
The Utility of Galectin-3 and HBME-1 Immunohistochemical Expression in Thyroid Cancer in the Maltese Population


Abstract
:1. Introduction
2. Materials and Method
2.1. Tissue Preparation and Staining
2.2. Immunostaining
2.3. Statistical Analysis
3. Interpretation and Analysis
4. Results
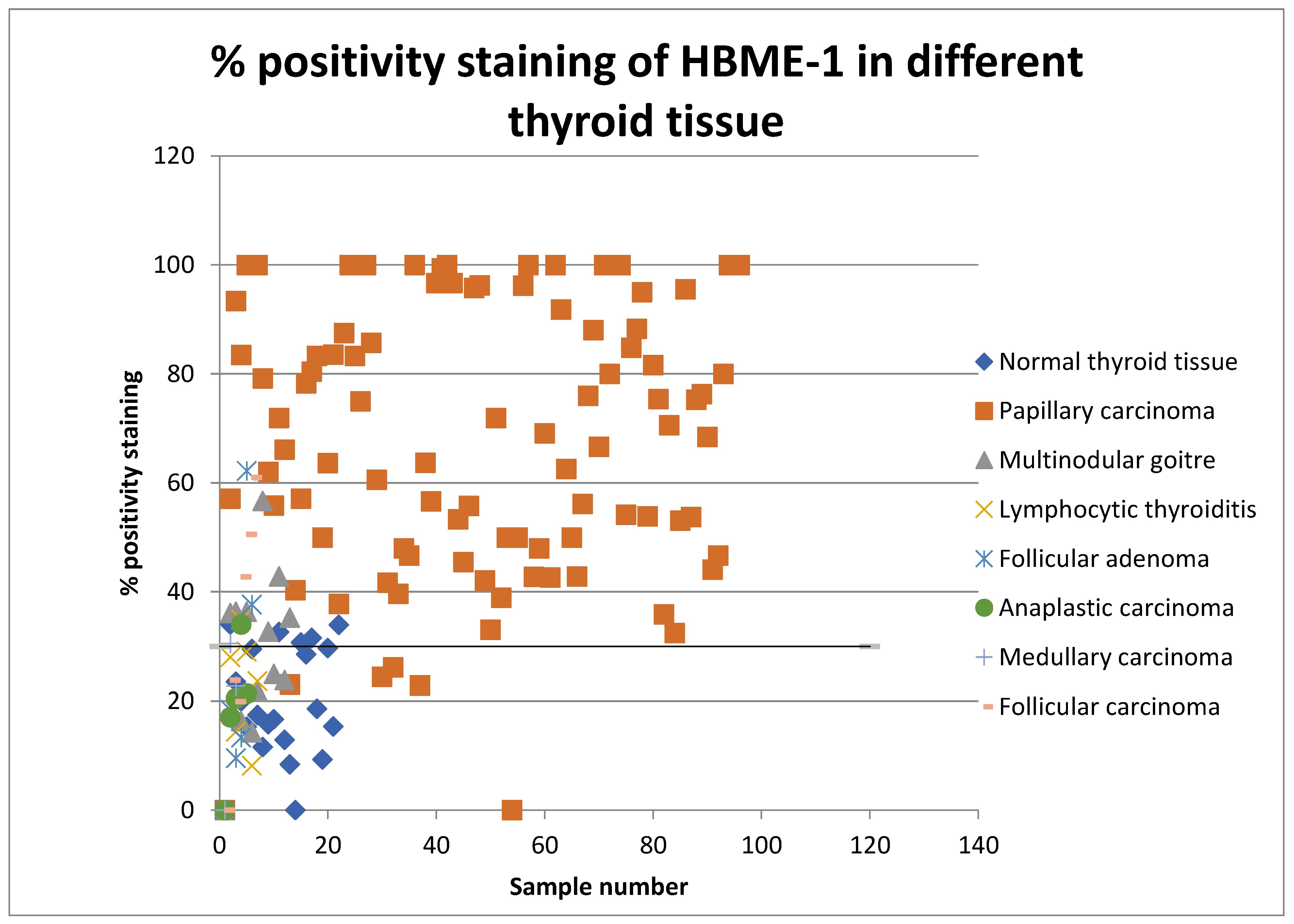
4.1. Immunohistochemical Results
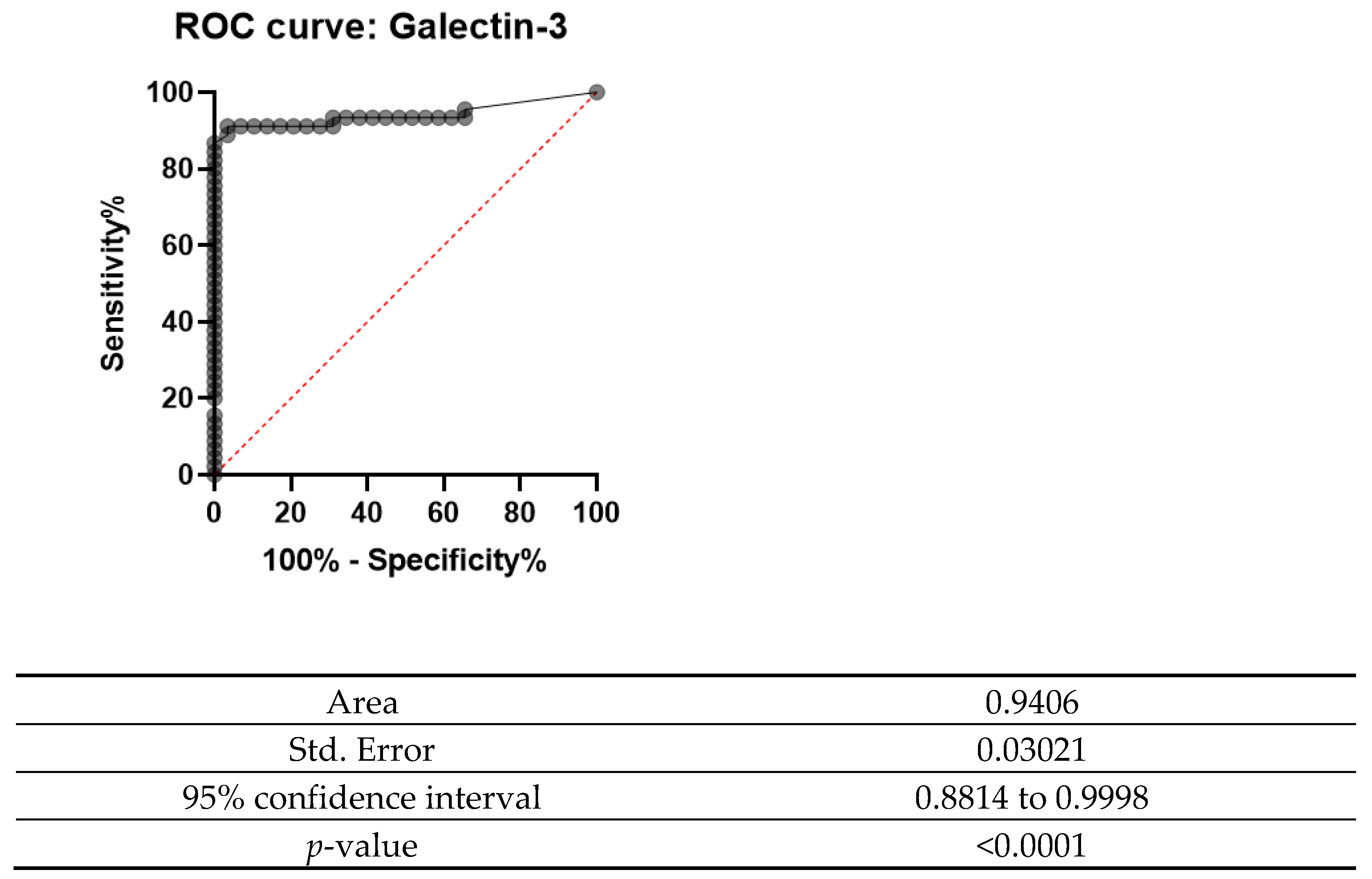
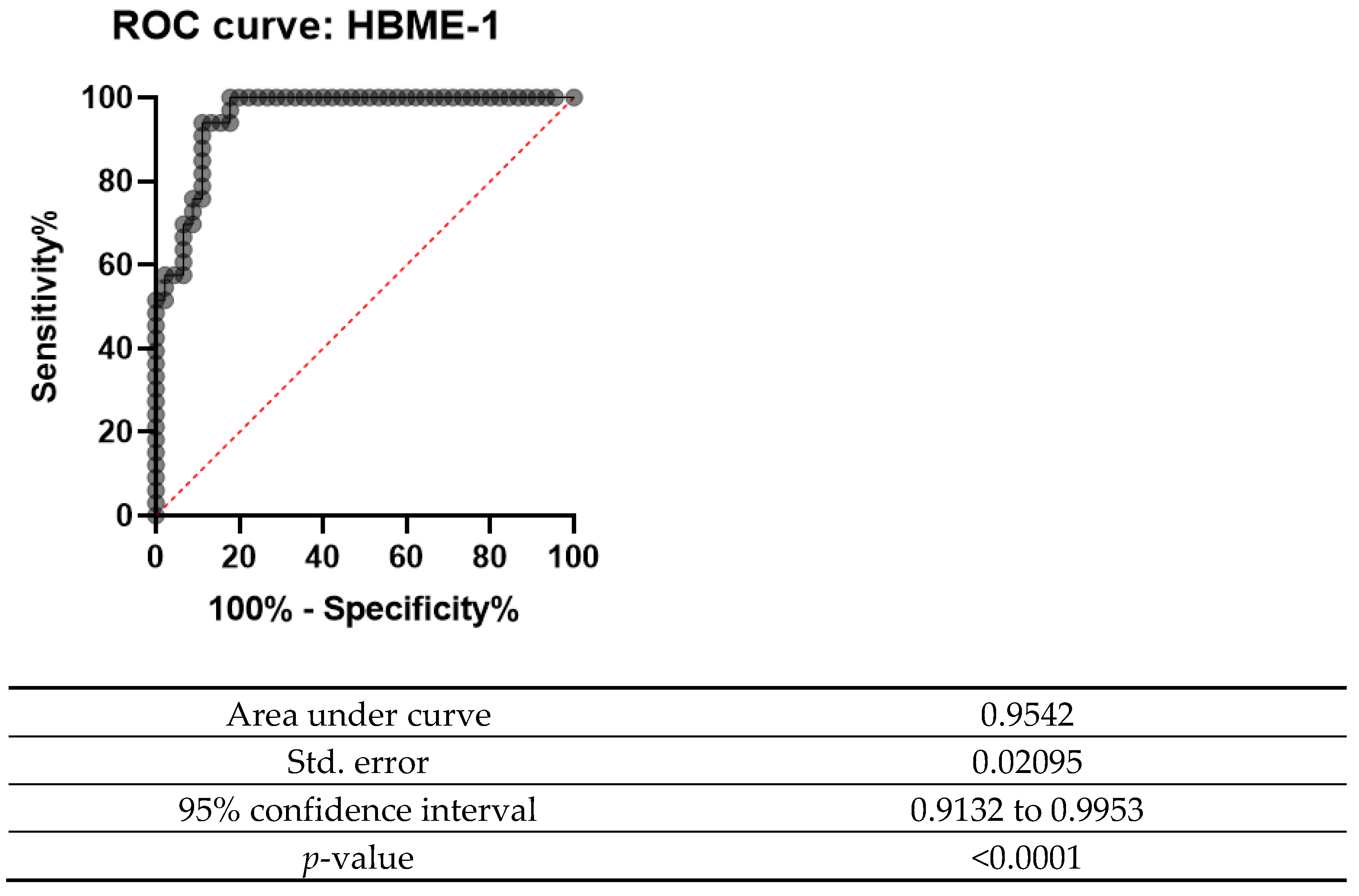
4.2. How Beneficial Are These Markers in the Clinical Setting?
5. Discussion
6. Conclusions
Limitations of This Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.; Laversanne, M.; Soerjomataram Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Longo, D.L.; Kasper, D.L.; Jameson, J.L.; Fauci, A.S.; Hauser, S.L.; Loscalzo, J. Harrison’s Principles of Internal Medicine, 16th ed.; McGraw-Hill Publishers: New York, NY, USA, 2012. [Google Scholar]
- Xu, D.; Wang, L.; Long, B.; Ye, X.; Ge, M.; Wang, K.; Guo, L.; Li, L. Radiofrequency ablation for postsurgical thyroid removal of differentiated thyroid carcinoma. Am. J. Transl. 2016, 8, 1876–1885. Available online: https://www.ncbi.nlm.nih.gov/pubmed/21190442 (accessed on 14 June 2019).
- Chen, A.Y.; Jemal, A.; Ward, E.M. Increasing incidence of differentiated thyroid cancer in the United States, 1988–2005. Cancer 2009, 115, 3801–3807. [Google Scholar] [CrossRef]
- Xu, B. Papillary Thyroid Carcinoma Overview. 2020. Available online: https://www.pathologyoutlines.com/topic/thyroidpapillary.html (accessed on 25 April 2022).
- Nikiforov, Y. RET/PTC re-arrangement in thyroid tumours. EndocrPathol. 2002, 13, 3–16. [Google Scholar] [CrossRef]
- Puxeddu, E.; Moretti, S.; Elisei, R.; Romei, C.; Pascucci, R.; Martinelli, M.; Marino, C.; Avenia, N.; Rossi, E.D.; Fadda, G.; et al. BRAF(V599E) Mutation is the Leading Genetic Event in Adult Sporadic Papillary Thyroid Carcinomas. J. Clin. Endocrinol. Metab. 2004, 89, 2414–2420. [Google Scholar] [CrossRef] [Green Version]
- Saad, A.; Falciglia, M.; Steward, D.L.; Nikiforov, Y.E. Amiodarone-induced Thyrotoxicosis and Thyroid Cancer: Clinical, Immunohistochemical, and Molecular Genetic Studies of a Case and Review of the Literature. Arch. Pathol. Lab. Med. 2004, 128, 807–810. [Google Scholar] [CrossRef]
- Mochizuki, K.; Kondo, T.; Nakazawa, T.; Iwashina, M.; Kawasaki, T.; Nakamura, N.; Yamane, T.; Murata, S.; Ito, K.; Kameyama, K.; et al. RET Rearrangements and BRAF Mutation in Undifferentiated Thyroid Carcinomas Having Papillary Carcinoma Components. Histopathology 2010, 57, 444–450. [Google Scholar] [CrossRef]
- Song, Q.; Wang, D.; Lou, Y.; Li, C.; Fang, C.; He, X.; Li, J. Diagnostic significance of CK19, TG, Ki 67 and galectin-3 expression for papillary thyroid carcinoma in the northeastern region of China. Diagn. Pathol. 2011, 6, 126. [Google Scholar] [CrossRef] [Green Version]
- Barroeta, J.E.; Baloch, Z.W.; Lal, P.; Pasha, T.L.; Zhang, P.J.; LiVolsi, V.A. Diagnostic Value of Differential Expression of CK19, Galectin-3, HBME-1, ERK, RET, and p16 in Benign and Malignant Follicular-derived Lesions of the Thyroid: An Immunohistochemical Tissue Microarray Analysis. Endocr. Pathol. 2006, 17, 225–234. Available online: https://www.ncbi.nlm.nih.gov/pubmed/17308359 (accessed on 5 May 2019). [CrossRef]
- Husain, A.S.; Jining, F.; Farah, T.; Al-Zohaili, O.; Husain, M.; Giorgadze, T. Differential expression of galectin-3, CK19, HBME1 and Ret iciprotein in the diagnosis of thyroid neoplasms by fine-needle aspiration biopsy. Cytojournal 2009, 6, 18. [Google Scholar]
- Newlaczyl, A.U.; Yu, L.G. Galectin-3—A Jack-of-All-Trades in Cancer. Cancer Lett. 2011, 313, 123–128. [Google Scholar] [CrossRef]
- Tang, W.; Huang, C.; Tang, C.; Xu, J.; Wang, H. Galectin-3 may serve as a potential marker for diagnosis and prognosis in papillary thyroid carcinoma: A meta-analysis. Onco Targets Ther. 2016, 9, 455–460. [Google Scholar] [CrossRef] [Green Version]
- Miskad, U.A.; Leiwakabessy, W.N.; Durry, M.F.; Rahawarin, H.; Cangara, M.H.; Djimahit, T. The Utility of Galectin-3 and HBME-1 in Differentiating Thyroid Lesions. Eur. J. Mol. Clin. Med. 2020, 7, 1177–1182. Available online: https://ejmcm.com/article_4599_36ffe00127a377c814d530ec7b8f5383.pdf (accessed on 5 May 2019).
- Rossi, E.D.; Straccia, P.; Palumbo, M.; Stigliano, E.; Revelli, L.; Lombardi, C.P.; Santeusanio, G.; Pontecorvi, A.; Fadda, G. Diagnostic and Prognostic Role of HBME-1, Galectin-3, and β-catenin in Poorly Differentiated and Anaplastic Thyroid Carcinomas. Appl. Immunohistochem. Mol. Morphol. 2013, 21, 237–241. [Google Scholar] [CrossRef]
- Ishibashi, H.; Suzuki, T.; Suzuki, S.; Moriya, T.; Kaneko, C.; Takizawa, T.; Sunamori, M.; Handa, M.; Kondo, T.; Sasano, H. Sex steroid hormone receptors in human thymoma. J. Clin. Endocrinol. Metab. 2003, 88, 2309–2317. [Google Scholar] [CrossRef]
- Zhang, L.; Krausz, T.; DeMay, R. A Pilot Study of Galectin03, HBME-1 and p27 Triple Immunostaining Pattern for Diagnosis of Indeterminate Thyroid Nodules in Cytology with Correlation to Histology. Appl. Immunohistochem. Mol. Morphol. 2015, 23, 481–490. [Google Scholar] [CrossRef] [Green Version]
- Griebeler, M.; Gharib, H. Thyroid Nodules and Cancer. In Endocrinology and Diabetes; Bandiera, F., Gharib, H., Griz, L., Faria, M., Eds.; Springer: Cham, Switzerland, 2022. [Google Scholar] [CrossRef]
- Nasr, M.R.; Mukhopadhyay, S.; Zhang, S.; Katzenstein, A.L. Immunohistochemical markers in diagnosis of papillary thyroid carcinoma: Utility of HBME1 combined with CK19 immunostaining. Mod. Pathol. 2006, 19, 1631–1637. [Google Scholar] [CrossRef]
- Collet, J.F.; Fajac, A. Galectin-3 immunodetection in fine-needle aspirates: Technical procedure and results. Ann. Pathol. 2006, 26, 347–351. [Google Scholar] [CrossRef]
- Giuliano, S.; Mirabelli, M.; Chiefari, E.; Vergine, M.; Gervasi, R.; Brunetti, F.; Innaro, N.; Donato, N.; Aversa, A.; Brunetti, A. Malignancy analysis of thyroid nodules in patients subjected to surgery with cytologcal and ultrasound based risk stratification. Endocrines 2020, 1, 102–118. [Google Scholar] [CrossRef]
- Artus, O.; Zenons, N.; Ilze, G.; Volanska, G.; Gardovskis, J. Immunohistochemical expression of HBME-1, E-cadherin and CD56 in the differential diagnosis of thyroid nodules. Medicina 2012, 48, 507–514. [Google Scholar] [CrossRef] [Green Version]
- Papotti, M.; Rodriguez, J.; Pompa, R.; Bartolazzi, A.; Rosai, J. Galectin-3 and HBME-1 Expression in Well-differentiated Thyroid Tumors with Follicular Architecture of Uncertain Malignant Potential. Mod. Pathol. 2005, 18, 541–546. [Google Scholar] [CrossRef]
- Mehdi, M.A.; JAsim, A.M.; Al-Ganber, M.F. The expression of Gal-3 and CK-19 in Hashimoto’s thyroiditis compared to Papillary thyroid carcinoma. Iraq. Med. J. 2018, 2, 86–90. [Google Scholar] [CrossRef]
- Herrmann, M.E.; LiVolsi, V.A.; Pasha, T.L.; Roberts, S.A.; Wojcik, E.M.; Baloch, Z.W. Immunohistochemical Expression of Galectin-3 in Benign and Malignant Thyroid Lesions. Arch. Pathol. Lab. Med. 2002, 126, 710–713. Available online: https://www.ncbi.nlm.nih.gov/pubmed/12033961 (accessed on 12 June 2019). [CrossRef]
- Cvejic, D.; Savin, S.; Golubovic, S.; Paunovic, I.; Tatic, S.; Havelka, M. Galectin-3 and Carcinoembryonic Antigen Expression in Medullary Thyroid Carcinoma: Possible Relation to Tumour Progression. Histopathology 2002, 37, 530–535. [Google Scholar] [CrossRef]
- Kovacs, R.B.; Foldes, J.; Winkler, G.; Bodo, M.; Sapi, Z. The investigation of galectin-3 in diseases of the thyroid gland. Eur. J. Endocrinol. 2003, 149, 449–453. [Google Scholar] [CrossRef] [Green Version]
- Alshenawy, H.A. Utility of Immunohistochemical Markers in Differential Diagnosis of Follicular-cell Derived Thyroid Lesions. J. Microsc. Ultrastruct. 2014, 2, 127–136. [Google Scholar] [CrossRef] [Green Version]
- Pusztaszeri, M.P.; Faquin, W.C.; Sadow, P.M. Tumor-Associated Inflammatory Cells in Thyroid Carcinomas. Surg. Pathol. Clin. 2014, 7, 501–514. [Google Scholar] [CrossRef]
- Kholova, I.; Kalfert, D.; Lintusaari, J.; Rajakorpi, E.; Ludvikova, M. Follicular epithelial Dysplasia as Hashimoto Thyroiditis- related Atypia: A Series of 91 specimen. Endocr. Pathol. 2021, 32, 368–374. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody | Clone and Source | Dilution | Source |
|---|---|---|---|
| Galectin-3 | Monoclonal, B2C10 | 1:400 | Santa Cruz biotechnology Inc., Santa Cruz, CA, USA |
| HBME-1 | Monoclonal HBME-1 | 1:50 | Santa Cruz biotechnology Inc., Santa Cruz, CA, USA |
| Secondary antibodies | Anti-mouse and anti-rabbit antibodies | No dilution | DAB Refine kit by Dako, Denmark |
| Diagnosis | Count |
|---|---|
| Papillary carcinoma | 23 |
| Papillary carcinoma and follicular adenoma | 6 |
| Papillary carcinoma and multinodular goitre | 7 |
| Papillary carcinoma and lymphocytic thyroiditis | 6 |
| Follicular carcinoma | 4 |
| Papillary carcinoma, lymphocytic thyroiditis and multinodular goiter | 4 |
| Papillary carcinoma, lymphocytic thyroiditis and follicular adenoma | 1 |
| Focus Papillary thyroid carcinoma with Hurthle cell carcinoma | 1 |
| Anaplastic carcinoma | 1 |
| Medullary carcinoma | 3 |
| Undifferentiated carcinoma | 1 |
| Type of thyroid cancer unknown | 1 |
| Type of Thyroid Lesion | Galectin-3 (Mean Staining Score) | p-Value | HBME-1 (Mean Staining Score) | p-Value | |
|---|---|---|---|---|---|
| Thyroid Carcinoma | Papillary carcinoma | 80.49 | 0.012 | 68.28 | 0.002 |
| Follicular carcinoma | 30.80 | 42.34 | |||
| Medullary carcinoma | 5.07 | 26.66 | |||
| Anaplastic carcinoma | 7.29 | 23.24 | |||
| Benign Thyroid Lesions | Follicular adenoma | 3.42 | 0.821 | 20.91 | 0.220 |
| Lymphocytic thyroiditis | 5.01 | 22.39 | |||
| Multinodular goiter | 3.91 | 30.20 | |||
| Normal thyroid tissue | 4.03 | 20.94 | |||
| Statistic | Value | 95% CI |
|---|---|---|
| Sensitivity | 92.86% | 85.10% to 97.33% |
| Specificity | 78.65% | 68.69% to 86.63% |
| Positive Predictive Value | 80.41% | 73.28% to 86.00% |
| Negative Predictive Value | 92.11% | 84.27% to 96.21% |
| Statistic | Value | 95% CI |
|---|---|---|
| Sensitivity | 95.00% | 83.08% to 99.39% |
| Specificity | 92.50% | 79.61% to 98.43% |
| Positive Predictive Value | 92.68% | 80.97% to 97.42% |
| Negative Predictive Value | 94.87% | 82.69% to 98.62% |
| Statistic | Value | 95% CI |
|---|---|---|
| Sensitivity | 90.91% | 78.33% to 97.47% |
| Specificity | 67.35% | 52.46% to 80.05% |
| Positive Predictive Value | 71.43% | 62.33% to 79.07% |
| Negative Predictive Value | 89.19% | 76.05% to 95.54% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vella, C.; Baldacchino, S.; Formosa, R.; Vassallo, J. The Utility of Galectin-3 and HBME-1 Immunohistochemical Expression in Thyroid Cancer in the Maltese Population. Endocrines 2022, 3, 225-239. https://doi.org/10.3390/endocrines3020021
Vella C, Baldacchino S, Formosa R, Vassallo J. The Utility of Galectin-3 and HBME-1 Immunohistochemical Expression in Thyroid Cancer in the Maltese Population. Endocrines. 2022; 3(2):225-239. https://doi.org/10.3390/endocrines3020021
Chicago/Turabian StyleVella, Christine, Shawn Baldacchino, Robert Formosa, and Josanne Vassallo. 2022. "The Utility of Galectin-3 and HBME-1 Immunohistochemical Expression in Thyroid Cancer in the Maltese Population" Endocrines 3, no. 2: 225-239. https://doi.org/10.3390/endocrines3020021
APA StyleVella, C., Baldacchino, S., Formosa, R., & Vassallo, J. (2022). The Utility of Galectin-3 and HBME-1 Immunohistochemical Expression in Thyroid Cancer in the Maltese Population. Endocrines, 3(2), 225-239. https://doi.org/10.3390/endocrines3020021