Abstract
Osteogenesis imperfecta (OI) often results in recurrent fractures and/or progressive bowing of the long bones, including the arms. Upper extremity deformity has been shown to negatively impact function. The objective of this retrospective case series is to assess the ability to correct deformity, improve function and evaluate the complications and revision rates in our patients with OI who have undergone forearm deformity correction. A retrospective study, approved by The University of Nebraska Medical Center Institutional Review Board, was conducted with OI patients who underwent forearm osteotomy and fixation of one or both forearm bones between December 2011 and August 2018. There were no exclusion criteria. The electronic medical records were reviewed for patient demographics, surgical details, revisions and complications. A total of 48 procedures on 27 forearms in 18 patients were performed during the study. Surgery was performed in children with forearm deformity and recurrent fractures that were interfering with function. Half of the patients had surgery on one forearm and half had surgery on both forearms. The majority of the patients have Type III OI. There were multiple complications, the most common being wire migration which required either replacement or advancement of the wire. In conclusion, forearm deformity in OI is possible, with good healing of osteotomies and fractures, although many patients may require multiple surgical interventions.
1. Introduction
Osteogenesis imperfecta (OI) is a heterogeneous genetic disorder most commonly causing Type I collagen abnormalities. Abnormal Type I collagen results in frequent fractures often from minimal trauma, bowing deformities of long bones, short stature and scoliosis. Disease severity varies significantly with some patients experiencing few fractures and little extra-skeletal manifestations (typically Type I) to patient with severe OI who present with frequent fractures, bowing of long bones, short stature and often scoliosis (Types III and IV) [1].
Orthopedic management of OI deals with the treatment of acute fractures and bowing deformities of the long bones. Surgical treatment of femoral and tibial bowing with osteotomies and intramedullary fixation is well accepted in patients with moderate to severe OI and has been shown to improve function and decrease fracture rates [2]. Upper extremity deformity correction has often not been the focus in pediatric patients, although there have been several recent studies showing humeral deformity correction and rodding led to improved function and decreased fracture burden [3,4,5]. Forearm deformity has not been addressed as commonly but can be a major functional concern. Amako et al. showed that children with mild upper extremity deformity have reduced mobility and children with severe deformity have reduced mobility and functional abilities [6]. Two recent publications from high volume OI centers reviewed patients who underwent forearm deformity correction and showed improved function and decreased fracture burden [5,7]. The objectives of this retrospective case series are to assess the ability to correct forearm deformity and function with variations of surgical intervention practiced in our clinic and to evaluate the rates of complication and revision surgery.
2. Materials and Methods
This is a retrospective Institutional Review Board (IRB) approved study of patients with OI at our institution who underwent forearm osteotomy and fixation for deformity correction between December 2011 and August 2018. There were no exclusion criteria. The electronic medical records were reviewed for patient demographics, surgical details, revisions and complications. Pediatric Outcomes Data Collection Instrument (PODCI) data were utilized if available. A total of 48 procedures on 27 forearms in 18 patients were performed during the study period. Patient demographics are shown in Table 1.

Table 1.
Demographics.
Surgery
The indication for surgery in all children was deformity with recurrent fracture and loss of motion interfering with function (Figure 1). Surgical treatment of the forearm bones was discussed with families when the children were experiencing multiple radius and/or ulna fractures that resulted in bowing of the forearm that resulted in difficulties with function. All surgeries were performed by the senior author. Forty-eight total bony procedures on 18 patients were performed with 9 patients having only one forearm corrected and 9 having both forearms corrected. In total, 29 total procedures were performed on the right (14 forearms) and 19 total procedures on the left (13 forearms). Fourteen patients are right-hand dominant, 1 is left-hand dominant, and 3 do not have hand dominance recorded in the chart. Bilateral forearm surgery was performed in separate operative trips for all except one patient whose mother requested that we treat both forearms in the same operative setting. If there were recent fractures, we attempted to percutaneously pass a k-wire in the radius or ulna as we manually corrected the deformity. If this was deemed unsafe, or if an osteotomy was needed to correct the deformity, we opened at the apex of the deformity and attempted to perform one osteotomy. We routinely performed this with a rongeur, passing a separate wire into the next segment before passing the wire across the osteotomy site. If the deformity could not be corrected fully we performed a second osteotomy. The ulnar wire was placed across the olecranon apophysis to protect the entire ulna down to the distal ulnar physis. The radial wire was placed through the radial styloid across the distal radial physis up to the proximal radial physis to protect the entire radius. The radius was typically approached through the anterior volar approach, with exceptions when dorsal or radial approaches were performed depending on the apex and severity of the radial bow. When the radius has significant bowing present, it was often subcutaneous, and the approach can be safer and more direct to approach it in a non-standard direct manner. Figure 2 shows typical preoperative deformity and postoperative healed osteotomies over 5 years. Post operatively patients were placed into a sugar tong splint for 4 weeks after surgery. Postoperative X-rays were performed at 4 weeks, and patients were then transitioned to a removable splint for an additional 3–4 weeks.

Figure 1.
A 4-year-old female with Type III OI with typical appearing recurrent fractures and deformity of the forearm.
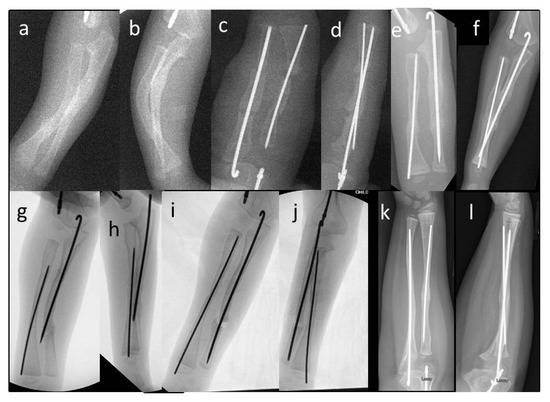
Figure 2.
(a,b) A 3.5-year-old male with Type III OI. Note significant radius and ulnar bowing and immediate postoperative deformity correction. 2 (c,d) With multi-level osteotomies and rod placement. (e,f) Healed osteotomies at 3 months post-op. (g,h) Two years later, at age 5.5, you can see how much the patient has grown and a fracture at the tip of the ulnar wire. (i,j) Immediate post-op after revision of the radial wire and fixation of the ulna with a new wire. (k,l) Most recent follow up X-ray at 9 years of age.
3. Results
There were no neurovascular complications of surgery. One patient who had a pseudarthrosis/non-union of the ulna and radius healed after revision rodding and bone grafting. Twelve forearms required more than one procedure (range 2–4 surgical procedures), with the majority of these due to prominent hardware. Fifteen forearms required only one surgery. The average radiographic follow-up was 1.9 years (range 8 days–5.5 years). All patients went on to heal their fractures or osteotomies at final radiographic follow-up. Five patients required revision for a wire that no longer protected the entire length of the bone or revision for bowing or fracture at the tip of a wire. One patient with Type III OI developed a cross union between the radius and ulna after severe deformity correction.
The following sections break down outcomes for patients based on one or both forearms corrected and one or multiple surgeries required.
3.1. Unilateral Forearm Surgery Patients
Nine patients (six females and three males) had surgery performed on one forearm, with a total of 13 surgeries. The average age of first surgery was 7.9 years (range 4.1–12.4). The OI type distribution is shown in Table 2. Five surgeries were on the right forearm and 4 surgeries were on the left. During the index surgery, fixation of the radius and ulna was performed on six patients and fixation of the ulna only on three. One patient subsequently had an additional surgery with fixation of the radius and ulna. Two patients were treated with titanium flexible nails, one with Type I and one with Type III, the other seven patients were treated with stainless steel 0.045” or 0.062” k-wires.
Table 2.
Unilateral Forearm Surgery.
Among the patients who had only one forearm corrected, seven have only required one surgery at an average of 3.4 years post-op, and two have required three surgeries. The first revision for both patients was for prominent ulnar wires that required trimming the wire in one patient, at 48 days post-op, and advancement of the wire in the other, at 55 days post-op. The second surgery for one patient (Type I OI) was due to recurrent fractures and deformity of the radius, which had not been rodded during the first surgery. This was performed 2 years after her index procedure. In her first surgery, the radius was felt to be well aligned and the ulna underwent open osteotomy and placement of a 2.0 mm titanium flexible nail. She subsequently underwent open osteotomies and rodding of both the radius, with a 2.5 mm titanium flexible nail, and ulna, with a new 2.0 mm titanium flexible nail, and has not required another surgery in 4.5 years. The other patient (Type III) sustained a proximal ulna fracture at the tip of the ulnar wire 4 years after her index procedure. The ulna had grown around the wire, so that the proximal ulna was no longer protected and the fracture occurred just proximal to the wire and avulsed her olecranon. She underwent open reduction and tension band fixation for the olecranon fracture, which healed uneventfully.
3.2. Bilateral Forearm Surgery Patients
Nine patients (four females and five males) had surgery on both forearms, for a total of 35 surgeries. The average age of the first forearm surgery was 5.3 years (range 2.2–10.2). Eight patients had each forearm operated on in separate operative settings and one had both forearms operated on in the same operating session per the mother’s request (4-year-old male with Type III OI). The patients who had both forearms operated on tend to have more severe OI than patients who had unilateral surgery; with eight patients having Type III OI and one with Type XV. The average age of the first forearm surgery was 5.27 years. All patients were treated with 0.045” or 0.062” k-wires, no patients were treated with flexible nails. Four patients have required more than one surgery on each forearm, four patients required only one surgery on each forearm and one patient required three surgeries on one forearm and one surgery on the contralateral forearm. Of the five patients who had more than one procedure done on each forearm, the number of surgeries per arm ranged from 2–4, with six procedures being done to advance or trim prominent wires.
3.3. Single versus Multiple Forearm Surgery
Fifteen forearms in eleven patients required only one surgery, see Table 3 for OI types. The average age of each surgery was 6.23 years (range 4.14–12.37 years), five patients were female and six patients were male. Implants included stainless steel 0.045” and 0.065” k-wires, two patients had ulnar fixation only and nine had fixation in the radius and the ulna. The average time from surgery to last X-ray follow-up was 432 days.
Table 3.
Single Forearm Surgery.
Twelve forearms in eight patients have required more than one surgery (range of 2–4 surgeries), see Table 4 for OI types. The average age of the first procedure was 6.19 years (range 2.22–10.71). The average time to first revision surgery was 1.19 years (range 18 days–2.86 years). Four forearms (three patients) required two surgeries, with an average age of the first surgery of 6.37 years, average age of revision 7.62 years. Six forearms (six patients) required three surgeries, average age 6.87 years, average age of first revision 7.89 years, second revision 9.6 years. Two forearms required four surgeries. One patient had their first surgery at 2.4 years, last surgery at 5.1 years with a current age of 7.6 years. The ulna was treated only at the first and second surgery, the radius was also treated at the third surgery. The other patient with four surgeries had their first surgery at 5.9 years with an ulnar osteotomy and wire placement, the first revision at 7.5 years, third at 7.8 years, fourth at 9.9 years with fixation of both radius and ulna.
Table 4.
Multiple Forearm Surgery.
3.4. Ulnar Fixation Only
Seven patients with eight forearms had only the ulna rodded during their first deformity correction. Three of these patients have not required a subsequent surgical intervention. Of the five patients who had more than one surgical intervention, two still only have hardware in the ulna and have not required radial hardware. Three underwent subsequent surgical interventions, including osteotomy and rod placement, to correct radius deformity.
The most common cause for revision surgery was prominent wires that required revision or shortening. We have addressed this by developing special tamps to bury the tip of the wires. Since adopting this burying technique, we have observed fewer migrated wires post-surgery. Also, as k-wires cannot elongate with patients as they grow, five patients required procedures for revision of a wire that no longer protected the entire length of the bone or revision for bowing at the tip of a wire. One of our questions in reviewing our cases was if procedures that involved fixation of the ulna only increased the odds of requiring repeat surgical intervention to the radius. Among our eight patients with forearms whose index procedure only treated the ulna, only three have developed deformity of the radius that required intervention. Two additional patients required a repeat trip to the operating room to correct the ulna again but still did not require surgical intervention of the radius.
We have attempted to decrease the frequency of wire migration by bending the tip of the ulnar wire into a shepherd’s crook and/or keeping the wire straight and fully tamping it into the cartilage of the olecranon (Figure 3). For the radial wire, we have had a special tamp fashioned (Figure 4) that fits the end of the 0.062” k-wire and confirm both radiographically and under direct vision that the wire is completely buried in the cartilage of the radial styloid. Our current cohort of patients is not large enough and has not been followed long enough to determine if these changes have decreased our wire prominence problems, longer-term follow-up will help to determine this.
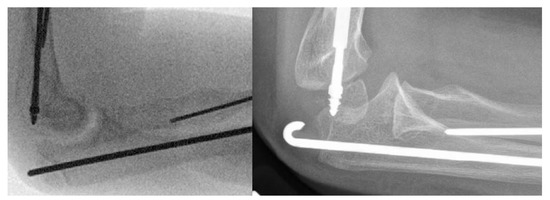
Figure 3.
Ulnar k-wire buried in the cartilage of the apophysis vs. ulnar wire buried with a crook in the wire.
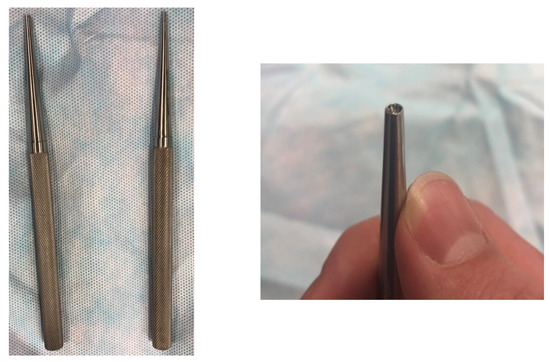
Figure 4.
Tamp utilized to bury the k-wire into the cartilage of the olecranon apophysis or the distal radial styloid cartilage.
4. Discussion
In this group of OI patients who underwent forearm deformity correction, over 80% had moderate to severe OI. Deformity correction and intramedullary rodding of the forearm decreased fracture burden by patient and parent report. Nine patients had surgery on one forearm and nine had surgery on both forearms. We prefer to treat one forearm at a time, so the children have at least one arm to use for play, schoolwork and to feed themselves with. Only one patient had both forearms operated in the same operating room trip and this was at the request of the patient’s mother. In terms of ulnar fixation only, we cannot draw a conclusion based on this small sample size. In our cohort, the majority of patients have not required further surgical intervention of either the radius or ulna. This may support the idea that if the ulna is the only bone of the two that has deformity, then it may be safe to only internally fixate the ulna.
A study in 2001 published by Khoshhal and Ellis out of Saudi Arabia reviewed 16 years of data in a total of 58 patients with OI, 5 of whom had upper extremity surgery. They reported a total of 11 primary upper extremity surgeries; 5 ulnar, 3 humeral and 3 radial. Their most common complication, as we experienced, was rod migration in the ulna requiring a second operative procedure. They noted that all five of their patients had difficulties with activities such as eating, transfers and independent dressing prior to correction of the deformities. All of their patients had improvement in these activities post operatively [8].
There is currently minimal orthopedic literature on the impact of upper extremity deformity in patients with OI and the impact of deformity correction on facture burden and function. There is one study, which showed that children with OI often have upper extremity deformities, 37% of patients, in both the humerus and the forearm. These deformities result in functional issues associated with self-care and mobility, and impair daily functional activities and independence as patients age. Children with Type III OI have the most severe deformities and mobility scores [6].
Prior to 1980, there were only five case reports of operative treatment of forearm deformities in OI patients. An orthopedic review article on OI published in 1971 discussed operative treatment in patients with OI and had one forearm procedure listed [9]. One of the case series on OI bony deformity surgical treatment was published in 1973 by Tiley and Albright. They reviewed all of their patients during a 12-year period. They identified four patients who had forearm deformity correction. They found that these patients had the most severe disease in their group of patients. These patients had severely limited forearm rotation and tended to hold their hands in a semi-pronated position. They found that the proximal ulna angulated posterolaterally, and the radius tended to angulate medially, and the distal forearm tended to bow in the opposite compensatory direction to the proximal bow. They report decent deformity correction at the time of surgery but did not feel that it helped to improve the patients forearm rotation and that ultimately as the children grew, they had recurrent deformity or hardware complications [10]. These procedures were all performed prior to modern medical treatment of OI. Our series of patients confirms that the majority of OI patients with forearm deformity have moderate to severe OI and that hardware complications continue to be the most common complication with recurrent deformity common.
One of the first studies to discuss operative interventions for children with OI and upper extremity deformities was published in 1980 by Root [11]. He reported that the indication for operative deformity correction of the upper extremity was when the upper extremity deformities interfered with upper limb function; including crutch use, inability to reach particular parts of the body or deformities associated with recurrent fractures. He reported on a total of 24 procedures in the upper extremity: 12 humerus corrections, 5 radius correction and 7 ulna corrections, with a total of 6 patients with forearm deformity corrections. In the paper he discussed that rodding of the radius and ulna is a very technically challenging procedure due to the often poor bone quality and the fact that the bones are usually severely deformed and are short. The authors concluded that these procedures are so extremely difficult that they felt that the operation is to be rarely indicated. From our series, we also experienced the technical challenge of deformity correction and hardware limitations due to the underlying bony disease. Like Root, we discuss with patients and their families the potential of surgical intervention of the upper extremities if the deformity or frequency of fractures is interfering with daily function.
Ashby et al. published their series of forearm rodding in 19 children with OI. Their mean age was significantly higher than ours at 9.5 years compared to ours at 6.37 years. The majority of their patients were Type III, similar to our series. The indications were forearm deformity resulting in functional limitations or recurrent fractures. They found that after forearm surgery the patient’s self-care and mobility scores increased significantly. They utilized K-wires for stabilization of both the radius and ulna in 16 cases, radius only in 5 cases and ulna only in 1 case. They also found several complications, most commonly prominent wires, which required revision. They also had two cases of non-union, which required repeat operation [7]. We also experienced the common complication of prominent wires in our case series, with wire revision being the most common reason for repeat surgery. In our small case series, we also had one case of a non-union, which required repeat operation and went on to heal successfully.
Franzone et al. [5] published their series of upper extremity surgeries in 2017, which included 19 forearms. The average age of their humeri and forearm surgeries was 8.7 years with most patients having Type III OI. The most common indication for surgery was progressive deformity with recurrent fractures resulting in functional difficulties. They utilized fixation in the radius and ulna in 10 patients, radius only in 3 patients and ulna only in 6 patients. Implants included k-wires and flexible nails. This series had seven forearm revisions with four patients requiring treatment for rod prominence or migration. Three patients required revision surgery due to re-fracture with rod bending. Similar to our case series, Franzone et al. also had several patients require revision surgery for wire migration.
The Ashby and Franzone publications, along with our patient cohort, demonstrate the good functional outcomes that can occur in these severe OI patients with forearm deformity correction but also highlight the concerns of poor bone quality with less than ideal implants available for these patients. Many patients with Type III OI cannot take an implant larger than a 0.062” k-wire, and, therefore, the concerns of wire-bending and subsequent re-bending of the forearm are present [7]. The inability to secure the implants often results in migration and resultant prominence which is common complication that occurs and results in the most repeat operations
Forearm deformity alone is not an adequate indication for forearm deformity correction with open osteotomies and fixation. The complications of these surgeries are very real: of the 27 forearms operated on in our study, 12 required multiple surgeries. None of the complications have resulted in long-term problems or neurovascular complications. That being said, there are a group of patients with OI who clearly benefit from forearm surgery, those with progressive deformity and recurrent fractures who are having functional difficulties secondary to the deformity, and resultant range of motion limitations are good candidates to consider performing forearm deformity correction. There is a suggestion based on our series that radial head dislocation can be related to isolated ulnar fractures and resultant progressive bowing. It is recognized that radial head dislocations are frequently painful and cause dysfunction in older patients with OI. Based on our experience, correction of ulnar alignment, even when there is some radial head subluxation, can reverse the progressive subluxation and potentially maintain motion and prevent dislocation.
This study has several significant limitations. First, this is a retrospective series of forearm deformities in all patients with OI who have been treated at our institution and, therefore, has all the limitations of a retrospective study. Second, we do not have consistent functional data, as we have only been collecting regular functional data from our patients on a consistent basis for the past 12–18 months. We are therefore unable to reliably report on function before and after surgery. Anecdotally, all patients and their families have been queried in follow-up if they are glad that they have had their forearms fixed, and they all universally are glad that they did, with the most common reasons given being improvement in function, especially with wheelchair mobility and decreased number of forearm fractures. This does add to the literature the number of patients with OI who have had forearm osteotomies and rodding for deformity and recurrent fractures with one of the recent studies having 19 forearms and the other having 19 patients with 22 forearms, and our study adding another 18 patients with 27 forearms.
In conclusion, forearm deformity correction and treatment of fractures with intramedullary wire fixation is a potential option in children with OI who have recurrent fracture or deformity of the forearm. Both fractures and osteotomies have the potential of healing well. Complications are common, with the majority of these related to backing out of the smooth implants or due to fracture or deformity at the end of the wires associated with growth.
Author Contributions
Conceptualization, M.W. and P.E.; methodology, M.W.; formal analysis, M.W.; investigation, M.W., P.E.; resources, M.W., P.E.; data curation, M.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of The University of Nebraska Medical Center (protocol code # 028-16-EP, 2-4-2016).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to rare disease and HIPPA data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Van Dijk, F.S.; Sillence, D.O. Osteogenesis Imperfecta: Clinical Diagnosis, Nomenclature and Severity Assessment. Am. J. Med. Genet. Part A 2014, 164, 1470–1481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruck, J.; Dahan-Oliel, N.; Montpetit, K.; Rauch, F.; Fassier, F. Fassier–Duval femoral rodding in children with osteogenesis imperfecta receiving bisphosphonates: Functional outcomes at one year. J. Child. Orthop. 2011, 5, 217–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashby, E.; Montpetit, K.; Hamdy, R.C.; Fassier, F. Functional Outcome of Humeral Rodding in Children with Osteogenesis Imperfecta. J. Pediatr. Orthop. 2018, 38, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Grossman, L.S.; Price, A.L.; Rush, E.T.; Goodwin, J.L.; Wallace, M.J.; Esposito, P.W. Initial experience with percutaneous IM rodding of the humeri in children with osteogenesis imperfecta. J. Pediatric Orthop. 2018, 38, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Franzone, J.M.; Bober, M.B.; Rogers, K.J.; McGreal, C.M.; Kruse, R.W. Re-alignment and intramedullary rodding of the humerus and forearm in children with osteogenesis imperfecta: Revision rate and effect on fracture rate. J. Child. Orthop. 2017, 11, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Amako, M.; Fassier, F.; Hamdy, R.C.; Aarabi, M.; Montpetit, K.; Glorieux, F.H. Functional analysis of upper limb deformities in osteogenesis imperfecta. J. Pediatr. Orthop. 2004, 24, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Ashby, E.; Montpetit, K.; Hamdy, R.C.; Fassier, F. Functional Outcome of Forearm Rodding in children with osteogenesis Imperfecta. J. Pediatr. Orthop. 2018, 38, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Khoshhal, K.I.; Ellis, R.D. Functional Outcome of Sofield Procedure in the Upper Limb in Osteogenesis Imperfecta. J. Pediatr. Orthop. 2001, 21, 236–237. [Google Scholar] [CrossRef] [PubMed]
- King, J.D.; Bobechko, W.P. Osteogenesis imperfecta: An orthopaedic description and surgical review. J. Bone Jt. Surgery. Br. Vol. 1971, 53, 72–89. [Google Scholar] [CrossRef]
- Tiley, F.; Albright, J.A. Osteogenesis imperfecta: Treatment by multiple osteotomy and intramedullary rod insertion. Report on thirteen patients. J. Bone Jt. Surg. Am. Vol. 1973, 55, 701–713. [Google Scholar] [CrossRef]
- Root, L. Upper limb surgery in osteogenesis imperfecta. Clin. Orthop. Relat. Res. 1981, 159, 141–146. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).