
Fully Digital Workflow in Full-Arch Implant Rehabilitation: A Descriptive Methodological Review


Abstract
1. Introduction
2. Methods
2.1. Research Methodology
2.2. Article Selection
2.3. Inclusion and Exclusion Criteria
2.4. Selection Process
3. Results
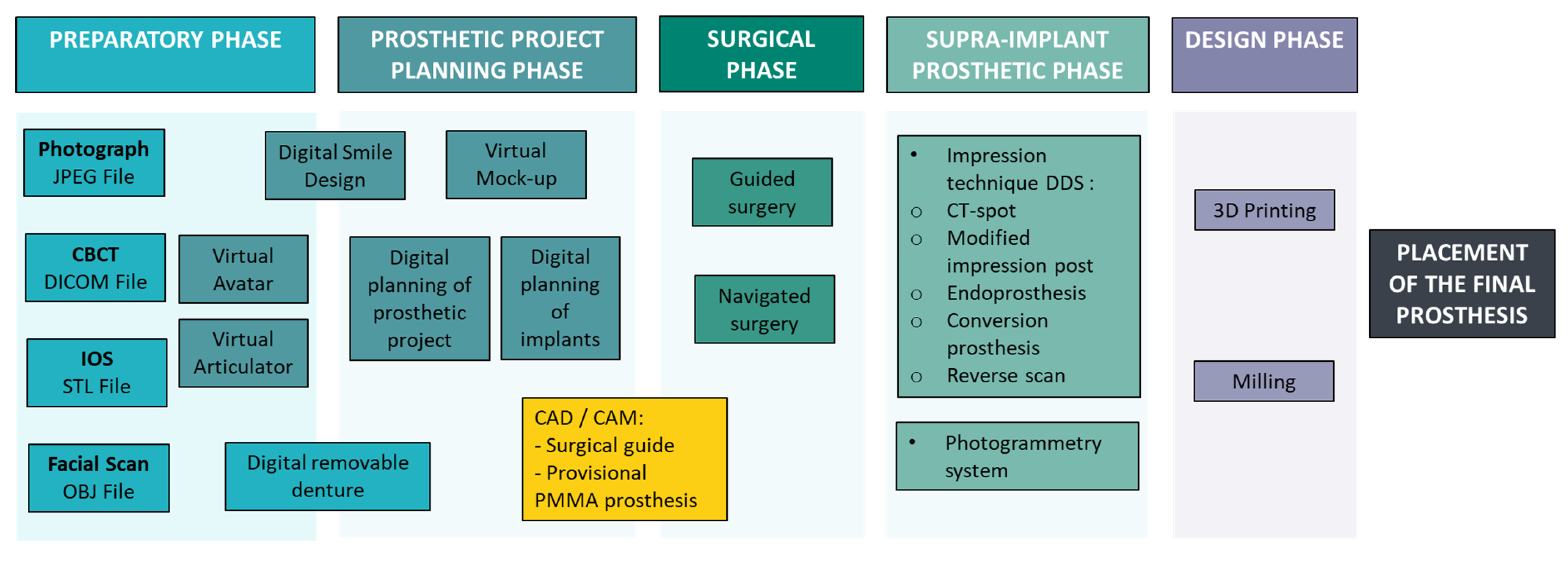
3.1. Preparatory Phase
3.1.1. Cone-Beam Computed Tomography (CBCT)
3.1.2. Intraoral Optical Scanning (IOS)
3.1.3. Digital Smile Design and Virtual Avatar Creation
- -
- Digital smile design (DSD). The digital smile design (DSD) protocol allows clinicians to create a virtual simulation of the patient’s future smile, allowing for non-invasive evaluation and customization of prosthetic outcomes before treatment. This process requires two facial photographs (at rest and in full smile) with an IOS [16,28]. The resulting STL files and images are imported into specialized software, where reference points guide the alignment of 3D dental models with the 2D facial framework [17]. This technology provides a realistic simulation of treatment results, enhancing patient satisfaction and engagement [22]. With CAD software (NemoStudioR, Nemotec SL, Madrid, Spain), a virtual diagnostic wax-up is generated and positioned in accordance with facial midlines and esthetic landmarks, improving communication between the clinician and dental technician and enabling implant planning in harmony with the patient’s facial anatomy [23].
- -
- Three-dimensional facial scanning. Three-dimensional facial scanning systems (Cloner II, Done3D; 3DMD face system) provide a detailed and accurate representation of the patient’s facial anatomy, facilitating advanced treatment planning in both dental and implant therapy [23]. The scans generate OBJ files, which are integrated into planning software (3dMDface System, 3dMD, Atlanta, GA, USA) to create virtual avatars that incorporate facial features, bone structure, dentition, and soft tissues. These virtual representations enable clinicians to conduct comprehensive treatment planning, even in the patient’s absence, and help in determining the need for alveolar ridge reduction to achieve optimal esthetic outcomes [24].
- -
- Virtual articulator. Virtual articulators (Zebris Amann Girrbach Artex Articulator, Zebris, Isny, Germany) embedded in CAD/CAM systems (such as CEREC, 3Shape, or Exocad) simulate mandibular movements similar to mechanical articulators, using average condylar settings to articulate digital models [25]. For full-arch implant-supported prosthetic rehabilitation, key parameters (vertical dimension, centric relation, guidance, and esthetics) are digitally transferred from removable prosthesis to the definitive implant restoration [12]. If no existing prosthesis is available, an interim removable denture is required to establish these parameters [13,14,26].
- -
- Dynamic virtual avatar. Recent advancements have enabled the development of dynamic virtual patients by integrating occlusion data into the digital avatar framework [24] (Figure 4). The static and dynamic relationships between the jaws are recorded using a provisional prosthesis and a mandibular movement tracking system (Jaw Motion analyzer, Zebris, Isny, Germany). A virtual facebow and a reference plane, established via CBCT, are used to mount the digital models on a virtual articulator (Zebris Amann Girrbach Artex Articulator, Zebris, Isny, Germany). The resulting data are then imported into CAD software (Exocad Software; Exocad GmbH, Darm-stadt, Germany) to construct a fully dynamic virtual patient, for precise rehabilitation planning.
3.2. Surgical Phase
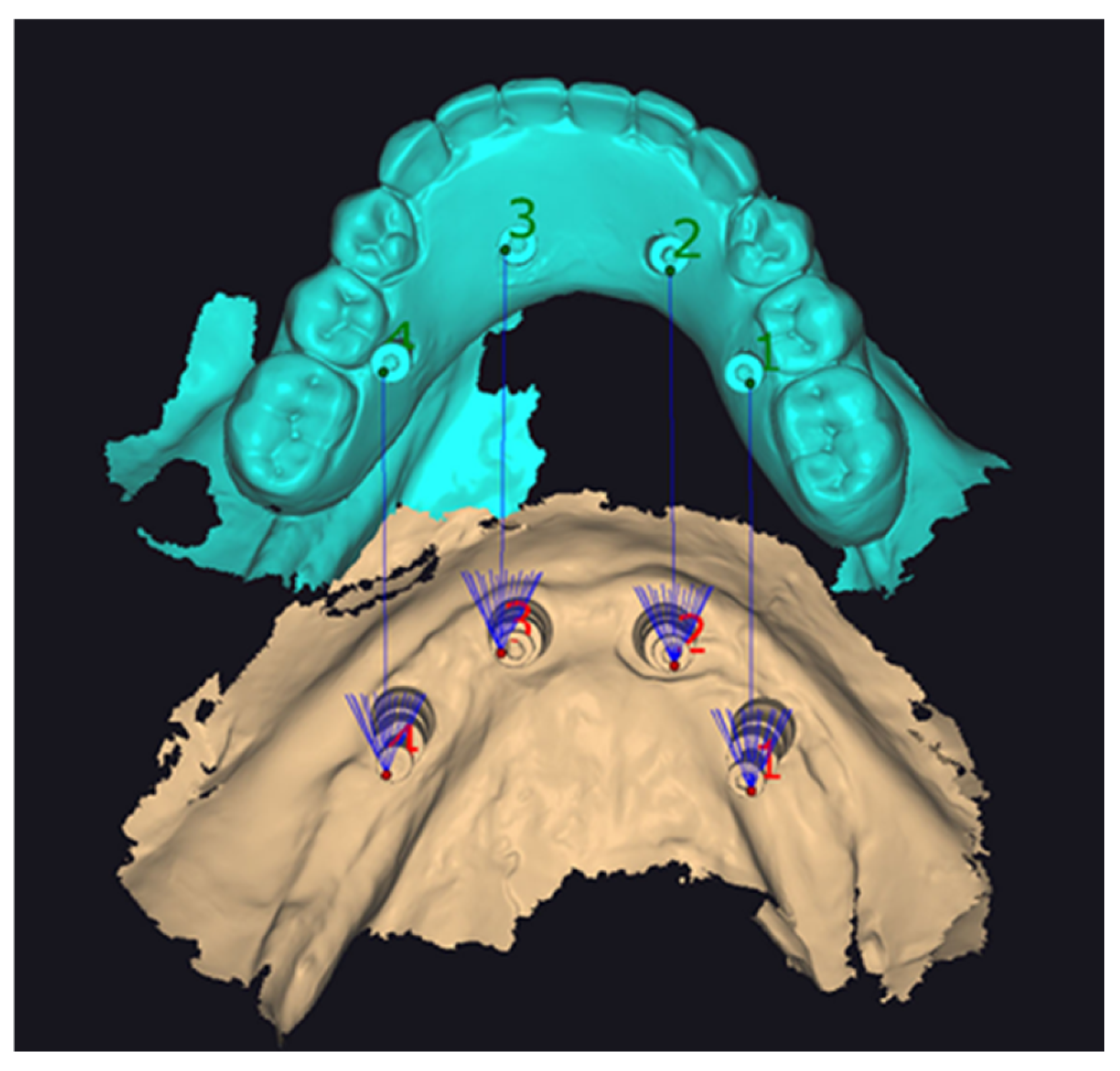
3.2.1. Implant Planning
3.2.2. Surgical Phase: Static Guided Surgery
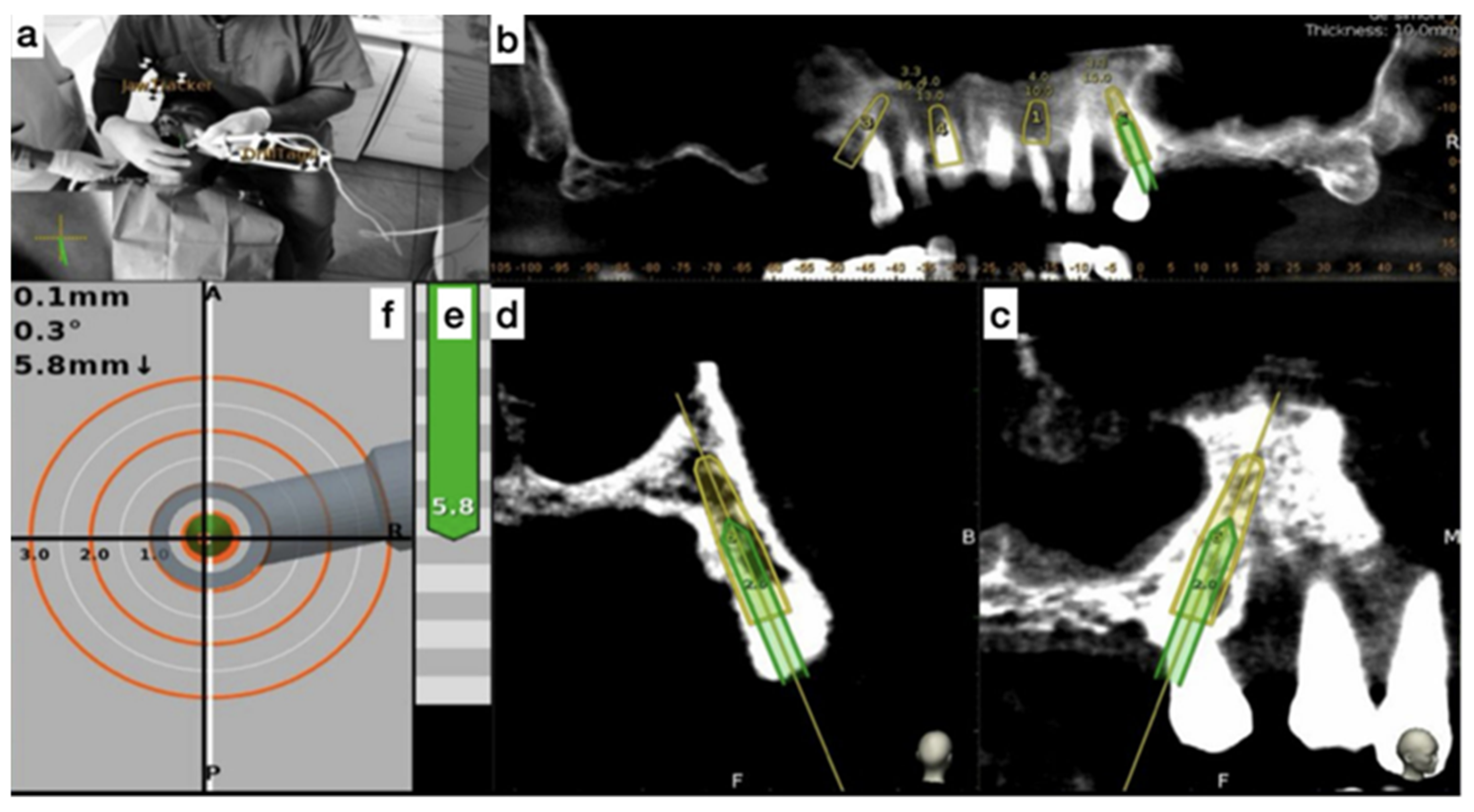
3.2.3. Surgical Phase: Dynamic Navigated Surgery
3.3. Prosthetic Phase
3.3.1. Supra-Implant Digital Impressions
- -
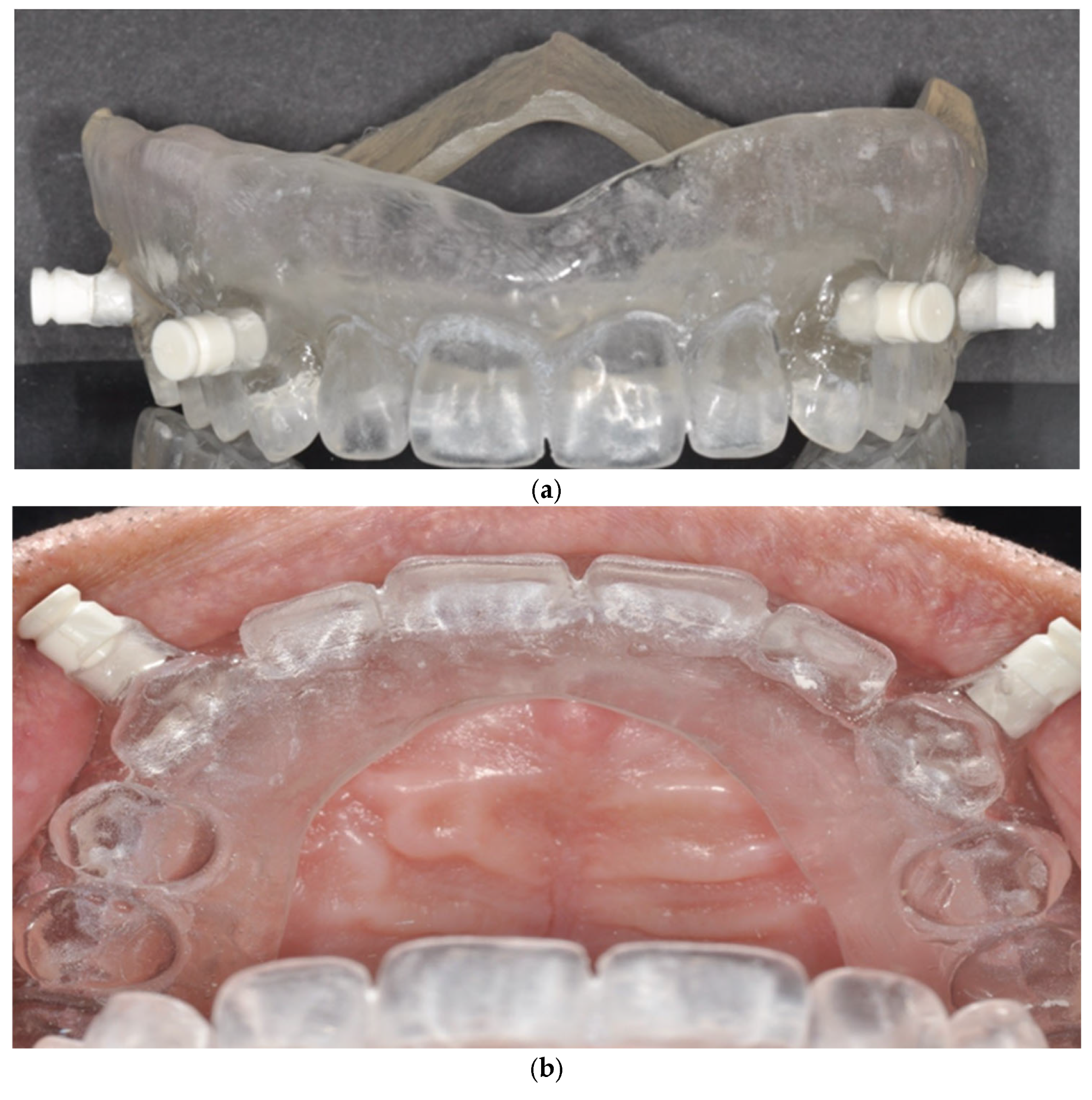
- Double digital scan (DDS) technique. It requires two digital scans of the same arch: the first is a standard supra-implant impression using scan bodies, and the second is performed with an auxiliary device, such as a provisional prosthesis, an existing denture, an endoprosthesis, or a surgical guide. These auxiliary devices are intended to create essential irregularities within the scanning area.
- -
- Photogrammetry system. In this review, only one study employed a photogrammetry system, where scan bodies (ICAM bodies, Imetric4D, Imaging, Switzerland) were attached to screw-retained abutments (SRA abutments, Straumann, Switzerland). Implant position data were recorded using a photogrammetry camera (ICAM 4d camera, Imetric4D Imaging Sarl, Courgenay, Switzerland). This study integrated with other digital data, including IOS, CBCT, facial scans, and a virtual facebow, enabling the fabrication of the final prosthesis [24].
3.3.2. Laboratory Phase
- -
- Three-dimensional Printing. Three-dimensional printing allows the manufacturing of models, surgical guides, endoprostheses, and provisional and definitive prostheses. Mainly used for guides and provisional prostheses, it also offers solutions for permanent prostheses. The materials include PMMA (polymethyl methacrylate) for provisional prostheses, endoprostheses, surgical guides, and resin for surgical guides [12,13,23].
- -
- Milling. Computer-assisted milling is a subtractive technique used in the digital fabrication of dental prostheses. Unlike 3D printing, which is an additive manufacturing process, milling is subtractive: a machine sculpts and shapes a solid block of raw material (such as zirconia, ceramics, titanium, metal alloys, or PMMA disks) to achieve the desired prosthetic form [2,12,18,26]. One study evaluating 16 edentulous maxillae found that PMMA prototypes fabricated via milling using the DDS technique achieved a perfect fit with no difference based on implant number [31]. Furthermore, monolithic zirconia shows promise as a durable prosthetic material for full-arch implant-supported restorations, potentially reducing clinical visits and minimizing common prosthetic complications such as the chipping or fracture of veneering porcelain [23].
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bonnet, G.; Batisse, C.; Travers, C.; Bessadet, M. Integration of CAD/CAM Technology in Global Dental Prosthetic Treatment: A Case Report. Int. Multispecialty J. Health 2016, 2, 9–12. [Google Scholar]
- Marinis, A.; Papaspyridakos, P.; Sicilia, E.; Bernardes, S.R.; Touloumi, F.; Chochlidakis, K.; Weber, H.-P. Digital Workflow for Double Complete Arch Zirconia Prostheses Utilizing a Novel Scan Body. J. Prosthodont. 2022, 31, 4–8. [Google Scholar] [CrossRef]
- El Osta, N.; Haddad, E.; Fakhouri, J.; Saad, R.; El Osta, L. Comparison of Psychometric Properties of GOHAI, OHIP-14, and OHIP-EDENT as Measures of Oral Health in Complete Edentulous Patients Aged 60 Years and More. Qual. Life Res. 2021, 30, 1199–1213. [Google Scholar] [CrossRef] [PubMed]
- El Osta, N.; Bessadet, M.; Drancourt, N.; Batisse, C. Time Efficiency and Cost of Fabricating Removable Complete Dentures Using Digital, Hybrid, and Conventional Workflows: A Systematic Review. J. Prosthet. Dent. 2025, 133, 1194–1208. [Google Scholar] [CrossRef] [PubMed]
- Batisse, C.; Nicolas, E. Comparison of CAD/CAM and Conventional Denture Base Resins: A Systematic Review. Appl. Sci. 2021, 11, 5990. [Google Scholar] [CrossRef]
- Drancourt, N.; Auduc, C.; Mouget, A.; Mouminoux, J.; Auroy, P.; Veyrune, J.-L.; El Osta, N.; Nicolas, E. Accuracy of Conventional and Digital Impressions for Full-Arch Implant-Supported Prostheses: An In Vitro Study. J. Pers. Med. 2023, 13, 832. [Google Scholar] [CrossRef]
- El Osta, N.; Bessadet, M.; Drancourt, N.; Nicolas, E.; Batisse, C. Response to Letter to the Editor Regarding, “Time Efficiency and Cost of Fabricating Removable Complete Dentures Using Digital, Hybrid, and Conventional Workflows: A Systematic Review” by El Osta et al. J. Prosthet. Dent. 2025, 134, 285–286. [Google Scholar] [CrossRef]
- Tohme, H.; Lawand, G.; Chmielewska, M.; Makhzoume, J. Comparison between Stereophotogrammetric, Digital, and Conventional Impression Techniques in Implant-Supported Fixed Complete Arch Prostheses: An in Vitro Study. J. Prosthet. Dent. 2023, 129, 354–362. [Google Scholar] [CrossRef]
- Lawand, G.; Ismail, Y.; Revilla-León, M.; Tohme, H. Effect of Implant Scan Body Geometric Modifications on the Trueness and Scanning Time of Complete Arch Intraoral Implant Digital Scans: An in Vitro Study. J. Prosthet. Dent. 2024, 131, 1189–1197. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Beretta, M.; Poli, P.P.; Tansella, S.; Aguzzi, M.; Meoli, A.; Maiorana, C. Cast-Free Digital Workflow for Implant-Supported Rehabilitation in a Completely Edentulous Patient: A Clinical Report. J. Prosthet. Dent. 2021, 125, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Venezia, P.; Torsello, F.; Santomauro, V.; Dibello, V.; Cavalcanti, R. Full Digital Workflow for the Treatment of an Edentulous Patient with Guided Surgery, Immediate Loading and 3D-Printed Hybrid Prosthesis: The BARI Technique 2.0. A Case Report. Int. J. Environ. Res. Public Health 2019, 16, 5160. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; De Souza, A.; Bathija, A.; Kang, K.; Chochlidakis, K. Complete Digital Workflow for Mandibular Full-Arch Implant Rehabilitation in 3 Appointments. J. Prosthodont. 2021, 30, 548–552. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; Chochlidakis, K.; Kang, K.; Chen, Y.-W.; Alghfeli, A.; Kudara, Y.; Weber, H.-P. Digital Workflow for Implant Rehabilitation with Double Full-Arch Monolithic Zirconia Prostheses. J. Prosthodont. 2020, 29, 460–465. [Google Scholar] [CrossRef]
- Meneghetti, P.; Moura, G.F.; Tavelli, L.; Li, J.; Siqueira, R.; Wang, H.-L.; Mendonça, G. A Fully Digital Approach for Implant Fixed Complete Dentures: A Case Report. J. Esthet. Restor. Dent. 2021, 33, 1070–1076. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Bedrossian, A.; De Souza, A.; Bokhary, A.; Gonzaga, L.; Chochlidakis, K. Digital Workflow in Implant Treatment Planning For Terminal Dentition Patients. J. Prosthodont. 2022, 31, 543–548. [Google Scholar] [CrossRef]
- Roberts, M.; Shull, F.; Schiner, B. Maxillary Full-Arch Reconstruction Using a Sequenced Digital Workflow. J. Esthet. Restor. Dent. 2020, 32, 336–356. [Google Scholar] [CrossRef]
- Sobczak, B.; Majewski, P. An Integrated Fully Digital Prosthetic Workflow for the Immediate Full-Arch Restoration of Edentulous Patients-A Case Report. Int. J. Environ. Res. Public Health 2022, 19, 4126. [Google Scholar] [CrossRef]
- Martins, J.; Rangel, J.; Nobre, M.d.A.; Ferro, A.; Nunes, M.; Almeida, R.; Guedes, C.M. A New Full Digital Workflow for Fixed Prosthetic Rehabilitation of Full-Arch Edentulism Using the All-on-4 Concept. Medicina 2024, 60, 720. [Google Scholar] [CrossRef]
- Bedrossian, E.A.; Papaspyridakos, P.; Bedrossian, E.; Gurries, C. The Reverse Scan Body Protocol: Completing the Digital Workflow. Compend. Contin. Educ. Dent. 2023, 44, e1–e4. [Google Scholar]
- Carosi, P.; Ferrigno, N.; De Renzi, G.; Laureti, M. Digital Workflow to Merge an Intraoral Scan and CBCT of Edentulous Maxilla: A Technical Report. J. Prosthodont. 2020, 29, 730–732. [Google Scholar] [CrossRef]
- Neto, A.D.T.; Costa, A.J.d.M.E.; Gil Choi, I.G.; Santos, A.; Dos Santos, J.F.; Cortes, A.R.G. Digital Workflow for Full-Arch Implant-Supported Prosthesis Based on Intraoral Scans of a Relative of the Patient. J. Oral Implant. 2020, 47, 68–71. [Google Scholar] [CrossRef]
- Costa, A.J.d.M.; Neto, A.D.T.; Burgoa, S.; Gutierrez, V.; Cortes, A.R.G. Fully Digital Workflow with Magnetically Connected Guides for Full-Arch Implant Rehabilitation Following Guided Alveolar Ridge Reduction. J. Prosthodont 2020, 29, 272–276. [Google Scholar] [CrossRef]
- Wang, J.; Wu, Y.-L.; Ma, J.; Wu, F.; Li, D.-H. A Novel Technique for Implant-Supported Fixed Complete Rehabilitation Based on a Dynamic Virtual Patient. J. Dent. 2023, 137, 104649. [Google Scholar] [CrossRef]
- Lepidi, L.; Chen, Z.; Ravida, A.; Lan, T.; Wang, H.-L.; Li, J. A Full-Digital Technique to Mount a Maxillary Arch Scan on a Virtual Articulator. J. Prosthodont. 2019, 28, 335–338. [Google Scholar] [CrossRef]
- Parpaiola, A.; Toia, M.; Norton, M.; Rodriguez, Y.; Baena, R.; Todaro, C.; Lupi, S.M. Fully Digital Workflow for Implant-Supported Fixed Restorations Consisting of a Titanium Primary Structure and a Zirconia Secondary Structure. Int. J. Oral Implant. 2023, 16, 351–358. [Google Scholar]
- Ragazzini, N.; Dds, P.B.; Monaco, C.; Ciocca, L. Digital Jaw Relation Record of Edentulous Patients in the CAD-CAM Workflow of the Implant-Supported Full-Arch Prosthesis. J Oral Implant. 2020, 47, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Cattoni, F.; Chirico, L.; Merlone, A.; Manacorda, M.; Vinci, R.; Gherlone, E.F. Digital Smile Designed Computer-Aided Surgery versus Traditional Workflow in “All on Four” Rehabilitations: A Randomized Clinical Trial with 4-Years Follow-Up. Int. J. Environ. Res. Public Health 2021, 18, 3449. [Google Scholar] [CrossRef] [PubMed]
- Stefanelli, L.V.; Mandelaris, G.A.; Franchina, A.; Pranno, N.; Pagliarulo, M.; Cera, F.; Maltese, F.; Angelis, F.D.; Carlo, S.D. Accuracy of Dynamic Navigation System Workflow for Implant Supported Full Arch Prosthesis: A Case Series. Int. J. Environ. Res. Public Health 2020, 17, 5038. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Vazouras, K.; Gotsis, S.; Bokhary, A.; Sicilia, E.; Kudara, Y.; Bedrossian, A.; Chochlidakis, K. Complete Digital Workflow for Prosthesis Prototype Fabrication with Double Digital Scanning: A Retrospective Study with 45 Edentulous Jaws. J. Prosthodont. 2023, 32, 571–578. [Google Scholar] [CrossRef]
- Chochlidakis, K.; Romeo, D.; Ercoli, C.; Papaspyridakos, P. Complete Digital Workflow for Prosthesis Prototype Fabrication with the Double Digital Scanning (DDS) Technique: A Prospective Study on 16 Edentulous Maxillae. J. Prosthodont. 2022, 31, 761–765. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author(s) | Study Design | Level of Evidence | Key Findings |
|---|---|---|---|
| Lepidi et al., 2019 [25] | Technical report | Level IV | Digital technique for aligning maxillary scans on a virtual articulator. |
| Venezia et al., 2019 [12] | Case report | Level IV | BARI 2.0 technique with 3D-printed hybrid prosthesis, guided surgery, and immediate loading. |
| Papaspyridakos et al., 2020 [14] | Case series | Level IV | Fully digital workflow for double full-arch monolithic zirconia prostheses. |
| Stefanelli et al., 2020 [29] | Case series | Level IV | Evaluated accuracy of dynamic navigation system for full-arch digital implant workflow. |
| Roberts et al., 2020 [17] | Case report | Level IV | Sequenced digital workflow for maxillary full-arch implant reconstruction. |
| Carosi et al., 2020 [21] | Technical report | Level IV | Merging intraoral scan with CBCT for edentulous maxilla rehabilitation. |
| Costa et al., 2020 [23] | Case report | Level IV | Application of magnetically retained guides in digital full-arch rehabilitation. |
| Ragazzini et al., 2021 [27] | Case report | Level IV | Digital jaw relation record in CAD-CAM workflow for full-arch prosthesis. |
| Papaspyridakos et al., 2021 [13] | Case report | Level IV | Complete digital workflow for mandibular full-arch implant rehabilitation completed in three visits. |
| Beretta et al., 2021 [11] | Case report | Level IV | Cast-free digital workflow in a completely edentulous patient. |
| Meneghetti et al., 2021 [15] | Case report | Level IV | Fully digital approach for implant-supported complete dentures. |
| Neto et al., 2021 [22] | Case report | Level IV | Digital workflow using intraoral scanning for full-arch prosthesis fabrication. |
| Cattoni et al., 2021 [28] | Randomized clinical trial | Level II | Comparison of digital vs. conventional workflows in All-on-4 implant rehabilitation. |
| Marinis et al., 2022 [2] | Case report | Level IV | Innovative scan body use for double full-arch zirconia prostheses via digital workflow. |
| Papaspyridakos et al., 2022 [16] | Case report | Level IV | Digital workflow in implant treatment planning for terminal dentition patients. |
| Chochlidakis et al., 2022 [31] | Prospective study | Level III | Use of double digital scanning technique in 16 fully edentulous maxillae. |
| Sobczak & Majewski, 2022 [18] | Case report | Level IV | Immediate full-arch restoration utilizing a fully digital workflow. |
| Wang et al., 2023 [24] | Case report | Level IV | Rehabilitation of edentulous patients using a dynamic virtual patient approach. |
| Bedrossian et al., 2023 [20] | Technical report | Level IV | Reverse scan body protocol to streamline fully digital workflow in full-arch rehabilitation. |
| Parpaiola et al., 2023 [26] | Case report | Level IV | Fully digital protocol with titanium primary and zirconia secondary structures. |
| Papaspyridakos et al., 2023 [30] | Retrospective study | Level III | Evaluation of double digital scanning technique in 45 edentulous jaws. |
| Martins et al., 2024 [19] | Case series | Level IV | Fully digital All-on-4 workflow for fixed full-arch supported prosthesis. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Auduc, C.; Douillard, T.; Nicolas, E.; El Osta, N. Fully Digital Workflow in Full-Arch Implant Rehabilitation: A Descriptive Methodological Review. Prosthesis 2025, 7, 85. https://doi.org/10.3390/prosthesis7040085
Auduc C, Douillard T, Nicolas E, El Osta N. Fully Digital Workflow in Full-Arch Implant Rehabilitation: A Descriptive Methodological Review. Prosthesis. 2025; 7(4):85. https://doi.org/10.3390/prosthesis7040085
Chicago/Turabian StyleAuduc, Chantal, Thomas Douillard, Emmanuel Nicolas, and Nada El Osta. 2025. "Fully Digital Workflow in Full-Arch Implant Rehabilitation: A Descriptive Methodological Review" Prosthesis 7, no. 4: 85. https://doi.org/10.3390/prosthesis7040085
APA StyleAuduc, C., Douillard, T., Nicolas, E., & El Osta, N. (2025). Fully Digital Workflow in Full-Arch Implant Rehabilitation: A Descriptive Methodological Review. Prosthesis, 7(4), 85. https://doi.org/10.3390/prosthesis7040085