
Predicting Myalgic Encephalomyelitis/Chronic Fatigue Syndrome from Early Symptoms of COVID-19 Infection


Abstract
:1. COVID-19 and Long COVID
2. Methods
2.1. Data Collection
2.1.1. ME/CFS Sample
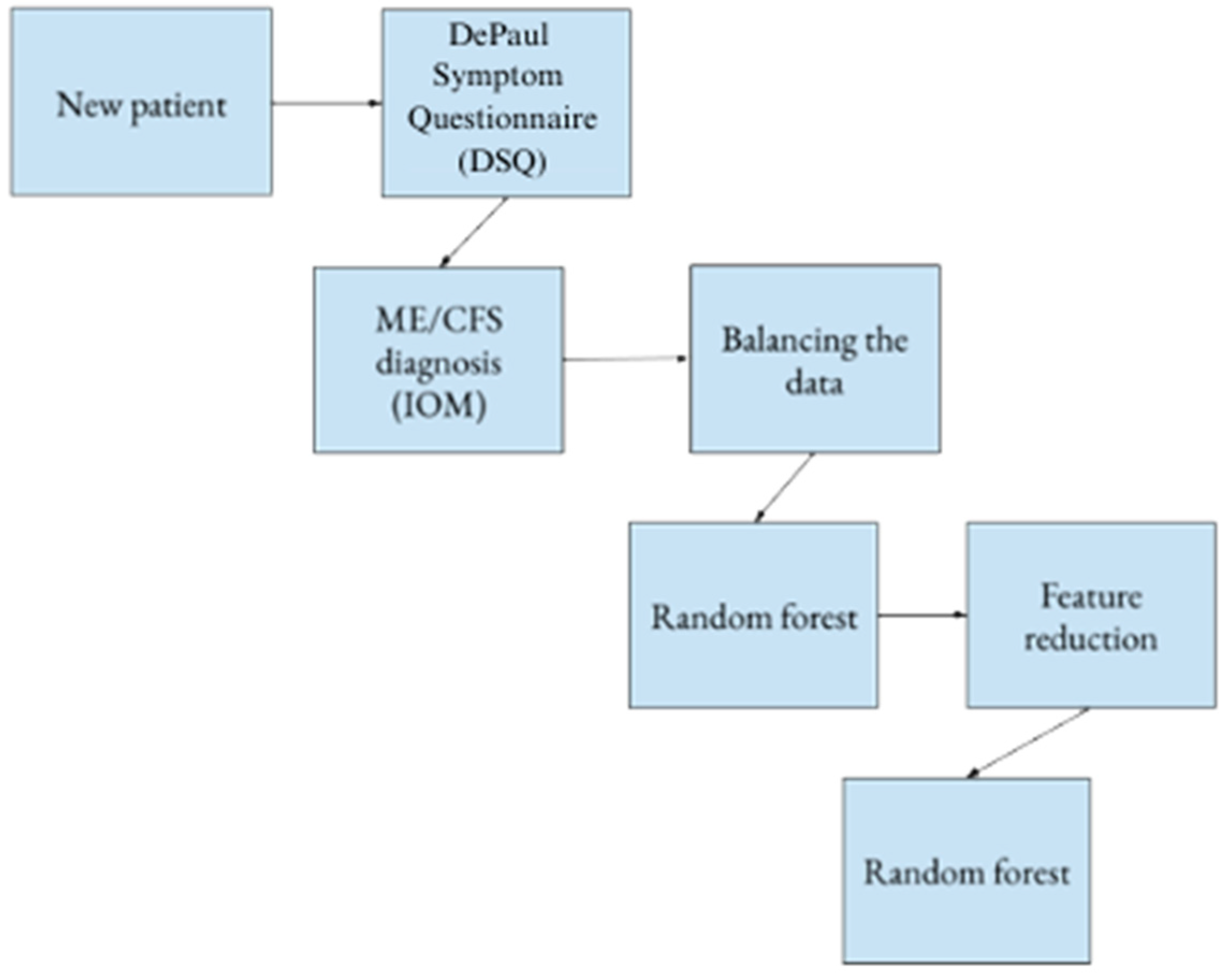
2.1.2. The DePaul Symptom Questionnaire (DSQ)
2.1.3. ME/CFS Diagnosis
2.1.4. Dataset Management
2.1.5. Statistical Analysis
2.1.6. Feature Reduction
2.1.7. Tests for Significance
- E1 = the error rate for model M1;
- E2 = the error rate for model M1;
- q = (E1 + E2)/2;
- n1 = the number of instances in test set A;
- n2 = the number of instances in test set B.
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 pathophysiology: A review. Clin. Immunol. 2020, 215, 108427. Available online: https://www.sciencedirect.com/science/article/pii/S152166162030262X (accessed on 20 July 2022). [CrossRef] [PubMed]
- Guo, Y.-R.; Cao, Q.-D.; Hong, Z.-S.; Tan, Y.-Y.; Chen, S.-D.; Jin, H.-J.; Tan, K.-S.; Wang, D.-Y.; Yan, Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak—An update on the status. Mil. Med. Res. 2020, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Cutler, D.M.; Summers, L.H. The COVID-19 Pandemic and the $16 trillion virus. JAMA 2020, 324, 1495–1496. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Who Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 20 July 2022).
- Daniel, S.J. Education and the COVID-19 pandemic. Prospects 2020, 49, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.M.; Tasnim, S.; Sultana, A.; Faizah, F.; Mazumder, H.; Zou, L.; McKyer, E.L.J.; Ahmed, H.U.; Ma, P. Epidemiology of mental health problems in COVID-19: A review. F1000Research 2020, 9, 636. Available online: https://pubmed.ncbi.nlm.nih.gov/33093946 (accessed on 20 July 2022). [CrossRef] [PubMed]
- Cao, X. COVID-19: Immunopathology and its implications for therapy. Nat. Rev. Immunol. 2020, 20, 269–270. [Google Scholar] [CrossRef]
- Rubin, R. As their numbers grow, COVID-19 Long Haulers stump experts. JAMA 2020, 324, 1381–1383. [Google Scholar] [CrossRef]
- Lamontagne, S.J.; Winters, M.F.; Pizzagalli, D.A.; Olmstead, M.C. Post-acute sequelae of COVID-19: Evidence of mood & cognitive impairment. Brain Behav. Immun. Health 2021, 17, 100347. [Google Scholar]
- YaleMedicine. Long Covid (Post-Acute Sequelae of SARS-Cov-2 Infection, Pasc). Available online: https://ym.care/5gs (accessed on 20 July 2022).
- Kenny, G.; McCann, K.; O’brien, C.; Savinelli, S.; Tinago, W.; Yousif, O.; Lambert, J.S.; O’broin, C.; Feeney, E.R.; De Barra, E.; et al. Identification of distinct Long COVID clinical phenotypes through cluster analysis of self-reported symptoms. Open Forum Infect. Dis. 2022, 9, ofac060. [Google Scholar] [CrossRef]
- CDC. Long Covid or Post-Covid Conditions. Available online: https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html (accessed on 20 July 2022).
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global prevalence of Post-Coronavirus Disease 2019 (COVID-19) Condition or Long COVID: A meta-analysis and systematic review. J. Infect. Dis. 2022, 226, 1593–1607. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’Em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef] [PubMed]
- Nehme, M.; Braillard, O.; Chappuis, F.; Courvoisier, D.S.; Guessous, I.; CoviCare Study Team. Prevalence of symptoms more than seven months after diagnosis of symptomatic COVID-19 in an outpatient setting. Ann. Intern. Med. 2021, 174, 1252–1260. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Li, X.; Gu, X.; Zhang, H.; Ren, L.; Guo, L.; Liu, M.; Wang, Y.; Cui, D.; Wang, Y.; et al. Health outcomes in people 2 years after surviving hospitalisation with COVID-19: A longitudinal cohort study. Lancet Respir. Med. 2022, 10, 863–876. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Yifan, T.; Ying, L.; Chunhong, G.; Jing, S.; Rong, W.; Zhenyu, L.; Zejuan, G.; Peihung, L. Symptom cluster of ICU nurses treating COVID-19 pneumonia patients in Wuhan, China. J. Pain Symptom Manag. 2020, 60, e48–e53. [Google Scholar] [CrossRef]
- Luo, Y.; Wu, J.; Lu, J.; Xu, X.; Long, W.; Yan, G.; Tang, M.; Zou, L.; Xu, D.; Zhuo, P.; et al. Investigation of COVID-19-related symptoms based on factor analysis. Ann. Palliat. Med. 2020, 9, 1851–1858. [Google Scholar] [CrossRef]
- Guo, P.; Ballesteros, A.B.; Yeung, S.P.; Liu, R.; Saha, A.; Curtis, L.; Kaser, M.; Haggard, M.P.; Cheke, L.G. COVCOG 1: Factors predicting physical, neurological and cognitive symptoms in Long COVID in a community sample. A first publication from the COVID and Cognition Study. Front. Aging Neurosci. 2022, 14, 804922. [Google Scholar] [CrossRef]
- Yancey, J.R.; Thomas, S.M. Chronic fatigue syndrome: Diagnosis and treatment. Am. Fam. Physician 2012, 86, 741–746. [Google Scholar]
- American Myalgic Encephalomyelitis and Chronic Fatigue Syndrome Society. How Many People Have ME/CFS? 2019. Available online: https://ammes.org/how-many-people-have-mecfs/ (accessed on 20 July 2022).
- Lim, E.-J.; Son, C.-G. Review of case definitions for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). J. Transl. Med. 2020, 18, 289. [Google Scholar] [CrossRef]
- Afari, N.; Buchwald, D. Chronic Fatigue Syndrome: A Review. Am. J. Psychiatry 2003, 160, 221–236. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The chronic fatigue syndrome: A comprehensive approach to its definition and study. International Chronic Fatigue Syndrome Study Group. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, B.M.; Jain, A.K.; De Meirleir, K.L.; Peterson, D.L.; Klimas, N.G.; Lerner, A.M.; Bested, A.C.; Flor-Henry, P.; Joshi, P.; Powles, A.C.P.; et al. Myalgic encephalomyelitis/chronic fatigue syndrome: Clinical working case definition, diagnostic and treatment protocols. J. Chronic Fatigue Syndr. 2003, 11, 7–115. [Google Scholar] [CrossRef]
- Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness; National Academies Press: Washington, DC, USA, 2015. [Google Scholar]
- Brurberg, K.G.; Fønhus, M.S.; Larun, L.; Flottorp, S.; Malterud, K. Case definitions for chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME): A systematic review. BMJ Open 2014, 4, e003973. [Google Scholar] [CrossRef]
- Wormgoor, M.E.A.; Rodenburg, S.C. The evidence base for physiotherapy in myalgic encephalomyelitis/chronic fatigue syndrome when considering post-exertional malaise: A systematic review and narrative synthesis. J. Transl. Med. 2021, 19, 1. [Google Scholar] [CrossRef]
- Hickie, I.; Davenport, T.; Wakefield, D.; Vollmer-Conna, U.; Cameron, B.; Vernon, S.D.; Reeves, W.C.; Lloyd, A. Post infective and chronic fatigue syndromes precipitated by viral and non-viral pathogens: Prospective cohort study. BMJ 2006, 333, 575. Available online: https://www.bmj.com/content/333/7568/575 (accessed on 20 July 2022). [CrossRef]
- Katz, B.Z.; Shiraishi, Y.; Mears, C.J.; Binns, H.J.; Taylor, R. Chronic Fatigue Syndrome After Infectious Mononucleosis in Adolescents. Pediatrics 2009, 124, 189–193. [Google Scholar] [CrossRef]
- Jason, L.A.; Islam, M.F. A classification system for post-acute sequelae of SARS-Cov-2 infection. Cent. Asian J. Med Hypotheses Ethics 2022, 3, 38–51. Available online: https://cajmhe.com/index.php/journal/article/view/146/66 (accessed on 20 July 2022). [CrossRef]
- Jason, L.A.; Sunnquist, M. The Development of the DePaul Symptom Questionnaire: Original, expanded, brief, and pediatric versions. Front. Pediatr. 2018, 6, 330. [Google Scholar] [CrossRef]
- Strand, E.B.; Lillestøl, K.; Jason, L.A.; Tveito, K.; Diep, L.M.; Valla, S.S.; Sunnquist, M.; Helland, I.B.; Herder, I.; Dammen, T. Comparing the DePaul Symptom Questionnaire with physician assessments: A preliminary study. Fatigue Biomed. Health Behav. 2016, 4, 52–62. [Google Scholar] [CrossRef]
- Murdock, K.W.; Wang, X.S.; Shi, Q.; Cleeland, C.S.; Fagundes, C.P.; Vernon, S.D. The utility of patient-reported outcome measures among patients with myalgic encephalomyelitis/chronic fatigue syndrome. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2016, 26, 913–921. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; So, S.; Brown, A.A.; Sunnquist, M.; Evans, M. Test–retest reliability of the DePaul Symptom Questionnaire. Fatigue: Biomed. Heal. Behav. 2015, 3, 16–32. [Google Scholar] [CrossRef]
- Ohanian, D.; Brown, A.; Sunnquist, M.; Furst, J.; Nicholson, L.; Klebek, L.; Jason, L.A. Identifying Key Symptoms Differentiating Myalgic Encephalomyelitis and Chronic Fatigue Syndrome from Multiple Sclerosis. Neurology 2016, 4, 41–45. [Google Scholar] [PubMed]
- Klebek, L.; Sunnquist, M.; Jason, L.A. Differentiating post-polio syndrome from myalgic encephalomyelitis and chronic fatigue syndrome. Fatigue: Biomed. Heal. Behav. 2019, 7, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Roiger, R.J.; Geatz, M.W. Data Mining: A Tutorial-Based Primer; Chapman & Hall/CRC: Boca Raton, FL, USA, 2003. [Google Scholar]
- Bernal, J.L.; Andrews, N.; Gower, C.; Robertson, C.; Stowe, J.; Tessier, E.; Simmons, R.; Cottrell, S.; Roberts, R.; O’Doherty, M.; et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on COVID-19 related symptoms, hospital admissions, and mortality in older adults in England: Test negative case-control study. BMJ 2021, 373, n1088. [Google Scholar] [CrossRef]
- Gross, C.P.; Essien, U.R.; Pasha, S.; Gross, J.R.; Wang, S.-Y.; Nunez-Smith, M. Racial and Ethnic Disparities in Population-Level Covid-19 Mortality. J. Gen. Intern. Med. 2020, 35, 3097–3099. [Google Scholar] [CrossRef]
- Romano, S.D.; Blackstock, A.J.; Taylor, E.V.; El Burai Felix, S.; Adjei, S.; Singleton, C.-M.; Fuld, J.; Bruce, B.B.; Boehmer, T.K. Trends in racial and ethnic disparities in COVID-19 hospitalizations, by region—United States, March-December 2020. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 560–565. [Google Scholar] [CrossRef]


{kind=link}
| Dataset | Accuracy | Sensitivity | Specificity |
|---|---|---|---|
| Original | 88.26 ± 0.22 | 95.33 ± 0.26 | 70.16 ± 0.30 |
| Balanced | 94.55 ± 0.78 | 91.41 ± 1.08 | 97.69 ± 0.87 |
| # | Feature Name | Domain |
|---|---|---|
| 1 | Fatigue/extreme tiredness | PEM |
| 2 | Mentally tired after the slightest effort | PEM |
| 3 | Feeling unrefreshed after you wake in the morning | Sleep |
| 4 | Minimum exercise makes you physically tired | PEM |
| 5 | Next-day soreness or fatigue after non-strenuous, everyday activities | PEM |
| 6 | Needing to nap daily | Sleep |
| 7 | Dread, heavy feeling after starting to exercise | PEM |
| 8 | Feeling hot or cold for no reason | Neuroendocrine |
| Dataset | Accuracy | Sensitivity | Specificity |
|---|---|---|---|
| Original | 89.46 ± 0.36 | 95.44 ± 0.35 | 74.17 ± 0.55 |
| Balanced | 93.47 ± 0.99 | 91.13 ± 1.22 | 95.81 ± 1.40 |
| First Model | Second Model | t Value |
|---|---|---|
| Original 54 items | Original 8 items | 0.46 |
| Balanced 54 items | Balanced 8 items | 0.58 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hua, C.; Schwabe, J.; Jason, L.A.; Furst, J.; Raicu, D. Predicting Myalgic Encephalomyelitis/Chronic Fatigue Syndrome from Early Symptoms of COVID-19 Infection. Psych 2023, 5, 1101-1108. https://doi.org/10.3390/psych5040073
Hua C, Schwabe J, Jason LA, Furst J, Raicu D. Predicting Myalgic Encephalomyelitis/Chronic Fatigue Syndrome from Early Symptoms of COVID-19 Infection. Psych. 2023; 5(4):1101-1108. https://doi.org/10.3390/psych5040073
Chicago/Turabian StyleHua, Chelsea, Jennifer Schwabe, Leonard A. Jason, Jacob Furst, and Daniela Raicu. 2023. "Predicting Myalgic Encephalomyelitis/Chronic Fatigue Syndrome from Early Symptoms of COVID-19 Infection" Psych 5, no. 4: 1101-1108. https://doi.org/10.3390/psych5040073
APA StyleHua, C., Schwabe, J., Jason, L. A., Furst, J., & Raicu, D. (2023). Predicting Myalgic Encephalomyelitis/Chronic Fatigue Syndrome from Early Symptoms of COVID-19 Infection. Psych, 5(4), 1101-1108. https://doi.org/10.3390/psych5040073