1. Introduction
Acute Otitis Media (AOM) is the most commonly-occurring bacterial complication in childhood, generally presenting alongside upper respiratory infections (URIs). It occurs most frequently in children under 2 years of age, and is one of the most common causes of consultation with primary care paediatricians (25–40%). It is estimated that 2 out of every 3 children suffer an episode before their first birthday, and over 90% do so before reaching the age of 5. It is the leading reason for the prescription of antibiotics for children. The pathogens most commonly involved in AOM are Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis [
1,
2]. Viruses are a contributing factor in AOM, but no direct role as the cause of inflammation of the middle ear has been proven. One study concluded that AOM has a major impact on health, given the high number of consultations, use of antibiotics, related surgery and the need for auditory rehabilitation [
3].
There is a high rate of relapse, leading to recurrent acute otitis media (RAOM). Thirty-three percent of children under 3 years of age have suffered 3 or more episodes and 10–20% of all children present repeat episodes of AOM [
4,
5]. Multiple preventative measures have been proposed for RAOM, such as not attending nursery, avoiding passive smoking and allergen exposure, inoculation against influenza, limiting the use of pacifiers [
6], the administration of probiotics [
7], and vaccination against pneumococcus, with insignificant results [
8,
9]. Prophylactic antibiotics have also been proposed during the colder months of the years, in 3–6-month cycles; no satisfactory results have been obtained [
10]. Finally, adenoidectomy and the insertion of grommets has also been recommended, with contradicting results [
11].
There is little available literature linking diet to the development of RAOM. Breastfeeding has been highlighted as a highly effective protection factor during early infancy. Unfortunately, the protective effect disappears before the end of breastfeeding [
12], at the time when weaning starts. Studies performed by our group on the role of the Mediterranean Diet in recurrent inflammatory processes during childhood, have revealed a significant reduction in URI and its most common bacterial complications, after modifying certain feeding errors in the patients’ diet. In line with our main line of argument in which we link recurrent inflammatory episodes with cessation of the Mediterranean diet, we considered completing this study on the effects of the Traditional Mediterranean Diet (TMD) [
13,
14,
15,
16,
17,
18] in patients diagnosed with RAOM.
3. Results
According to the sample size calculation, the programme “Learning to eat the Mediterranean Way” was proposed for the families of 104 patients meeting the inclusion criteria, of which, 4 opted not to take part. Of the 100 patients initially included, 5 abandoned the programme after the first session and a further 2 after the fourth session. Five left for social or personal difficulties in adopting the diet, while the other two did not agree with the limitation of certain foods. Three patients were excluded after surgical intervention by ENT specialists, not coordinated with our team. The study was therefore completed by a total of 90 patients, of which 48 were female and 42 male, with an average age of 2.9 years (
Table 4).
All the patients included in the study were assessed after 4 months and 12 months by the nutritionist and the paediatrician. The results obtained were similar in both sexes, and so they are treated jointly hereafter. The number of episodes of AOM decreased from 3.84 ± 0.73 in the previous year, compared to 0.48 ± 0.65 (
p < 0.001) during the year of treatment. The level of intensity of AOM dropped from 1.6 ± 0.65 (mild-moderate) to 0.09 ± 0.18 (
p < 0.001) (none-mild). URIs decreased from 6.56 ± 1.45 to 2.64 ± 1.45 (
p < 0.001). The need to go to the emergency room also decreased from 2.1 ± 0.89 occasions per year, to 0.35 ± 0.21 (
p < 0.001).
Table 5 shows the data from the previous year and at the end of the study year.
The level of family satisfaction was high, as shown on the questionnaire, in terms of the improvement observed (
Table 1) which was completed by all the participating tutors. The anthropometric variables before the study, at 4 months and after the process, are shown in
Table 6.
The patients’ eating habits had also improved across the sample at the end of the programme. So, there was an increase in the number of patients eating fruit, vegetables, whole grains and fermented dairy produce; similarly, there was a drop in the number of patients who did not have breakfast or who would eat factory-baked goods, as well as the proportion of patients eating sweets on a daily basis. According to this data, the average score on the KidMed scale showed a positive evolution, from a mid-high rating at the start of the process to an optimum rating at the end (
Table 7).
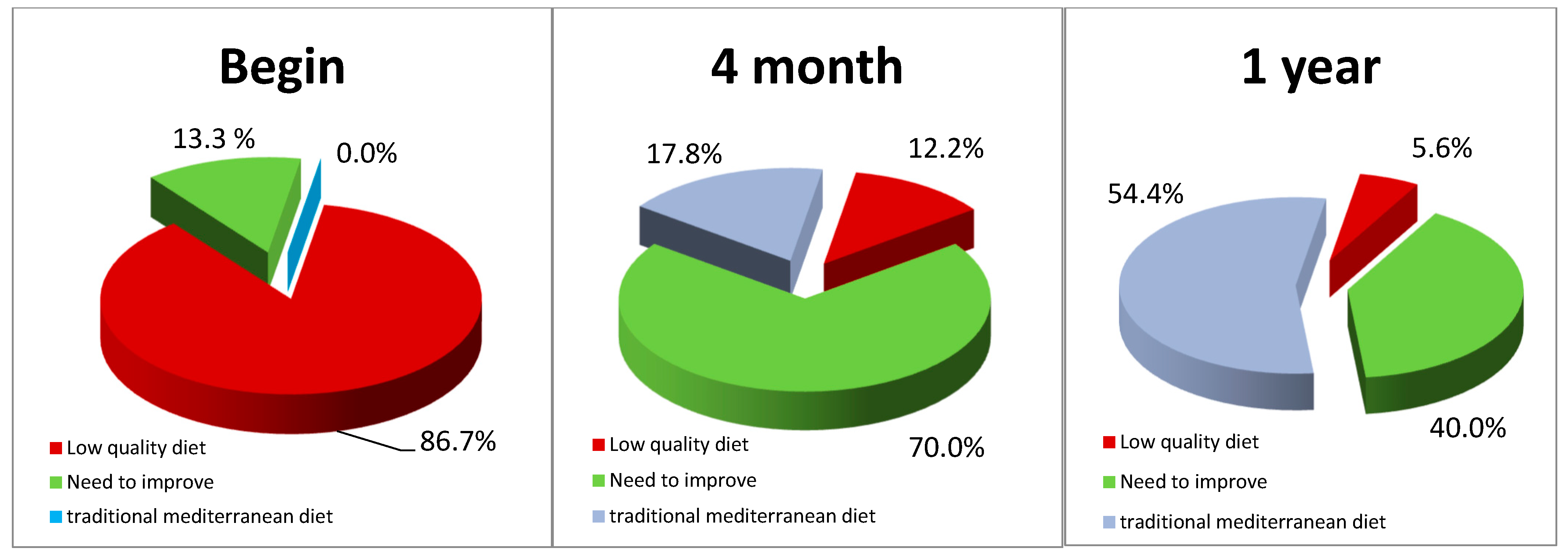
The TMD test also showed a satisfactory evolution, from low quality levels to optimum levels (
Table 8 and
Figure 1). Of the 17 children who were asked for inflammatory markers, all had elevated TNF-alpha and some also raised other markers such as IL-1, IL-6 and PCR-hs. These values were negativized in 16 patients at the end of the nutritional treatment, while the symptoms disappeared.
4. Discussion
We are studying the effects of the Mediterranean Diet on inflammatory diseases that affect the ENT area. We promote an original way of treating these diseases, since until now the conventional treatment is based on pharmacological and surgical treatment. From our point of view, the mucosa that covers the entire ENT area is in a pro-inflammatory and hyper-reactive state, as a consequence of the alterations produced by an inadequate diet. For us there is no difference in the nutritional treatment of the different mucous membranes that cover the ENT area. We have published several studies, in which we apply nutritional therapy in recurrent inflammatory diseases of the ENT area, such as recurrent acute rhinosinusitis, recurrent colds, otitis media with effusion, persistent nasal obstruction, recurrent wheezing (childhood asthma) and now this study on RAOM [
13,
14,
15,
16,
17,
18]. We believe that it has a place in this special issue, since it is a good example of nutritional therapy in mucositis, which affects the ENT area. The results have been very satisfactory. It is the same treatment that we apply to recurrent rhinosinusitis, and we believe that the pathogenic mechanisms involved are the same. In the editorial that presides over this special issue: “Promotion and restoration of health with the amazing Mediterranean Diet vs an increase in childhood pathology due to the disastrous Diet of ‘Western civilization”, we explain more extensively the need to improve the food diet, if we want to solve the great inflammatory problems that affect the mucous membranes (-itis). In short, we are trying to show a global view of the alterations that affect the ENT mucosa. and we believe that this article can be a good example to understand the effects of the Mediterranean Diet on different inflammatory and recurrent diseases, as the title of this special issue indicates. According to our results, the Mediterranean diet is capable of preventing and contributing to the resolution of most inflammatory diseases of the ENT area.
Given the results obtained, we consider than a high nutritional quality diet such as the Traditional Mediterranean Diet can significantly reduce the prevalence of recurrent AOM and prevent pharmacological and surgical intervention. At the end of the intervention year, none of the patients treated met the criteria for classification as recurrent AOM. 60% of the patients did not have any AOM again, and 28% only one, when the usual thing with the conventional treatment is that new episodes had been repeated and had ended up in the ENT specialist consultation, many of them being intervened with tubal implants and/or adenoidectomy. The number of AOM episodes decreased by 87.5%, from an average of almost 4, to less than 0.5% episodes per year.
Although the effectiveness of the immune system increases with age and recurrent episodes spontaneously disappear, neither could such a convincing and satisfactory evolution be prevented, preventing patients from having surgery. Even the youngest children stopped having AOM within a few weeks of starting nutritional therapy. We observed a notable decrease in the degree of intensity of AOM, such that in addition to a reduction in total AOM cases, patients who followed nutritional guidelines experienced fewer symptoms. It is important to note that during the time that the incorporation of patients to the study lasted, we extended the application of TMD to the entire paediatric population (siblings, relatives, patients with other recurrent pathologies, and infants under two years of age). This led to a progressive decrease in patients diagnosed with AOM, so the achievement of the sample size was delayed [
29].
As we have verified in previous studies [
14], URIs, which are among the main factors predisposing patients for inflammation in the middle ear, decreased notably [
30]. In our study, we observed a 60% reduction in URIs compared to the previous year. Likewise, intense pain as a result of AOM is one of the most frequent causes of paediatric emergencies, and we observed a significant reduction of 83.5% in such emergencies compared to the previous year. As a consequence of the decrease in URIs and AOM, the use of symptomatic treatment decreased by 63.2%. Likewise, antibiotic treatment was reduced by 86.4%, which indicates the greater benignity of infectious processes. The degree of satisfaction that the parents showed in the clinical evolution test was high, with scores that indicate a good therapeutic and clinical evolution. In the first four months, improvements were already observed with respect to the situation of the previous year, so that loyalty increased and monitoring was easier. There was a good tolerance to the proposed diet, with easy adaptation and without great culinary difficulties. The patients showed satisfactory pondered growth rates. Their weight, height and BMI percentile evolved as expected. A positive result was the slight decrease in BMI and fat mass levels and a small increase in height and lean body mass. The group of patients who underwent blood tests showed a striking elevation of TNF-α as well as, to a lesser extent, other inflammatory markers, which could suggest that a pro-inflammatory diet could alter the inflammatory mechanisms [
31,
32]. Although this data suggests that the intake of healthy food and/or avoiding poor quality food may play a key role in the control of AOM, there are almost no bibliographical references in scientific literature. We find this absence surprising, as if it were taken for granted that the quality of food is not important in the balance and maintenance of the inflammatory and immune system. Our proposal is very simple: let’s give the body the food and lifestyle it needs to defend itself and avoid those factors that harm it. We want to highlight that the majority of published studies on the treatment of RAOM are based on the application of external actions to the organism, such as the use of drugs or surgical intervention. Primary prevention and strengthening of the immune system have not been taken into account, dietary factors have not been considered, when probably the deconfiguration of the inflammatory system and the immune system are at the base of the RAOM [
33,
34]. Research has suggested the protective effect of breastfeeding for at least 6 months, although other risk factors accumulate after that age [
35]. Among them, the early introduction of adapted milk has been noted [
10,
36] as well as the abuse of antibiotics [
37]. A pan-European study [
38] has shown that children consuming excess refined flours and processed animal-based products and a diet poor in fruit and vegetables have high inflammatory markers. This means that overall, they can be considered to be in a pro-inflammatory state. It has also been shown that patients with AOM show altered regulation of key immune mediators during health and pathogenesis, and are susceptible to being treated by an immunomodulatory intervention [
39]. Predominantly eating food with a low glycaemic index/load-typical of TMD—helps to control insulin levels; this hormone may interfere in the formation of anti-inflammatory eicosanoids, by blocking the la ∆-desaturase enzyme [
40]. Similarly, the TMD is rich in vitamins, minerals and antioxidants, many of which are indispensable co-factors in the enzymatic chemical reactions involved in the body’s immune processes. Children with RAOM have been shown to have poor responses of pro-inflammatory cytokines and antiviral chemokines [
41]. HMGB1 (High-mobility group box protein 1) that acts as a mediator between innate and acquired immunity, is overexpressed and can play a role in the progression and recurrence of RAOM acting as an inflammatory marker and cytokine [
42].
The TMD is an ancient diet, dating back to way before documented history, and which has stood the test of time. Many of the foodstuffs eaten as part of the Western diet contain materials not recognised or assimilated by the human body. Many of these products are not absorbed by the intestine, thus encouraging non-specific microflora that is alien to human intestinal microbiota. The excess “antigenic load” inherent in the Western diet of today—which has multiplied available foodstuffs by the thousand—may misadjust our immune system, making it weaker and notably hyperplasic [
43]. Children with RAOM show immaturity in antigen presenting cells with a suboptimal response of T cells and B memory [
44]. The absence of Toll-2 receptors (TLR2) can lead to prolonged inflammation of the middle ear. TLR2 is essential for the timely resolution of inflammation since it has been proven to promote macrophage recruitment and bacterial clearance in the mouse [
45]. The pro-inflammatory actions of PAF (platelec-activating factor) can be favourably modulated with TMD and regulate its metabolism [
46]. The benefits of breastfeeding in the prevention of AOM have been proven, due the presence in breast milk of antibodies, antibacterial enzymes, glycosylated proteins, anti-viral fats and leukocytes [
10], but also due to decoy receptors for bacterial pathogens, such as oligosacarids [
47]. Components that favour the development of standard saprophytic flora, which prevents the development of oto-pathogens [
48]. These components are currently being added to formula milk, to improve its immune boosting quality [
49]. Probiotics are also added, with satisfactory results in the reduction of URI and AOM [
6]. After ceasing breastfeeding, the occurrence of AOM, increases with artificial feeding [
50]. It is important to remember the “transient hypogammaglobulinemia” of infancy. At the age of 12 months, IgA levels are just 20% of those in adults [
51], and it therefore does not seem appropriate to increase the “antigenic load” of an infant’s diet, which under the historical feeding pattern, was limited to breast milk until beyond the age of 18 months, and the introduction of just a few complementary foods. Finally, we must take into account the “intestinal and nasopharyngeal microbiota” [
52]. The mechanisms by which the intestinal flora regulates our immune responses are unclear, but it is seems sensible to encourage the development an microbiota typical of the human species, given that evolution and genetic coding must have established a specific symbiosis between nutrition, intestinal microbiota and immunity that should not be altered [
53,
54].
Among the limitations of the study, we note the impossibility of establishing a control group with standard dietary guidelines, since we had considered them pro-inflammatory and unsuitable for children. We also had difficulty obtaining our sample, since we extended the TMD to the entire paediatric space, which resulted in a reduction in the incidence of AOM. We consider the presence of nutritionists essential to be able to make satisfactory changes in the diet and to be able to reproduce these studies. We believe that the absence of these professionals is the cause of the poor nutrition that our society suffers.
The change in the “medical model” entailed by these research studies should not go unnoticed. It is no longer a question of providing a remedy for an illness using external drugs that are alien to the human defence system. The proposed treatment is based on equipping the body with everything it needs to heal itself. This could be applied to other childhood pathologies, as described in previous publications [
29,
54]. We are still far from a detailed understanding of the complex web of the pathogenic mechanisms of inflammation, the microbiota and its connection to the immune system, but we can take clinical resolution as “evidence”, following the lead of “common sense”, which is none other than a return to basic eating habits: The Traditional Mediterranean Diet. This diet may make an important contribution to the healing and prevention of recurrent AOM.






{kind=link}