
Factors Affecting Quality of Life in Liver Transplant Candidates: An Observational Study

 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
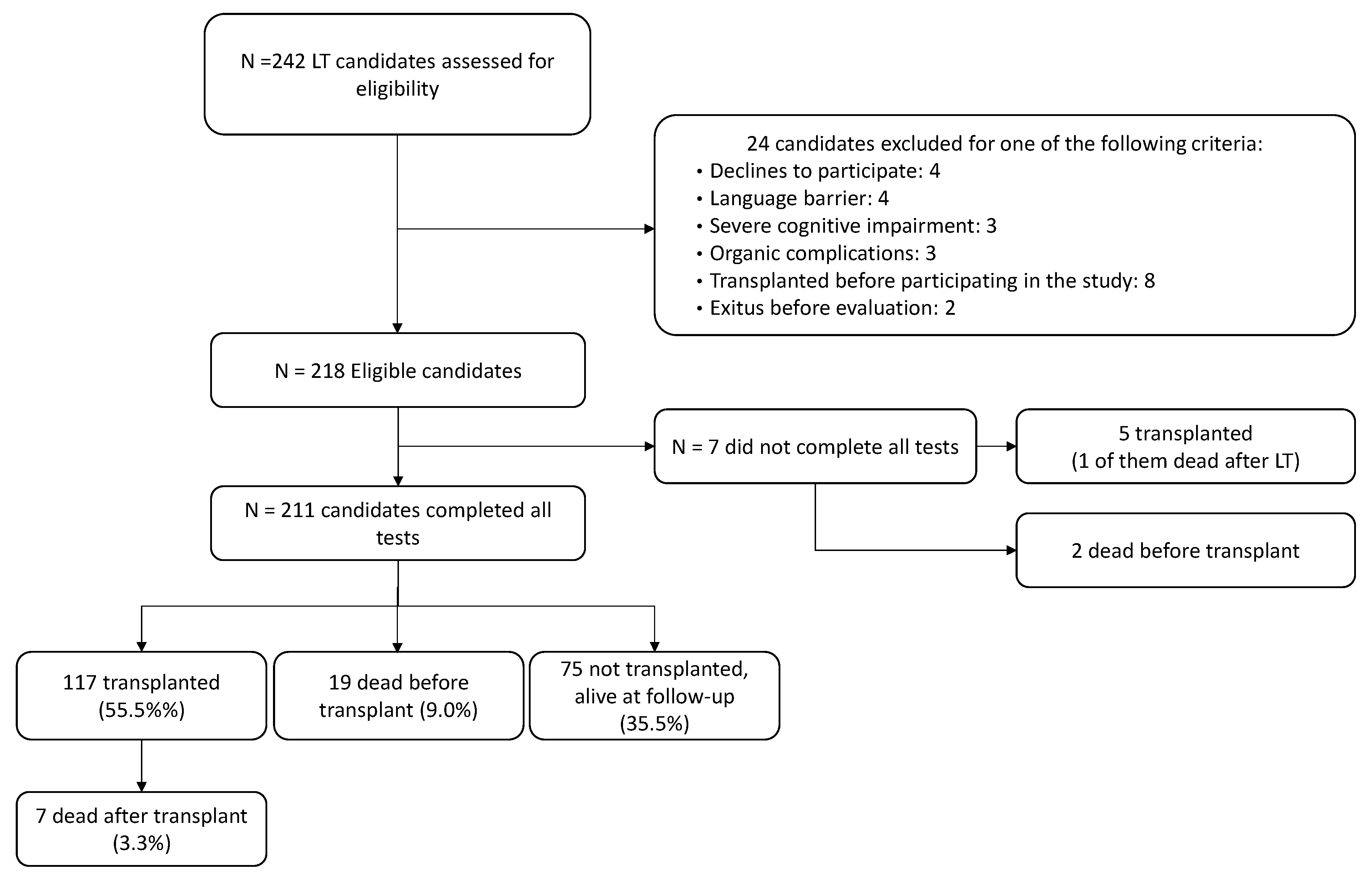
2.2. Participants
2.3. Baseline Sociodemographic and Clinical Variables
2.4. Ethical Considerations
2.5. Statistical Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maldonado, J.R.; Sher, Y.; Lolak, S.; Swendsen, H.; Skibola, D.; Neri, E.; David, E.E.; Sullivan, C.; Standridge, K. The Stanford Integrated Psychosocial Assessment for Transplantation: A Prospective Study of Medical and Psychosocial Outcomes. Psychosom. Med. 2015, 77, 1018–1030. [Google Scholar] [CrossRef]
- Lopez-Lazcano, A.I.; López-Pelayo, H.; Lligoña, A.; Sánchez, N.; Vilas-Riotorto, V.; Priego, A.; Sánchez-González, R.; Rodríguez-Urrutia, A.; Quesada-Franco, M.; Maldonado, J.R.; et al. Translation, adaptation, and reliability of the Stanford Integrated Psychosocial Assessment for Transplantation in the Spanish population. Clin. Transplant. 2019, 33, e13688. [Google Scholar] [CrossRef]
- WHO; ONT. Organ Donation and Transplantation Activities 2017: Global Observatory on Donation and Transplantation (GODT); Godt: Madrid, Spain, 2017. [Google Scholar]
- Onghena, L.; Develtere, W.; Poppe, C.; Geerts, A.; Troisi, R.; Vanlander, A.; Berrevoet, F.; Rogiers, X.; Van Vlierberghe, H.; Verhelst, X. Quality of life after liver transplantation: State of the art. World J. Hepatol. 2016, 8, 749–756. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Measuring Healthy Days: Population Assessment of Health-Related Quality of Life; Centers for Disease Control and Prevention: Atlanta, Georgia, 2000. [Google Scholar]
- Gutteling, J.J.; De Man, R.A.; Busschbach, J.J.V.; Darlington, A.-S.E. Overview of research on health-related quality of life in patients with chronic liver disease. Neth. J. Med. 2007, 65, 227–234. [Google Scholar]
- Younossi, Z.M.; Boparai, N.; Price, L.L.; Kiwi, M.L.; McCormick, M.; Guyatt, G. Health-related quality of life in chronic liver disease: The impact of type and severity of disease. Am. J. Gastroenterol. 2001, 96, 2199–2205. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.-K.; Hepgul, N.; Higginson, I.J.; Gao, W. Symptom prevalence and quality of life of patients with end-stage liver disease: A systematic review and meta-analysis. Palliat. Med. 2019, 33, 24–36. [Google Scholar] [CrossRef] [Green Version]
- Marchesini, G.; Bianchi, G.; Amodio, P.; Salerno, F.; Merli, M.; Panella, C.; Loguercio, C.; Apolone, G.; Niero, M.; Abbiati, R. Factors associated with poor health-related quality of life of patients with cirrhosis. Gastroenterology 2001, 120, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Stine, J.G.; Stukenborg, G.J.; Wang, J.; Adkins, A.; Niccum, B.; Zimmet, A.; Argo, C.K. Liver transplant candidates have impaired quality of life across health domains as assessed by computerized testing. Ann. Hepatol. 2020, 19, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Saab, S.; Ibrahim, A.B.; Shpaner, A.; Younossi, Z.M.; Lee, C.; Durazo, F.; Han, S.; Esrason, K.; Wu, V.; Hiatt, J.; et al. MELD fails to measure quality of life in liver transplant candidates. Liver Transplant. 2005, 11, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Benzing, C.; Krezdorn, N.; Förster, J.; Hinz, A.; Krenzien, F.; Atanasov, G.; Schmelzle, M.; Hau, H.-M.; Bartels, M. Health-related quality of life and affective status in liver transplant recipients and patients on the waiting list with low MELD scores. HPB 2016, 18, 449–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavaggioni, G.; Poli, E.; Ferri, F.; Parlati, L.; Monaco, V.; Melcore, C.; Lattanzi, B.; Merli, M.; Mennini, G.; Melandro, F.; et al. MELDNa score is associated with psychopathology and reduced quality of life in cirrhotic patients with a liver transplant perspective. Metab. Brain Dis. 2017, 32, 923–933. [Google Scholar] [CrossRef] [PubMed]
- Togashi, J.; Sugawara, Y.; Akamatsu, N.; Tamura, S.; Yamashiki, N.; Kaneko, J.; Sakamoto, Y.; Aoki, T.; Hasegawa, K.; Kokudo, N. Quality of life after adult living donor liver transplantation: A longitudinal prospective follow-up study. Hepatol. Res. 2013, 43, 1052–1063. [Google Scholar] [CrossRef] [PubMed]
- Estraviz, B.; Quintana, J.M.; Valdivieso, A.; Bilbao, A.; Padierna, A.; De Urbina, J.O.; Sarabia, S. Factors influencing change in health-related quality of life after liver transplantation. Clin. Transplant. 2007, 21, 481–499. [Google Scholar] [CrossRef] [PubMed]
- Afendy, A.; Kallman, J.B.; Stepanova, M.; Younoszai, Z.; Aquino, R.D.; Bianchi, G.; Marchesini, G.; Younossi, Z.M. Predictors of health-related quality of life in patients with chronic liver disease. Aliment. Pharmacol. Ther. 2009, 30, 469–476. [Google Scholar] [CrossRef]
- Labidi, A.; Hidri, S.; Hafi, M.; Serghini, M.; Zouiten, L.; Boubaker, J. Health-related quality of life in cirrhotic patients: A case-control study. Tunis. Med. 2019, 97, 990–996. [Google Scholar]
- Cowling, T.; Jennings, L.W.; Goldstein, R.M.; Sanchez, E.Q.; Chinnakotla, S.; Klintmalm, G.B.; Levy, M.F. Liver transplantation and health-related quality of life: Scoring differences between men and women. Liver Transplant. 2004, 10, 88–96. [Google Scholar] [CrossRef]
- Santos, G.; Gonçalves, L.; Buzzo, N.; Mendes, T.; Dias, T.; Da Silva, R.; Da Silva, R.; De Felicio, H.; Júnior, R.S.; Miyazaki, M. Quality of Life, Depression, and Psychosocial Characteristics of Patients Awaiting Liver Transplants. Transplant. Proc. 2012, 44, 2413–2415. [Google Scholar] [CrossRef] [PubMed]
- Saracino, R.M.; Jutagir, D.R.; Cunningham, A.; Foran-Tuller, K.A.; Driscoll, M.A.; Sledge, W.H.; Emre, S.H.; Fehon, D.C. Psychiatric Comorbidity, Health-Related Quality of Life, and Mental Health Service Utilization Among Patients Awaiting Liver Transplant. J. Pain Symptom Manag. 2018, 56, 44–52. [Google Scholar] [CrossRef] [Green Version]
- Golfieri, L.; Gitto, S.; Vukotic, R.; Andreone, P.; Marra, F.; Morelli, M.C.; Cescon, M.; Grandi, S. Impact of psychosocial status on liver transplant process. Ann. Hepatol. 2019, 18, 804–809. [Google Scholar] [CrossRef]
- Dew, M.A.; Rosenberger, E.M.; Myaskovsky, L.; DiMartini, A.F.; Dabbs, A.J.D.; Posluszny, D.M.; Steel, J.; Switzer, G.E.; Shellmer, D.A.; Greenhouse, J.B. Depression and anxiety as risk factors for morbidity and mortality after organ transplantation: A systematic review and meta-analysis. Transplantation 2016, 100, 988–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fineberg, S.K.; West, A.; Na, P.J.; Oldham, M.; Schilsky, M.; Hawkins, K.A.; Lee, H.B.; Na, M.P.J. Utility of pretransplant psychological measures to predict posttransplant outcomes in liver transplant patients: A systematic review. Gen. Hosp. Psychiatry 2016, 40, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Eftekar, M.; Pun, P. Psychiatric risk factors predicting post-liver transplant physical and psychiatric complications: A literature review. Australas. Psychiatry 2016, 24, 385–392. [Google Scholar] [CrossRef]
- Addolorato, G.; Bataller, R.; Burra, P.; DiMartini, A.; Graziadei, I.; Lucey, M.R.; Mathurin, P.; O’Grady, J.; Pageaux, G.; Berenguer, M. Liver Transplantation for Alcoholic Liver Disease. Transplantation 2016, 100, 981–987. [Google Scholar] [CrossRef]
- Colmenero, J.; Castro-Narro, G.; Navasa, M. Utilidad del MELD (Model for End-stage Liver Disease) para asignar prioridades en el trasplante hepático. Gastroenterol. Hepatol. 2010, 33, 330–336. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.; Prieto, L.; Antó, J.M. The Spanish version of the SF-36 Health Survey (the SF-36 health questionnaire): An instrument for measuring clinical results. Med. Clin. 1995, 104, 771–776. [Google Scholar]
- Vilagut, G.; Ferrer, M.; Rajmil, L.; Rebollo, P.; Permanyer-Miralda, G.; Quintana, J.M.; Santed, R.; Valderas, J.M.; Ribera, A.; Domingo-Salvany, A.; et al. The Spanish version of the Short Form 36 Health Survey: A decade of experience and new developments. Gac. Sanit. 2005, 19, 135–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrero, M.J.; Blanch, J.; Peri, J.M.; De Pablo, J.; Pintor, L.; Bulbena, A. A validation study of the hospital anxiety and depression scale (HADS) in a Spanish population. Gen. Hosp. Psychiatry 2003, 25, 277–283. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Teegen, E.M.; Krebs, I.; Langelotz, C.; Pratschke, J.; Rau, B. Gender Mainstreaming and Transplant Surgery. Visc. Med. 2016, 32, 286–289. [Google Scholar] [CrossRef] [Green Version]
- Gove, W.R. Gender differences in mental and physical illness: The effects of fixed roles and nurturant roles. Soc. Sci. Med. 1984, 19, 77–84. [Google Scholar] [CrossRef]
- Agrawal, S.; Umapathy, S.; Dhiman, R.K. Minimal Hepatic Encephalopathy Impairs Quality of Life. J. Clin. Exp. Hepatol. 2015, 5, S42–S48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montagnese, S.; Bajaj, J.S. Impact of Hepatic Encephalopathy in Cirrhosis on Quality-of-Life Issues. Drugs 2019, 79, 11–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, C.F.; Amodio, P.; Bajaj, J.S.; Dhiman, R.K.; Montagnese, S.; Taylor-Robinson, S.D.; Vilstrup, H.; Jalan, R. Hepatic encephalopathy: Novel insights into classification, pathophysiology and therapy. J. Hepatol. 2020, 73, 1526–1547. [Google Scholar] [CrossRef]
- Patel, A.V.; Wade, J.B.; Thacker, L.R.; Sterling, R.K.; Siddiqui, M.S.; Stravitz, R.T.; Sanyal, A.J.; Luketic, V.; Puri, P.; Fuchs, M.; et al. Cognitive reserve is a determinant of health-related quality of life in patients with cirrhosis, independent of covert hepatic encephalopathy and model for end-stage liver disease score. Clin. Gastroenterol. Hepatol. 2015, 13, 987–991. [Google Scholar] [CrossRef] [Green Version]
- Morana, J.-G. Psychological evaluation and follow-up in liver transplantation. World J. Gastroenterol. 2009, 15, 694–696. [Google Scholar] [CrossRef] [Green Version]
- Randolph, C.; Hilsabeck, R.; Kato, A.; Kharbanda, P.; Yu-Yuan International Society for Hepatic Encephalopathy and Nitrogen Metabolism (ISHEN); Mapelli, D.; Ravdin, L.D.; Romero-Gomez, M.; Stracciari, A.; Weissenborn, A.S.A.K. Neuropsychological assessment of hepatic encephalopathy: ISHEN practice guidelines. Liver Int. 2009, 29, 629–635. [Google Scholar] [CrossRef]
- Labenz, C.; Toenges, G.; Schattenberg, J.M.; Nagel, M.; Huber, Y.; Marquardt, J.U.; Galle, P.R.; Wörns, M.-A. Health-related quality of life in patients with compensated and decompensated liver cirrhosis. Eur. J. Intern. Med. 2019, 70, 54–59. [Google Scholar] [CrossRef]
- Montoro-Gurich, C.; Garcia-Vivar, C. The Family in Europe: Structure, Intergenerational Solidarity, and New Challenges to Family Health. J. Fam. Nurs. 2019, 25, 170–189. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| N (%) | Physical Functioning | Role Physical | Bodily Pain | General Health | Vitality | Social Functioning | Role Emotional | Mental Health | |
|---|---|---|---|---|---|---|---|---|---|
| Totals (Median, RIQ) | 211 | 60 (30–85) | 25 (0–100) | 70 (45–100) | 40 (30–50) | 50 (30–70) | 80 (55–100) | 100 (66.7–100) | 80 (60–92) |
| Age | |||||||||
| ≤60 | 115 (54.5%) | 65 (32.5–90) | 25 (0–100) | 70 (45–100) | 40 (30–50) | 50 (27.5–70) | 80 (51.3–100) | 100 (66.7–100) | 80 (60–90) |
| >60 | 96 (45.5%) | 55 (30–81.3) | 37.5 (0–100) | 72.5 (45–100) | 35 (25–50) | 50 (30–75) | 80 (55–100) | 100 (100–100) | 82 (60–92) |
| Gender | |||||||||
| Female | 54 (25.6%) | 45 (17.5–75) | 0 (0–75) | 57.5 (32.5–79.4) | 35 (21.3–48.8) | 47.5 (30–63.8) | 67.5 (35.6–100) | 100 (0–100) | 74 (56–87) |
| Male | 157 (74.4%) | 65 (35–90) † | 50 (0–100) † | 77.5 (45–100) † | 40 (30–50) | 50 (30–80) | 87.5 (60–100) * | 100 (100–100) ‡ | 84 (64–92) * |
| Cirrhosis etiology | |||||||||
| Alcohol-related liver disease | 138 (65.4%) | 55 (25–85) | 50 (0–100) | 77.5 (45–100) | 40 (30–50) | 50 (30–73.75) | 80 (55–100) | 100 (100–100) | 80 (64–95) |
| Others | 73 (34.6%) | 65 (35–85) | 25 (0–100) | 67.5 (35–90) | 40 (30–50) | 50 (25–65) | 77.5 (42.5–100) | 100 (66.7–100) | 76 (56–88) |
| Primary diagnosis for tx | |||||||||
| Hepatocellular carcinoma | 47 (22.3%) | 85 (57.5–95) ‡ | 100 (37.5–100) ‡ | 90 (67.5–100) ‡ | 50 (40–65) ‡ | 65 (50–80) ‡ | 100 (80–100)‡ | 100 (100–100) ‡ | 88 (80–96) ‡ |
| Others | 164 (77.7%) | 50 (25–81.3) | 25 (0–100) | 67.5 (40.6–90) | 35 (25–45) | 45 (20–65) | 76.3 (41.3–100) | 100 (66.7–100) | 74 (52–88) |
| Level of education | |||||||||
| Primary education or less | 41 (19.4%) | 50 (35–80) | 0 (0–75) | 67.5 (32.5–90) | 40 (30–50) | 50 (20–60) | 77.5 (47.5–100) | 100 (66.7–100) | 72 (52–92) |
| Secondary education | 57 (27.0%) | 60 (25–90) | 25 (0–100) | 77.5 (47.5–100) | 35 (25–50) | 50 (20–80) | 77.5 (65–100) | 100 (66.7–100) | 80 (60–92) |
| High school diploma | 82 (38.9%) | 65 (31.3–85) | 50 (0–100) | 77.5 (45–100) | 40 (26.3–55) | 50 (31.3–73.8) | 87.5 (51.3–100) | 100 (100–100) | 82 (64–92) |
| University or beyond | 31 (14.7%) | 65 (40–85) | 50 (0–75) | 67.5 (40–80) | 35 (30–45) | 45 (27.5–65) | 80 (51.3–100) | 100 (83.3–100) | 76 (64–92) |
| Civil status | |||||||||
| Single | 10 (4.7%) | 72.5 (37.5–93.8) | 0 (0–87.5) | 85 (31.3–100) | 40 (23.8–76.3) | 50 (33.8–68.8) | 82.5 (33.1–100) | 100 (75–100) | 84 (71–97) |
| Married | 149 (70.6%) | 60 (35–85) | 25 (0–100) | 70 (45–100) | 40 (30–50) | 50 (30–70) | 80 (55–100) | 100 (100–100) | 80 (60–92) |
| Divorced | 43 (20.4%) | 55 (25–72.5) | 50 (0–100) | 67.5 (45–100) | 35 (20–52.5) | 50 (27.5–65) | 77.5 (35–100) | 100 (33.3–100) | 80 (54–92) |
| Widowed | 9 (4.3%) | 75 (30–85) | 50 (0–100) | 67.5 (45–87.5) | 25 (15–45) | 55 (25–70) | 90 (80–100) | 100 (66.7–100) | 84 (60–100) |
| Encephalopathy | |||||||||
| No | 97 (46.0%) | 75 (50–95) | 50 (0–100) | 77.5 (45–100) | 45 (35–60) | 55 (40–80) | 90 (67.5–100) | 100 (100–100) | 84 (64–92) |
| Yes | 114 (54.0%) | 45 (25–75) ‡ | 25 (0–93.8) | 67.5 (43.1–97.5) | 35 (21.3–45) ‡ | 45 (20–60) ‡ | 76.3 (35.6–100) † | 100 (66.7–100) | 76 (56–92) * |
| MELD | |||||||||
| <19 | 136 (64.5%) | 75 (40–90) | 50 (0–100) | 77.5 (47.0–90) | 40 (30–55) | 55 (35–80) | 90 (67.5–100) | 100 (100–100) | 84 (68–93) |
| ≥19 | 75 (35.5%) | 45 (20–65) † | 0 (0–87.5) † | 67.5 (32.5–100) | 35 (25–45) | 40 (17.5–55) ‡ | 65 (30–90) ‡ | 100 (50–100) * | 68 (48–88) ‡ |
| HADS-Anxiety | |||||||||
| <8 | 173 (82.0%) | 70 (45–90) | 50 (0–100) | 77.5 (55–100) | 40 (30–55) | 55 (35–80) | 90 (67.5–100) | 100 (100–100) | 84 (68–96) |
| ≥8 | 38 (18.0%) | 25 (15–38.8) ‡ | 0 (0–25) ‡ | 43.8 (20.6–61.3) ‡ | 30 (15–35) ‡ | 25 (15–40) ‡ | 42.5 (15–66.9) ‡ | 50 (0–100) ‡ | 44 (37–62) ‡ |
| HADS-Depression | |||||||||
| <8 | 174 (82.5%) | 70 (45–90) | 50 (0–100) | 77.5 (55–100) | 40 (30–53.8) | 55 (40–80) | 90 (65.6–100) | 100 (100–100) | 84 (68–95) |
| ≥8 | 37 (17.5%) | 25 (15–40) ‡ | 0 (0–0) ‡ | 45 (10–62.5) ‡ | 25 (15–30) ‡ | 20 (5–30) ‡ | 35 (12.5–67.5) ‡ | 33.33 (0–100) ‡ | 44 (36–56) ‡ |
| Status | |||||||||
| Alive before LT | 192 (91.0%) | 65 (33.8–85) | 37.5 (0–100) | 68.8 (45–100) | 40 (28.8–50) | 50 (30–70) | 83.8 (55–100) | 100 (100–100) | 80 (60–92) |
| Death before LT | 19 (9.0%) | 35 (17.5–46.5) † | 25 (0–50) | 77.5 (38.8–100) | 35 (30–55) | 45 (20–57.5) | 60 (22.5–80) † | 100 (66.7–100) | 68 (48–86) |
| Physical Functioning | Role Physical | Bodily Pain | General Health | Vitality | Social Functioning | Role Emotional | Mental Health | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| R-squared, p | 0.458 | 0.00 * | 0.293 | 0.00 * | 0.268 | 0.00 * | 0.264 | 0.00 * | 0.398 | 0.00 * | 0.467 | 0.00 * | 0.318 | 0.00 * | 0.614 | 0.00 * |
| Constant | 94.45 | 48.46 | 77.51 | 37.0 | 61.15 | 99.1 | 82.86 | 88.8 | ||||||||
| B | p | B | p | B | p | B | p | B | p | B | p | B | p | B | p | |
| Age | −0.39 | 0.09 | 0.32 | 0.41 | 0.00 | 0.99 | 0.16 | 0.36 | 0.19 | 0.40 | −0.03 | 0.89 | 0.00 | 0.99 | 0.11 | 0.43 |
| Gender | 14.56 | 0.00 * | 13.66 | 0.04 * | 9.00 | 0.05 | 3.56 | 0.24 | 3.21 | 0.39 | 7.99 | 0.04 * | 18.09 | 0.00 * | 2.27 | 0.34 |
| Cirrhosis etiology | 5.81 | 0.13 | −1.01 | 0.87 | 0.51 | 0.91 | 0.31 | 0.91 | −2.33 | 0.52 | −0.59 | 0.88 | −0.33 | 0.95 | −3.65 | 0.12 |
| Level of education | ||||||||||||||||
| Primary education | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Secondary education | 5.29 | 0.28 | 3.78 | 0.64 | 0.83 | 0.88 | 2.6 | 0.48 | 3.09 | 0.50 | 2.75 | 0.58 | 5.25 | 0.42 | 2.67 | 0.36 |
| High school diploma | 3.79 | 0.36 | 14.86 | 0.03 * | 0.45 | 0.93 | 3.49 | 0.26 | 3.48 | 0.37 | −0.19 | 0.96 | 2.13 | 0.70 | 2.5 | 0.31 |
| University or beyond | 4.35 | 0.42 | 9.63 | 0.28 | −5.95 | 0.35 | −0.71 | 0.86 | 1.16 | 0.82 | 1.17 | 0.83 | 3.44 | 0.64 | 3.58 | 0.27 |
| Civil status | ||||||||||||||||
| Single | 8.60 | 0.31 | −12.42 | 0.37 | −0.01 | 1.00 | 11.73 | 0.07 | 2.57 | 0.75 | −3.02 | 0.72 | −0.37 | 0.97 | 2.31 | 0.65 |
| Married | 6.37 | 0.13 | −5.73 | 0.40 | −0.79 | 0.87 | 3.04 | 0.33 | −1.55 | 0.69 | 7.48 | 0.08 | 6.67 | 0.23 | 0.39 | 0.88 |
| Widowed | 14.05 | 0.11 | 6.16 | 0.67 | −1.3 | 0.90 | −9.45 | 0.15 | −1.88 | 0.82 | 13.83 | 0.12 | 5.6 | 0.63 | 2.75 | 0.60 |
| Divorced | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Encephalopathy | −9.16 | 0.01 * | −0.03 | 1.00 | −1.25 | 0.76 | −9.45 | 0.00 * | −6.69 | 0.04 * | −3.04 | 0.39 | 0.36 | 0.94 | 0.19 | 0.93 |
| MELD | −1.04 | 0.00 * | −1.00 | 0.02 * | −0.01 | 0.98 | −0.08 | 0.69 | −0.41 | 0.11 | −1.14 | 0.00 * | −0.16 | 0.65 | −0.33 | 0.04 * |
| HADS-Anxiety | −0.48 | 0.45 | −1.59 | 0.13 | −1.93 | 0.01 * | −0.66 | 0.17 | −0.99 | 0.10 | −1.12 | 0.08 | −3.04 | 0.00 * | −2.65 | 0.00 * |
| HADS-Depression | −3.12 | 0.00 * | −3.26 | 0.00 * | −1.99 | 0.00 * | −1.02 | 0.02 * | −2.80 | 0.00 * | −3.27 | 0.00 * | −1.82 | 0.02 * | −1.70 | 0.00 * |
| Gender | High School Diploma | Encephalopathy | MELD | HADS-Anxiety | HADS-Depression | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | 95% CI | B | 95% CI | B | 95% CI | B | 95% CI | B | 95% CI | B | 95% CI | |
| Physical Functioning | 14.56 | 6.75–22.34 | −9.16 | −15.96–−2.36 | −1.04 | −1.57–−0.52 | −3.12 | −4.3–−1.95 | ||||
| Role Physical | 13.66 | 0.80–26.51 | 14.86 | 1.59–28.13 | −1.00 | −1.87–−0.14 | −3.26 | −5.19–−1.33 | ||||
| Bodily Pain | −1.93 | −3.39–−0.47 | −1.99 | −3.37–−0.62 | ||||||||
| General Health | −9.45 | −14.59–−4.31 | −1.02 | −1.90–−0.13 | ||||||||
| Vitality | −6.69 | −13.13–−0.25 | −2.80 | −3.92–−1.69 | ||||||||
| Social Functioning | 7.99 | 0.07–15.92 | −1.14 | −1.67–−0.61 | −3.27 | −4.46–−2.08 | ||||||
| Role Emotional | 18.09 | 7.56–28.62 | −3.04 | −4.71–−1.36 | −1.82 | −3.4–−0.24 | ||||||
| Mental Health | −0.33 | −0.65–−0.12 | −2.65 | −3.39–−1.90 | −1.70 | −2.41–−0.99 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Lazcano, A.I.; López-Pelayo, H.; Gual, A.; Lligoña, A.; Vilas-Riotorto, V.; Caballeria, E.; Bruguera, P.; Pintor, L. Factors Affecting Quality of Life in Liver Transplant Candidates: An Observational Study. Transplantology 2021, 2, 64-74. https://doi.org/10.3390/transplantology2010007
López-Lazcano AI, López-Pelayo H, Gual A, Lligoña A, Vilas-Riotorto V, Caballeria E, Bruguera P, Pintor L. Factors Affecting Quality of Life in Liver Transplant Candidates: An Observational Study. Transplantology. 2021; 2(1):64-74. https://doi.org/10.3390/transplantology2010007
Chicago/Turabian StyleLópez-Lazcano, Ana Isabel, Hugo López-Pelayo, Antoni Gual, Anna Lligoña, Vanessa Vilas-Riotorto, Elsa Caballeria, Pol Bruguera, and Luis Pintor. 2021. "Factors Affecting Quality of Life in Liver Transplant Candidates: An Observational Study" Transplantology 2, no. 1: 64-74. https://doi.org/10.3390/transplantology2010007