
Prognostic Factors after Hepatectomy for Hepatocellular Carcinoma—The Importance of Pathological Immunophenotyping, the Steatohepatitic Subtype and the Impact of the Hepatic Pedicle Clamping


 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Operative Details
2.4. Morbidity and Mortality
2.5. Post-Operative Follow-Up
2.6. Histopathological Analysis
2.6.1. Non-Tumoral Parenchyma
2.6.2. Immunohistochemical Staining
2.7. Statistical Analysis
3. Results
3.1. Morbidity and Mortality
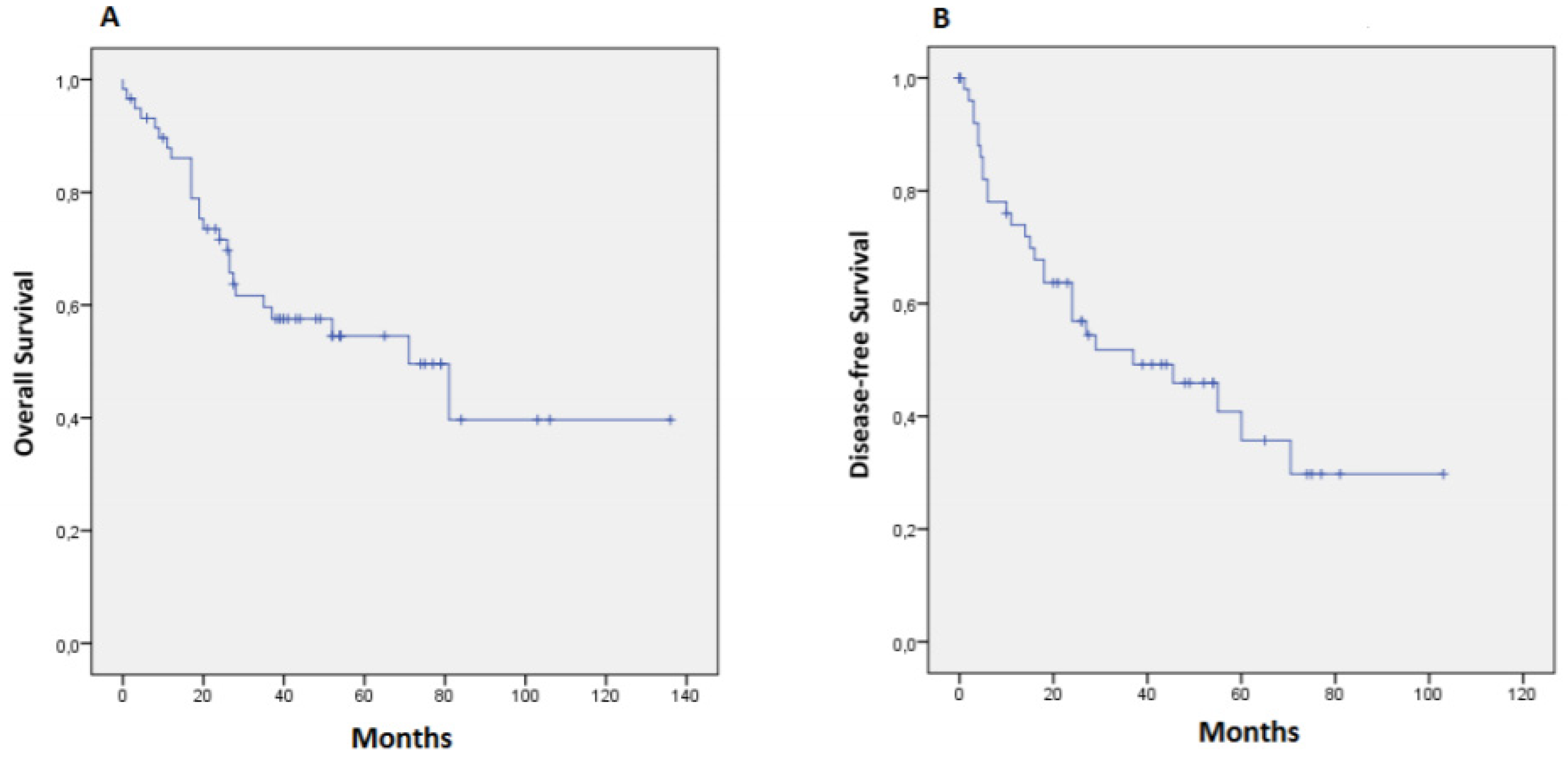
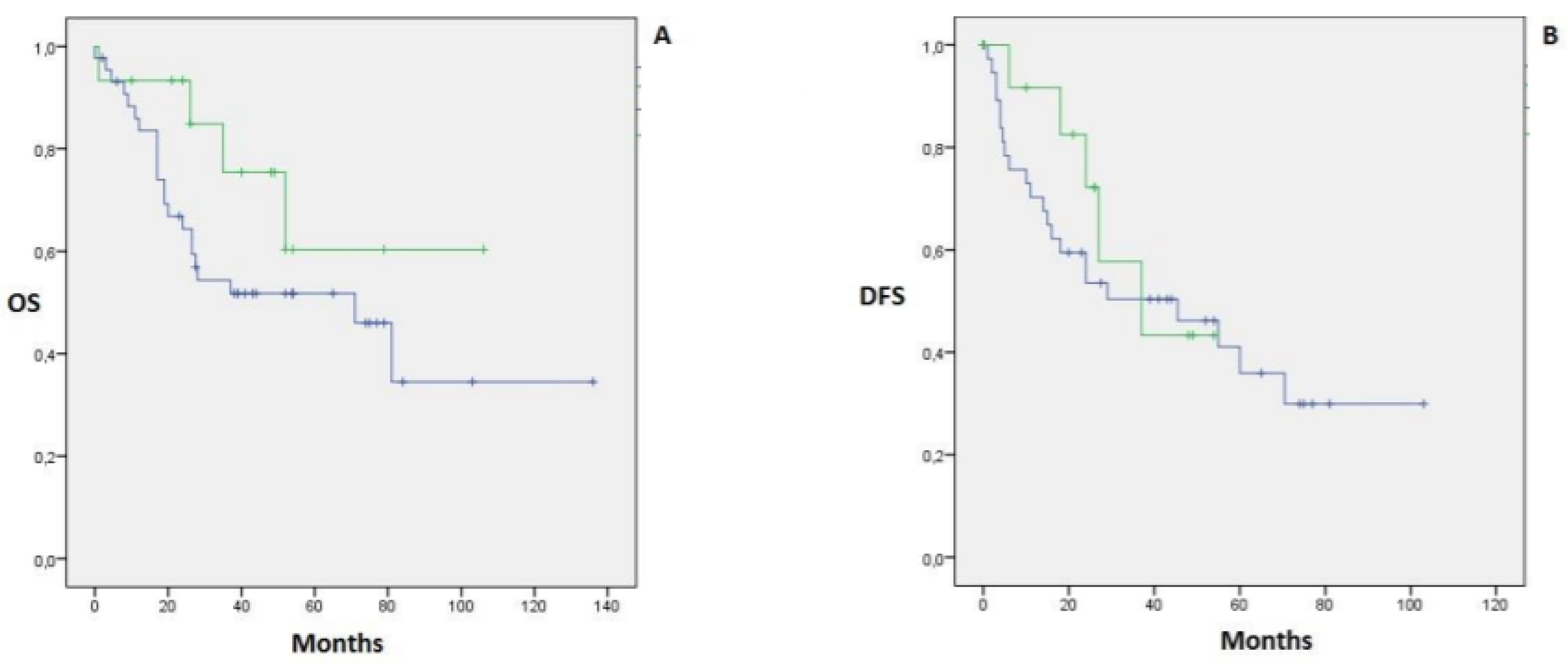
3.2. Overall and Disease-Free Survival
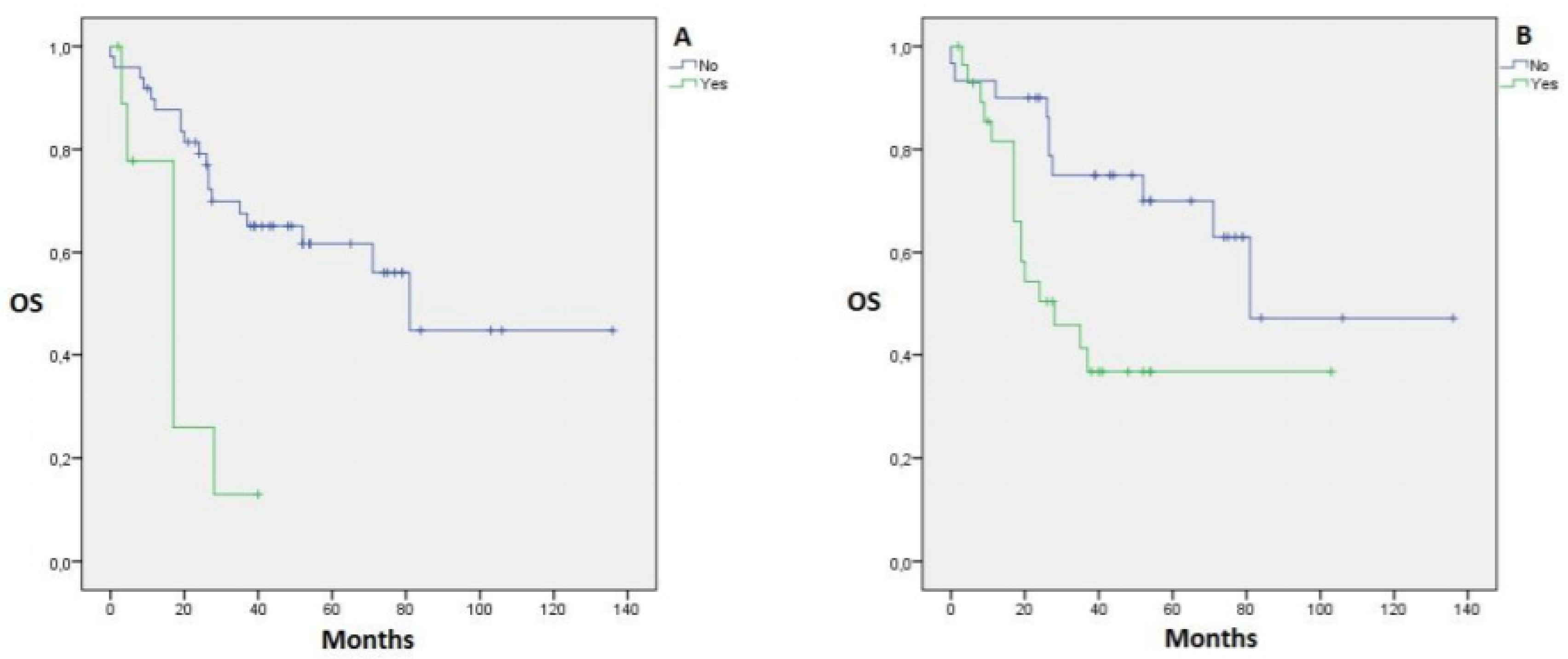
3.3. Clinical and Operative Factors with Impact on Survival
3.4. Pathologic Factors with Impact on Survival
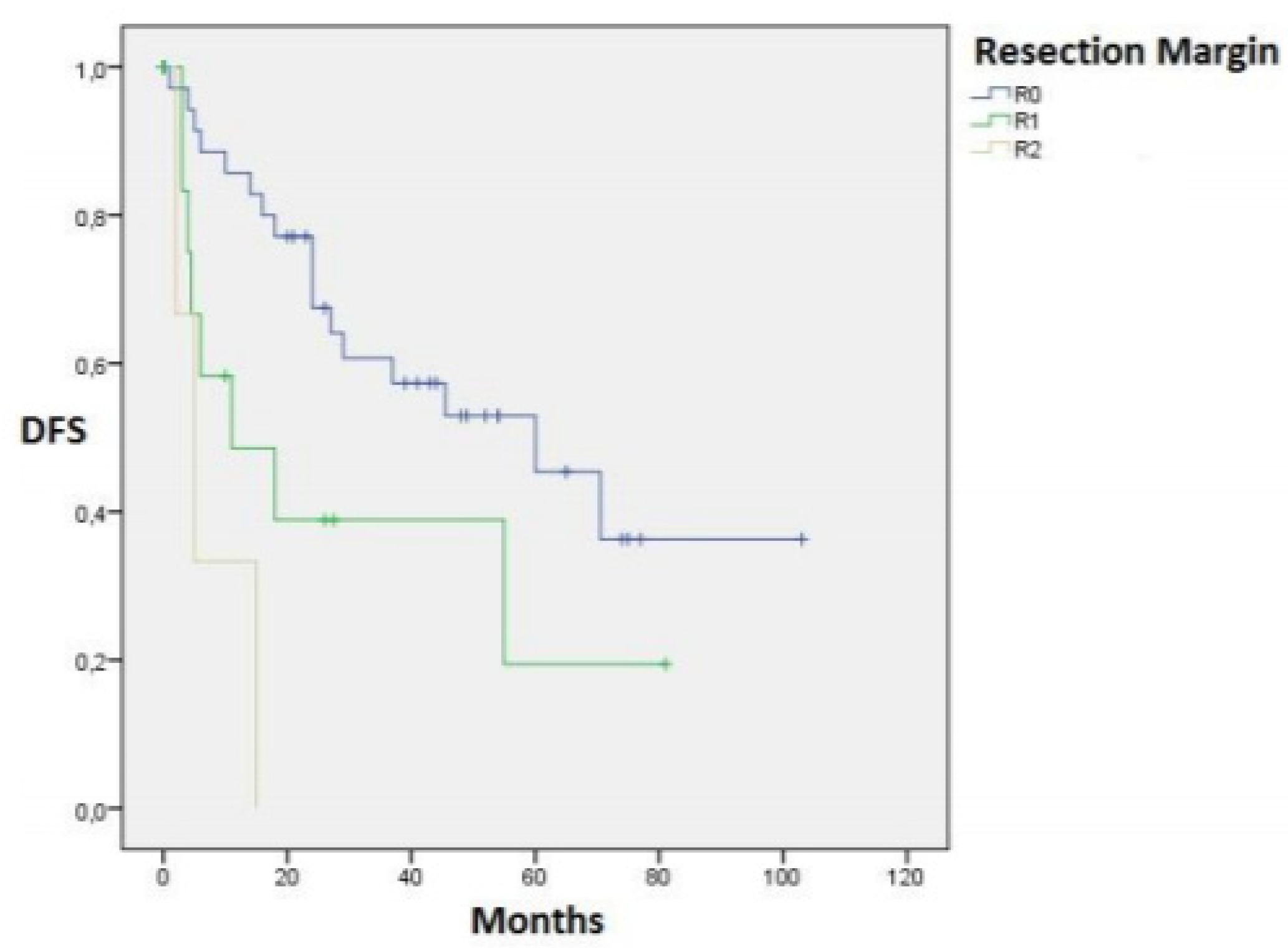
3.4.1. Resection Margins
3.4.2. Non-Tumoral Parenchyma
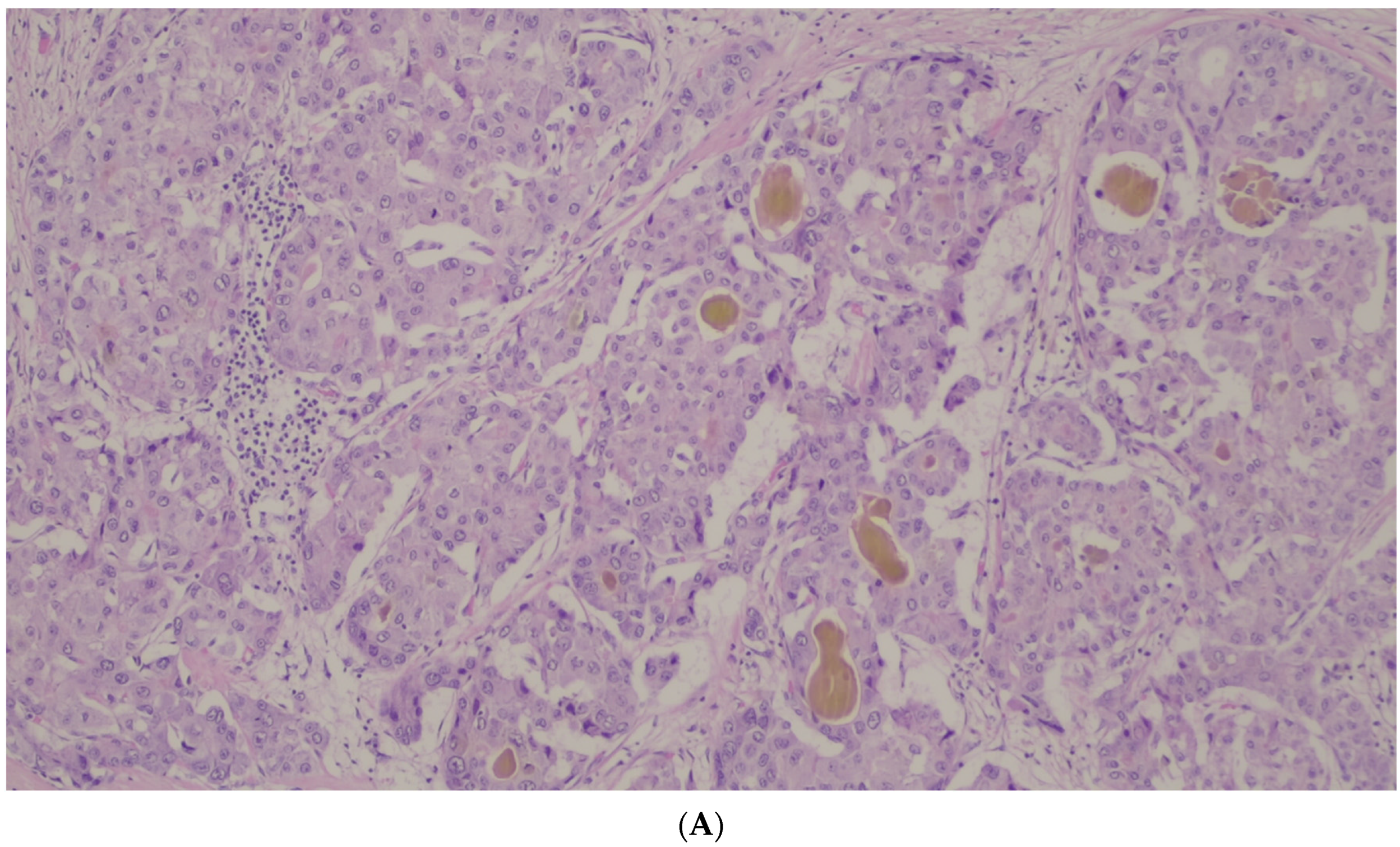
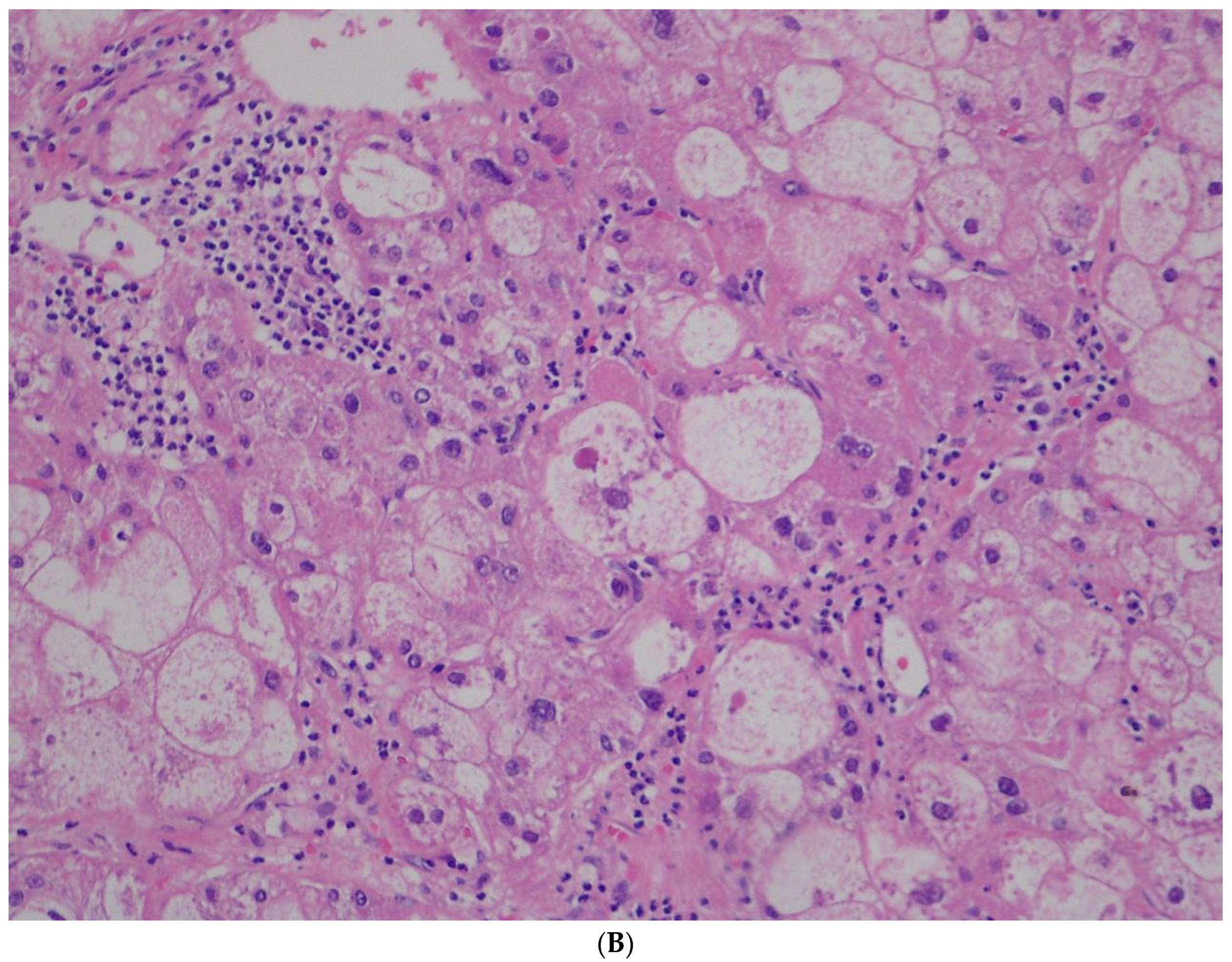
3.4.3. Tumoral Parenchyma
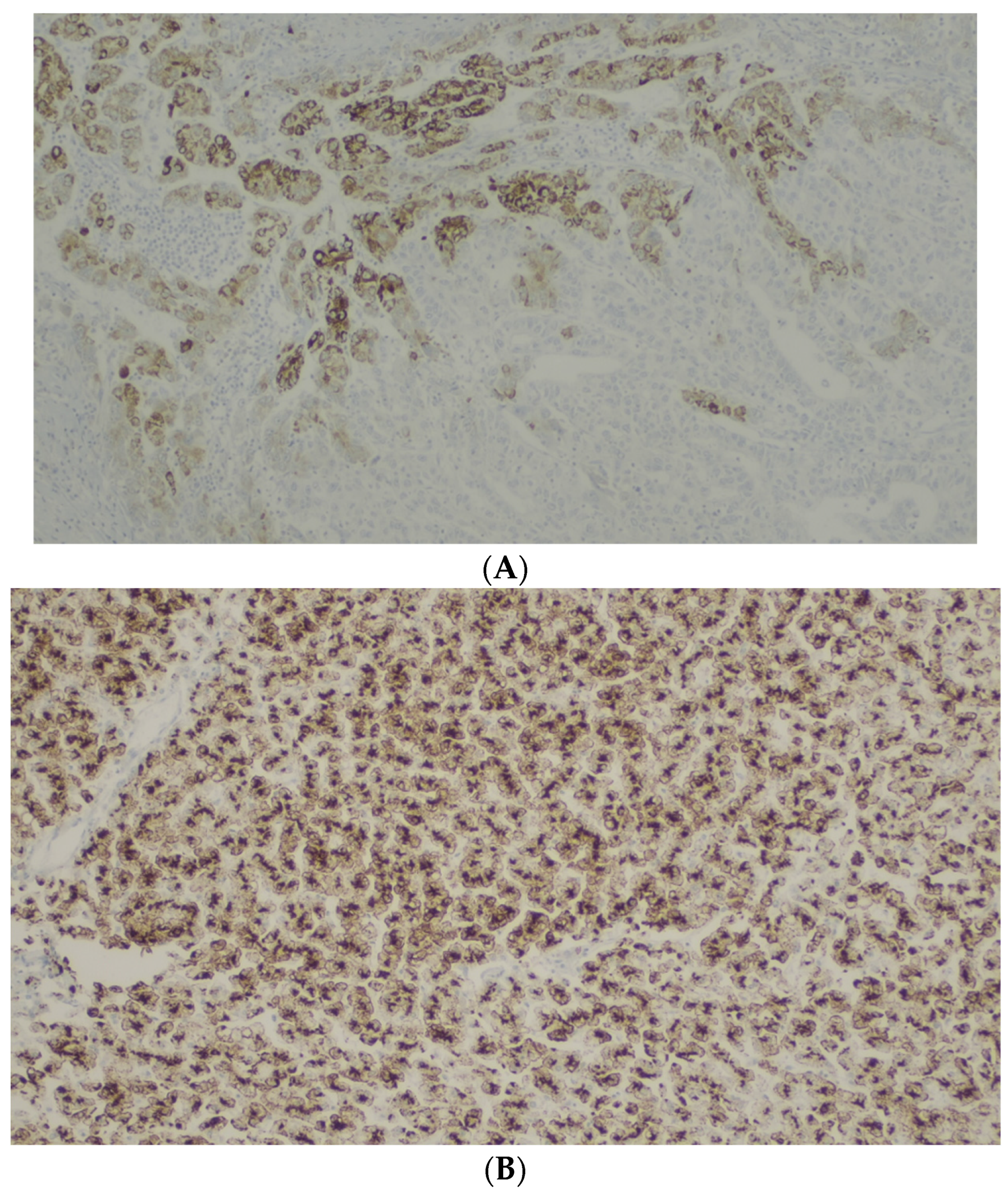
3.4.4. Immunohistochemical Staining
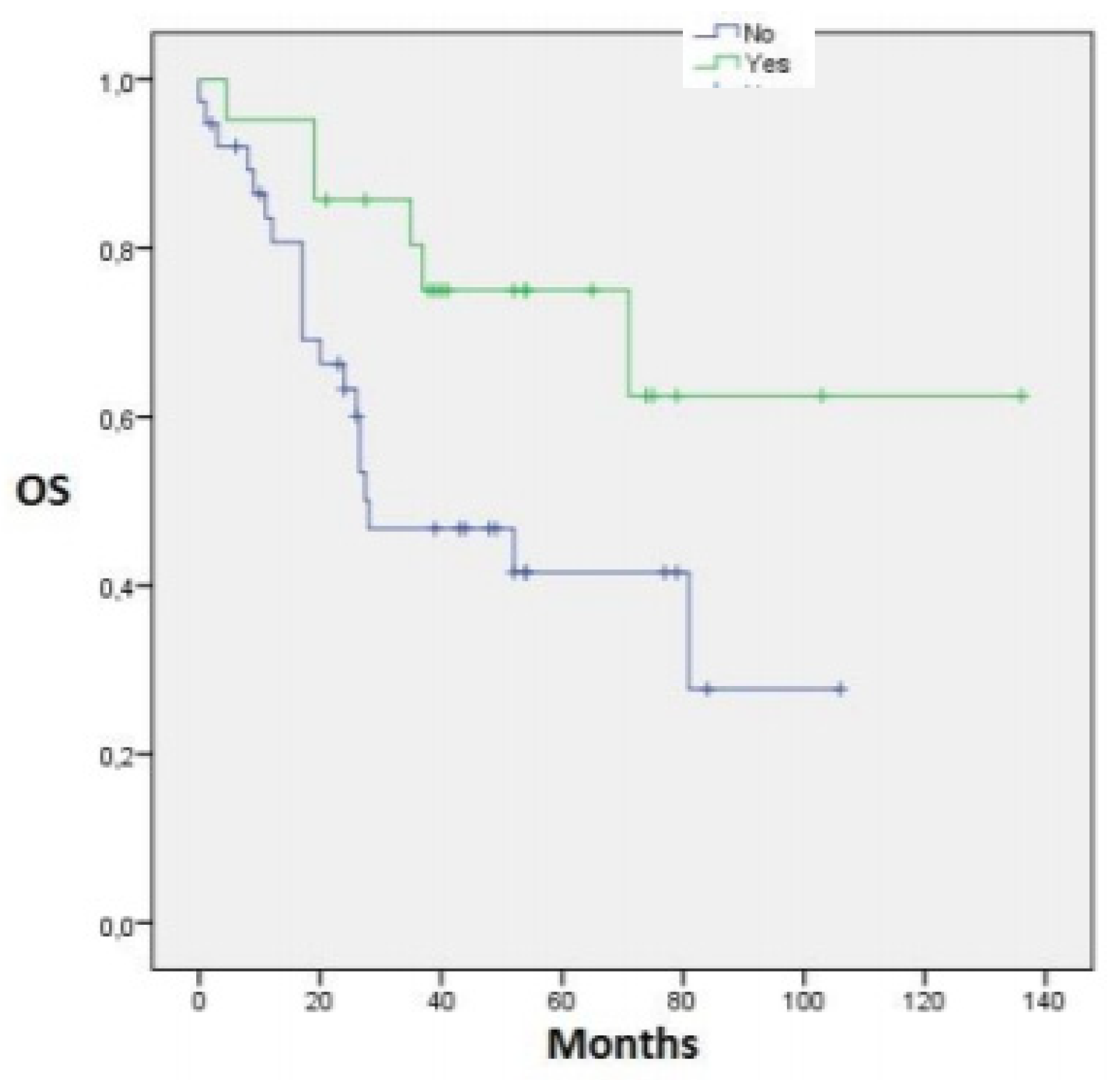
3.5. Cox Regression
3.5.1. Overall Survival
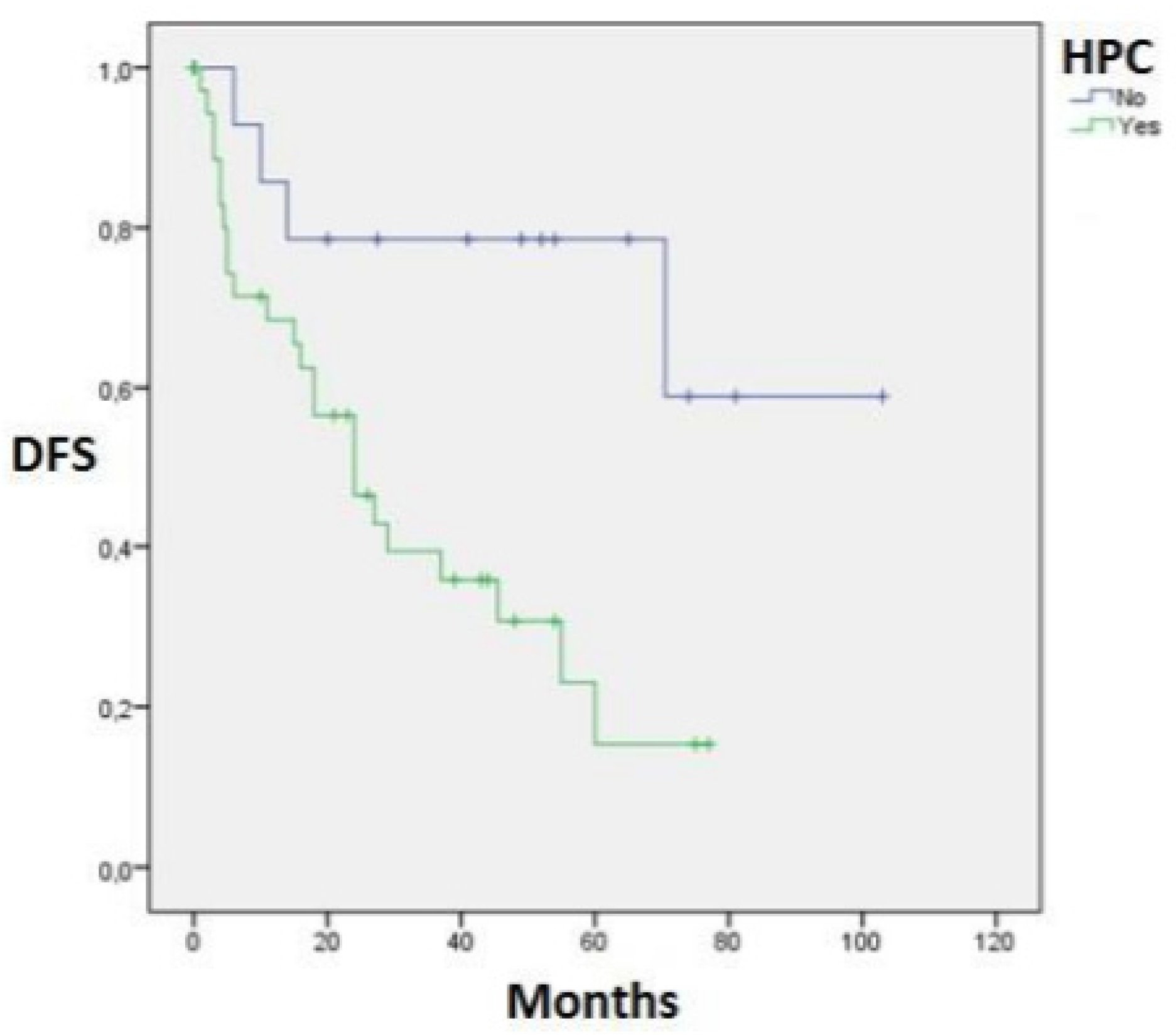
3.5.2. Disease-Free Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rawla, P.; Sunkara, T.; Muralidharan, P.; Raj, J.P. Update in global trends and aetiology of hepatocellular carcinoma. Wspolczesna Onkol. 2018, 22, 141–150. [Google Scholar] [CrossRef]
- Singal, A.G.; El-Serag, H.B. Hepatocellular Carcinoma from Epidemiology to Prevention: Translating Knowledge into Practice. Clin. Gastroenterol. Hepatol. 2015, 13, 2140–2151. [Google Scholar] [CrossRef]
- Harnois, D.M. Hepatitis C virus infection and the rising incidence of hepatocellular carcinoma. Mayo Clin. Proc. 2012, 87, 7–8. [Google Scholar] [CrossRef]
- Cholankeril, G.; Patel, R.; Khurana, S.; Satapathy, S.K. Hepatocellular carcinoma in non-alcoholic steatohepatitis: Current knowledge and implications for management. World J. Hepatol. 2017, 9, 533–543. [Google Scholar] [CrossRef]
- Rahman, R. Primary hepatocellular carcinoma and metabolic syndrome: An update. World J. Gastrointest. Oncol. 2013, 5, 186. [Google Scholar] [CrossRef]
- Tsoulfas, G. Hepatocellular carcinoma and metabolic syndrome: The times are changing and so should we. World J. Gastroenterol. 2019, 25, 3842–3848. [Google Scholar] [CrossRef]
- Siegel, A.B.; Zhu, A.X. Metabolic syndrome and hepatocellular carcinoma: Two growing epidemics with a potential link. Cancer 2009, 115, 5651–5661. [Google Scholar] [CrossRef]
- Madkhali, A.A.; Fadel, Z.T.; Aljiffry, M.M.; Hassanain, M.M. Surgical treatment for hepatocellular carcinoma. Saudi J. Gastroenterol. 2015, 21, 11–17. [Google Scholar] [CrossRef]
- Zamora-Valdes, D.; Taner, T.; Nagorney, D.M. Surgical Treatment of Hepatocellular Carcinoma. Cancer Control 2017, 24, 1073274817729258. [Google Scholar] [CrossRef]
- Feng, X.; Liu, Z.; Zheng, S.; Dong, J.; Li, X. The Pringle manoeuvre should be avoided in hepatectomy for cancer patients due to its side effects on tumor recurrence and worse prognosis. Med. Hypotheses 2009, 72, 398–401. [Google Scholar] [CrossRef]
- Wei, X.; Zheng, W.; Yang, Z.; Liu, H.; Tang, T.; Li, X.; Liu, X. Effect of the intermittent Pringle maneuver on liver damage after hepatectomy: A retrospective cohort study. World J. Surg. Oncol. 2019, 17, 142. [Google Scholar] [CrossRef]
- Al-Saeedi, M.; Ghamarnejad, O.; Khajeh, E.; Shafiei, S.; Salehpour, R.; Golriz, M.; Mieth, M.; Weiss, K.H.; Longerich, T.; Hoffmann, K.; et al. Pringle Maneuver in Extended Liver Resection: A propensity score analysis. Sci. Rep. 2020, 10, 108847. [Google Scholar] [CrossRef]
- Hamaguchi, Y.; Mori, A.; Fujimoto, Y.; Ito, T.; Iida, T.; Yagi, S.; Okajima, H.; Kaido, T.; Uemoto, S. Longer warm ischemia can accelerate tumor growth through the induction of HIF-1α and the IL-6-JAK-STAT3 signaling pathway in a rat hepatocellular carcinoma model. J. Hepato-Biliary-Pancreat. Sci. 2016, 23, 771–779. [Google Scholar] [CrossRef]
- Colecchia, A.; Schiumerini, R.; Cucchetti, A.; Cescon, M.; Taddia, M.; Marasco, G.; Festi, D. Prognostic factors for hepatocellular carcinoma recurrence. World J. Gastroenterol. 2014, 20, 5935–5950. [Google Scholar] [CrossRef]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; the WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology 2019, 76, 182–188. [Google Scholar] [CrossRef]
- Arnaoutakis, D.J.; Mavros, M.N.; Shen, F.; Alexandrescu, S.; Firoozmand, A.; Popescu, I.; Weiss, M.; Wolfgang, C.L.; Choti, M.A.; Pawlik, T.M. Recurrence patterns and prognostic factors in patients with hepatocellular carcinoma in noncirrhotic liver: A multi-institutional analysis. Ann. Surg. Oncol. 2014, 21, 147–154. [Google Scholar] [CrossRef]
- Olofson, A.M.; Gonzalo, D.H.; Chang, M.; Liu, X. Steatohepatitic Variant of Hepatocellular Carcinoma: A Focused Review. Gastroenterol. Res. 2018, 11, 391–396. [Google Scholar] [CrossRef]
- Yeh, M.M.; Liu, Y.; Torbenson, M. Steatohepatitic variant of hepatocellular carcinoma in the absence of metabolic syndrome or background steatosis: A clinical, pathological, and genetic study. Hum. Pathol. 2015, 46, 1769–1775. [Google Scholar] [CrossRef]
- Shibahara, J.; Ando, S.; Sakamoto, Y.; Kokudo, N.; Fukayama, M. Hepatocellular carcinoma with steatohepatitic features: A clinicopathological study of Japanese patients. Histopathology 2014, 64, 951–962. [Google Scholar] [CrossRef]
- Boulter, L.; Lu, W.Y.; Forbes, S.J. Differentiation of progenitors in the liver: A matter of local choice. J. Clin. Investig. 2013, 123, 1867–1873. [Google Scholar] [CrossRef]
- Lo, R.C.L.; Ng, I.O.L. Hepatocellular tumors: Immunohistochemical analyses for classification and prognostication. Chin. J. Cancer Res. 2011, 23, 245–253. [Google Scholar] [CrossRef]
- Li, J.; Gao, J.Z.; Du, J.L.; Wei, L.X. Prognostic and clinicopathological significance of glypican-3 overexpression in hepatocellular carcinoma: A meta-analysis. World J. Gastroenterol. 2014, 20, 6336–6344. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, M.; Ma, H.; Song, X.; He, L.; Ye, X.; Li, X. Overexpression of glypican-3 is a predictor of poor prognosis in hepatocellular carcinoma an updated meta-analysis. Medicine 2018, 97, e11130. [Google Scholar] [CrossRef]
- Martins, J.; Alexandrino, H.; Oliveira, R.; Cipriano, M.A.; Falcão, D.; Ferreira, L.; Martins, R.; Serôdio, M.; Martins, M.; Tralhão, J.G.; et al. Sinusoidal dilation increases the risk of complications in hepatectomy for CRCLM—Protective effect of bevacizumab and diabetes mellitus, serum gamma-glutamyltranspeptidase as predictive factor. Eur. J. Surg. Oncol. 2016, 42, 713–721. [Google Scholar] [CrossRef]
- Ha, S.Y.; Choi, M.; Lee, T.; Park, C.K. The prognostic role of mitotic index in hepatocellular carcinoma patients after curative hepatectomy. Cancer Res. Treat. 2016, 48, 180–189. [Google Scholar] [CrossRef]
- Bedossa, P.; Poynard, T. An algorithm for the grading of activity in chronic hepatitis C. Hepatology 1996, 24, 289–293. [Google Scholar] [CrossRef]
- Ishak, K.; Baptista, A.; Bianchi, L.; Callea, F.; De Groote, J.; Gudat, F.; Denk, H.; Desmet, V.; Korb, G.; MacSween, R.N.; et al. Histological grading and staging of chronic hepatitis. J. Hepatol. 1995, 22, 696–699. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.-C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef]
- Shirakawa, H.; Kuronuma, T.; Nishimura, Y.; Hasebe, T.; Nakano, M.; Gotohda, N.; Takahashi, S.; Nakagohri, T.; Konishi, M.; Kobayashi, N.; et al. Glypican-3 is a useful diagnostic marker for a component of hepatocellular carcinoma in human liver cancer. Int. J. Oncol. 2009, 34, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Tsoulfas, G.; Agorastou, P.; Tooulias, A.; Marakis, G.N. Current and future challenges in the surgical treatment of hepatocellular carcinoma: A review. Int. Surg. 2014, 99, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Torzilli, G.; Belghiti, J.; Kokudo, N.; Takayama, T.; Capussotti, L.; Nuzzo, G.; Vauthey, J.-N.; Choti, M.A.; De Santibanes, E.; Donadon, M.; et al. A snapshot of the effective indications and results of surgery for hepatocellular carcinoma in tertiary referral centers: Is it adherent to the EASL/AASLD recommendations? An observational study of the HCC east-west study group. Ann. Surg. 2013, 257, 929–937. [Google Scholar] [CrossRef]
- Belli, A.; Cioffi, L.; Russo, G.; Belli, G. Liver resection for hepatocellular carcinoma in patients with portal hypertension: The role of laparoscopy. Hepatobiliary Surg. Nutr. 2015, 4, 417–41721. [Google Scholar] [CrossRef]
- Utsunomiya, T.; Shimada, M.; Kudo, M.; Ichida, T.; Matsui, O.; Izumi, N.; Matsuyama, Y.; Sakamoto, M.; Nakashima, O.; Ku, Y.; et al. A comparison of the surgical outcomes among patients with HBV-positive, HCV-positive, and non-B non-C hepatocellular carcinoma: A nationwide study of 11,950 patients. Ann. Surg. 2015, 261, 513–520. [Google Scholar] [CrossRef]
- Imamura, H.; Matsuyama, Y.; Tanaka, E.; Ohkubo, T.; Hasegawa, K.; Miyagawa, S.; Sugawara, Y.; Minagawa, M.; Takayama, T.; Kawasaki, S.; et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J. Hepatol. 2003, 38, 200–207. [Google Scholar] [CrossRef]
- Zhou, Y.; Si, X.; Wu, L.; Su, X.; Li, B.; Zhang, Z. Influence of viral hepatitis status on prognosis in patients undergoing hepatic resection for hepatocellular carcinoma: A meta-analysis of observational studies. World J. Surg. Oncol. 2011, 9, 108. [Google Scholar] [CrossRef]
- Miyagawa, S.; Kawasaki, S.; Makuuchi, M. Comparison of the characteristics of hepatocellular carcinoma between hepatitis B and C viral infection: Tumor multicentricity in cirrhotic liver with hepatitis C. Hepatology 1996, 24, 307–310. [Google Scholar] [CrossRef]
- Dufour, J.F.; Anstee, Q.M.; Bugianesi, E.; Harrison, S.; Loomba, R.; Paradis, V.; Tilg, H.; Wong, V.W.-S.; Zelber-Sagi, S. Current therapies and new developments in NASH. Gut 2022, 71, 2123–2134. [Google Scholar] [CrossRef]
- Heyens, L.J.M.; Busschots, D.; Koek, G.H.; Robaeys, G.; Francque, S. Liver Fibrosis in Non-alcoholic Fatty Liver Disease: From Liver Biopsy to Non-invasive Biomarkers in Diagnosis and Treatment. Front. Med. 2021, 8, 615978. [Google Scholar] [CrossRef]
- Schwabe, R.F.; Tabas, I.; Pajvani, U.B. Mechanisms of Fibrosis Development in NASH. Gastroenterology 2020, 158, 1913. [Google Scholar] [CrossRef]
- Tralhão, J.G.; Hoti, E.; Oliveiros, B.; Abrantes, A.M.; Botelho, M.F.; Castro-Sousa, F. Intermittent pringle maneuver and hepatic function: Perioperative monitoring by noninvasive ICG-clearance. World J. Surg. 2009, 33, 2627–2634. [Google Scholar] [CrossRef]
- Alexandrino, H.; Varela, A.T.; Teodoro, J.S.; Martins, M.A.; Rolo, A.P.; Tralhão, J.G.; Palmeira, C.M.; e Sousa, F.C. Mitochondrial bioenergetics and posthepatectomy liver dysfunction. Eur. J. Clin. Investig. 2016, 46, 627–635. [Google Scholar] [CrossRef]
- Hao, S.; Chen, S.; Yang, X.; Wan, C. Impact of intermittent portal clamping on the early recurrence of hepatocellular carcinoma after surgery. Surg. Today 2016, 46, 1290–1295. [Google Scholar] [CrossRef]
- Hao, S.; Chen, S.; Yang, X.; Wan, C. Adverse impact of intermittent portal clamping on long-term postoperative outcomes in hepatocellular carcinoma. Ann. R. Coll. Surg. Engl. 2017, 99, 22–27. [Google Scholar] [CrossRef]
- Ozaki, M.; Todo, S. Surgical stress and tumor behavior: Impact of ischemia-reperfusion and hepatic resection on tumor progression. Liver Transplant. 2007, 13, 1623–1626. [Google Scholar] [CrossRef]
- Man, K.; Ng, K.T.; Lo, C.M.; Ho, J.W.; Sun, B.S.; Sun, C.K.; Lee, T.K.; Poon, R.T.P.; Fan, S.T. Ischemia-reperfusion of small liver remnant promotes liver tumor growth and metastases—Activation of cell invasion and migration pathways. Liver Transplant. 2007, 13, 1669–1677. [Google Scholar] [CrossRef]
- Xiaobin, F.; Shuguo, Z.; Jian, Z.; Yudong, Q.; Lijian, L.; Kuansheng, M.; Xiaowu, L.; Feng, X.; Dong, Y.; Shuguang, W.; et al. Effect of the pringle maneuver on tumor recurrence of hepatocellular carcinoma after curative resection (EPTRH): A randomized, prospective, controlled multicenter trial. BMC Cancer 2012, 12, 340. [Google Scholar] [CrossRef]
- Laurent, C.; Blanc, J.F.; Nobili, S.; Cunha, A.S.; le Bail, B.; Bioulac-Sage, P.; Balabaud, C.; Capdepont, M.; Saric, J. Prognostic factors and longterm survival after hepatic resection for hepatocellular carcinoma originating from noncirrhotic liver. J. Am. Coll. Surg. 2005, 201, 656–662. [Google Scholar] [CrossRef]
- Poon, R.T.P.; Fan, S.T.; Ng, I.O.L.; Wong, J. Significance of resection margin in hepatectomy for hepatocellular carcinoma: A critical reappraisal. Ann. Surg. 2000, 231, 544–551. [Google Scholar] [CrossRef]
- Shimada, K.; Sakamoto, Y.; Esaki, M.; Kosuge, T.; Morizane, C.; Ikeda, M.; Ueno, H.; Okusaka, T.; Arai, Y.; Takayasu, K. Analysis of prognostic factors affecting survival after initial recurrence and treatment efficacy for recurrence in patients undergoing potentially curative hepatectomy for hepatocellular carcinoma. Ann. Surg. Oncol. 2007, 14, 2337–2347. [Google Scholar] [CrossRef]
- Salomao, M.; Remotti, H.; Vaughan, R.; Siegel, A.B.; Lefkowitch, J.H.; Moreira, R.K. The steatohepatitic variant of hepatocellular carcinoma and its association with underlying steatohepatitis. Hum. Pathol. 2012, 43, 737–746. [Google Scholar] [CrossRef]
- Jain, D.; Nayak, N.C.; Kumaran, V.; Saigal, S. Steatohepatitic hepatocellular carcinoma, a morphologic indicator of associated metabolic risk factors: A study from India. Arch. Pathol. Lab. Med. 2013, 137, 961–966. [Google Scholar] [CrossRef]
- Chan, A.W.H.; Yu, S.; Yu, Y.H.; Tong, J.H.M.; Wang, L.; Tin, E.K.Y.; Chong, C.C.N.; Chan, S.L.; Wong, G.L.H.; Wong, V.W.S.; et al. Steatotic hepatocellular carcinoma: A variant associated with metabolic factors and late tumour relapse. Histopathology 2016, 69, 971–984. [Google Scholar] [CrossRef]
- Raposo, L.; Severo, M.; Barros, H.; Santos, A.C. The prevalence of the metabolic syndrome in Portugal: The PORMETS study. BMC Public Health 2017, 17, 555. [Google Scholar] [CrossRef]
- Uenishi, T.; Kubo, S.; Yamamoto, T.; Shuto, T.; Ogawa, M.; Tanaka, H.; Tanaka, S.; Kaneda, K.; Hirohashi, K. Cytokeratin 19 expression in hepatocellular carcinoma predicts early postoperative recurrence. Cancer Sci. 2003, 94, 851–857. [Google Scholar] [CrossRef]
- Lee JIl Lee, J.-W.; Kim, J.M.; Kim, J.K.; Chung, H.J.; Kim, Y.S. Prognosis of hepatocellular carcinoma expressing cytokeratin 19: Comparison with other liver cancers. World J. Gastroenterol. 2012, 18, 4751–4757. [Google Scholar] [CrossRef]
- Lu, X.Y.; Xi, T.; Lau, W.Y.; Dong, H.; Zhu, Z.; Shen, F.; Wu, M.-C.; Cong, W.-M. Hepatocellular carcinoma expressing cholangiocyte phenotype is a novel subtype with highly aggressive behavior. Ann. Surg. Oncol. 2011, 18, 2210–2217. [Google Scholar] [CrossRef]
- Xue, R.; Feng, J.; Meng, Q.; Lv, F.; Zhu, Y.; Yu, H.; Zhang, S.; Song, C.; Sun, L.; Yue, Z.; et al. The significance of glypican-3 expression profiling in the tumor cellular origin theoretical system for hepatocellular carcinoma progression. J. Gastroenterol. Hepatol. 2017, 32, 1503–1511. [Google Scholar] [CrossRef]
- Wu, Y.; Liu, H.; Ding, H.-G. GPC-3 in hepatocellular carcinoma: Current perspectives. J. Hepatocell. Carcinoma 2016, 3, 63–67. [Google Scholar] [CrossRef]
- Feng, J.; Zhu, R.; Chang, C.; Yu, L.; Cao, F.; Zhu, G.; Chen, F.; Xia, H.; Lv, F.; Zhang, S.; et al. CK19 and glypican 3 expression profiling in the prognostic indication for patients with HCC after surgical resection. PLoS ONE 2016, 11, e0151501. [Google Scholar] [CrossRef]
- Srivastava, S.; Wong, K.F.; Ong, C.W.; Huak, C.Y.; Yeoh, K.G.; Teh, M.; Luk, J.M.; Salto-Tellez, M. A morpho-molecular prognostic model for hepatocellular carcinoma. Br. J. Cancer 2012, 107, 334–339. [Google Scholar] [CrossRef]
- Tsujikawa, H.; Masugi, Y.; Yamazaki, K.; Itano, O.; Kitagawa, Y.; Sakamoto, M. Immunohistochemical molecular analysis indicates hepatocellular carcinoma subgroups that reflect tumor aggressiveness. Hum. Pathol. 2016, 50, 24–33. [Google Scholar] [CrossRef]
- Caetano Oliveira, R.; Martins, R.; Abrantes, A.M.; Jesus, Â.; Teixeira, P.; Canhoto, C.; Guerreiro, P.; Costa, B.; Silva, M.R.; Tralhão, J.G.; et al. Morphophenotypic Classification of Hepatocellular Carcinoma: The Biliary/Stem Cell Subgroup and Worst Outcome—Implications on Patient Selection. J. Gastrointest. Surg. 2020, 25, 698–707. [Google Scholar] [CrossRef]
- Zhuo, J.Y.; Lu, D.; Tan, W.Y.; Zheng, S.S.; Shen, Y.Q.; Xu, X. CK19-positive Hepatocellular Carcinoma is a Characteristic Subtype. J. Cancer 2020, 11, 5069–5077. [Google Scholar] [CrossRef]
- Moldogazieva, N.T.; Mokhosoev, I.M.; Zavadskiy, S.P.; Terentiev, A.A. Proteomic Profiling and Artificial Intelligence for Hepatocellular Carcinoma Translational Medicine. Biomedicines 2021, 9, 159. [Google Scholar] [CrossRef]
- Allaume, P.; Rabilloud, N.; Turlin, B.; Bardou-Jacquet, E.; Loréal, O.; Calderaro, J.; Khene, Z.-E.; Acosta, O.; De Crevoisier, R.; Rioux-Leclercq, N.; et al. Artificial Intelligence-Based Opportunities in Liver Pathology—A Systematic Review. Diagnostics 2023, 13, 1799. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hepatectomies | |
| Left Hepatectomy | 7 (11.9%) |
| Right Hepatectomy | 8 (13.6%) |
| Segments | |
| One segmentectomy | 34 (57.6%) |
| Bisegmentectomy | 5 (8.5%) |
| Major hepatectomy (≥3 segments) | 20 (33.9%) |
| Resection margins status | |
| R0 | 42 (71.2%) |
| R1 | 14 (23.7%) |
| R2 | 3 (5.1%) |
| Macroscopic type of tumor | |
| Nodular | 54 (91.5%) |
| Diffuse | 2 (3.4%) |
| Satellite | 3 (5.1%) |
| Tumor size | |
| <5 cm | 37 (62.7%) |
| ≥5 cm | 22 (37.3%) |
| Capsule | |
| Yes | 29 (49.2%) |
| No | 30 (50.8%) |
| Macroscopic necrosis | |
| Yes | 26 (44.1%) |
| No | 33 (55.9%) |
| Macroscopic vascular invasion | |
| Yes | 10 (16.9%) |
| No | 49 (83.1%) |
| Microscopic vascular invasion | |
| Yes | 29 (49.2%) |
| No | 30 (50.8%) |
| WHO grading | |
| G1 | 8 (13.6%) |
| G2 | 41 (69.5%) |
| G3 | 9 (15.3%) |
| G4 | 1 (1.7%) |
| Mitotic index | |
| <5 mitotic cells—low mitotic index | 50 (84.7%) |
| ≥5 mitotic cell—high mitotic index | 9 (15.3%) |
| Histological subtype of tumor | |
| C-HCC | 44 (74.6%) |
| SH-HCC | 15 (25.4%) |
| Metavir | |
| M0 | 16 (27.1%) |
| M1 | 4 (6.8%) |
| M2 | 5 (8.5%) |
| M3 | 9 (15.3%) |
| M4 | 25 (42.4%) |
| Ishak | |
| F0 | 16 (27.1%) |
| F1 | 1 (1.7%) |
| F2 | 4 (6.8%) |
| F3 | 4 (6.8%) |
| F4 | 5 (8.5%) |
| F5 | 4 (6.8%) |
| F6 | 25 (42.4%) |
| NASH | |
| Yes | 5 (8.5%) |
| No | 28 (47.5%) |
| Non-applicable | 26 (44.1%) |
| CK19 | |
| Positive (≥5%) | 6 (10.2%) |
| Negative (<5%) | 51 (86.4% |
| Absent | 2 (3.4%) |
| GLP-3 | |
| Positive (≥10%) | 38 (64.4%) |
| Negative (<10%) | 18 (30.5%) |
| Absent | 3 (5.1%) |
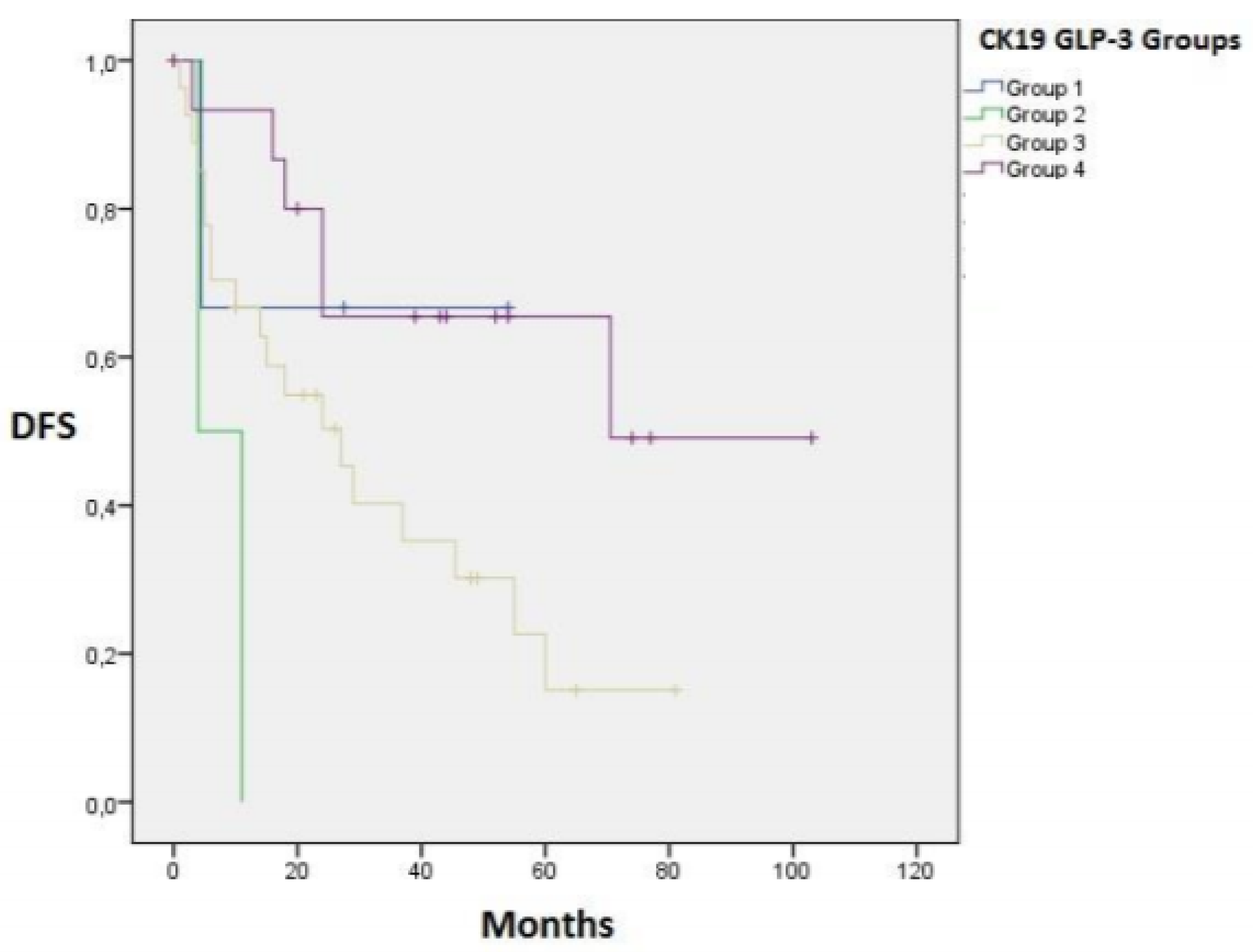
| Group 1 (CK19+/GLP-3+) | 4 (6.8%) |
| Group 2 (CK19+/GLP-3−) | 2 (3.4%) |
| Group 3(CK19−/GLP-3+) | 34 (57.6%) |
| Group 4 (CK19−/GLP-3−) | 16 (27.1%) |
| Absent | 3 (5.1%) |
| Grade | N (%) | Clinical Conditions |
|---|---|---|
| No complication | 28 (47.5%) | |
| Clavien I | 0 (0%) | |
| Clavien II | 15 (25.4%) | |
| Clavien IIIa | 7 (11.9%) | Ascites 1 3 (5.1%) Abscess 2 2 (3.4%) Biloma 2 1 (1.7%) Pleural effusion 3 1 (1.7%) |
| Clavien IIIb | 5 (8.5%) | Abscess 4 4 (6.8%) Surgical incision infection and evisceration 1 (1.7%) |
| Clavien IVa | 0 (0%) | |
| Clavien IVb | 1 (1.7%) | Hemorrhage and Hemodynamic instability 5 1 (1.7%) |
| Clavien V | 3 (5.1%) | Liver failure 1 (1.7%) Hemorrhage and Hemodynamic instability 2 (3.4%) |
| Overall Survival (OS) | |||
|---|---|---|---|
| Median OS | 5-year OS | p-value | |
| MaVI+ | 17 ± 4 months | 0% | 0.000 |
| MaVI− | 81 ± 11 months | 56% | |
| MiVI+ | 28 ± 9 months | 36% | 0.01 |
| MiVI− | 132 ± 12 months | 63% | |
| Disease-free survival (DFS) | |||
| Median DFS | 5-year DFS | p-value | |
| MaVI+ | 5 ± 1 months | 0% | <0.001 |
| MaVI− | 55 ± 11 months | 38% | |
| MiVI+ | 15 ± 4 months | 25% | <0.001 |
| MiVI− | 71 ± 11 months | 44% | |
| Disease-Free Survival (DFS) | |||
|---|---|---|---|
| Median DFS | 5-Year DFS | p-Value | |
| Group 1 (CK19+/ GLP-3+) | 38 ± 14 months | 0% | 0.01 |
| Group 2 (CK19+/ GLP-3−) | 4 ± 3.5 months | 0% | |
| Group 3(CK19−/ GLP-3+) | 27 ± 8 months | 15% | - |
| Group 4 (CK19−/ GLP-3−) | 71 ± 11 months | 49% | |
| HR | 95% CI | p-Value | |
|---|---|---|---|
| HCV | 4.02 | 1.66–9.77 | 0.002 |
| MaVI | 4.48 | 1.79–11.20 | 0.001 |
| MiVI | 3.91 | 1.52–10.04 | 0.005 |
| MS | 0.19 | 0.07–0.52 | 0.001 |
| HR | 95% CI | p-Value | |
|---|---|---|---|
| HPC | 4.07 | 1.37–12.12 | 0.012 |
| R2 | 2.60 | 1.44–4.71 | 0.002 |
| MaVI | 6.16 | 2.21–17.14 | 0.000 |
| MiVI | 2.83 | 1.08–7.42 | 0.035 |
| Group 2 (CK19+/ GLP-3−) | 9.99 | 1.89–52.76 | 0.007 |
| Group 3 (CK19−/ GLP-3+) | 2.67 | 1.11–6.44 | 0.029 |
| Group 4 (CK19−/ GLP-3−) | 0.36 | 0.14–0.91 | 0.031 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viana, L.; Oliveira, R.C.; Martins, R.; Alexandrino, H.; Cipriano, M.A.; Tralhão, J.G. Prognostic Factors after Hepatectomy for Hepatocellular Carcinoma—The Importance of Pathological Immunophenotyping, the Steatohepatitic Subtype and the Impact of the Hepatic Pedicle Clamping. Gastrointest. Disord. 2024, 6, 402-420. https://doi.org/10.3390/gidisord6020027
Viana L, Oliveira RC, Martins R, Alexandrino H, Cipriano MA, Tralhão JG. Prognostic Factors after Hepatectomy for Hepatocellular Carcinoma—The Importance of Pathological Immunophenotyping, the Steatohepatitic Subtype and the Impact of the Hepatic Pedicle Clamping. Gastrointestinal Disorders. 2024; 6(2):402-420. https://doi.org/10.3390/gidisord6020027
Chicago/Turabian StyleViana, Lorrane, Rui Caetano Oliveira, Ricardo Martins, Henrique Alexandrino, Maria Augusta Cipriano, and José Guilherme Tralhão. 2024. "Prognostic Factors after Hepatectomy for Hepatocellular Carcinoma—The Importance of Pathological Immunophenotyping, the Steatohepatitic Subtype and the Impact of the Hepatic Pedicle Clamping" Gastrointestinal Disorders 6, no. 2: 402-420. https://doi.org/10.3390/gidisord6020027
APA StyleViana, L., Oliveira, R. C., Martins, R., Alexandrino, H., Cipriano, M. A., & Tralhão, J. G. (2024). Prognostic Factors after Hepatectomy for Hepatocellular Carcinoma—The Importance of Pathological Immunophenotyping, the Steatohepatitic Subtype and the Impact of the Hepatic Pedicle Clamping. Gastrointestinal Disorders, 6(2), 402-420. https://doi.org/10.3390/gidisord6020027