Abstract
The aim of this in vitro study was to investigate cytotoxic effects of dual-cure bulk-fill resin materials polymerized with a third-generation LED light-curing unit (LCU) on L929 fibroblast cells in terms of morphology and viability. Three novel dual-cure, flowable bulk-fill materials (Fill-Up!™), a bioactive material (ACTIVA™ BioACTIVE-RESTORATIVE™), and a dual-cure bulk-fill composite material (HyperFIL® HAp) polymerized by LED LCU (VALO™ Cordless) were tested. Each material was placed in plastic rings (4 mm × 5 mm) in a single layer. Unpolymerized rings filled with each material were placed in direct contact with cells and then polymerized. After polymerization, the removed medium was readded to wells. In this study, four control groups were performed: the medium-free control group, medium control group, physical control group, and light applied control group. Three samples were prepared from each group. After 24 h, the morphology of cells was examined and a WST-1 test was performed. The percentage of cell viability (PCV) of each group was calculated. The experiment was repeated three times. Data were analyzed by a Kruskal–Wallis Test and a Mann–Whitney U test. p < 0.05 was considered significant. The PCV of all groups were found to be significantly lower than the medium control group (p < 0.05). The lowest PCV was obtained in HyperFIL® Hap, while highest was in the Fill-Up!™. In the morphology of cells related to the experimental groups, it was observed that the spindle structures of cells were disrupted due to cytotoxicity; cells became rounded and intercellular space increased. There were no significant differences between the control groups (p > 0.05). All control groups showed acceptable PCV (>70%) and cells were spindle-like, similar to the original fibroblast cells. It can be suggested that clinicians should pay attention when applying dual-cure bulk-fill materials in deep cavities, or they should use a liner material under these materials.
1. Introduction
Resin-based composites are usually placed in increments of less than 2 mm to ensure adequate light curing and to reduce polymerization shrinkage [1]. However, this is time-consuming in deep cavities, and it has the risk of incorporating air bubbles and the possibility of contamination between the increments. Recently, new composite materials, so-called ‘bulk fill’, was introduced to the market that is claimed to be curable up to a 4 mm thickness [2].
Although the use of new generation bulk-fill composite resins in >4 mm depths may prove to be convenient for physicians, their use is still far from being widely accepted. This is mainly due to the lack of sufficient information on their physical, chemical, and cytotoxic properties in the literature [3].
Nowadays dual-cure bulk-fill resin materials, a flowable bulk-fill material with antibacterial zinc oxide (Fill-Up!™), bioactive material (ACTIVA™ BioACTIVE-RESTORATIVE™), and dual-cure bulk-fill composite material containing nano-hydroxyapatite (HyperFIL® HAp) have been launched. These materials provide unlimited depth of cure with a single layer placement. Additionally, they contain both light-cure and chemical cure components [4]. The light cure component provides rapid, initial hardening of the top layers of the composite, stabilizing the restorations, while the deeper layers of the composite that receive insufficient light irradiation are polymerized by the slower chemical-cure reaction [5]. As a result, the new dual-cure bulk-fill composites eliminate the issues of light attenuation that would disrupt the setting of the deepest portions of the filling [6].
The biocompatibility of a substance is the state of being compatible with the biological functions of the tissue, without showing toxic and harmful effects. Among the criteria for dental materials to be clinically successful, their biocompatibility is also important [7]. In studies evaluating the biocompatibility of restorative materials, various test methods are used, such as the in vitro cell culture method, in vivo animal experiments, and clinical testing [8]. Determination of cell viability, investigation of changes in cell morphology, and mediator activities in cells are methods used to evaluate the biocompatibility of restorative materials in cell culture studies [9].
Studies investigating the cytotoxicity of dual-cure bulk-fill materials are still limited [10,11], and none have compared the cytotoxicity among themselves.
Therefore, the aim of this in vitro cell culture study was to investigate the cytotoxicity of three current bulk-fill composite materials polymerized with a third-generation multi-wavelength LED light-curing unit (LCU) on L929 mouse fibroblast cells using direct contact cell culture method in terms of cell morphology and viability (WST-1 test). The null hypothesis was bulk-fill composite resin materials do not have cytotoxic effects on the morphology and the viability of L929 cells.
2. Materials and Methods
In this study, a flowable bulk-fill material containing antibacterial zinc oxide (Fill-Up!™, Coltene, Whaledent, Switzerland, [FU]), a bioactive material that can be placed bulk (ACTIVA™ BioACTIVE-RESTORATIVE™, Pulpdent Corporation, Watertown, NY, USA, [ABR]), and a dual-cure bulk-fill composite material containing nano-hydroxyapatite (HyperFIL® HAp, Parkell, Edgewood, NY, USA, [HFH]) were used as restorative materials (Table 1). For the polymerization of these materials; a third-generation LED LCU (VALO™ Cordless, Ultradent, South Jordan, UT, USA) with a multi-wavelength (395–480 nm) was used in standard mode (1000 mW/cm2).

Table 1.
Experimental materials used in the study.
2.1. Cell Culture
L929 fibroblast cells were purchased from the American Type Culture Collection (ATCC, Manassas, VA, USA) and maintained in Eagle’s Minimum Essential Medium (EMEM, Berlin, Germany) supplemented with 10% fetal bovine serum (Gibco, Carlsbad, CA, USA), 1% L-Glutamine and 1% Penicillin/Streptomycin (Gibco, USA). L929 cells were cultured in culture flasks in a humidified incubator (ESCO, Horsham, PA, USA) with 5% CO2 atmosphere at 37 °C. In each well of the 24 well-plates, 5 × 104 cells were seeded. After 24 h, the density of the cells was checked under a microscope. The experiments were started when the cell density reached 80%.
2.2. Preparation of the Specimens
2.2.1. Experimental Groups
The study was carried out in a sterile cabinet (SafeFAST Classic, Faster, Italy) to ensure aseptic conditions. Plastic rings (4 mm depth × 5 mm diameter) were used, which had previously been sterilized twice in an autoclave. Before starting the experiment, the medium covering the L929 fibroblast cells was removed. Then, each material (FU, ABR, and HFH) was placed in a single layer in the ring. The rings that were filled with unpolymerized material were placed in direct contact with the fibroblast cells [11]. A previously sterilized and specially designed barrier was applied to the relevant well, where the material is applied. This barrier was designed to ensure that each transparent well is isolated from other wells to prevent the light from passing through the other wells. Then, the rings were polymerized with a LED LCU (VALO™ Cordless) according to the manufacturer’s recommendations for 10 s, 20 s, and 40 s, respectively. After the barrier was removed, the medium was readded to the cells in each well (Figure 1).
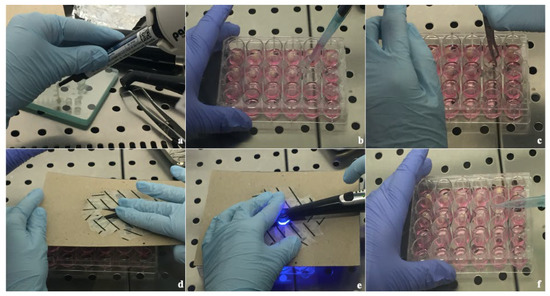
Figure 1.
Application of experimental groups (a) Placing the material in the molds, (b) Removal of cells medium, (c) Placement of material on cells, (d) Placement of the barrier, (e) Polymerization of the material, and (f) Addition of cell mediums.
2.2.2. Control Groups
There were four control groups in the study.
- The Medium Control Group (MC): The medium of L929 cells was not removed. No light was applied to the cells;
- The Medium-Free Control Group (MFC): The purpose of this control group was to investigate to what extent the 40 s waiting time (which is the longest polymerization time of the materials) would affect the viability of the cells when preparing the samples in an outside environment. While preparing this group, the medium of L929 cells was removed. No light was applied to the cells. After waiting for 40 s, the medium was readded;
- The Physical Control Group (PC): The purpose of this control group was to mimic the weight of the test material with a cotton pellet, a sterile neutral material, to examine whether any cell death would occur on the cell group they were applied to. After removing the medium, plastic rings with only cotton pellets were placed directly on the cells and the medium was readded;
- The Light Applied Control Group (LAC): The purpose of this control group was to investigate whether there would be any cell death when light was applied for 40 s (which is the longest polymerization applied to the tested materials), and then the medium was readded.
Three samples were prepared for each experimental and control group. Each experiment was repeated three times for the reliability of the study.
The study design is shown in Table 2.
Table 2.
The study design of the experimental and the control groups prepared in well plates.
2.3. Evaluation of Cell Morphology and Assessment of Cell Viability Using WST-1 Assay
After 24 h, material samples and physical control samples were removed from each well. Then, morphological alteration of L929 cells for each experimental and control group was observed using an optical microscope (Novel, China).
WST-1 test was performed to determine the number of viable cells [12]. After WST-1 (Cell Proliferation Assessment Agent, Roche, Indianapolis IN, USA) was added to the wells, the plates were incubated for 3 h at 37 °C in an incubator containing 5% CO2. Absorbance was measured at a wavelength of 440 nm in a microplate reader (BioTek Synergy H1 Hybrid Reader, Winooski VT, USA).
The WST-1 test was repeated three times for all experimental and control groups in terms of the study’s reliability.
2.4. Statistical Analyzes
The cell viability was calculated as a percentage (%). IBM SPSS Statistics 22 program (SPSS IBM, Turkey) was used for the statistical analysis. While evaluating the data, the conformity of the parameters to the normal distribution was evaluated with the Shapiro Wilks test, and it was found that the parameters did not show a normal distribution. In addition to descriptive statistical analyses [median (minimum and maximum), mean and standard deviation, the Kruskal–Wallis test for intergroup comparison, and the Mann Whitney U Test for pairwise comparisons were used. The overall significance level of the study was accepted as p < 0.05.
3. Results
3.1. Alteration in the Morphology of Cells
In the experimental groups, it was observed that the smooth and spindle structures of L929 fibroblast cells were disrupted, became rounded, and the intercellular space increased (Figure 2a–c).
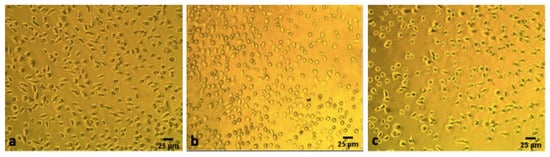
Figure 2.
The morphological views of cells. Experimental Groups: (a) Fill-Up!™ polymerized with VALO™ Cordless LCU, (b) ACTIVA™ BioACTIVE-RESTORATIVE™ polymerized with VALO™ Cordless LCU, and (c) HyperFIL® HAp polymerized with VALO™ Cordless. The scale bar in each image equals to 25 μm.
In the control groups, L929 fibroblast cells were found to be smooth and spindle, and the intercellular space was determined to very little (Figure 3a–d).
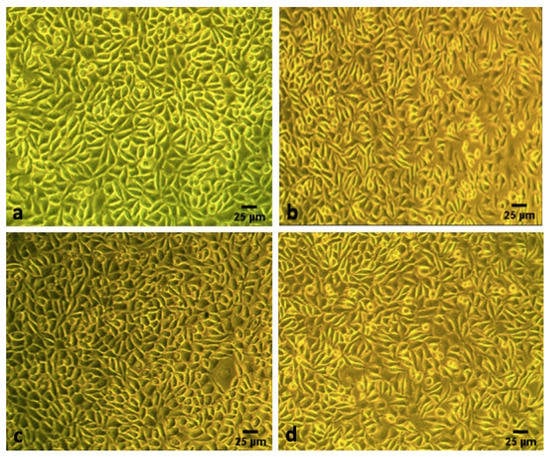
Figure 3.
The morphological views of cells. Control Groups: (a) The medium control group, (b) The medium-free control group, (c) The physical control group, and (d) The light applied control group. The scale bar in each image equals to 25 μm.
3.2. Viability of the Cells (WST-1 Test)
The increase in absorbance in the WST-1 test indicates a high number of viable cells [12].
According to the absorbance of the MC group, the cell viability of this group was accepted as 100%. The percentage of cell viability (PCV) of the experimental groups—the MFC group, PC group, and LAC group—was calculated and compared with the PCV of the MC group.
There was no statistically significant difference between the experimental groups—FU, ABR, HFH—in terms of the PCV (p > 0.05) (Figure 4).
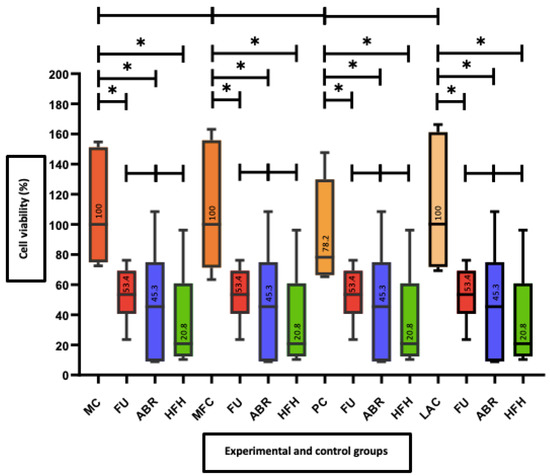
Figure 4.
Comparison of cell viability (%) of experimental and control groups. Cell viability was expressed as a percentage of medium control group cell cultures. Results of Kruskal–Wallis test and Mann–Whitney U test. *: Indicates statistically significant differences in cell viability (p < 0.05). MC: Medium Control, FU: Fill Up!™, ABR: ACTIVA™ BioACTIVE-RESTORATIVE™, HFH: HyperFIL® HAp, MFC: Medium-Free Control, PC: Physical Control, LAC: Light Applied Control.
When each control group was compared with the experimental groups, the PCV of the control groups was statistically significantly higher than all experimental groups (p < 0.05) (Figure 4).
No statistically significant differences were found between the control groups—MC, MFC, PC, and LAC–in terms of the PCV (p > 0.05) (Figure 4).
4. Discussion
In this in vitro study, the cytotoxicity of dual-cure bulk-fill restorative materials on L929 fibroblast cells was evaluated using the WST-1 test. According to ISO 10993-5 [13], when a material has cell viability lower than 70%, it is accepted that this material has cytotoxic potential. In the results of the study, the PCV of the dual-cure bulk-fill materials were as follows: FU: 53.4%, ABR: 45.3%, and HFH: 20.8%. In the normal appearance of L929 fibroblast cells, the cells look smooth and spindle-shaped [14]. When the morphology of L929 fibroblast cells in contact with the experimental materials was examined, it was observed that the smooth and spindle structures of the cells were disrupted, the cells became rounded, and the intercellular space increased. This means that all of the dual-cure bulk-fill materials were found cytotoxic on the cells. Therefore, the null hypothesis was rejected.
Dual-cure systems are used to ensure sufficient polymerization in deep areas where light is cannot insufficient. Based on these systems, dual-cure composite resins have been recommended for core build-ups and luting of all-ceramic restorations. In addition, dual-cure bulk-fill composites are also used in the restoration of deep cavities [6,15].
Although advances in composite resin materials are promising mechanically, physically, and aesthetically, a material must also be biocompatible to be safely used in the oral environment [16]. Therefore, it is important to question new composites and other dental materials in terms of biocompatibility, besides their physical properties [16,17].
Direct cell contact tests [18], extract tests [19], and indirect contact tests [20] are used in in vitro cell culture studies. Cao et al. reported that the cell-material direct contact method better mimics the in vivo physiological environment [21]. Similar to the Kazak et al. study [11], discs filled with non-polymerized dual-cure bulk-fill materials were placed directly on the cells, thereby ensuring direct contact between the cells and the materials. In their study [11], the cytotoxic effects of the components released from the materials (Tetric N-Ceram Buk-Fill, Tetric N-Ceram, and Clearfil Majesty ES-2) on the cells were evaluated. Similar to their research method, in this study, the experimental materials were polymerized after being placed directly on the cells.
As mentioned in ISO 10993-5 [13], continuous cell lines, such as L929 and Balb/3T3 mouse fibroblasts, are routinely used to test the cytotoxicity of dental materials [21,22]. L929 cell lines provide good reproducibility for in vitro cytotoxicity screening owing to their homogenous morphology and growth characteristics [23]. In addition, studies have reported that L929 is more sensitive and reliable than other cell lines [22,24]. Dental materials usually interact with the oral epithelial cells, and they can also interact with the underlying fibroblasts [25]. Besides in gingival connective tissue, fibroblasts are also the predominant cell type in the pulp and might be affected by eluted substances from dental restorative materials if the odontoblastic layer is destroyed [26]. Therefore, in this in vitro study, L929 fibroblast cell lines were preferred.
According to the results of a previous study conducted in 2019 in which they investigated the cytotoxic effects of three bulk-fill materials (HyperFIL®, ACTIVA™ BioACTIVE-RESTORATIVE™, and Estelite Bulk Fill flow) on fibroblast cells by the direct contact method using the LED LCU, it was found that the PCV of ACTIVA™ BioACTIVE-RESTORATIVE™ was lower than other materials, consistent with the results of this study (45.3%) [27].
Lopez-Garcia has investigated the biological effects of three new bioactive materials polymerized with LED LCU on stem cells obtained from the human dental pulp by in vitro extraction. It has been determined that metabolic activity is high and cytotoxicity is low in cell cultures in contact with ACTIVA™ Kids BioACTIVE-RESTORATIVE™ extract [28]. Abou ElReash et al. evaluated the biocompatibility of ACTIVA™ BioACTIVE-RESTORATIVE™ placing subcutaneous tissue implants in rats. They concluded that ACTIVA™ BioACTIVE-RESTORATIVE™ material exhibited excellent biocompatibility and healing ability after 1 week, 2 weeks, and 4 weeks of evaluation [10]. Karabulut et al. used ACTIVA™ BioACTIVE Base/Liner material in their study and evaluated the subcutaneous connective tissue reactions of these bioactive materials. According to the data, they suggested that ACTIVA™ BioACTIVE Base/Liner material was well tolerated by tissues in 60 day evaluation periods [29]. The results of the above studies are different from this study. The different results might be due to the different test methods chosen, LED LCU, and cell types, and the different times during the biocompatibility are evaluated.
According to the manufacturer of ABR, this bioactive material contains a blend of diurethane and other methacrylates with modified polyacrylic acid in its organic content. Although the names of the methacrylates in the material were not shared in detail in the study of Kazak et al. [27], it has been reported that DMABEE (4-N, N-dimethyl amino benzoic acid ethylester), MAA (methacrylic acid), MEHQ (4-methoxyphenol), and EGDMA (ethylene glycol dimethacrylate) monomers were released from the same material by the liquid chromatography-mass/mass spectrometry (LC-MS/MS) method. It is known that the biocompatibility of composite resins is correlated with the amount of the organic substances released and the structure of the organic substances [30]. Monomers releasing from the resin matrix due to insufficient polymerization may produce cytotoxic results over time [17,31]. Therefore, the reason for the lower PCV calculated in ABR may be the unspecified monomers releasing into the environment.
In a study examining the cytotoxic effects of dental materials releasing fluoride, it was found that the decrease in cell viability was higher with the increase in fluoride release and fluoride release was associated with cytotoxicity [32]. In the cytotoxicity studies of bulk-fill composites, it was found that fluoride-containing bulk-fill materials showed higher cytotoxicity than other experimental groups [33,34]. Therefore, another reason for the PCV of ABR remaining below the acceptable PCV in this study may be related to the fluoride ion contained in the material.
In previous studies on the toxic effects of conventional and bulk-fill composites, it was stated that the highest PCV was obtained in materials with the highest filling ratio and the lowest monomer ratio [35,36,37]. The filler ratio (56% by weight) of the ABR used in this study is lower than the other materials used. The PCV of ABR was below the acceptable PCV (70%), which can be attributed to the inorganic filler ratio of the material that is lower and the organic matrix ratio that is higher than the other materials used in the study.
In studies investigating the cytotoxicity of glass ionomer cements, it was reported that while Al3+, Ca2+, and Na+ ions releasing from the powder part of the material do not have a cytotoxic effect on the cells, the polyacrylic acid in the liquid part causes cytotoxicity [19,38]. Therefore, it can be thought that the modified polyacrylic acid consisting in the ABR may be the reason for the lower PCV that was below the acceptable percentage.
HFH is a newly developed and very recently introduced material. To our best knowledge, there is no study investigating the cytotoxic effects of this material in the literature. Kazak et al., investigated the cytotoxic effects of three bulk-fill materials on fibroblast cells by the direct method and found that the HyperFIL® Dual Cure Bulk Fill material was biocompatible [27]. In this study, HFH, which is the nano-hydroxyapatite added form of HyperFIL®, was used. Although the cell type and the test method were similar to the study of Kazak et al. [27], HFH, which can be defined as the upgraded version of HyperFIL®, was found cytotoxic (20.8%) in terms of cell viability. The difference between these results can be due to the different contents of similar materials.
Imazato et al. [39] reported that resin-modified glass ionomer cements containing HEMA were more toxic than BisGMA/TEGDMA based composite resins. Soderlhom et al. [40,41,42] reported that composite resins can release high levels of barium ions into artificial saliva. HFH contains HEMA and barium ions. Therefore, these two components in the structure of HFH may have caused the PCV below the acceptable percentage.
As with HFH, no studies are evaluating the cytotoxic effects of FU. Depth of cure (DOC) is one of the parameters that can give information about the surface microhardness of a material, which is also related to the remaining unreacted monomer. If the microhardness value calculated by the bottom/top ratio of a material is above 80%, then this value indicates the adequate DOC of that material [43]. The DOC is closely related by light absorption and scatter within the material [44]. Besides, it is dependent on the filler (type, size, and load), light irradiance, exposure time, radiant exposure, resin composition, and shade. The presence of unreacted monomer within the resin-based composite may also attenuate the irradiating light, prevent the formation of free radicals and thus reduce the DOC [45]. Aggarwal et al. compared the DOC of resin-based composites and found that Fill-Up!™ did not reach the adequate microhardness value of 80% [46]. Based on this result, after polymerization unreacted monomers may remain in the structure of FU and these unreacted monomers may have caused the cell viability below the acceptable percentage.
In this study, the PCV calculated in the experimental groups was below 70%. Schmalz reported that in in vitro cytotoxicity tests, when the materials and cells were placed in the closest possible position, more cytotoxic effects and exaggerated results can be observed compared to the results that can be obtained under clinical conditions [47]. In addition, in this study, more exaggerated results may have been obtained since the experiments were conducted under laboratory conditions. However, it should not be forgotten that laboratory conditions give a clue about clinical conditions. Besides, the results of the laboratory conditions guide the clinicians during clinical applications. Therefore, in vitro cytotoxicity tests are pioneering tests in terms of simulating clinical situations.
According to the results of the study, although the PCV of the PC group (78.2%) was calculated lower than the PCV of the other three control groups (100%), no statistically significant difference was observed between the groups (p > 0.05). Based on this, it can be considered that the PC group, formed to simulate the similar weight of the material + plastic ring, did not have a negative effect on cell viability and morphology.
Choosing a single type of cell line (L929), using only two parameters (cell viability and cell morphology), evaluating only the 24 h cytotoxicity, and not evaluating the degradation of the experimental materials exposed to the medium were the limitations of the study. The determination of the cytotoxic effects of the test materials not according to the release of toxic compounds but only according to the content was another limitation of the study. Therefore, conducting in vitro cytotoxicity studies longer than 24 h to make a more comprehensive interpretation about the clinical success of these materials, determining the monomer release, and evaluating the clinical follow-up study results together will provide more reliable results.
5. Conclusions
- The cytotoxic effects of the materials on cell viability have been shown to parallel with the cell morphology;
- It can be suggested that clinicians should pay attention, while applying dual-cure bulk-fill materials in deep cavities or should use a liner material under these materials.
Author Contributions
Conceptualization, N.D. and F.B.; methodology, S.S.K.; validation, A.K.; investigation, V.B.Y. and S.S.K.; resources, S.S.K.; data curation, S.S.K.; writing—original draft preparation, S.S.K.; writing—review and editing, A.K. and N.D.; visualization, S.S.K. and V.B.Y.; project administration, N.D. All authors have read and agreed to the published version of the manuscript.
Funding
This thesis was supported by Bezmialem Vakif University Scientific Research Project Unit (Project number: 9.2018/4).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to owe a debt of gratitude to Magrur Kazak from Bahcesehir University, School of Dental Medicine, Department of Restorative Dentistry, for her scientific contribution to the paper. This thesis was presented as a poster presentation at the 10th ConsEuro Virtual Congress (22–24 April 2021).
Conflicts of Interest
The authors declare that there is no conflict of interest.
References
- Leprince, J.G.; Palin, W.M.; Hadis, M.A.; Devaux, J.; Leloup, G. Progress in dimethacrylate-based dental composite technology and curing efficiency. Dent. Mater. 2013, 29, 139–156. [Google Scholar] [CrossRef] [PubMed]
- Uzel, Y.; Kuru, R.; Eden, E. The effect of different application procedures on microleakage and microhardness of a bulk-fill composite material. J. Ege Univ. Faculty Dent. 2017, 38, 48–53. [Google Scholar] [CrossRef]
- Ilie, N.; Bucuta, S.; Draenert, M. Bulk-fill resin-based composites: An in vitro assessment of their mechanical performance. Oper. Dent. 2013, 38, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Kwon, T.Y.; Bagheri, R.; Kim, Y.K.; Kim, K.H.; Burrow, M.F. Cure mechanisms in materials for use in esthetic dentistry. J. Investig. Clin. Dent. 2012, 3, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Taubock, T.T.; Bortolotto, T.; Buchalla, W.; Attin, T.; Krejci, I. Influence of light-curing protocols on polymerization shrinkage and shrinkage force of a dual-cured core build-up resin composite. Eur. J. Oral Sci. 2010, 118, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Vandewalker, J.P.; Casey, J.A.; Lincoln, T.A.; Vandewalle, K.S. Properties of dual-cure, bulk-fill composite resin restorative materials. Gen. Dent. 2016, 64, 68–73. [Google Scholar]
- Wataha, J.C. Predicting clinical biological responses to dental materials. Dent. Mater. 2012, 28, 23–40. [Google Scholar] [CrossRef]
- Murray, P.E.; García Godoy, C.; García Godoy, F. How is the biocompatibilty of dental biomaterials evaluated? Med. Oral Patol. Oral Cir. Bucal. 2007, 12, 258–266. [Google Scholar]
- Gencoglu, N.; Kelasioglu, F. Investigation of cytotoxicity of some root canal sealers. J. Istanbul Univ. Fac. Dent. 1994, 28, 109–112. [Google Scholar]
- ElReash, A.A.; Hamama, H.; Abdo, W.; Wu, Q.; El-Din, A.Z.; Xiaoli, X. Biocompatibility of new bioactive resin composite versus calcium silicate cements: An animal study. BMC Oral Health 2019, 19, 194. [Google Scholar] [CrossRef]
- Kazak, M.; Donmez, N.; Bahadori, F.; Yenigun, V.B.; Kocyigit, A. A preliminary research study on the cytotoxicity of expired and non-expired composite resins: In vitro study. Odovtos 2020, 22, 123–134. [Google Scholar]
- Mosmann, T. Rapid colorimetric assay for cellular growth and survival: Application to proliferation and cytotoxicity assays. J. Immunol. Methods 1983, 65, 55–63. [Google Scholar] [CrossRef]
- ISO 10993-5; 2009-Biological Evaluation of Medical Devices-Part 5: Tests for In Vitro Cytotoxicity. International Organization for Standardization: Geneve, Switzerland, 2009.
- Toz, T.; Kiremitci, A.; Cakmak, A.S.; Tan, O.U.; Palaska, E.; Gumusderelioglu, M.; Ozcan, M. A comparative study on monomer elution and cytotoxicity of different adhesive restoration materials. J. Adhes. Sci. Technol. 2017, 31, 414–429. [Google Scholar] [CrossRef][Green Version]
- Monterubbianesi, R.; Orsini, G.; Tosi, G.; Conti, C.; Librando, V.; Procaccini, M.; Putignano, A. Spectroscopic and mechanical properties of a new generation of bulk fill composites. Front. Physiol. 2016, 7, 652. [Google Scholar] [CrossRef] [PubMed]
- Murray, P.E.; Smith, A.J. Saving pulps—A biological basis. An overview. Prim. Dent. Care 2002, 9, 21–26. [Google Scholar] [CrossRef]
- Geurtsen, W. Biocompatibility of resin-modified filling materials. Crit. Rev. Oral Biol. Med. 2000, 11, 333–355. [Google Scholar] [CrossRef]
- Schedle, A.; Franz, A.; Rausch-Fan, X.; Spittler, A.; Lucas, T.; Samorapoompichit, P.; Sperr, W.; Boltz-Nitulescu, G. Cytotoxic effects of dental composites, adhesive substances, compomers and cements. Dent. Mater. 1998, 14, 429–440. [Google Scholar] [CrossRef]
- Selimović-Dragaš, M.; Huseinbegović, A.; Kobašlija, S.; Hatibović-Kogfman, S. A comparison of the in vitro cytotoxicity of conventional and resin modified glass ionomer cements. Bosn. J. Basic Med. Sci. 2012, 12, 273–278. [Google Scholar] [CrossRef]
- Ulker, H.E.; Sengun, A. Cytotoxicity evaluation of self adhesive composite resin cements by dentin barrier test on 3D pulp cells. Eur. J. Dent. 2009, 3, 120–126. [Google Scholar] [CrossRef]
- Cao, T.; Saw, T.Y.; Heng, B.C.; Liu, H.; Yap, A.U.J.; Ng, M.L. Comparison of different test models for the assessment of cytotoxicity of composite resins. J. Appl. Toxicol. 2005, 25, 101–108. [Google Scholar] [CrossRef]
- Taira, M.; Nakao, H.; Matsumoto, T.; Takahashi, J. Cytotoxic effect of methyl methacrylate on 4 cultured fibroblasts. Int. J. Prosthodont. 2000, 13, 311–315. [Google Scholar] [PubMed]
- Saw, T.Y.; Cao, T.; Yap, A.U.J.; Ng, M.M.L. Tooth slice organ culture and established cell line culture models for cytotoxicity assessment of dental materials. Toxicol. In Vitro 2005, 19, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Thonemann, B.; Schmalz, G.; Hiller, K.A.; Schweikl, H. Responses of L929 mouse fibroblasts, primary and immortalized bovine dental papilla-derived cell lines to dental resin components. Dent. Mater. 2002, 18, 318–323. [Google Scholar] [CrossRef]
- Skin, H.-P.A. Mucosal reactions associated with dental materials. Eur. J. Oral Sci. 1998, 106, 707–712. [Google Scholar]
- Wataha, J.C.; Lockwood, P.E.; Bouillaguet, S.; Noda, M. In vitro biological response to core and flowable dental restorative materials. Dent. Mater. 2003, 19, 25–31. [Google Scholar] [CrossRef]
- Kazak, M.; Donmez, N.; Bahadori, F.; Yenigun, V.B.; Kocyigit, A. Investigation of in vitro cytotoxic effects of different content bulk-fill materials polymerized with a new generation light curing unit and determination of cytotoxicity origins by LC-MS/MS method. In Proceedings of the Turkish Society of Restorative Dentistry, 23rd International Scientific Congress, Antalya, Turkey, 6–8 December 2019; Abstract Book. pp. 114–115. [Google Scholar]
- López-García, S.; Pecci-Lloret, M.P.; Pecci-Lloret, M.R.; Oñate-Sánchez, R.E.; García-Bernal, D.; Castelo-Baz, P.; Rodríguez-Lozano, F.J.; Guerrero-Gironés, J. In vitro evaluation of the biological effects of ACTIVA Kids BioACTIVE restorative, Ionolux, and Riva Light Cure on human dental pulp stem cells. Materials 2019, 12, 3694. [Google Scholar] [CrossRef]
- Karabulut, B.; Donmez, N.; Goret, C.C.; Atas, C.; Kuzu, O. Reactions of subcutaneous connective tissue to mineral trioxide aggregate, Biodentine®, and a newly developed BioACTIVE Base/Liner. Scanning 2020, 2020, 6570159. [Google Scholar] [CrossRef]
- Eckhardt, A.; Harorli, T.; Limtanyakul, J.; Hiller, K.A.; Bosl, C.; Bolay, C.; Reichl, F.X.; Schmalz, G.; Schweikl, H. Inhibition of cytokine and surface antigen expression in LPS-stimulated murine macrophages by triethylene glycol dimethacrylate. Biomaterials 2009, 30, 1665–1674. [Google Scholar] [CrossRef]
- Ferracane, J. Elution of leachable components from composites. J. Oral Rehabil. 1994, 21, 441–452. [Google Scholar] [CrossRef]
- Kanjevac, T.; Milovanovic, M.; Volarevic, V.; Lukic, M.L.; Arsenijevic, N.; Markovic, D.; Zdravkovic, N.; Tesic, Z.; Lukic, A. Cytotoxic effects of glass ionomer cements on human dental pulp stem cells correlate with fluoride release. Med. Chem. 2012, 8, 40–45. [Google Scholar] [CrossRef]
- Demirel, G.; Gur, G.; Demirsoy, F.F.; Altuntas, E.G.; Yener-Ilce, B.; Kilicarslan, M.A. Cytotoxic effects of contemporary bulk-fill dental composites: A real-time cell analysis. Dent. Mater. J. 2020, 39, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Toh, W.; Yap, A.; Lim, S. In vitro biocompatibility of contemporary bulk-fill composites. Oper. Dent. 2015, 40, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Yoruc, A.B.H.; Kızılbey, K.A.; Karaul, A.; Cakmakcioglu, O. Effects of curing systems and light units on cytotoxicity of dental composites. IJOER 2016, 2, 117–126. [Google Scholar]
- Goncalves, F.; Campos, L.M.P.; Rodrigues-Júnior, E.C.; Costa, F.V.; Marques, P.A.; Francci, C.E.; Braga, R.R.; Boaro, L.C.C. A comparative study of bulk-fill composites: Degree of conversion, post-gel shrinkage and cytotoxicity. Braz. Oral Res. 2018, 32, e17. [Google Scholar] [CrossRef]
- Attik, N.; Hallay, F.; Bois, L.; Brioude, A.; Grosgogeat, B.; Colon, P. Mesoporous silica fillers and resin composition effect on dental composites cytocompatibility. Dent. Mater. 2017, 33, 166–174. [Google Scholar] [CrossRef]
- de Souza Costa, C.A.; Hebling, J.; Garcia-Godoy, F.; Hanks, C.T. In vitro cytotoxicity of five glass-ionomer cements. Biomaterials 2003, 24, 3853–3858. [Google Scholar] [CrossRef]
- Imazato, S.; Horikawa, D.; Takeda, K.; Kiba, W.; Izutani, N.; Yoshikawa, R.; Hayashi, M.; Ebisu, S.; Nakano, T. Proliferation and differentiation potential of pluripotent mesenchymal precursor C2C12 cells on resin-based restorative materials. Dent. Mater. J. 2010, 29, 341–346. [Google Scholar] [CrossRef]
- Soderholm, K.J.M. Filler leachability during water storage of six composite materials. Scand. J. Dent. Res. 1990, 98, 82–88. [Google Scholar] [CrossRef]
- Soderholm, K.J.M.; Mukherjee, R.; Longmate, J. Filler leachability of composites stored in distilled water or artificial saliva. J. Dent. Res. 1996, 75, 1692–1699. [Google Scholar] [CrossRef]
- Soderholm, K.J.M.; Yang, M.C.; Garcea, I. Filler particle leachability of experimental dental composites. Eur. J. Oral Sci. 2000, 108, 555–560. [Google Scholar] [CrossRef]
- Bouschlicher, M.R.; Rueggeberg, F.A.; Wilson, B.M. Correlation of bottom-to-top surface microhardness and conversion ratios for a variety of resin composite compositions. Oper. Dent. 2004, 29, 698–704. [Google Scholar] [PubMed]
- Leprince, J.G.; Leveque, P.; Nysten, B.; Gallez, B.; Devaux, J.; Leloup, G. New insight into the “depth of cure” of dimethacrylate-based dental composites. Dent. Mater. 2012, 28, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Jang, J.; Park, S.; Hwang, I. Polymerization shrinkage and depth of cure of bulk-fill resin composites and highly filled flowable resin. Oper. Dent. 2015, 40, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, N.; Jain, A.; Gupta, H.; Abrol, A.; Singh, C.; Rapgay, T. The comparative evaluation of depth of cure of bulk-fill composites—An in vitro study. J. Conserv. Dent. 2019, 22, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Schmalz, G. Use of cell cultures for toxicity testing of dental materials-advantages and limitations. J. Dent. 1994, 22, S6–S11. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).