
The COVID-19 Pandemic Affected Hepatitis C Virus Circulation and Genotypic Frequencies—Implications for Hepatitis C Prevention, Treatment and Research



Abstract
:1. Introduction
1.1. Impact of COVID-19 on Other Viral Infections
1.2. HCV Diversity
2. The Hypothesis
3. Evaluation of the Hypothesis
4. Conclusions
4.1. Limitations of the Hypothesis
4.2. Final Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Handanagic, S.; Shadaker, S.; Drobeniuc, J.; Tsereteli, M.; Alkhazashvili, M.; Adesigbin, C.; Adamu, I.; Adabe, R.; Agwuocha, C.; Adisa, O.; et al. Lessons learned from global hepatitis C elimination programs. J. Infect. Dis. 2023. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, G.K.; Taylor, J.; Kok, J.; E Dwyer, D.; Dilcher, M.; Hua, H.; Levy, A.; Smith, D.; A Minney-Smith, C.; Wood, T.; et al. Circulation of influenza and other respiratory viruses during the COVID-19 pandemic in Australia and New Zealand, 2020–2021. West. Pac. Surveill. Response J. 2023, 14, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Verma, P.; Baskey, U.; Choudhury, K.R.; Dutta, S.; Bakshi, S.; Das, R.; Mondal, P.; Bhaduri, S.; Majhi, D.; Dutta, S.; et al. Changing pattern of circulating dengue serotypes in the endemic region: An alarming risk to the healthcare system during the pandemic. J. Infect. Public Health 2023, 16, 2046–2057. [Google Scholar] [CrossRef] [PubMed]
- Bin Saleh, K.; Badreldin, H.A.; Alqahtani, T.; Alsuhebany, N.; Alowais, S.A.; Al Sulaiman, K.; Alrashed, M.; Alsaeed, Y.; Alyousef, A.; Aldugiem, R.; et al. Assessing the influence of COVID-19 on influenza prevalence: A multicenter time series study. J. Infect. Public Health 2023, 16, 1989–1993. [Google Scholar] [CrossRef] [PubMed]
- Grohskopf, L.A.; Blanton, L.H.; Ferdinands, J.M.; Chung, J.R.; Broder, K.R.; Talbot, H.K.; Morgan, R.L.; Fry, A.M. Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices—United States, 2022–23 Influenza Season. MMWR Recomm. Rep. 2022, 71, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Li, X.; Tan, M.; Cheng, Y.; Chen, T.; Wei, H.; Zeng, X.; Xie, Y.; Liu, J.; Xiao, N.; et al. Epidemiological and Virological Surveillance of Seasonal Influenza Viruses—China, 2020–2021. China CDC Wkly. 2021, 3, 918–922. [Google Scholar] [CrossRef] [PubMed]
- Bancej, C.; Rahal, A.; Lee, L.; Buckrell, S.; Schmidt, K.; Bastien, N. National FluWatch mid-season report, 2021–2022: Sporadic influenza activity returns. Can. Commun. Dis. Rep. 2022, 48, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.; Qi, J.; Wu, J.; Zheng, M. Changes in Influenza Activity and Circulating Subtypes During the COVID-19 Outbreak in China. Front. Med. 2022, 9, 829799. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Mailloux, B.J.; Cook, E.M.; Culligan, P.J. Change of urban park usage as a response to the COVID-19 global pandemic. Sci. Rep. 2023, 13, 19324. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, H.; Liu, Y.; Pearson, C.A.B.; Jarvis, C.I.; Grundy, C.; Quilty, B.J.; Diamond, C.; Eggo, R.M.; Simons, D.; Gimma, A.; et al. Changing travel patterns in China during the early stages of the COVID-19 pandemic. Nat. Commun. 2020, 11, 5012. [Google Scholar] [CrossRef] [PubMed]
- Laury, J.; Hiebert, L.; Ward, J.W. Impact of COVID-19 Response on Hepatitis Prevention Care and Treatment: Results from Global Survey of Providers and Program Managers. Clin. Liver Dis. 2021, 17, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Lemoine, M.; Kim, J.U.; Ndow, G.; Bah, S.; Forrest, K.; Rwegasha, J.; Bouyou, M.; Napon, D.; Somda, S.; Sawadogo, A.; et al. Effect of the COVID-19 pandemic on viral hepatitis services in sub-Saharan Africa. Lancet Gastroenterol. Hepatol. 2020, 5, 966–967. [Google Scholar] [CrossRef] [PubMed]
- Wingrove, C.; Ferrier, L.; James, C.; Wang, S. The impact of COVID-19 on hepatitis elimination. Lancet Gastroenterol. Hepatol. 2020, 5, 792–794. [Google Scholar] [CrossRef] [PubMed]
- Blach, S.; Kondili, L.A.; Aghemo, A.; Cai, Z.; Dugan, E.; Estes, C.; Gamkrelidze, I.; Ma, S.; Pawlotsky, J.-M.; Razavi-Shearer, D.; et al. Impact of COVID-19 on global HCV elimination efforts. J. Hepatol. 2021, 74, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Messina, J.P.; Humphreys, I.; Flaxman, A.; Brown, A.; Cooke, G.S.; Pybus, O.G.; Barnes, E. Global distribution and prevalence of hepatitis C virus genotypes. Hepatology 2015, 61, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Timm, J.; Roggendorf, M. Sequence diversity of hepatitis C virus: Implications for immune control and therapy. World J. Gastroenterol. 2007, 13, 4808–4817. [Google Scholar] [CrossRef] [PubMed]
- Tung, H.D.; Chen, J.J. Genetic history of hepatitis C virus genotype 6 in Taiwan. J. Formos. Med. Assoc. 2023. online ahead of print. [Google Scholar]
- Simmonds, P.; Alberti, A.; Alter, H.J.; Bonino, F.; Bradley, D.W.; Brechot, C.; Brouwer, J.T.; Chan, S.W.; Chayama, K.; Chen, D.S.; et al. A proposed system for the nomenclature of hepatitis C viral genotypes. Hepatology 1994, 19, 1321–1324. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, M.; Ismail, M.H.; Leitner, T.; Faleo, G.; Alwazzeh, M.J.; Mbisa, J.L.; Fiore, J.R.; Santantonio, T.A. A novel candidate hepatitis C virus genotype 4 subtype identified by next generation sequencing full-genome characterization in a patient from Saudi Arabia. Front. Microbiol. 2023, 14, 1285367. [Google Scholar] [CrossRef] [PubMed]
- Hanafiah, K.M.; Groeger, J.; Flaxman, A.D.; Wiersma, S.T. Global epidemiology of hepatitis C virus infection: New estimates of age-specific antibody to HCV seroprevalence. Hepatology 2013, 57, 1333–1342. [Google Scholar] [CrossRef] [PubMed]
- Guntipalli, P.; Pakala, R.; Gara, S.K.; Ahmed, F.; Bhatnagar, A.; Coronel, M.-K.E.; Razzack, A.; Solimando, A.; Thompson, A.; Andrews, K.; et al. Worldwide prevalence, genotype distribution and management of hepatitis C. Acta Gastroenterol. Belg. 2021, 84, 637–656. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H. Meta-analysis of genetic association studies. Ann. Lab. Med. 2015, 35, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Sacco, P.L.; De Domenico, M. Public health challenges and opportunities after COVID-19. Bull. World Health Organ. 2021, 99, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Kandeel, A.; Fahim, M.; Abukamar, S.; BahaaEldin, H.; Abuelsood, H.; Samy, S.; Deghedy, O.; Sheta, A.; Naguib, A.; El Guindy, N.; et al. Evidence for the elimination of viral hepatitis B and C in Egypt: Results of a nationwide survey in 2022. Liver Int. 2024, 44, 955–965. [Google Scholar] [CrossRef] [PubMed]
- Saludes, V.; Bordoy, A.E.; Yela, E.; Turú, E.; Not, A.; López-Corbeto, E.; Egea-Cortés, L.; González-Candelas, F.; Casabona, J.; Group for the Study and Control of Infectious Diseases in Prison (GRUMIP); et al. Incidence and molecular epidemiology of hepatitis C virus reinfection in prisons in Catalonia, Spain (Re-HCV study). Sci. Rep. 2023, 13, 16012. [Google Scholar] [CrossRef] [PubMed]
- Hedskog, C.; Parhy, B.; Chang, S.; Zeuzem, S.; Moreno, C.; Shafran, S.D.; Borgia, S.M.; Asselah, T.; Alric, L.; Abergel, A.; et al. Identification of 19 Novel Hepatitis C Virus Subtypes-Further Expanding HCV Classification. Open Forum Infect. Dis. 2019, 6, ofz076. [Google Scholar] [CrossRef] [PubMed]
- Casotto, V.; Amidei, C.B.; Saia, M.; Gregori, D.; Zanetto, A.; Fedeli, U.; Russo, F.P. Mortality related to HCV and other chronic liver diseases in Veneto (Italy), 2008–2021: Changes in trends and age-period-cohort effects. Liver Int. 2024, 44, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Jiang, L.; Liao, S.; Wu, F.; Yang, G.; Hou, L.; Liu, L.; Pan, X.; Jia, W.; Zhang, Y. Vaccines’ New Era-RNA Vaccine. Viruses 2023, 15, 1760. [Google Scholar] [CrossRef] [PubMed]
- Patra, T.; Meyer, K.; Haga, Y.; Reagan, E.K.; Weissman, D.; Ray, R. Hepatitis C virus E1 and modified E2 delivered from an mRNA vaccine induces protective immunity. NPJ Vaccines 2023, 8, 42. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
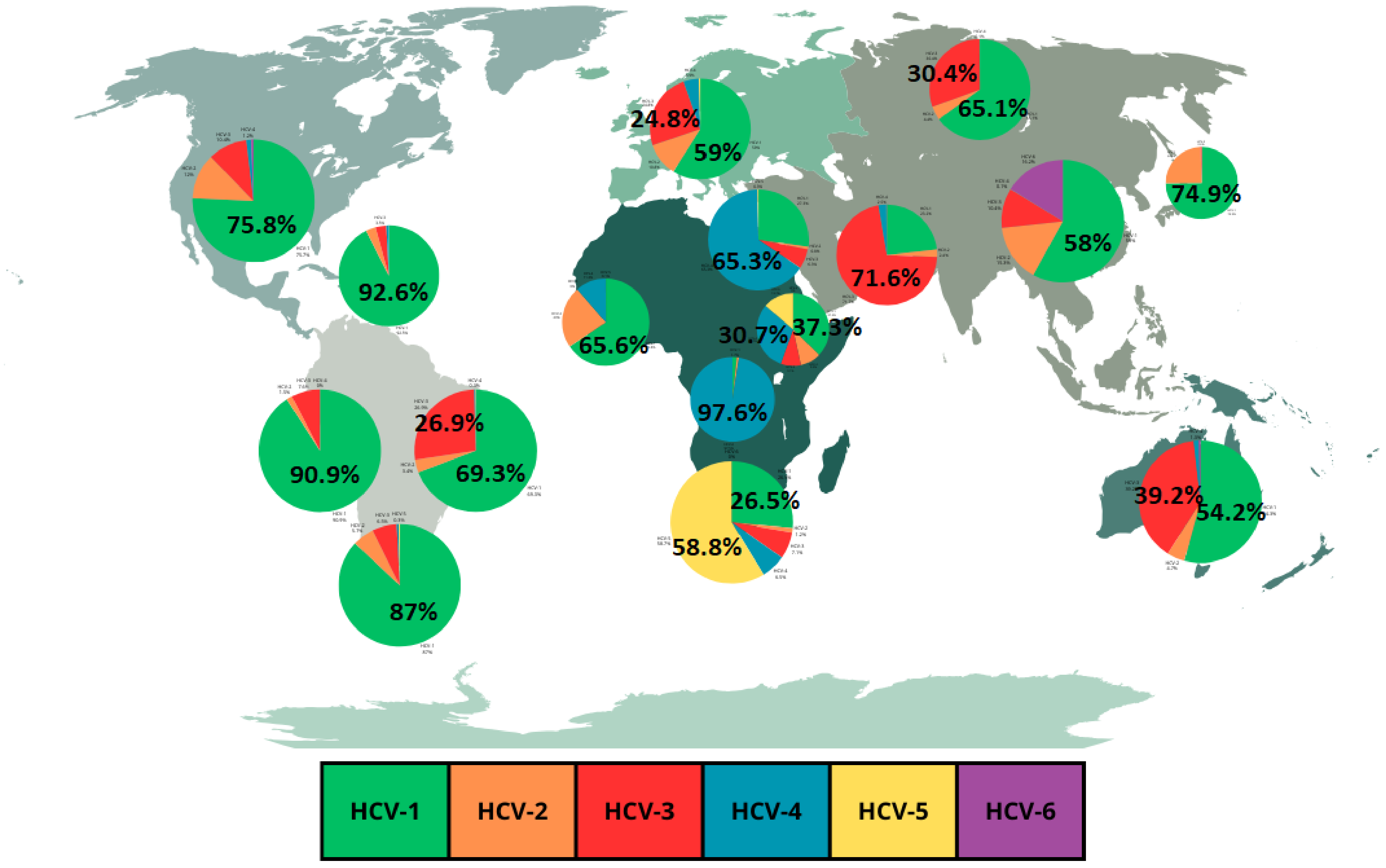
| Main Region | HCV-1 | HCV-2 | HCV-3 | HCV-4 | HCV-5 | HCV-6 |
| North America | 75.8% | 12% | 10.4% | 1.2% | 0.1% | 0.6% |
| Caribbean | 92.6% | 3.2% | 3.5% | 0.8% | 0 | 0 |
| Tropical Latin America | 69.3% | 3.4% | 26.9% | 0.3% | 0.1% | 0 |
| Andean Latin America | 90.9% | 1.5% | 7.6% | 0 | 0 | 0 |
| Southern Latin America | 87% | 5.7% | 6.5% | 0.5% | 0.3% | 0 |
| Southern Africa | 26.5% | 1.2% | 7.1% | 6.5% | 58.8% | 0 |
| Central Africa | 1.7% | 0.8% | 0 | 97.6% | 0 | 0 |
| Eastern Africa | 37.3% | 92.% | 9.1% | 30.7% | 13.7% | 0 |
| Western Africa | 65.6% | 23% | 0 | 11.3% | 0.1% | 0 |
| North Africa/Middle East | 27.3% | 0.8% | 6.3% | 65.3% | 0.3% | 0 |
| Western Europe | 59% | 10.8% | 24.8% | 4.9% | 0.5% | 0 |
| Eastern Europe | 65.1% | 4.4% | 30.4% | 0.1% | 0 | 0 |
| South Asia | 23.2% | 2.4% | 71.6% | 2.5% | 0.1% | 0.1% |
| East Asia | 58% | 15.3% | 10.4% | 0.1% | 0 | 16.2% |
| Asia Pacific | 74.9% | 24.5% | 0.6% | 0 | 0 | 0 |
| Australasia | 54.2% | 4.7% | 39.2% | 1.3% | 0 | 0.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliveira Correa, J.D.; Chies, J.A.B. The COVID-19 Pandemic Affected Hepatitis C Virus Circulation and Genotypic Frequencies—Implications for Hepatitis C Prevention, Treatment and Research. Epidemiologia 2024, 5, 160-166. https://doi.org/10.3390/epidemiologia5020011
Oliveira Correa JD, Chies JAB. The COVID-19 Pandemic Affected Hepatitis C Virus Circulation and Genotypic Frequencies—Implications for Hepatitis C Prevention, Treatment and Research. Epidemiologia. 2024; 5(2):160-166. https://doi.org/10.3390/epidemiologia5020011
Chicago/Turabian StyleOliveira Correa, Julio Daimar, and José Artur Bogo Chies. 2024. "The COVID-19 Pandemic Affected Hepatitis C Virus Circulation and Genotypic Frequencies—Implications for Hepatitis C Prevention, Treatment and Research" Epidemiologia 5, no. 2: 160-166. https://doi.org/10.3390/epidemiologia5020011
APA StyleOliveira Correa, J. D., & Chies, J. A. B. (2024). The COVID-19 Pandemic Affected Hepatitis C Virus Circulation and Genotypic Frequencies—Implications for Hepatitis C Prevention, Treatment and Research. Epidemiologia, 5(2), 160-166. https://doi.org/10.3390/epidemiologia5020011