
Mapping the Glymphatic Pathway Using Imaging Advances

 , , ,
, , , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
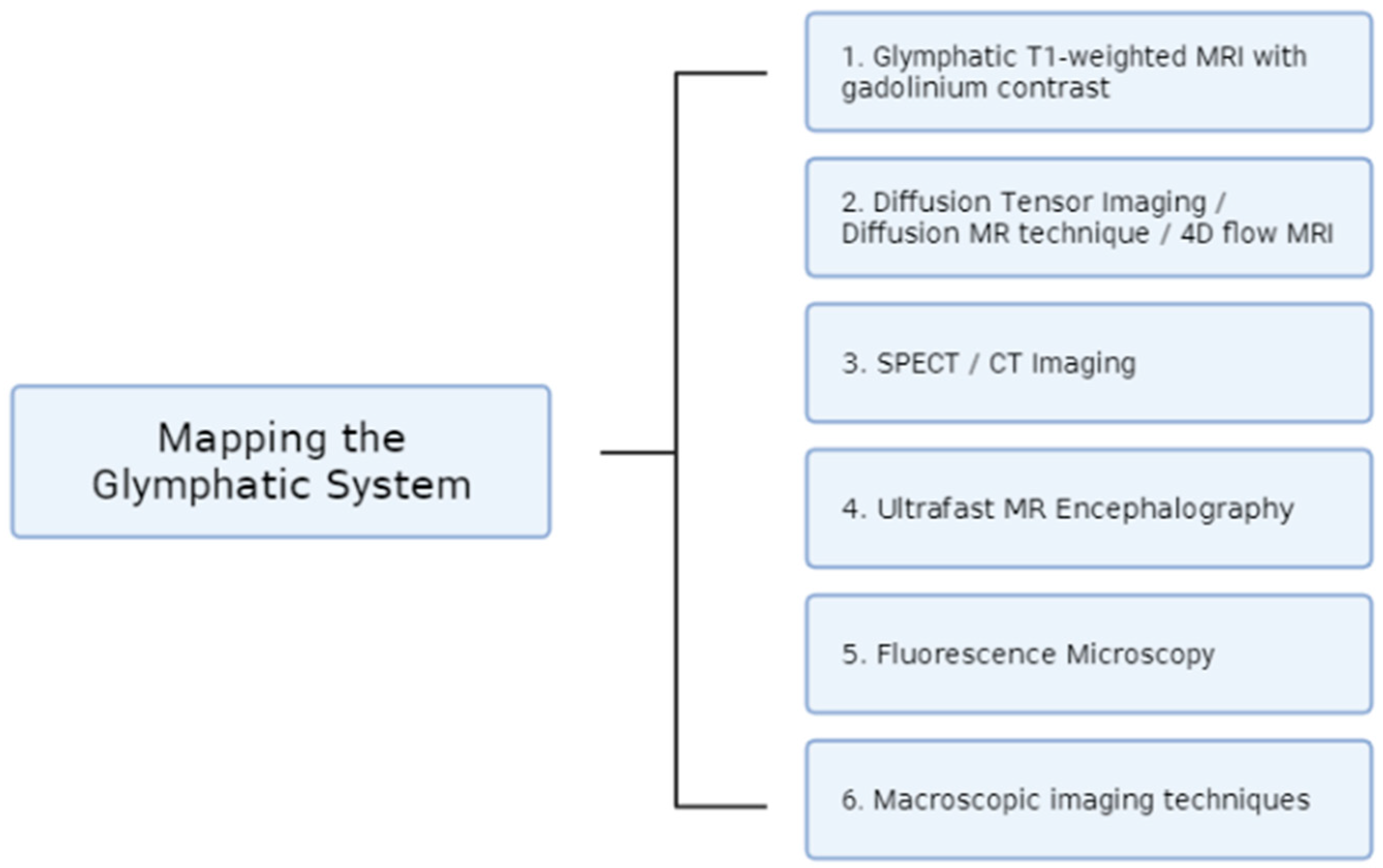
2. Imaging Techniques
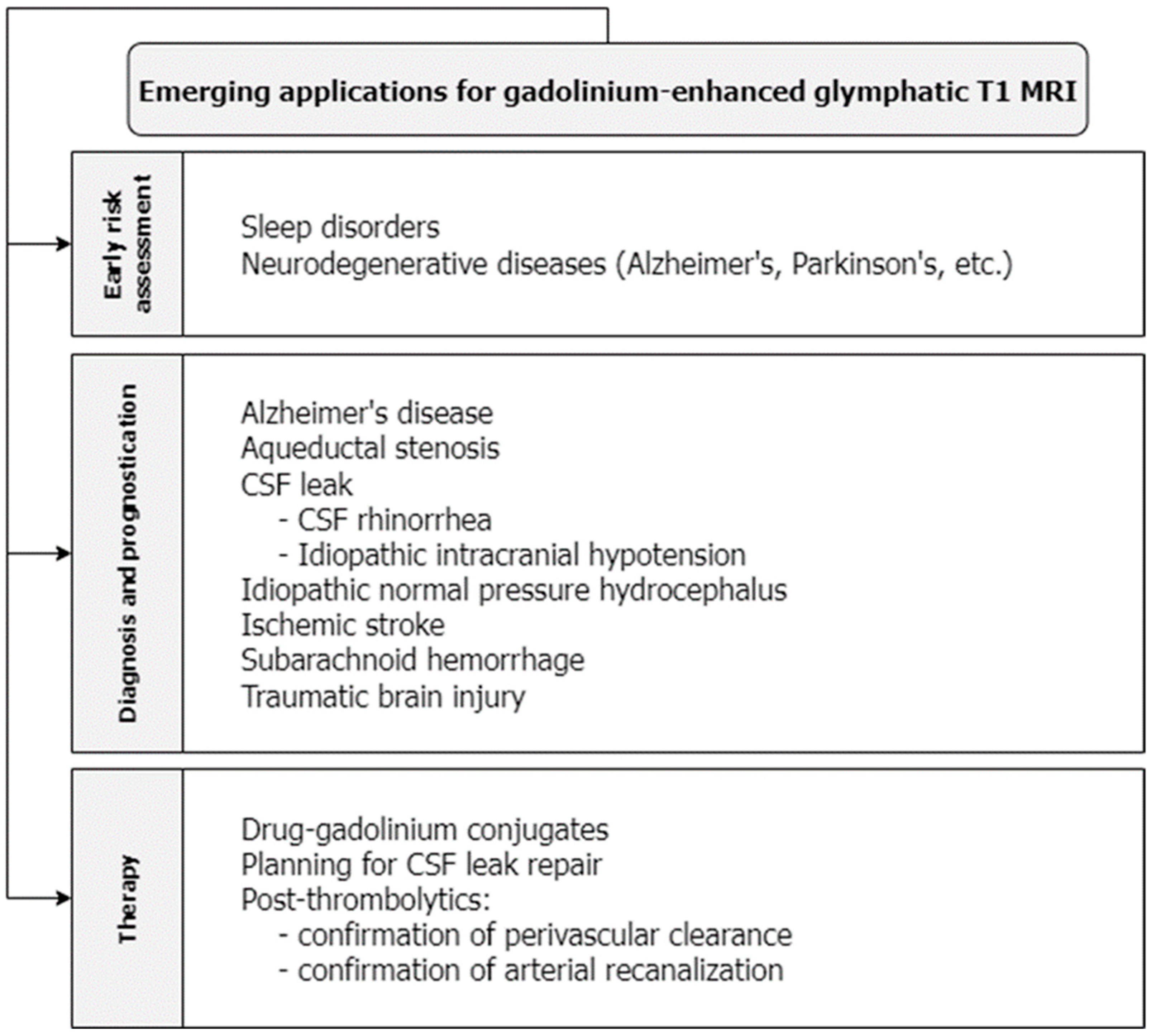
2.1. Glymphatic T1-Weighted MRI with Gadolinium Contrast
- Intrathecal gadolinium enhancement of glymphatic T1 MRI:
- b.
- Intravenous gadolinium enhancement of glymphatic T1 MRI:
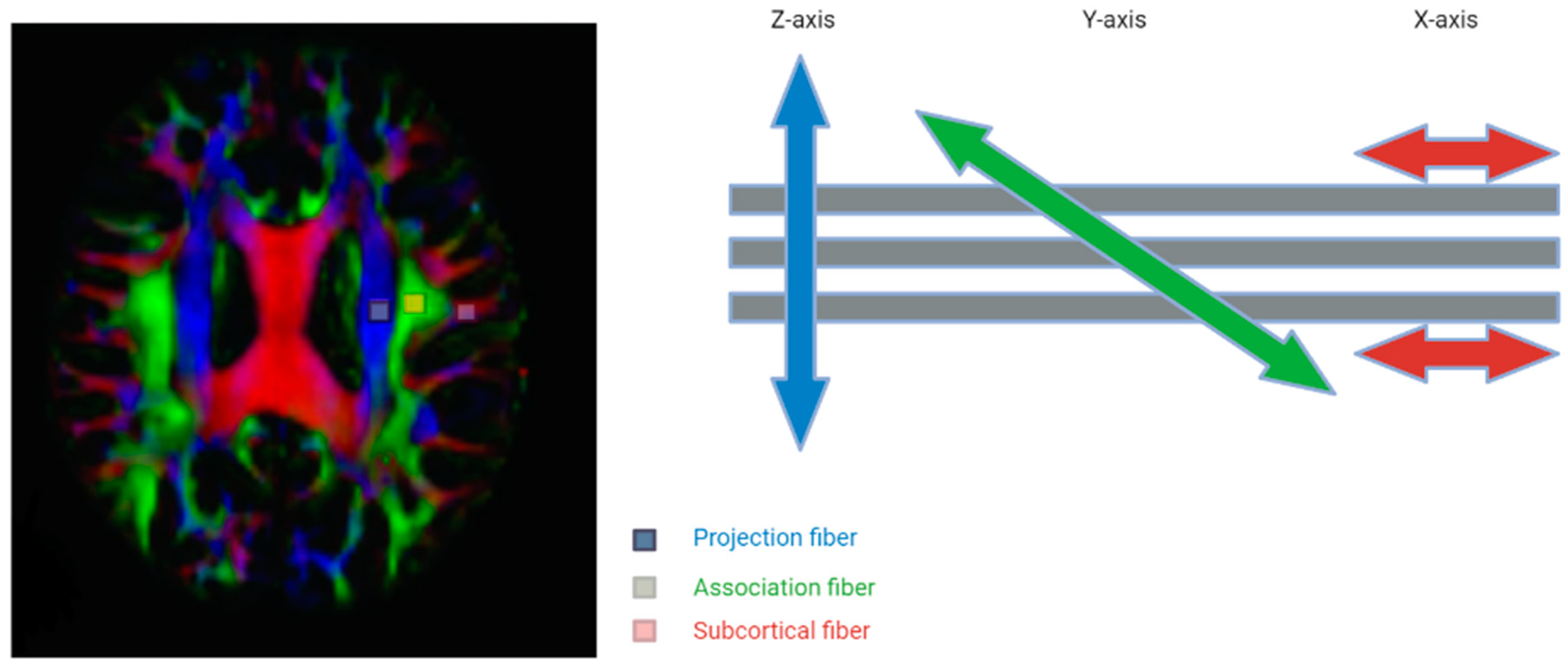
2.2. Diffusion Tensor Imaging/Diffusion MR Technique/4D Flow MRI
2.3. SPECT/CT Imaging
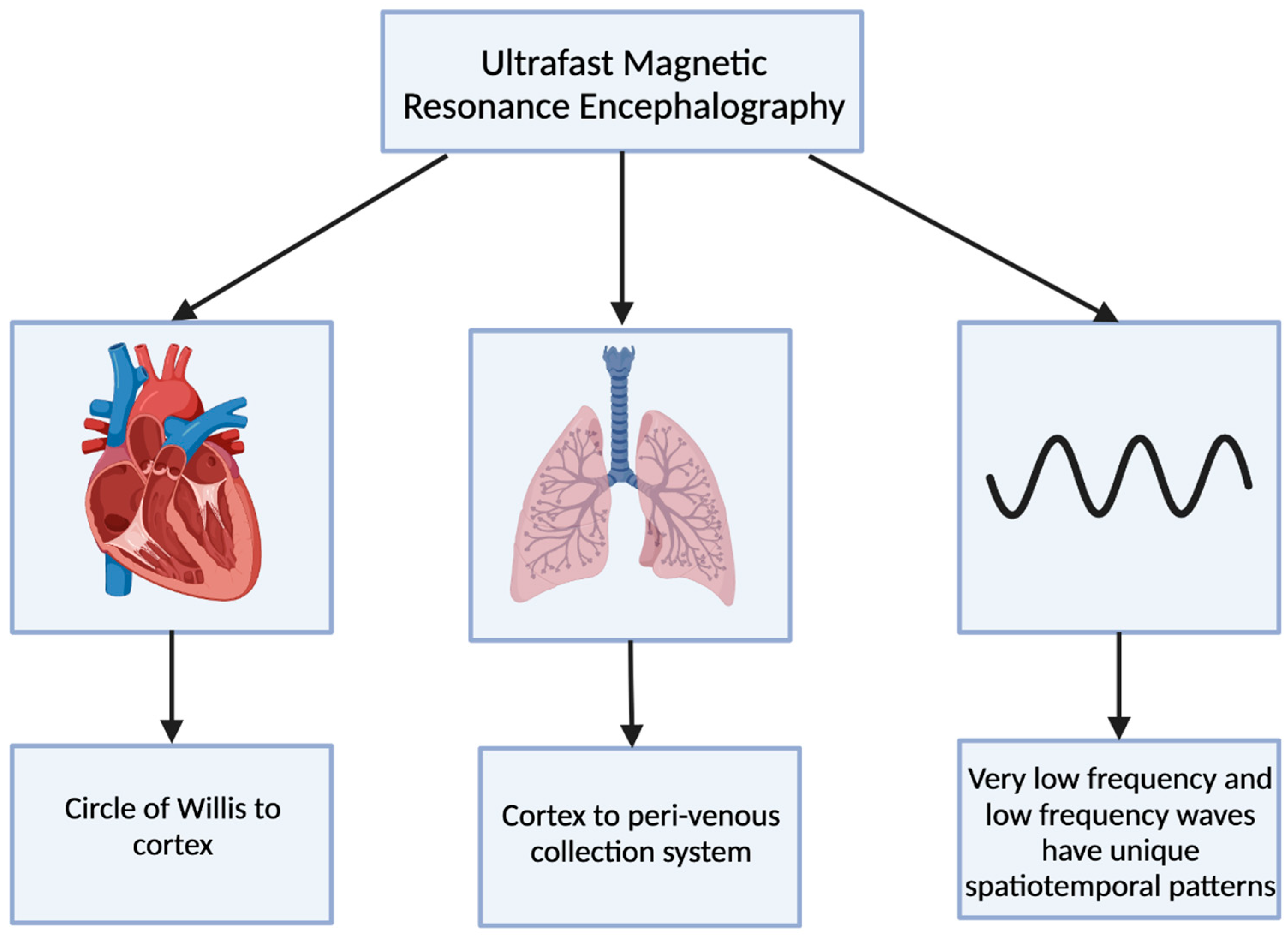
2.4. Ultrafast MR Encephalography
2.5. Fluorescence Microscopy
2.6. Macroscopic Imaging Techniques
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Shaykevich, S.; Chan, R.W.; Rana, C.; Eltaeb, M.; Little, J.P.; Razansky, D.; Razansky, D.; Chan, C.; Shoham, S. Optoacoustic imaging of the glymphatic system. Veins Lymphat. 2022, 11, 10967. [Google Scholar] [CrossRef]
- Nycz, B.; Mandera, M. The features of the glymphatic system. Auton. Neurosci. 2021, 232, 102774. [Google Scholar] [CrossRef] [PubMed]
- Klostranec, J.M.; Vucevic, D.; Bhatia, K.D.; Kortman, H.G.J.; Krings, T.; Murphy, K.P.; terBrugge, K.G.; Mikulis, D.J. Current Concepts in Intracranial Interstitial Fluid Transport and the Glymphatic System: Part II-Imaging Techniques and Clinical Applications. Radiology 2021, 301, 516–532. [Google Scholar] [CrossRef]
- Iliff, J.J.; Chen, M.J.; Plog, B.A.; Zeppenfeld, D.M.; Soltero, M.; Yang, L.; Singh, I.; Deane, R.; Nedergaard, M. Impairment of glymphatic pathway function promotes tau pathology after traumatic brain injury. J. Neurosci. 2014, 34, 16180–16193. [Google Scholar] [CrossRef] [PubMed]
- Taoka, T.; Naganawa, S. Glymphatic imaging using MRI. J. Magn. Reason. Imaging 2020, 51, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Bae, Y.J.; Kim, J.S.; Jung, W.S.; Choi, J.W.; Roh, T.H.; You, N.; Kim, S.H.; Han, M. Glymphatic system evaluation using diffusion tensor imaging in patients with traumatic brain injury. Neuroradiology 2023, 65, 551–557. [Google Scholar] [CrossRef]
- Lilius, T.O.; Rosenholm, M.; Klinger, L.; Mortensen, K.N.; Sigurdsson, B.; Mogensen, F.L.; Hauglund, N.L.; Nielsen, M.S.N.; Rantamäki, T.; Nedergaard, M. SPECT/CT imaging reveals CNS-wide modulation of glymphatic cerebrospinal fluid flow by systemic hypertonic saline. iScience 2022, 25, 105250. [Google Scholar] [CrossRef]
- Kiviniemi, V.; Wang, X.; Korhonen, V.; Keinänen, T.; Tuovinen, T.; Autio, J.; LeVan, P.; Keilholz, S.; Zang, Y.F.; Hennig, J.; et al. Ultra-fast magnetic resonance encephalography of physiological brain activity-Glymphatic pulsation mechanisms? J. Cereb. Blood Flow Metab. 2016, 36, 1033–1045. [Google Scholar] [CrossRef]
- Bèchet, N.B.; Kylkilahti, T.M.; Mattsson, B.; Petrasova, M.; Shanbhag, N.C.; Lundgaard, I. Light sheet fluorescence microscopy of optically cleared brains for studying the glymphatic system. J. Cereb. Blood Flow Metab. 2020, 40, 1975–1986. [Google Scholar] [CrossRef]
- Plog, B.A.; Mestre, H.; Olveda, G.E.; Sweeney, A.M.; Kenney, H.M.; Cove, A.; Dholakia, K.Y.; Tithof, J.; Nevins, T.D.; Lundgaard, I.; et al. Transcranial optical imaging reveals a pathway for optimizing the delivery of immunotherapeutics to the brain. JCI Insight 2018, 3, 120922. [Google Scholar] [CrossRef]
- Arlt, S.; Cepek, L.; Rustenbeck, H.H.; Prange, H.; Reimers, C.D. Gadolinium encephalopathy due to accidental intrathecal administration of gadopentetate dimeglumine. J. Neurol. 2007, 254, 810–812. [Google Scholar] [CrossRef]
- Reeves, C.; Galang, E.; Padalia, R.; Tran, N.; Padalia, D. Intrathecal Injection of Gadobutrol: A Tale of Caution. J. Pain. Palliat. Care Pharmacother. 2017, 31, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Edeklev, C.S.; Halvorsen, M.; Løvland, G.; Vatnehol, S.A.S.; Gjertsen, Ø.; Nedregaard, B.; Sletteberg, R.; Ringstad, G.; Eide, P.K. Intrathecal Use of Gadobutrol for Glymphatic MR Imaging: Prospective Safety Study of 100 Patients. AJNR Am. J. Neuroradiol. 2019, 40, 1257–1264. [Google Scholar] [CrossRef] [PubMed]
- Iliff, J.J.; Lee, H.; Yu, M.; Feng, T.; Logan, J.; Nedergaard, M.; Benveniste, H. Brain-wide pathway for waste clearance captured by contrast-enhanced MRI. J. Clin. Investig. 2013, 123, 1299–1309. [Google Scholar] [CrossRef] [PubMed]
- Ringstad, G.; Valnes, L.M.; Dale, A.M.; Pripp, A.H.; Vatnehol, S.S.; Emblem, K.E.; Mardal, K.A.; Eide, P.K. Brain-wide glymphatic enhancement and clearance in humans assessed with MRI. JCI Insight 2018, 3, 121537. [Google Scholar] [CrossRef]
- Lee, H.; Choi, S.H.; Anzai, Y. Glymphatic MRI techniques in sleep and neurodegenerative diseases. Curr. Opin. Pulm. Med. 2022, 28, 499–510. [Google Scholar] [CrossRef]
- Petiet, A.; Santin, M.; Bertrand, A.; Wiggins, C.J.; Petit, F.; Houitte, D.; Hantraye, P.; Benavides, J.; Debeir, T.; Rooney, T.; et al. Gadolinium-staining reveals amyloid plaques in the brain of Alzheimer’s transgenic mice. Neurobiol. Aging 2012, 33, 1533–1544. [Google Scholar] [CrossRef]
- Aydin, K.; Terzibasioglu, E.; Sencer, S.; Sencer, A.; Suoglu, Y.; Karasu, A.; Kiris, T.; Turantan, M.I. Localization of cerebrospinal fluid leaks by gadolinium-enhanced magnetic resonance cisternography: A 5-year single-center experience. Neurosurgery 2008, 62, 584–589, discussion 584–589. [Google Scholar] [CrossRef]
- Schick, U.; Musahl, C.; Papke, K. Diagnostics and treatment of spontaneous intracranial hypotension. Minim. Invasive Neurosurg. 2010, 53, 15–20. [Google Scholar] [CrossRef]
- Ramalho, J.; Ramalho, M.; Jay, M.; Burke, L.M.; Semelka, R.C. Gadolinium toxicity and treatment. Magn. Reason. Imaging 2016, 34, 1394–1398. [Google Scholar] [CrossRef]
- Ramalho, J.; Semelka, R.C.; Ramalho, M.; Nunes, R.H.; AlObaidy, M.; Castillo, M. Gadolinium-Based Contrast Agent Accumulation and Toxicity: An Update. AJNR Am. J. Neuroradiol. 2016, 37, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- Gaberel, T.; Gakuba, C.; Goulay, R.; De Lizarrondo, S.M.; Hanouz, J.L.; Emery, E.; Touze, E.; Vivien, D.; Gauberti, M. Impaired glymphatic perfusion after strokes revealed by contrast-enhanced MRI: A new target for fibrinolysis? Stroke 2014, 45, 3092–3096. [Google Scholar] [CrossRef]
- Li, L.; Chopp, M.; Ding, G.; Davoodi-Bojd, E.; Zhang, L.; Li, Q.; Zhang, Y.; Xiong, Y.; Jiang, Q. MRI detection of impairment of glymphatic function in rat after mild traumatic brain injury. Brain Res. 2020, 1747, 147062. [Google Scholar] [CrossRef]
- Taoka, T.; Jost, G.; Frenzel, T.; Naganawa, S.; Pietsch, H. Impact of the Glymphatic System on the Kinetic and Distribution of Gadodiamide in the Rat Brain: Observations by Dynamic MRI and Effect of Circadian Rhythm on Tissue Gadolinium Concentrations. Investig. Radiol. 2018, 53, 529–534. [Google Scholar] [CrossRef]
- Lee, S.; Yoo, R.E.; Choi, S.H.; Oh, S.H.; Ji, S.; Lee, J.; Huh, K.Y.; Lee, J.Y.; Hwang, I.; Kang, K.M.; et al. Contrast-enhanced MRI T1 Mapping for Quantitative Evaluation of Putative Dynamic Glymphatic Activity in the Human Brain in Sleep-Wake States. Radiology 2021, 300, 661–668. [Google Scholar] [CrossRef]
- Taoka, T.; Naganawa, S. Gadolinium-based Contrast Media, Cerebrospinal Fluid and the Glymphatic System: Possible Mechanisms for the Deposition of Gadolinium in the Brain. Magn. Reason. Med. Sci. 2018, 17, 111–119. [Google Scholar] [CrossRef]
- Richmond, S.B.; Rane, S.; Hanson, M.R.; Albayram, M.; Iliff, J.J.; Kernagis, D.; Rosenberg, J.T.; Seidler, R.D. Quantification approaches for magnetic resonance imaging following intravenous gadolinium injection: A window into brain-wide glymphatic function. Eur. J. Neurosci. 2023, 57, 1689–1704. [Google Scholar] [CrossRef]
- van de Haar, H.J.; Burgmans, S.; Jansen, J.F.; van Osch, M.J.; van Buchem, M.A.; Muller, M.; Hofman, P.A.; Verhey, F.R.; Backes, W.H. Blood-Brain Barrier Leakage in Patients with Early Alzheimer Disease. Radiology 2016, 281, 527–535. [Google Scholar] [CrossRef]
- Iliff, J.J.; Nedergaard, M. Is there a cerebral lymphatic system? Stroke 2013, 44 (Suppl. 1), S93–S95. [Google Scholar] [CrossRef]
- Taoka, T.; Masutani, Y.; Kawai, H.; Nakane, T.; Matsuoka, K.; Yasuno, F.; Kishimoto, T.; Naganawa, S. Evaluation of glymphatic system activity with the diffusion MR technique: Diffusion tensor image analysis along the perivascular space (DTI-ALPS) in Alzheimer’s disease cases. Jpn. J. Radiol. 2017, 35, 172–178. [Google Scholar] [CrossRef]
- Luo, C.; Yao, X.; Li, J.; He, B.; Liu, Q.; Ren, H.; Liang, F.; Li, M.; Lin, H.; Peng, J.; et al. Paravascular pathways contribute to vasculitis and neuroinflammation after subarachnoid hemorrhage independently of glymphatic control. Cell Death Dis. 2016, 7, e2160. [Google Scholar] [CrossRef] [PubMed]
- Tarasoff-Conway, J.M.; Carare, R.O.; Osorio, R.S.; Glodzik, L.; Butler, T.; Fieremans, E.; Axel, L.; Rusinek, H.; Nicholson, C.; Zlokovic, B.V.; et al. Clearance systems in the brain-implications for Alzheimer disease. Nat. Rev. Neurol. 2015, 11, 457–470. [Google Scholar] [CrossRef] [PubMed]
- Hanyu, H.; Shindo, H.; Kakizaki, D.; Abe, K.; Iwamoto, T.; Takasaki, M. Increased water diffusion in cerebral white matter in Alzheimer’s disease. Gerontology 1997, 43, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Hanyu, H.; Sakurai, H.; Iwamoto, T.; Takasaki, M.; Shindo, H.; Abe, K. Diffusion-weighted MR imaging of the hippocampus and temporal white matter in Alzheimer’s disease. J. Neurol. Sci. 1998, 156, 195–200. [Google Scholar] [CrossRef]
- Egle, M.; Hilal, S.; Tuladhar, A.M.; Pirpamer, L.; Hofer, E.; Duering, M.; Wason, J.; Morris, R.G.; Dichgans, M.; Schmidt, R.; et al. Prediction of dementia using diffusion tensor MRI measures: The OPTIMAL collaboration. J. Neurol. Neurosurg. Psychiatry 2022, 93, 14–23. [Google Scholar] [CrossRef]
- Iliff, J.J.; Wang, M.; Liao, Y.; Plogg, B.A.; Peng, W.; Gundersen, G.A.; Benveniste, H.; Vates, G.E.; Deane, R.; Goldman, S.A.; et al. A paravascular pathway facilitates CSF flow through the brain parenchyma and the clearance of interstitial solutes, including amyloid β. Sci. Transl. Med. 2012, 4, 147ra111. [Google Scholar] [CrossRef]
- Kress, B.T.; Iliff, J.J.; Xia, M.; Wang, M.; Wei, H.S.; Zeppenfeld, D.; Xie, L.; Kang, H.; Xu, Q.; Liew, J.A.; et al. Impairment of paravascular clearance pathways in the aging brain. Ann. Neurol. 2014, 76, 845–861. [Google Scholar] [CrossRef]
- Ren, Z.; Iliff, J.J.; Yang, L.; Yang, J.; Chen, X.; Chen, M.J.; Giese, R.N.; Wang, B.; Shi, X.; Nedergaard, M. ‘Hit Run’ model of closed-skull traumatic brain injury (TBI) reveals complex patterns of post-traumatic AQP4 dysregulation. J. Cereb. Blood Flow Metab. 2013, 33, 834–845. [Google Scholar] [CrossRef]
- Le Bihan, D.; Mangin, J.F.; Poupon, C.; Clark, C.A.; Pappata, S.; Molko, N.; Chabriat, H. Diffusion tensor imaging: Concepts and applications. J. Magn. Reason. Imaging 2001, 13, 534–546. [Google Scholar] [CrossRef]
- Barzó, P.; Marmarou, A.; Fatouros, P.; Hayasaki, K.; Corwin, F. Contribution of vasogenic and cellular edema to traumatic brain swelling measured by diffusion-weighted imaging. J. Neurosurg. 1997, 87, 900–907. [Google Scholar] [CrossRef]
- Sorensen, A.G.; Buonanno, F.S.; Gonzalez, R.G.; Schwamm, L.H.; Lev, M.H.; Huang-Hellinger, F.R.; Reese, T.G.; Weisskoff, R.M.; Davis, T.L.; Suwanwela, N.; et al. Hyperacute stroke: Evaluation with combined multisection diffusion-weighted and hemodynamically weighted echo-planar MR imaging. Radiology 1996, 199, 391–401. [Google Scholar] [CrossRef]
- Zhuang, B.; Sirajuddin, A.; Zhao, S.; Lu, M. The role of 4D flow MRI for clinical applications in cardiovascular disease: Current status and future perspectives. Quant. Imaging Med. Surg. 2021, 11, 4193–4210. [Google Scholar] [CrossRef]
- Lövblad, K.O.; Baird, A.E.; Schlaug, G.; Benfield, A.; Siewert, B.; Voetsch, B.; Connor, A.; Burzynski, C.; Edelman, R.R.; Warach, S. Ischemic lesion volumes in acute stroke by diffusion-weighted magnetic resonance imaging correlate with clinical outcome. Ann. Neurol. 1997, 42, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Alexandrov, A.V.; Bladin, C.F.; Norris, J.W. Intracranial blood flow velocities in acute ischemic stroke. Stroke 1994, 25, 1378–1383. [Google Scholar] [CrossRef]
- Ha, S.Y.; Kang, Y.; Lee, H.J.; Hwang, M.; Baik, J.; Park, S. Intracranial Flow Velocity Quantification Using Non-Contrast Four-Dimensional Flow MRI: A Prospective Comparative Study with Transcranial Doppler Ultrasound. Diagnostics 2021, 12, 23. [Google Scholar] [CrossRef] [PubMed]
- Mestre, H.; Du, T.; Sweeney, A.M.; Liu, G.; Samson, A.J.; Peng, W.; Mortensen, K.N.; Stæger, F.F.; Bork, P.A.R.; Bashford, L.; et al. Cerebrospinal fluid influx drives acute ischemic tissue swelling. Science 2020, 367, eaax7171. [Google Scholar] [CrossRef] [PubMed]
- Goulay, R.; Flament, J.; Gauberti, M.; Naveau, M.; Pasquet, N.; Gakuba, C.; Emery, E.; Hantraye, P.; Vivien, D.; Aron-Badin, R.; et al. Subarachnoid Hemorrhage Severely Impairs Brain Parenchymal Cerebrospinal Fluid Circulation in Nonhuman Primate. Stroke 2017, 48, 2301–2305. [Google Scholar] [CrossRef]
- Valotassiou, V.; Malamitsi, J.; Papatriantafyllou, J.; Dardiotis, E.; Tsougos, I.; Psimadas, D.; Alexiou, S.; Hadjigeorgiou, G.; Georgoulias, P. SPECT and PET imaging in Alzheimer’s disease. Ann. Nucl. Med. 2018, 32, 583–593. [Google Scholar] [CrossRef]
- van der Vaart, M.G.; Meerwaldt, R.; Slart, R.H.; van Dam, G.M.; Tio, R.A.; Zeebregts, C.J. Application of PET/SPECT imaging in vascular disease. Eur. J. Vasc. Endovasc. Surg. 2008, 35, 507–513. [Google Scholar] [CrossRef][Green Version]
- Goffin, K.; van Laere, K. Single-photon emission tomography. Handb. Clin. Neurol. 2016, 135, 241–250. [Google Scholar] [CrossRef]
- Sigurdsson, B.; Hauglund, N.L.; Lilius, T.O.; Mogensen, F.L.; Mortensen, K.N.; Beschorner, N.; Klinger, L.; Bærentzen, S.L.; Rosenholm, M.P.; Shalgunov, V.; et al. A SPECT-based method for dynamic imaging of the glymphatic system in rats. J. Cereb. Blood Flow Metab. 2023, 43, 1153–1165. [Google Scholar] [CrossRef] [PubMed]
- Xie, L.; Kang, H.; Xu, Q.; Chen, M.J.; Liao, Y.; Thiyagarajan, M.; O’Donnell, J.; Christensen, D.J.; Nicholson, C.; Iliff, J.J.; et al. Sleep drives metabolite clearance from the adult brain. Science 2013, 342, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Lilius, T.O.; Blomqvist, K.; Hauglund, N.L.; Liu, G.; Stæger, F.F.; Bærentzen, S.; Du, T.; Ahlström, F.; Backman, J.T.; Kalso, E.A.; et al. Dexmedetomidine enhances glymphatic brain delivery of intrathecally administered drugs. J. Control. Release 2019, 304, 29–38. [Google Scholar] [CrossRef]
- Nguyen, G.A.H.; Liang, C.; Mukherjee, J. [124I]IBETA: A New Aβ Plaque Positron Emission Tomography Imaging Agent for Alzheimer’s Disease. Molecules 2022, 27, 4552. [Google Scholar] [CrossRef]
- Wang, Y.; Klunk, W.E.; Debnath, M.L.; Huang, G.F.; Holt, D.P.; Shao, L.; Mathis, C.A. Development of a PET/SPECT agent for amyloid imaging in Alzheimer’s disease. J. Mol. Neurosci. 2004, 24, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Lilius, T.O.; Mortensen, K.N.; Deville, C.; Lohela, T.J.; Stæger, F.F.; Sigurdsson, B.; Fiordaliso, E.M.; Rosenholm, M.; Kamphuis, C.; Beekman, F.J.; et al. Glymphatic-assisted perivascular brain delivery of intrathecal small gold nanoparticles. J. Control. Release 2023, 355, 135–148. [Google Scholar] [CrossRef]
- Korhonen, V.; Hiltunen, T.; Myllylä, T.; Wang, X.; Kantola, J.; Nikkinen, J.; Zang, Y.F.; LeVan, P.; Kiviniemi, V. Synchronous multiscale neuroimaging environment for critically sampled physiological analysis of brain function: Hepta-scan concept. Brain Connect 2014, 4, 677–689. [Google Scholar] [CrossRef]
- Kaur, J.; Davoodi-Bojd, E.; Fahmy, L.M.; Zhang, L.; Ding, G.; Hu, J.; Zhang, Z.; Chopp, M.; Jiang, Q. Magnetic Resonance Imaging and Modeling of the Glymphatic System. Diagnostics 2020, 10, 344. [Google Scholar] [CrossRef]
- Iliff, J.J.; Wang, M.; Zeppenfeld, D.M.; Venkataraman, A.; Plog, B.A.; Liao, Y.; Deane, R.; Nedergaard, M. Cerebral arterial pulsation drives paravascular CSF-interstitial fluid exchange in the murine brain. J. Neurosci. 2013, 33, 18190–18199. [Google Scholar] [CrossRef]
- Mestre, H.; Tithof, J.; Du, T.; Song, W.; Peng, W.; Sweeney, A.M.; Olveda, G.; Thomas, J.H.; Nedergaard, M.; Kelley, D.H. Flow of cerebrospinal fluid is driven by arterial pulsations and is reduced in hypertension. Nat. Commun. 2018, 9, 4878. [Google Scholar] [CrossRef]
- Sanderson, M.J.; Smith, I.; Parker, I.; Bootman, M.D. Fluorescence microscopy. Cold Spring Harb. Protoc. 2014, 2014, pdb.top071795. [Google Scholar] [CrossRef] [PubMed]
- Plog, B.A.; Nedergaard, M. The Glymphatic System in Central Nervous System Health and Disease: Past, Present, and Future. Annu. Rev. Pathol. 2018, 13, 379–394. [Google Scholar] [CrossRef] [PubMed]
- Dunst, S.; Tomancak, P. Imaging Flies by Fluorescence Microscopy: Principles, Technologies, and Applications. Genetics 2019, 211, 15–34. [Google Scholar] [CrossRef]
- Wu, X.; Li, J.R.; Fu, Y.; Chen, D.Y.; Nie, H.; Tang, Z.P. From static to dynamic: Live observation of the support system after ischemic stroke by two photon-excited fluorescence laser-scanning microscopy. Neural. Regen. Res. 2023, 18, 2093–2107. [Google Scholar] [CrossRef]
- Li, J.; Wu, X.; Fu, Y.; Nie, H.; Tang, Z. Two-photon microscopy: Application advantages and latest progress for. Rev. Neurosci. 2023, 34, 559–572. [Google Scholar] [CrossRef]
- Helmchen, F.; Kleinfeld, D. Chapter 10. In vivo measurements of blood flow and glial cell function with two-photon laser-scanning microscopy. Methods Enzymol. 2008, 444, 231–254. [Google Scholar] [CrossRef]
- De, A.K.; Goswami, D. Adding new dimensions to laser-scanning fluorescence microscopy. J. Microsc. 2009, 233, 320–325. [Google Scholar] [CrossRef] [PubMed]
- MacRitchie, N.; Maffia, P. Light sheet fluorescence microscopy for quantitative three-dimensional imaging of vascular remodelling. Cardiovasc. Res. 2021, 117, 348–350. [Google Scholar] [CrossRef] [PubMed]
- Jermyn, M.; Kolste, K.; Pichette, J.; Sheehy, G.; Angulo-Rodríguez, L.; Paulsen, K.D.; Roberts, D.W.; Wilson, B.C.; Petrecca, K.; Leblond, F. Macroscopic-imaging technique for subsurface quantification of near-infrared markers during surgery. J. Biomed. Opt. 2015, 20, 036014. [Google Scholar] [CrossRef][Green Version]
- Lukina, M.; Yashin, K.; Kiseleva, E.E.; Alekseeva, A.; Dudenkova, V.; Zagaynova, E.V.; Bederina, E.; Medyanic, I.; Becker, W.; Mishra, D.; et al. Label-Free Macroscopic Fluorescence Lifetime Imaging of Brain Tumors. Front. Oncol. 2021, 11, 666059. [Google Scholar] [CrossRef]
- Yuan, Y.; Yan, Z.; Miao, J.; Cai, R.; Zhang, M.; Wang, Y.; Wang, L.; Dang, W.; Wang, D.; Xiang, D.; et al. Autofluorescence of NADH is a new biomarker for sorting and characterizing cancer stem cells in human glioma. Stem. Cell Res. Ther. 2019, 10, 330. [Google Scholar] [CrossRef]
- Shcheslavskiy, V.I.; Shirmanova, M.V.; Dudenkova, V.V.; Lukyanov, K.A.; Gavrina, A.I.; Shumilova, A.V.; Zagaynova, E.; Becker, W. Fluorescence time-resolved macroimaging. Opt. Lett. 2018, 43, 3152–3155. [Google Scholar] [CrossRef]
- Erkkilä, M.T.; Reichert, D.; Gesperger, J.; Kiesel, B.; Roetzer, T.; Mercea, P.A.; Drexler, W.; Unterhuber, A.; Leitgeb, R.A.; Woehrer, A.; et al. Macroscopic fluorescence-lifetime imaging of NADH and protoporphyrin IX improves the detection and grading of 5-aminolevulinic acid-stained brain tumors. Sci. Rep. 2020, 10, 20492. [Google Scholar] [CrossRef] [PubMed]
- Harrison, I.F.; Ismail, O.; Machhada, A.; Colgan, N.; Ohene, Y.; Nahavandi, P.; Ahmed, Z.; Fisher, A.; Meftah, S.; Murray, T.K.; et al. Impaired glymphatic function and clearance of tau in an Alzheimer’s disease model. Brain 2020, 143, 2576–2593. [Google Scholar] [CrossRef]
- Wagnières, G.A.; Star, W.M.; Wilson, B.C. In vivo fluorescence spectroscopy and imaging for oncological applications. Photochem. Photobiol. 1998, 68, 603–632. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Butte, P.V.; Mamelak, A.N.; Nuno, M.; Bannykh, S.I.; Black, K.L.; Marcu, L. Fluorescence lifetime spectroscopy for guided therapy of brain tumors. Neuroimage 2011, 54, S125–S135. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thakkar, R.N.; Kioutchoukova, I.P.; Griffin, I.; Foster, D.T.; Sharma, P.; Valero, E.M.; Lucke-Wold, B. Mapping the Glymphatic Pathway Using Imaging Advances. J 2023, 6, 477-491. https://doi.org/10.3390/j6030031
Thakkar RN, Kioutchoukova IP, Griffin I, Foster DT, Sharma P, Valero EM, Lucke-Wold B. Mapping the Glymphatic Pathway Using Imaging Advances. J. 2023; 6(3):477-491. https://doi.org/10.3390/j6030031
Chicago/Turabian StyleThakkar, Rajvi N., Ivelina P. Kioutchoukova, Ian Griffin, Devon T. Foster, Pratiksha Sharma, Eduardo Molina Valero, and Brandon Lucke-Wold. 2023. "Mapping the Glymphatic Pathway Using Imaging Advances" J 6, no. 3: 477-491. https://doi.org/10.3390/j6030031
APA StyleThakkar, R. N., Kioutchoukova, I. P., Griffin, I., Foster, D. T., Sharma, P., Valero, E. M., & Lucke-Wold, B. (2023). Mapping the Glymphatic Pathway Using Imaging Advances. J, 6(3), 477-491. https://doi.org/10.3390/j6030031