
“You Can’t Manage What You Can’t Measure”: Perspectives of Transplant Recipients on Two Lifestyle Interventions for Weight Management

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Design
2.2. Participant Recruitment and Selection
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Participants
3.2. Themes and Sub-Themes
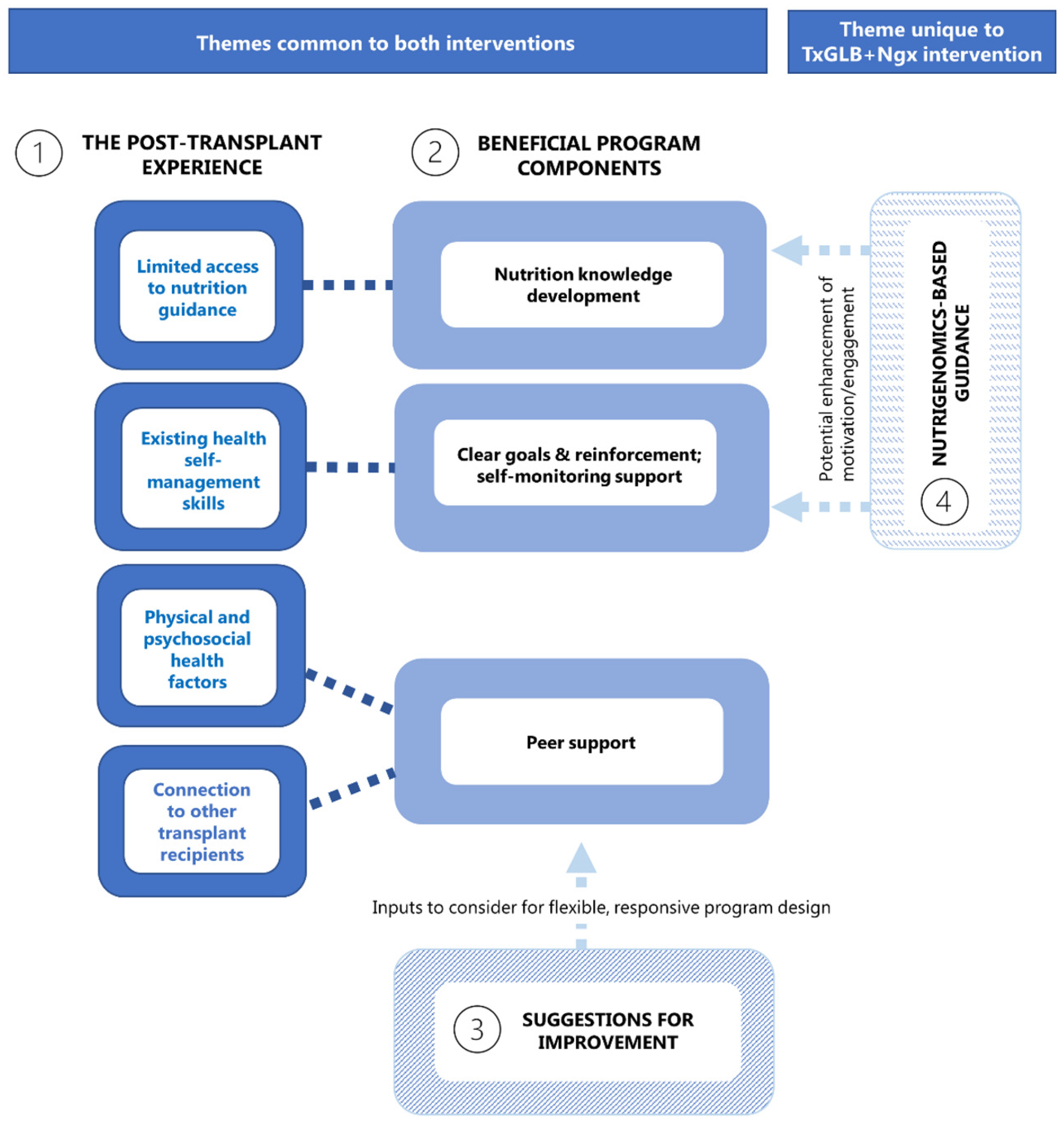
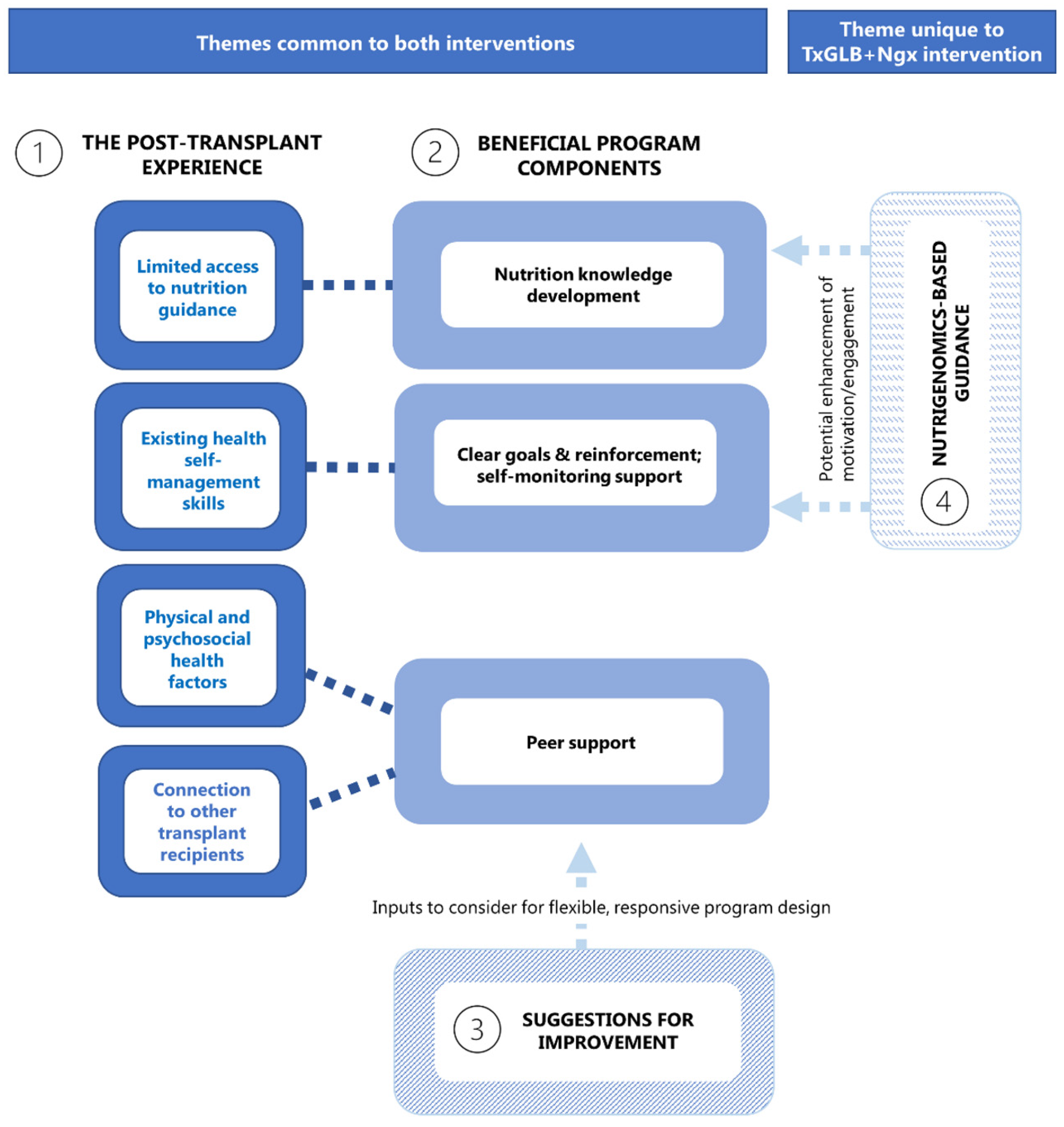
3.2.1. Themes in Both Intervention Groups
Theme 1—The Post-Transplant Experience
The day after the surgery, I was told I can eat and drink anything I wanted. Not as much as I wanted, but anything I wanted, so I went from an extremely restrictive to completely non-restrictive [diet], with no conversations with any dietitians or nutritionists afterwards. It was never felt a need for that.(FG, P12)
And then [after] transplanting, ok what now? They say, “Eat a square meal”, well—what does that really mean?(FG, P1)
I was underweight at the time and, you know, got told “Well, you can gain weight” and then I just had a heyday because “Yeah, woohoo, first time in my life I can gain weight.” And I took it to heart and I–boy, did I gain weight.(FG, P1)
I was given a food calendar and that was about it. And I had wanted more.(FG, P11)
I wish I had been followed more closely so that someone could give me help on what to eat so that I could gain weight—but healthy.(FG, P1)
Post-transplant, it took a long time for me to recover because I had a lot of additional issues—yeah, it took a long time to get used to that. So I’m at 4 ½, 5 years post-transplant. It was, ok, this is where I’m at, I’ve got a good handle on what I can and can’t do, and so now I’m kind of back into working on the other stuff.(INT, P18)
Post-transplant, first recommendations are, you know, load up on protein, ‘cause you have to heal. And you’re like, “but wait a sec, I am conditioned not to do that”.(FG, P10)
Well, before your transplant you’re pretty much down to nothing, you know, as far as your health and your strength. And then, you know, you’re building yourself back after your transplant, so it was—I think I built too far. So then it was like, ok now I need to get balanced.(FG, P9)
But I think it’s kind of hard too, because [transplant recipients] are on a lot of medications. And a lot of medications are making you sick to your stomach.(INT, P17)
I think we’re kind of unique individuals and diet is a very important part of our lives, especially being post-transplant patients. I have to watch it more than maybe the average person, just so that you know, my organ will last longer and I will be healthier.(FG, P12)
I know that I need to be healthy as a transplant recipient so that I can live for a long time and keep my—like, the healthy body is important for a healthy heart which is my transplant type.(INT, P16)
What I hear from all of my heart transplant friends is that it’s really hard to find a new normal. And people outside of our circle think, “Oh, you’ve got a new heart, you’re fine.” Like, “What’s wrong?”, you know what I mean? And they don’t understand the amount of medications or—all of my transplant friends that I had five years ago, they’ve all had something major: rejection, now one has cancer, one had a bleed to the brain, one had lost her colon. I mean it’s all—so it’s a lot—to me it’s a lot of psychological stuff.(INT, P17)
And then of course our spouses too. Like, I think there’s a lot of spouses that have PTSD [post-traumatic stress disorder] and stuff like that, I truly believe that, because it’s a change for them as well.(INT, P17)
In terms of motivation to participate, I echo everybody’s sentiments, but I would also add that I wanted to, knowing this was a new study, just help to the benefit of the transplant community as well.(FG, P10)
Theme 2—Beneficial Program Components
You know, this is science, it does work. And you know, if you listen to the news every day you get a different diet tip every day and most of it’s garbage and doesn’t apply to you. This is my plan, it applies only to me. And if I follow it, it’ll work.(FG, P2)
I really like—from this 12-month study that we’re part of—is to gain knowledge and I really like the visual plate of the food placement part [GLB “MyPlate” lesson].(FG, P3)
I thought I ate healthy before. And then this kind of highlighted some areas that I could get better at, which over last year, according to all this I have done well with.(FG, P14)
I find you can’t manage what you can’t measure, and you know, this sheet that you’ve given us is, it’s a road map, it tells us what to do. And if you follow it, and you measure your food, and stick to it, it will work, and that’s what I found out over the last year.(FG, P2)
In the beginning, the first month I think, I didn’t use the app. And it was like, oh my goodness, the—you know, figuring out everything was a little daunting, right? Because for me, looking everything up, had that added—you know, it took longer to read, it took longer to find, it took longer to do. And then when I decided to try the app, it was like, “Ah, this is so much easier.”(INT, P18)
I did look forward to it, I did look forward to coming. For sure. Because we all got along really well. So that was a good thing, the group thing was good.(FG, P1)
[Participant FG, P6] started a Facebook page…. It was nice because we could chat with each other and say, “Hey, I found this recipe and it keys in to what we just learned.”(FG, P1)
Theme 3—Suggestions for Improvement
3.2.2. Theme Unique to the Nutrigenomics-Based Intervention (Tx-GLB + Ngx)
Theme 4—Unique Aspects of Nutrigenomics-Based Recommendations
It’s personalized, which is a big advantage. So it tells you—as opposed to the standard recommendations for the general population—the idea with this is that it’s got an advantage specifically for me.(INT, P16)
I always knew an avocado was good for you, but seeing that I have an enhanced response to those kinds of fats—now I have a push to put that into my diet, that extra—(FG, P7)
… and I’ve done the same with the exact same food too, yeah, for sure.(FG, P10)
This eating between meals that we talked about. I know—I always want to snack! And when I read that—when I first read that, I went “Ah! It’s not my fault.” And now I recognize that, and I embrace it, and I just make better choices, and I think I’m a little easier on myself.(FG, P7)
All of a sudden, I had this whole big list of things that I had to look at, and it was hard for me. And especially because I’m a person who likes to get things right, then it was a lot of work. And so initially it was—like, I was dedicating a lot of time every day to trying to figure out how I was going to do things.(INT, P16)
When I started, I had to just focus on one or two. Because if I focussed on all of these things, I got really overwhelmed. So I had to pick a couple.(FG, P7)
What I’ve realized is it is hard work, I mean just understanding it, you know—between all the fats and the balance that, you know, your calories have to be divided into this percentage, this percentage, this percentage…you do have to take time, cutting vegetables and having all that fresh, whole food, it does take time. But that’s the commitment.(FG, P9)
I started trusting myself and I would—I could eyeball my cup of cereal, and I was pretty good at eyeballing it. So that was the first step. And then over the course of the six months, you kind of figure out what foods have—you know, something that’s going to be high in protein.(INT, P16)
I was doing it regularly for probably like 4 months or so, actually—so I was pretty impressed with myself. And then I got to know kind of like what to expect, and then if something new came in, then I would check it maybe?(FG, P7)
I have 4 or 5 kind of “go-to” lunches that I don’t have to think about, don’t have to worry about—I can just go “Yeah, that’s a good one, ok” and off I go.(INT, P18)
And then I just decided, I feel better, my day’s better, I last longer without snacking, I just feel better by doing this. And then I just—so I’ve done it for the whole year.(FG, P7)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Entwistle, T.R.; Green, A.C.; Fildes, J.E.; Miura, K. Adherence to Mediterranean and low-fat diets among heart and lung transplant recipients: A randomized feasibility study. Nutr. J. 2018, 17, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Hickman, I.J.; Hannigan, A.K.; Johnston, H.E.; Elvin-Walsh, L.; Mayr, H.L.; Staudacher, H.M.; Barnett, A.; Stoney, R.; Salisbury, C.; Jarrett, M.; et al. Telehealth-delivered, Cardioprotective Diet and Exercise Program for Liver Transplant Recipients: A Randomized Feasibility Study. Transplant. Direct 2021, 7, e667. [Google Scholar] [CrossRef]
- Kuningas, K.; Driscoll, J.; Mair, R.; Smith, H.; Dutton, M.; Day, E.; Sharif, A.A. Comparing Glycaemic Benefits of Active Versus Passive Lifestyle Intervention in Kidney Allograft Recipients: A Randomized Controlled Trial. Transplantation 2020, 104, 1491–1499. [Google Scholar] [CrossRef]
- Vallis, T.M.; Macklin, D.; Russell-Mayhew, S. Canadian Adult Obesity Clinical Practice Guidelines: Effective Psychological and Behavioural Interventions in Obesity Management. Available online: https://obesitycanada.ca/guidelines/behavioural (accessed on 18 February 2021).
- Williamson, D. Fifty Years of Behavioral/Lifestyle Interventions for Overweight and Obesity: Where Have We Been and Where Are We Going? Obesity 2017, 25, 1867–1875. [Google Scholar] [CrossRef] [Green Version]
- DiCecco, S.R.; Francisco-Ziller, N. Obesity and organ transplantation: Successes, failures, and opportunities. Nutr. Clin. Pract. 2014, 29, 171–191. [Google Scholar] [CrossRef]
- Hoogeveen, E.K.; Aalten, J.; Rothman, K.J.; Roodnat, J.I.; Mallat, M.J.; Borm, G.; Weimar, W.; Hoitsma, A.J.; de Fijter, J.W. Effect of obesity on the outcome of kidney transplantation: A 20-year follow-up. Transplantation 2011, 91, 869–874. [Google Scholar] [CrossRef]
- Van Son, J.; Stam, S.P.; Gomes-Neto, A.W.; Osté, M.C.; Blokzijl, H.; van den Berg, A.P.; Porte, R.J.; Bakker, S.J.; de Meijer, V.E. Post-transplant obesity impacts long-term survival after liver transplantation. Metabolism 2020, 106, 154204. [Google Scholar] [CrossRef]
- Baker, R.J.; Mark, P.; Patel, R.K.; Stevens, K.K.; Palmer, N. Renal association clinical practice guideline in post-operative care in the kidney transplant recipient. BMC Nephrol. 2017, 18, 1–41. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Liver transplantation. J. Hepatol. 2016, 64, 433–485. [Google Scholar] [CrossRef]
- Been-Dahmen, J.; Grijpma, J.W.; Ista, E.; Dwarswaard, J.; Maasdam, L.; Weimar, W.; Van Staa, A.; Massey, E.K. Self-management challenges and support needs among kidney transplant recipients: A qualitative study. J. Adv. Nurs. 2018, 74, 2393–2405. [Google Scholar] [CrossRef]
- Flattery, M.P.; Salyer, J.; Maltby, M.C.; Joyner, P.L.; Elswick, R.K. Lifestyle and health status differ over time in long-term heart transplant recipients. Prog. Transplant. 2006, 16, 232–238. [Google Scholar] [CrossRef]
- Hickman, I.J.; Coran, D.; Wallen, M.P.; Kelly, J.; Barnett, A.; Gallegos, D.; Jarrett, M.; McCoy, S.M.; Campbell, K.L.; Macdonald, G.A. ‘Back to Life’—Using knowledge exchange processes to enhance lifestyle interventions for liver transplant recipients: A qualitative study. Nutr. Diet. 2019, 76, 399–406. [Google Scholar] [CrossRef]
- Jamieson, N.J.; Hanson, C.S.; Josephson, M.A.; Gordon, E.J.; Craig, J.C.; Halleck, F.; Budde, K.; Tong, A. Motivations, Challenges, and Attitudes to Self-management in Kidney Transplant Recipients: A Systematic Review of Qualitative Studies. Am. J. Kidney Dis. 2016, 67, 461–478. [Google Scholar] [CrossRef]
- Stanfill, A.; Bloodworth, R.; Cashion, A. Lessons learned: Experiences of gaining weight by kidney transplant recipients. Prog. Transpl. 2012, 22, 71–78. [Google Scholar] [CrossRef]
- University of Pittsburgh Diabetes Prevention Support Centre. Group Lifestyle Balance Program. Available online: https://www.diabetesprevention.pitt.edu/for-the-public/ (accessed on 18 February 2021).
- Kramer, M.K.; Kriska, A.M.; Venditti, E.M.; Miller, R.G.; Brooks, M.M.; Burke, L.E.; Siminerio, L.M.; Solano, F.X.; Orchard, T.J. Translating the Diabetes Prevention Program: A comprehensive model for prevention training and program delivery. Am. J. Prev. Med. 2009, 37, 505–511. [Google Scholar] [CrossRef]
- Ali, M.K.; Echouffo-Tcheugui, J.; Williamson, D.F. How effective were lifestyle interventions in real-world settings that were modeled on the diabetes prevention program? Health Aff. 2012, 31, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Mudaliar, U.; Zabetian, A.; Goodman, M.; Echouffo-Tcheugui, J.B.; Albright, A.L.; Gregg, E.W.; Ali, M.K. Cardiometabolic Risk Factor Changes Observed in Diabetes Prevention Programs in US Settings: A Systematic Review and Meta-analysis. PLoS Med. 2016, 13, e1002095. [Google Scholar] [CrossRef]
- Allaire, B.T.; Tjaden, A.H.; Venditti, E.M.; Apolzan, J.W.; Dabelea, D.; Delahanty, L.M.; Edelstein, S.L.; Hoskin, M.A.; Temple, K.A.; Wylie-Rosett, J.; et al. DPP Research Group. Diet quality, weight loss, and diabetes incidence in the Diabetes Prevention Program (DPP). BMC Nutr. 2020, 6, 74. [Google Scholar] [CrossRef]
- Diabetes Prevention Program (DPP) Research Group. The Diabetes Prevention Program (DPP): Description of lifestyle intervention. Diabetes Care 2002, 25, 2165–2171. [Google Scholar] [CrossRef] [Green Version]
- University of Pittsburgh Diabetes Prevention Support Centre. 2017 Diabetes Prevention Program Group Lifestyle Balance™ Materials. Available online: https://www.diabetesprevention.pitt.edu/group-lifestyle-balance-materials/ (accessed on 18 February 2021).
- University of Pittsburgh Diabetes Prevention Support Centre. DPP-Group Lifestyle Balance Publications. Available online: https://www.diabetesprevention.pitt.edu/for-the-public/for-health-providers/glb-publications/ (accessed on 18 February 2021).
- Horne, J.; Gilliland, J.; O’Connor, C.; Seabrook, J.; Hannaberg, P.; Madill, J. Study protocol of a pragmatic randomized controlled trial incorporated into the Group Lifestyle Balance™ program: The nutrigenomics, overweight/obesity and weight management trial (the NOW trial). BMC Public Health 2019, 19, 310. [Google Scholar] [CrossRef] [Green Version]
- Fenwick, P.H.; Jeejeebhoy, K.; Dhaliwal, R.; Royall, D.; Brauer, P.; Tremblay, A.; Klein, D.; Mutch, D.M. Lifestyle genomics and the metabolic syndrome: A review of genetic variants that influence response to diet and exercise interventions. Crit. Rev. Food Sci. Nutr. 2019, 59, 2028–2039. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [Green Version]
- Baldeh, T.; MacDonald, T.; Kosa, S.D.; Lawson, D.O.; Stalteri, R.; Olaiya, O.R.; Alotaibi, A.; Thabane, L.; Mbuagbaw, L. More pilot trials could plan to use qualitative data: A meta-epidemiological study. Pilot Feasibility Stud. 2020, 6, 164. [Google Scholar] [CrossRef]
- O’Cathain, A.; Hoddinott, P.; Lewin, S.; Thomas, K.J.; Young, B.; Adamson, J.; Jansen, Y.J.; Mills, N.; Moore, G.; Donovan, J.L. Maximising the impact of qualitative research in feasibility studies for randomised controlled trials: Guidance for researchers. Pilot Feasibility Stud. 2015, 1, 32. [Google Scholar] [CrossRef] [Green Version]
- Dew, M.A.; DeVito Dabbs, A.J. Harnessing the Power of Qualitative Research in Transplantation. Am. J. Kidney Dis. 2016, 67, 357–359. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Chapman, J.R.; Israni, A.; Gordon, E.J.; Craig, J.C. Qualitative research in organ transplantation: Recent contributions to clinical care and policy. Am. J. Transplant. 2013, 13, 1390–1399. [Google Scholar] [CrossRef]
- Wall, A. The unlimited possibilities for qualitative research in liver transplantation. Liver Transpl. 2021. [Google Scholar] [CrossRef]
- Tong, A.; Dew, M.A. Qualitative research in transplantation: Ensuring relevance and rigor. Transplantation 2016, 100, 710–712. [Google Scholar] [CrossRef]
- Thorne, S.; Kirkham, S.R.; O’Flynn-Magee, K. The analytic challenge in interpretive description. Int. J. Qual. Methods 2004, 3, 1–11. [Google Scholar] [CrossRef]
- Thorne, S. Interpretive Description: Qualitative Research for Applied Practice, 2nd ed.; Routledge: New York, NY, USA, 2016; ISBN 9781629582993. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Krueger, R.A. Moderating Focus Groups; SAGE: London, UK, 2004; Available online: https://ocul-uwo.primo.exlibrisgroup.com/permalink/01OCUL_UWO/1hdoga6/alma991044769356505163 (accessed on 23 February 2021).
- Woolf, N.H.; Silver, C. Qualitative Analysis Using NVivo: The Five-Level QDA® Method; Routledge: New York, NY, USA, 2017; ISBN 1138743666. [Google Scholar]
- Saldaña, J. The Coding Manual for Qualitative Researchers; SAGE: Los Angeles, CA, USA, 2009; ISBN 9781847875488. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Gibbs, G.R. Analyzing Qualitative Data; SAGE: Los Angeles, CA, USA, 2007; ISBN 9780761949800. [Google Scholar]
- Fade, S.A.; Swift, J.A. Qualitative research in nutrition and dietetics: Data analysis issues. J. Hum. Nutr. Diet 2011, 24, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Poch, E.; González, D.; Giner, V.; Bragulat, E.; Coca, A.; de La Sierra, A. Molecular basis of salt sensitivity in human hypertension. Evaluation of renin-angiotensin-aldosterone system gene polymorphisms. Hypertension 2001, 38, 1204–1209. [Google Scholar] [CrossRef] [Green Version]
- Stutzmann, F.; Cauchi, S.; Durand, E.; Calvacanti-Proença, C.; Pigeyre, M.; Hartikainen, A.L.; Sovio, U.; Tichet, J.; Marre, M.; Weill, J.; et al. Common genetic variation near MC4R is associated with eating behaviour patterns in European populations. Int. J. Obes. 2009, 33, 373–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolton, L.A.; Walsh, S.M.; O’Sullivan, N.B.; Barnes, E.; McCormick, A.P.; Corish, C.A. Patient Perspectives of Weight Gain Following Orthotopic Liver Transplantation: A Qualitative Study. Liver Transpl. 2020, 26, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Castle, E.M.; Greenwood, J.; Chilcot, J.; Greenwood, S.A. Usability and experience testing to refine an online intervention to prevent weight gain in new kidney transplant recipients. Br. J. Health Psychol. 2021, 26, 232–255. [Google Scholar] [CrossRef]
- Vanhoof, J.; Vandenberghe, B.; Geerts, D.; Philippaerts, P.; De Mazière, P.; DeVito Dabbs, A.; De Geest, S.; Dobbels, F.; Picasso-Tx consortium. Shedding light on an unknown reality in solid organ transplant patients’ self-management: A contextual inquiry study. Clin. Transplant 2018, 32, e13314. [Google Scholar] [CrossRef]
- Michie, S.; Ashford, S.; Sniehotta, F.F.; Dombrowski, S.U.; Bishop, A.; French, D.P. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: The CALO-RE taxonomy. Psychol. Health 2011, 26, 1479–1498. [Google Scholar] [CrossRef]
- Lieber, S.R.; Kim, H.P.; Baldelli, L.; Evon, D.M.; Teal, R.; Nash, R.; Magee, G.; Desai, C.S.; Gerber, D.; Serrano, P.; et al. What liver transplant recipients want in a smartphone intervention to enhance recovery: Prototype for the LiveRight transplant app. Liver Transpl. 2020. [Google Scholar] [CrossRef]
- Gibson, C.A.; Gupta, A.; Greene, J.L.; Lee, J.; Mount, R.R.; Sullivan, D.K. Feasibility and acceptability of a televideo physical activity and nutrition program for recent kidney transplant recipients. Pilot Feasibility Stud. 2020, 6, 126. [Google Scholar] [CrossRef]
- Horne, J.; Gilliland, J.; O’Connor, C.; Seabrook, J.; Madill, J. Enhanced long-term dietary change and adherence in a nutrigenomics-guided lifestyle intervention compared to a population-based (GLB/DPP) lifestyle intervention for weight management: Results from the NOW randomised controlled trial. BMJ Nutr. Prev. Health 2020, 3, 49–59. [Google Scholar] [CrossRef]
- Sutcliffe, K.; Melendez-Torres, G.J.; Burchett, H.; Richardson, M.; Rees, R.; Thomas, J. The importance of service-users’ perspectives: A systematic review of qualitative evidence reveals overlooked critical features of weight management programmes. Health Expect. 2018, 21, 563–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Themes | Sub-Themes |
|---|---|
| 1. The post-transplant experience | 1A. Limited access to nutrition guidance |
| 1B. Existing health self-management skills | |
| 1C. Physical and psychosocial health factors | |
| 1D. Connection to other transplant recipients | |
| 2. Beneficial program components | 2A. Nutrition knowledge development |
| 2B. Clear goals and reinforcement; Self-monitoring guidance | |
| 2C. Peer support | |
| 3. Suggestions for improvement | Varied suggestions |
| Themes | Sub-Themes |
|---|---|
| 4. Unique aspects of nutrigenomics- based guidance | 4A. Advantages: Personalization |
| 4B. Challenges: Implementing recommendations | |
| 4C. Problem-solving: Learning trajectory |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anderson, S.; Brown, C.; Venneri, K.; Horne, J.R.; Matthews, J.I.; Madill, J.E. “You Can’t Manage What You Can’t Measure”: Perspectives of Transplant Recipients on Two Lifestyle Interventions for Weight Management. Transplantology 2021, 2, 210-223. https://doi.org/10.3390/transplantology2020020
Anderson S, Brown C, Venneri K, Horne JR, Matthews JI, Madill JE. “You Can’t Manage What You Can’t Measure”: Perspectives of Transplant Recipients on Two Lifestyle Interventions for Weight Management. Transplantology. 2021; 2(2):210-223. https://doi.org/10.3390/transplantology2020020
Chicago/Turabian StyleAnderson, Suzanne, Catherine Brown, Katherine Venneri, Justine R. Horne, June I. Matthews, and Janet E. Madill. 2021. "“You Can’t Manage What You Can’t Measure”: Perspectives of Transplant Recipients on Two Lifestyle Interventions for Weight Management" Transplantology 2, no. 2: 210-223. https://doi.org/10.3390/transplantology2020020
APA StyleAnderson, S., Brown, C., Venneri, K., Horne, J. R., Matthews, J. I., & Madill, J. E. (2021). “You Can’t Manage What You Can’t Measure”: Perspectives of Transplant Recipients on Two Lifestyle Interventions for Weight Management. Transplantology, 2(2), 210-223. https://doi.org/10.3390/transplantology2020020