
Electrocardiographic Predictors of Mortality: Data from a Primary Care Tele-Electrocardiography Cohort of Brazilian Patients

 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Collection
2.5. Data Analysis
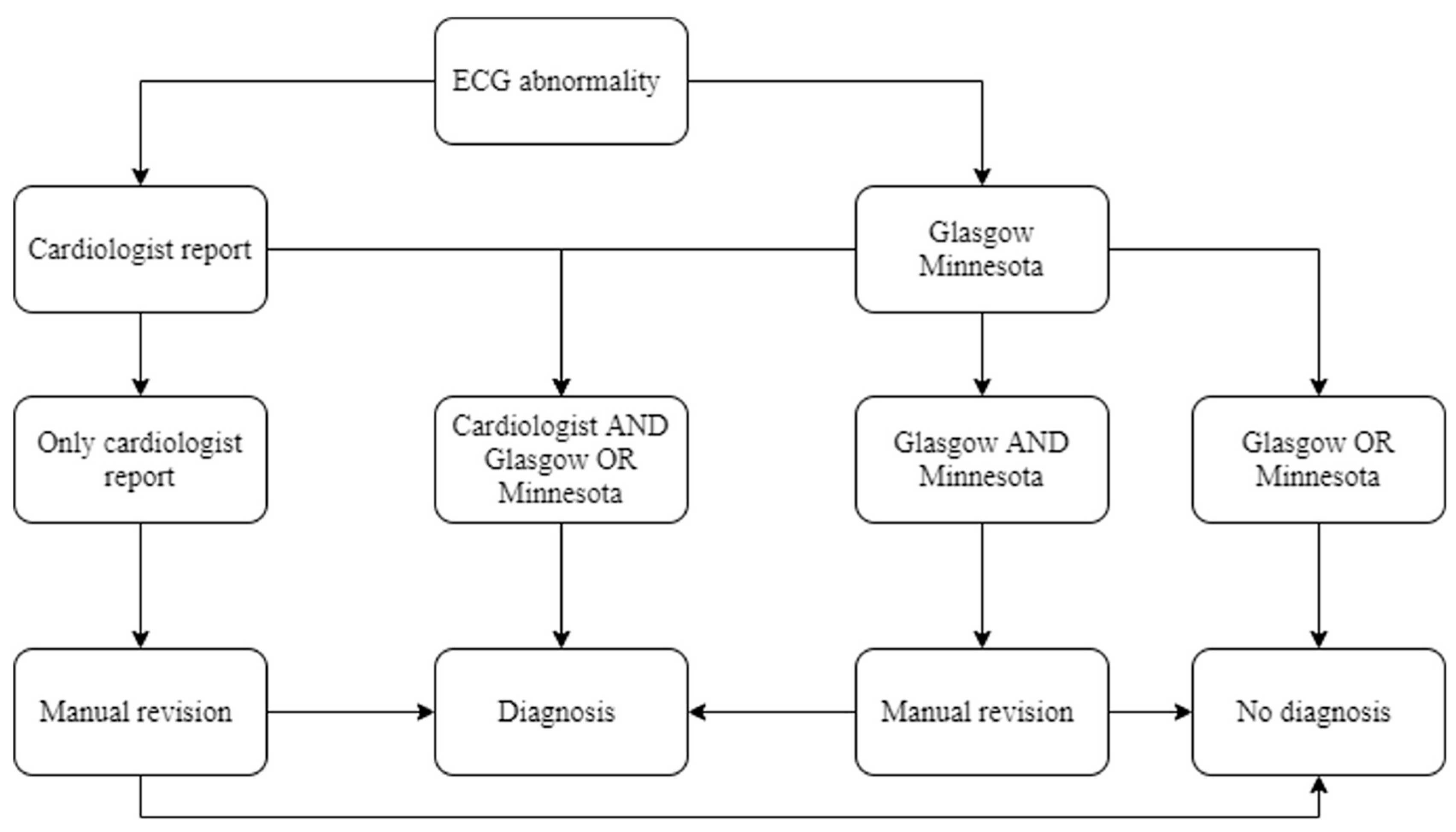
Major Electrocardiographic Abnormalities
2.6. Outcomes
2.7. Probabilistic Linkage
2.8. Statistical Analysis
3. Results
3.1. CODE Cohort
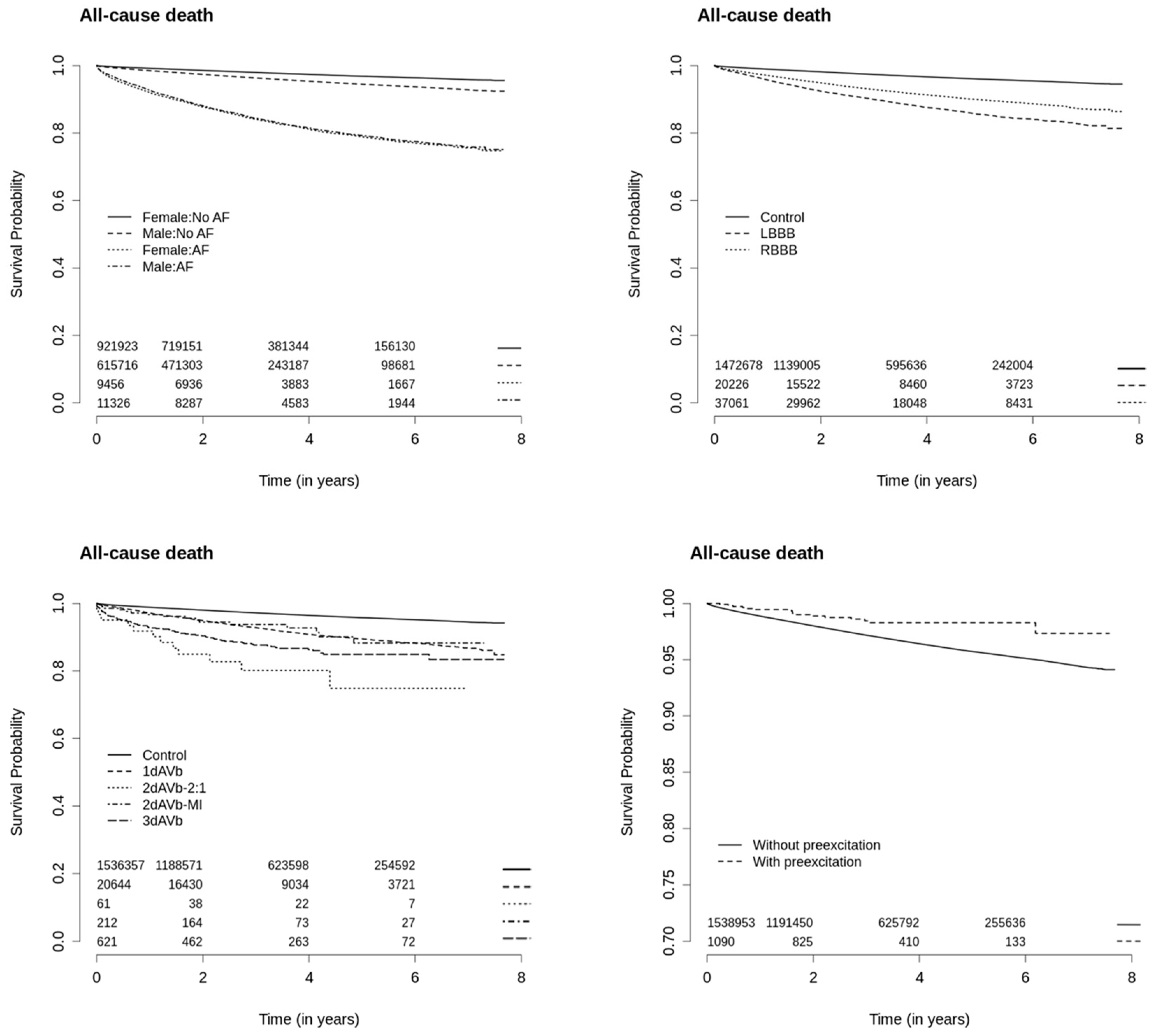
3.2. Survival Analysis: ECG Abnormalities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brant, L.C.C.; Nascimento, B.R.; Passos, V.M.A.; Duncan, B.B.; Bensenõr, I.J.M.; Malta, D.C.; Souza, M.F.M.; Ishitani, L.H.; França, E.; Oliveira, M.S.; et al. Variações e diferenciais da mortalidade por doença cardiovascular no Brasil e em seus estados, em 1990 e 2015: Estimativas do Estudo Carga Global de Doença. Rev. Bras. Epidemiol. 2017, 20 (Suppl. 1), 116–128. [Google Scholar] [CrossRef]
- Dawber, T.R.; Kannel, W.B.; Love, D.E.; Streeper, R.B. The electrocardiogram in heart disease detection; a comparison of the multiple and single lead procedures. Circulation 1952, 5, 559–566. [Google Scholar] [CrossRef]
- Blackburn, H.; Keys, A.; Simonson, E.; Rautaharju, P.; Punsar, S. The electrocardiogram in population studies. A classification system. Circulation 1960, 5, 559–566. [Google Scholar]
- Marty, A.T. Minnesota Code Manual of Electrocardiographic Findings. Crit. Care Med. 1983, 11, 583. [Google Scholar] [CrossRef]
- Blackburn, H.; Taylor, H.L.; Keys, A. Coronary heart disease in seven countries. XVI. The electrocardiogram in prediction of five-year coronary heart disease incidence among men aged forty through fifty-nine. Circulation 1970, 41 (Suppl. 4), 154–161. [Google Scholar] [CrossRef] [PubMed]
- Kannel, W.B.; Gordon, T.; Castelli, W.P.; Margolis, J.R. Electrocardiographic left ventricular hypertrophy and risk of coronary heart disease. The Framingham study. Ann. Intern. Med. 1970, 72, 813–822. [Google Scholar] [CrossRef] [PubMed]
- Pooling Project ResearchGroup. Relationship of blood pressure, serum cholesterol, smoking habit, relative weight and ECG abnormalities to incidence of major coronary events: Final report of the pooling project. J. Chronic Dis. 1978, 31, 201–306. [Google Scholar] [CrossRef]
- Zhang, Z.M.; Prineas, R.J.; Soliman, E.Z.; Baggett, C.; Heiss, G. Prognostic significance of serial Q/ST-T changes by the Minnesota Code and Novacode in the Atherosclerosis Risk in Communities [ARIC] study. Eur. J. Prev. Cardiol. 2012, 19, 1430–1436. [Google Scholar] [CrossRef][Green Version]
- Zhang, Z.; Prineas, R.J.; Eaton, C.B. Evaluation and Comparison of the Minnesota Code and Novacode for Electrocardiographic Q-ST Wave Abnormalities for the Independent Prediction of Incident Coronary Heart Disease and Total Mortality [from the Women’s Health Initiative]. Am. J. Cardiol. 2010, 106, 18–25. [Google Scholar] [CrossRef]
- Machado, D.B.; Crow, R.S.; Boland, L.L.; Hannan, P.J.; Taylor, H.A.; Folsom, A.R. Electrocardiographic Findings and Incident Coronary Heart Disease Among Participants in the Atherosclerosis Risk in Communities [ARIC] Study. Am. J. Cardiol. 2006, 97, 1176–1181. [Google Scholar] [CrossRef]
- Greenland, P.; Xie, X.; Liu, K.; Colangelo, L.; Liao, Y.; Daviglus, M.L.; Agulnek, A.N.; Stamler, J. Impact of minor electrocardiographic ST-segment and/or T-wave abnormalities on cardiovascular mortality during long-term follow-up. Am. J. Cardiol. 2003, 91, 1068–1074. [Google Scholar] [CrossRef]
- Savage, D.D.; Rautaharju, P.M.; Bailey, J.J.; Horton, M.R.; Hadden, W.; Lacroix, A.Z.; Haynes, S.G.; Wolf, H.K.; Prineas, R.J. The emerging prominence of computer electrocardiography in large population-based surveys. J. Electrocardiol. 1987, 20, 48–52. [Google Scholar]
- Ribeiro, A.L.; da Cunha Pereira, S.V.; Bergmann, K.; Ladeira, R.M.; Oliveira, R.A.M.; Lotufo, P.A.; Mill, J.G.; Barreto, S.M. Challenges to implementation of the ECG reading center in ELSA-Brazil. Rev. Saude Publica 2013, 47 (Suppl. 2), 87–94. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Van der Ende, M.Y.; Siland, J.E.; Snieder, H.; Van der Harst, P.; Rienstra, M. Population-based values and abnormalities of the electrocardiogram in the general Dutch population: The LifeLines Cohort Study. Clin. Cardiol. 2017, 40, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Palhares, D.M.F.; Marcolino, M.S.; Santos, T.M.M.; da Silva, J.L.P.; Gomes, P.R.; Ribeiro, L.B.; Macfarlane, P.W.; Ribeiro, A.L.P. Normal limits of the electrocardiogram derived from a large database of Brazilian primary care patients. BMC Cardiovasc. Disord. 2017, 17, 152. [Google Scholar] [CrossRef] [PubMed]
- Goldman, A.; Hod, H.; Chetrit, A.; Dankner, R. Incidental abnormal ECG findings and long-term cardiovascular morbidity and all-cause mortality: A population based prospective study. Int. J. Cardiol. 2019, 295, 36–41. [Google Scholar] [CrossRef]
- Strauss, D.G.; Mewton, N.; Verrier, R.L.; Nearing, B.D.; Marchlinski, F.E.; Killian, T.; Moxley, J.; Tereshchenko, L.G.; Wu, K.C.; Winslow, R.; et al. Screening entire health system ecg databases to identify patients at increased risk of death. Circ. Arrhythmia Electrophysiol. 2013, 6, 1156–1162. [Google Scholar] [CrossRef][Green Version]
- Curry, S.J.; Krist, A.H.; Owens, D.K.; Barry, M.J.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W., Jr.; Kemper, A.R.; Kubik, M.; et al. Screening for cardiovascular disease risk with electrocardiography us preventive services task force recommendation statement. JAMA J. Am. Med. Assoc. 2018, 319, 2308–2314. [Google Scholar] [CrossRef] [PubMed]
- Goff, D.C., Jr.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J.; et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129 (Suppl. 2), 49–73. [Google Scholar] [CrossRef]
- Shah, A.J.; Vaccarino, V.; Janssens, A.C.J.W.; Flanders, W.D.; Kundu, S.; Veledar, E.; Wilson, P.W.F.; Soliman, E.Z. An electrocardiogram-based risk equation for incident cardiovascular disease from the National Health and Nutrition Examination Survey. JAMA Cardiol. 2016, 1, 779–786. [Google Scholar] [CrossRef]
- Ribeiro, A.L.P.; Paixão, G.M.M.; Gomes, P.R.; Ribeiro, M.H.; Ribeiro, A.H.; Canazart, J.A.; Oliveira, D.M.; Ferreira, M.P.; Lima, E.M.; Moraes, J.L.; et al. Tele-electrocardiography and bigdata: The CODE (Clinical Outcomes in Digital Electrocardiography) study. J. Electrocardiol. 2019, 57, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Alkmim, M.B.; Figueira, R.M.; Marcolino, M.S.; Cardoso, C.D.; Abreu, M.P.; Cunha, L.; Cunha, D.F.; Antunes, A.P.; Resende, A.G.A.; Resende, E.S.; et al. Improving patient access to specialized health care: The Telehealth Network of Minas Gerais, Brazil. Bull. World Health Organ. 2012, 90, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Alkmim, M.B.; Silva, C.B.G.; Figueira, R.M.; Santos, D.V.V.; Ribeiro, L.B.; Da Paixão, M.C.; Marcolino, M.S.; Paiva, J.C.; Ribeiro, A.L.P. Brazilian national service of telediagnosis in electrocardiography. Stud. Health Technol. Inform. 2019, 264, 1635–1636. [Google Scholar] [CrossRef] [PubMed]
- Kligfield, P.; Gettes, L.S.; Bailey, J.J.; Childers, R.; Deal, B.J.; Hancock, E.W.; van Herpen, G.; Kors, J.A.; Macfarlane, P.W.; Mirvis, D.M.; et al. Recommendations for the Standardization and Interpretation of the Electrocardiogram. Circulation 2007, 115, 1306–1324. [Google Scholar] [CrossRef]
- Hochreiter, S.; Schmidhuber, J. Long Short-term Memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef]
- Mikolov, T.; Karafiát, M.; Burget, L.; Cernocký, J.; Khudanpur, S. Recurrent neural network based language model. In Proceedings of the 11th Annual Conference of the International Speech Communication Association, Interspeech, Chiba, Japan, 26–30 September 2010; Volume 2, pp. 1045–1048. [Google Scholar]
- Pedrosa, J.A.O.; Oliveira, D.; Meira, W., Jr.; Ribeiro, A. Automated classification of cardiology diagnoses based on textual medical reports. In Proceedings of the Symposium On Knowledge Discovery, Mining And Learning (Kdmile), Porto Alegre, Brazil, 20 October 2020; Volume 8, pp. 185–192. [Google Scholar] [CrossRef]
- Paixão, G.M.M.; Silva, L.G.S.; Gomes, P.R.; Lima, E.M.; Ferreira, M.P.F.; Oliveira, D.M.; Ribeiro, M.H.; Ribeiro, A.H.; Nascimento, J.N.; Canazart, J.A.; et al. Evaluation of Mortality in Atrial Fibrillation: Clinical Outcomes in Digital Electrocardiography [CODE] Study. Glob. Heart 2020, 15, 48. [Google Scholar] [CrossRef]
- Paixão, G.M.M.; Lima, E.M.; Gomes, P.R.; Ferreira, M.P.F.; Oliveira, D.M.; Ribeiro, M.H.; Ribeiro, A.H.; Nascimento, J.N.; Canazart, J.A.; Ribeiro, L.B.; et al. Evaluation of mortality in bundle branch block patients from an electronic cohort: Clinical Outcomes in Digital Electrocardiography [CODE] study. J. Electrocardiol. 2019, 57, 56–60. [Google Scholar] [CrossRef]
- Paixão, G.M.M.; Lima, E.M.; Batista, L.M.; Santos, L.F.; Araujo, S.L.O.; Araujo, R.M.; Oliveira, D.M.; Nascimento, J.N.; Gomes, P.R.; Ribeiro, A.L.P. Ventricular pre-excitation in primary care patients: Evaluation of the risk of mortality. J. Cardiovasc. Electrophysiol. 2021, 32, 1290–1295. [Google Scholar] [CrossRef]
- Faquim, J.P.S.; Guerra, L.D.S.; Carnut, L.; Zilbovicius, C. Atenção Primária à Saúde. J. Manag. Prim. Health Care 2021, 12, 1–7. [Google Scholar] [CrossRef]
- Lin, J.S.; Evans, C.V.; Johnson, E.; Redmond, N.; Coppola, E.L.; Smith, N. Nontraditional risk factors in cardiovascular disease risk assessment: Updated evidence report and systematic review for the US preventive services task force. JAMA J. Am. Med. Assoc. 2018, 320, 281–297. [Google Scholar] [CrossRef]
- Chen, M.; Mao, S.; Liu, Y. Big data: A survey. Mob. Netw. Appl. 2014, 19, 171–209. [Google Scholar] [CrossRef]
- Ferreira, J.P.; Rossignol, P.; Dewan, P.; Lamiral, Z.; White, W.B.; Pitt, B.; Mc Murray, J.J.V.; Zannad, F. Income level and inequality as complement to geographical differences in cardiovascular trials. Am. Heart J. 2019, 218, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Marcolino, M.S.; Palhares, D.M.; Ferreira, L.R.; Ribeiro, A.L. Electrocardiogram and Chagas Disease A Large Population Database of Primary Care Patients. Glob. Heart 2015, 10, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.H.; Ribeiro, M.H.; Paixão, G.M.M.; Oliveira, D.M.; Gomes, P.R.; Canazart, J.A.; Ferreira, M.P.S.; Andersson, C.R.; Macfarlane, P.W.; Meira, W., Jr. Automatic diagnosis of the 12-lead ECG using a deep neural network. Nat. Commun. 2020, 11, 1760. [Google Scholar] [CrossRef] [PubMed]
- Attia, Z.I.; Noseworthy, P.A.; Lopez-Jimenez, F.; Asirvatham, S.J.; Deshmukh, A.J.; Gersh, B.J.; Carter, R.E.; Yao, X.; Rabinstein, A.A.; Erickson, B.J.; et al. An artificial intelligence-enabled ECG algorithm for the identification of patients with atrial fibrillation during sinus rhythm: A retrospective analysis of outcome prediction. Lancet 2019, 394, 861–867. [Google Scholar] [CrossRef]
- Attia, Z.I.; Friedman, P.A.; Noseworthy, P.A.; Lopez-Jimenez, F.; Ladewig, D.J.; Satam, G.; Pellikka, P.A.; Munger, T.M.; Asirvatham, S.J.; Scott, C.G.; et al. Age and Sex Estimation Using Artificial Intelligence From Standard 12-Lead ECGs. Circ. Arrhythm Electrophysiol. 2019, 12, e007284. [Google Scholar] [CrossRef]
- Raghunath, S.; Ulloa Cerna, A.E.; Jing, L.; Van Maanen, D.P.; Stough, J.; Hartzel, D.N.; Nemani, A.; Carbonati, T.; Johnson, K.W.; Young, K.; et al. Prediction of mortality from 12-lead electrocardiogram voltage data using a deep neural network. Nat. Med. 2020, 26, 886–891. [Google Scholar] [CrossRef]
- Lima, E.M.; Ribeiro, A.H.; Paixão, G.M.M.; Ribeiro, M.H.; Pinto-Filho, M.M.; Gomes, P.R.; Oliveira, D.M.; Sabino, E.C.; Duncan, B.B.; Giatti, L.; et al. Deep neural network-estimated electrocardiographic age as a mortality predictor. Nat. Commun. 2021, 12, 5117. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| N | % | |
|---|---|---|
| Comorbidities | ||
| Hypertension | 492,637 | 31.611 |
| Diabetes | 101,470 | 6.511 |
| Current smoking | 108,814 | 6.982 |
| Dyslipidemia | 60,590 | 3.888 |
| Chagas disease | 34,590 | 2.220 |
| Myocardial infarction | 11,604 | 0.745 |
| COPD | 11,266 | 0.723 |
| ECG abnormalities | ||
| Atrial fibrillation | 20,782 | 1.334 |
| Left bundle branch block | 20,226 | 1.298 |
| Right bundle branch block | 37,031 | 2.376 |
| Ventricular pre-excitation * | 1090 | 0.065 |
| First degree AVB | 20,644 | 1.325 |
| Second degree AVB Mobitz I | 212 | 0.014 |
| Second degree AVB 2:1 | 61 | 0.004 |
| Third degree AVB | 621 | 0.040 |
| ECG Abnormalities | Survival Analysis Estimate | Overall Mortality 95% CI | p-Value | Cardiovascular Mortality [HR; 95% CI] | p-Value |
|---|---|---|---|---|---|
| Atrial fibrillation | HR | 2.10 [2.03–2.17] | <0.001 | 2.06 [1.86–2.29] | <0.001 |
| Left bundle branch block | HR | 1.69 [1.62–1.76] | <0.001 | 1.76 [1.55–2.01] | <0.001 |
| Right bundle branch block | HR | 1.32 [1.27–1.36] | <0.001 | 1.12 [0.99–1.28] | 0.06 |
| Ventricular pre-excitation | HR | 1.41 [0.56–3.57] | 0.470 | NA | |
| First degree AVB | RS | 0.76 [0.71–0.81] | <0.001 | NA | |
| Second degree AVB Mobitz I | RS | 0.65 [0.34–1.24] | 0.269 | NA | |
| Second degree AVB 2:1 | RS | 0.21 [0.09–0.52] | 0.005 | NA | |
| Third degree AVB | RS | 0.36 [0.26–0.49] | <0.001 | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paixão, G.M.M.; Lima, E.M.; Gomes, P.R.; Oliveira, D.M.; Ribeiro, M.H.; Nascimento, J.S.; Ribeiro, A.H.; Macfarlane, P.W.; Ribeiro, A.L.P. Electrocardiographic Predictors of Mortality: Data from a Primary Care Tele-Electrocardiography Cohort of Brazilian Patients. Hearts 2021, 2, 449-458. https://doi.org/10.3390/hearts2040035
Paixão GMM, Lima EM, Gomes PR, Oliveira DM, Ribeiro MH, Nascimento JS, Ribeiro AH, Macfarlane PW, Ribeiro ALP. Electrocardiographic Predictors of Mortality: Data from a Primary Care Tele-Electrocardiography Cohort of Brazilian Patients. Hearts. 2021; 2(4):449-458. https://doi.org/10.3390/hearts2040035
Chicago/Turabian StylePaixão, Gabriela M. M., Emilly M. Lima, Paulo R. Gomes, Derick M. Oliveira, Manoel H. Ribeiro, Jamil S. Nascimento, Antonio H. Ribeiro, Peter W. Macfarlane, and Antonio L. P. Ribeiro. 2021. "Electrocardiographic Predictors of Mortality: Data from a Primary Care Tele-Electrocardiography Cohort of Brazilian Patients" Hearts 2, no. 4: 449-458. https://doi.org/10.3390/hearts2040035
APA StylePaixão, G. M. M., Lima, E. M., Gomes, P. R., Oliveira, D. M., Ribeiro, M. H., Nascimento, J. S., Ribeiro, A. H., Macfarlane, P. W., & Ribeiro, A. L. P. (2021). Electrocardiographic Predictors of Mortality: Data from a Primary Care Tele-Electrocardiography Cohort of Brazilian Patients. Hearts, 2(4), 449-458. https://doi.org/10.3390/hearts2040035