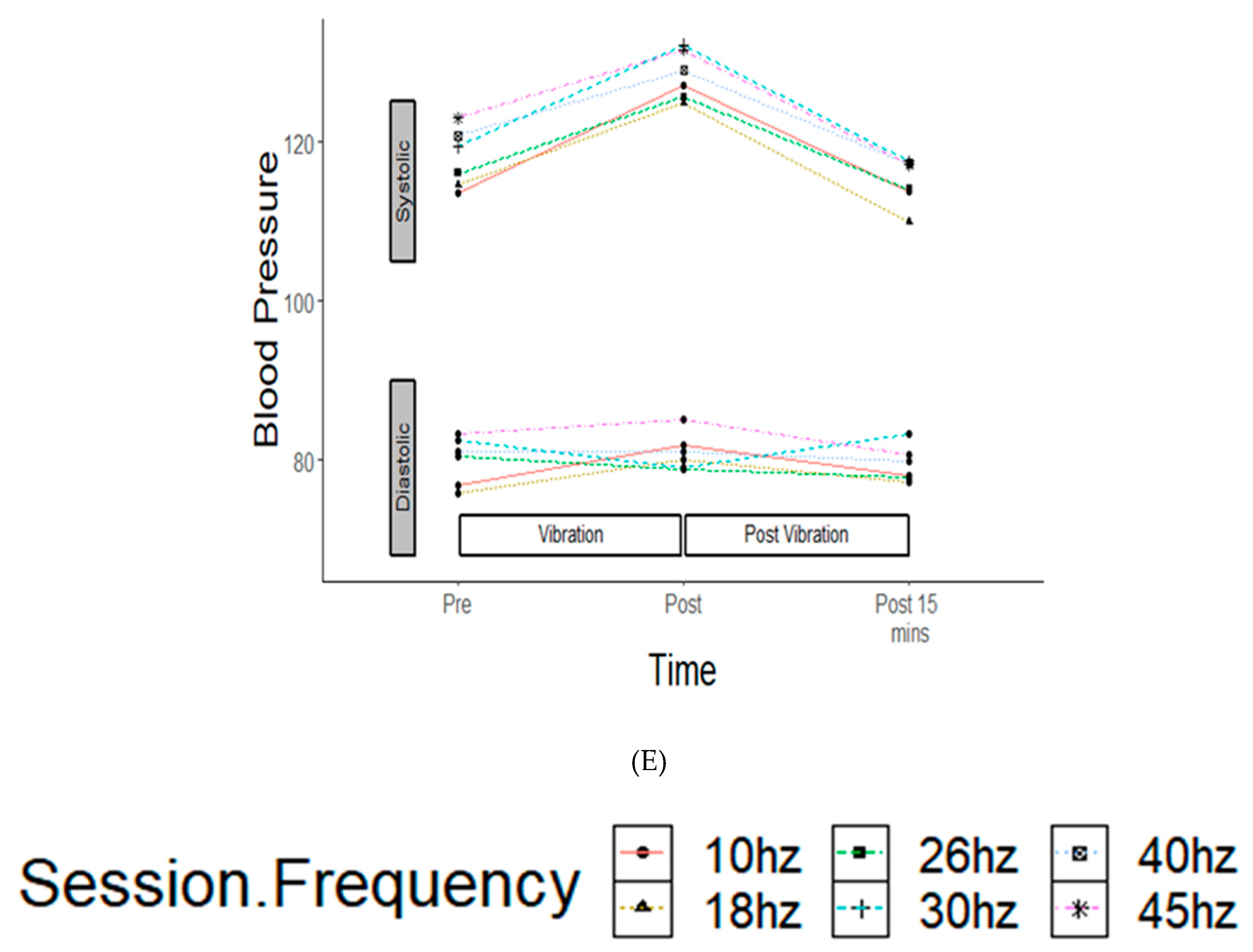
3.3. Blood Pressure
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Zepetnek, J.O.T.; Giangregorio, L.M.; Craven, B.C. Whole-body vibration as potential intervention for people with low bone mineral density and osteoporosis: A review. J. Rehabil. Res. Dev. 2009, 46, 529–542. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Liu, A.; Sun, M.; Zhu, H.; Wu, H. Effect of whole-body vibration on reduction of bone loss and fall prevention in postmenopausal women: A meta-analysis and systematic review. J. Orthop. Surg. Res. 2016, 11, 24. [Google Scholar] [CrossRef] [PubMed]
- Ahlborg, L.; Andersson, C.; Julin, P. Whole-body vibration training compared with resistance training: Effect on spasticity, muscle strength and motor performance in adults with cerebral palsy. J. Rehabil. Med. 2006, 38, 302–308. [Google Scholar] [CrossRef]
- Song, S.; Lee, K.; Jung, S.; Park, S.; Cho, H.; Lee, G. Effect of Horizontal Whole-Body Vibration Training on Trunk and Lower-Extremity Muscle Tone and Activation, Balance, and Gait in a Child with Cerebral Palsy. Am. J. Case Rep. 2018, 19, 1292–1300. [Google Scholar] [CrossRef]
- Moezy, A.; Olyaei, G.R.; Hadian, M.R.; Razi, M.; Faghihzadeh, S. A comparative study of whole body vibration training and conventional training on knee proprioception and postural stability after anterior cruciate ligament reconstruction. Br. J. Sports Med. 2008, 42, 373–385. [Google Scholar] [CrossRef] [PubMed]
- Costantino, C.; Bertuletti, S.; Romiti, D. Efficacy of Whole-Body Vibration Board Training on Strength in Athletes After Anterior Cruciate Ligament Reconstruction: A Randomized Controlled Study. Clin. J. Sport Med. 2018, 28, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Sierra-Guzmán, R.; Jiménez-Diaz, F.; Ramírez, C.; Esteban, P.; Abián-Vicén, J. Whole-Body–Vibration Training and Balance in Recreational Athletes with Chronic Ankle Instability. J. Athl. Train. 2018, 53, 355–363. [Google Scholar] [CrossRef]
- Cloak, R.; Nevill, A.; Day, S.; Wyon, M. Six-Week Combined Vibration and Wobble Board Training on Balance and Stability in Footballers with Functional Ankle Instability. Clin. J. Sport Med. 2013, 23, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Sierra-Guzmán, R.; Jiménez, J.F.; Ramírez, C.; Esteban, P.; Abián-Vicén, J. Effects of Synchronous Whole Body Vibration Training on a Soft, Unstable Surface in Athletes with Chronic Ankle Instability. Endoscopy 2017, 38, 447–455. [Google Scholar] [CrossRef]
- Fagnani, F.; Giombini, A.; Di Cesare, A.; Pigozzi, F.; Di Salvo, V. The Effects of a Whole-Body Vibration Program on Muscle Performance and Flexibility in Female Athletes. Am. J. Phys. Med. Rehabil. 2006, 85, 956–962. [Google Scholar] [CrossRef] [Green Version]
- Cochrane, D.J. Acute whole body vibration training increases vertical jump and flexibility performance in elite female field hockey players. Br. J. Sports Med. 2005, 39, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Järvinen, T.; Järvinen, T.; Kääriäinen, M.; Kalimo, H.; Järvinen, M. Biology of muscle trauma. Am. J. Sports Med. 2005, 33, 745–766. [Google Scholar] [CrossRef] [PubMed]
- Games, K.E.; Sefton, J. Whole-body vibration influences lower extremity circulatory and neurological function. Scand. J. Med. Sci. Sports 2013, 23, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Yamada, E.; Kusaka, T.; Miyamoto, K.; Tanaka, S.; Morita, S.; Tanaka, S.; Tsuji, S.; Mori, S.; Norimatsu, H.; Itoh, S. Vastus lateralis oxygenation and blood volume measured by near-infrared spectroscopy during whole body vibration. Clin. Physiol. Funct. Imaging 2005, 25, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Maloney-Hinds, C.; Petrofsky, J.S.; Zimmerman, G. The effect of 30 Hz vs. 50 Hz passive vibration and duration of vibration on skin blood flow in the arm. Med. Sci. Monit. 2008, 14, 112–116. [Google Scholar]
- Lythgo, N.; Eser, P.; De Groot, P.; Galea, M. Whole-body vibration dosage alters leg blood flow. Clin. Physiol. Funct. Imaging 2009, 29, 53–59. [Google Scholar] [CrossRef]
- Coza, A.; Nigg, B.M.; Dunn, J.F. Effects of Vibrations on Gastrocnemius Medialis Tissue Oxygenation. Med. Sci. Sports Exerc. 2011, 43, 509–515. [Google Scholar] [CrossRef]
- Cardinale, M.; Ferrari, M.; Quaresima, V. Gastrocnemius Medialis and Vastus Lateralis Oxygenation during Whole-Body Vibration Exercise. Med. Sci. Sports Exerc. 2007, 39, 694–700. [Google Scholar] [CrossRef]
- Hazell, T.J.; Thomas, G.W.R.; DeGuire, J.R.; Lemon, P.W.R. Vertical whole-body vibration does not increase cardiovascular stress to static semi-squat exercise. Eur. J. Appl. Physiol. 2008, 104, 903–908. [Google Scholar] [CrossRef]
- Team, R.C. R: A Language Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2010. [Google Scholar]
- RStudio. Rstudio: Integrated Development Environment for R. 2014. Available online: https://www.rstudio.com/products/rstudio/ (accessed on 1 August 2021).
- Kerschan-Schindl, K.; Grampp, S.; Henk, C.; Resch, H.; Preisinger, E.; Fialka-Moser, V.; Imhof, H. Whole-body vibration exercise leads to alterations in muscle blood volume. Clin. Physiol. 2001, 21, 377–382. [Google Scholar] [CrossRef]
- Calvisi, V.; Angelozzi, M.; Franco, A.; Mottola, L.; Crisostomi, S.; Corsica, C.; Ferrari, M.; Quaresima, V. Influence of whole-body vibration static exercise on quadriceps oxygenation. In Oxygen Transport to Tissue Xxvii; Cicco, G., Bruley, D.F., Ferrari, M., Harrison, D.K., Eds.; Springer: Boston, MA, USA, 2006; Volume 578, pp. 137–141. [Google Scholar]
- Hortobágyi, T.; Lesinski, M.; Fernandez-del-Olmo, M.; Granacher, U. Small and inconsistent effects of whole body vi-bration on athletic performance: A systematic review and meta-analysis. Eur. J. Appl. Physiol. 2015, 115, 1605–1625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rønnestad, B.R. Acute Effects of Various Whole-Body Vibration Frequencies on Lower-Body Power in Trained and Untrained Subjects. J. Strength Cond. Res. 2009, 23, 1309–1315. [Google Scholar] [CrossRef] [PubMed]
- Farzam, P.; Starkweather, Z.; Franceschini, M.A. Validation of a novel wearable, wireless technology to estimate oxygen levels and lactate threshold power in the exercising muscle. Physiol. Rep. 2018, 6, e13664. [Google Scholar] [CrossRef] [PubMed]
- Games, K.E.; Sefton, J.M.; Wilson, A.E. Whole-Body Vibration and Blood Flow and Muscle Oxygenation: A Meta-Analysis. J. Athl. Train. 2015, 50, 542–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Age (y/o) | Height (cm) | Weight (kg) | Females/Males |
|---|---|---|---|---|
| Vertical Vibration (n = 14) | 24.1 ± 3.1 | 169.7 ± 7.5 | 75.0 ± 19.6 | 6/8 |
| Side Alternating Vibration (n = 13) | 23.4 ± 2.7 | 168.1 ± 10.9 | 72.5 ± 14.2 | 5/8 |
| Main Effects | Variable | Post Hoc | p Value |
|---|---|---|---|
| Time | Session frequency | 0.001 | |
| Time | Popliteal artery diameter | 0.008 | |
| Post hoc: 5 min post-vibration | 0.04 | ||
| Time | Heart rate | 5, 1- and 15 min post-vibration | 0.001 |
| Frequency | Skin temperature: Posterior leg | 0.01 | |
| Anterior lower leg | 0.04 | ||
| Posterior upper leg | 0.001 | ||
| Anterior upper leg | 0.01 | ||
| Time | Muscle oxygenation | 0.001 | |
| Post hoc: increases with time of vibration | |||
| Time | Systolic blood pressure | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lyons, K.D.; Parks, A.G.; Dadematthews, O.D.; McHenry, P.A.; Sefton, J.M. Vertical and Side-Alternating Whole Body Vibration Platform Parameters Influence Lower Extremity Blood Flow and Muscle Oxygenation. Vibration 2022, 5, 557-567. https://doi.org/10.3390/vibration5030031
Lyons KD, Parks AG, Dadematthews OD, McHenry PA, Sefton JM. Vertical and Side-Alternating Whole Body Vibration Platform Parameters Influence Lower Extremity Blood Flow and Muscle Oxygenation. Vibration. 2022; 5(3):557-567. https://doi.org/10.3390/vibration5030031
Chicago/Turabian StyleLyons, Kaitlin D., Aaron G. Parks, Oluwagbemiga D. Dadematthews, Paige A. McHenry, and JoEllen M. Sefton. 2022. "Vertical and Side-Alternating Whole Body Vibration Platform Parameters Influence Lower Extremity Blood Flow and Muscle Oxygenation" Vibration 5, no. 3: 557-567. https://doi.org/10.3390/vibration5030031
APA StyleLyons, K. D., Parks, A. G., Dadematthews, O. D., McHenry, P. A., & Sefton, J. M. (2022). Vertical and Side-Alternating Whole Body Vibration Platform Parameters Influence Lower Extremity Blood Flow and Muscle Oxygenation. Vibration, 5(3), 557-567. https://doi.org/10.3390/vibration5030031