

Dual-Mobility Cups in Patients Undergoing Primary Total Hip Arthroplasty with Prior Lumbar Spine Fusion: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Search Protocol
2.2. Article Selection
- Population: patients undergoing elective primary THA with prior lumbar spine fusion;
- Intervention: dual-mobility cups;
- Comparison: either other types of cups or no cups;
- Outcome: incidence of postoperative complications.
2.3. Data Collection and Data Items
2.4. Statistical Analysis
3. Results
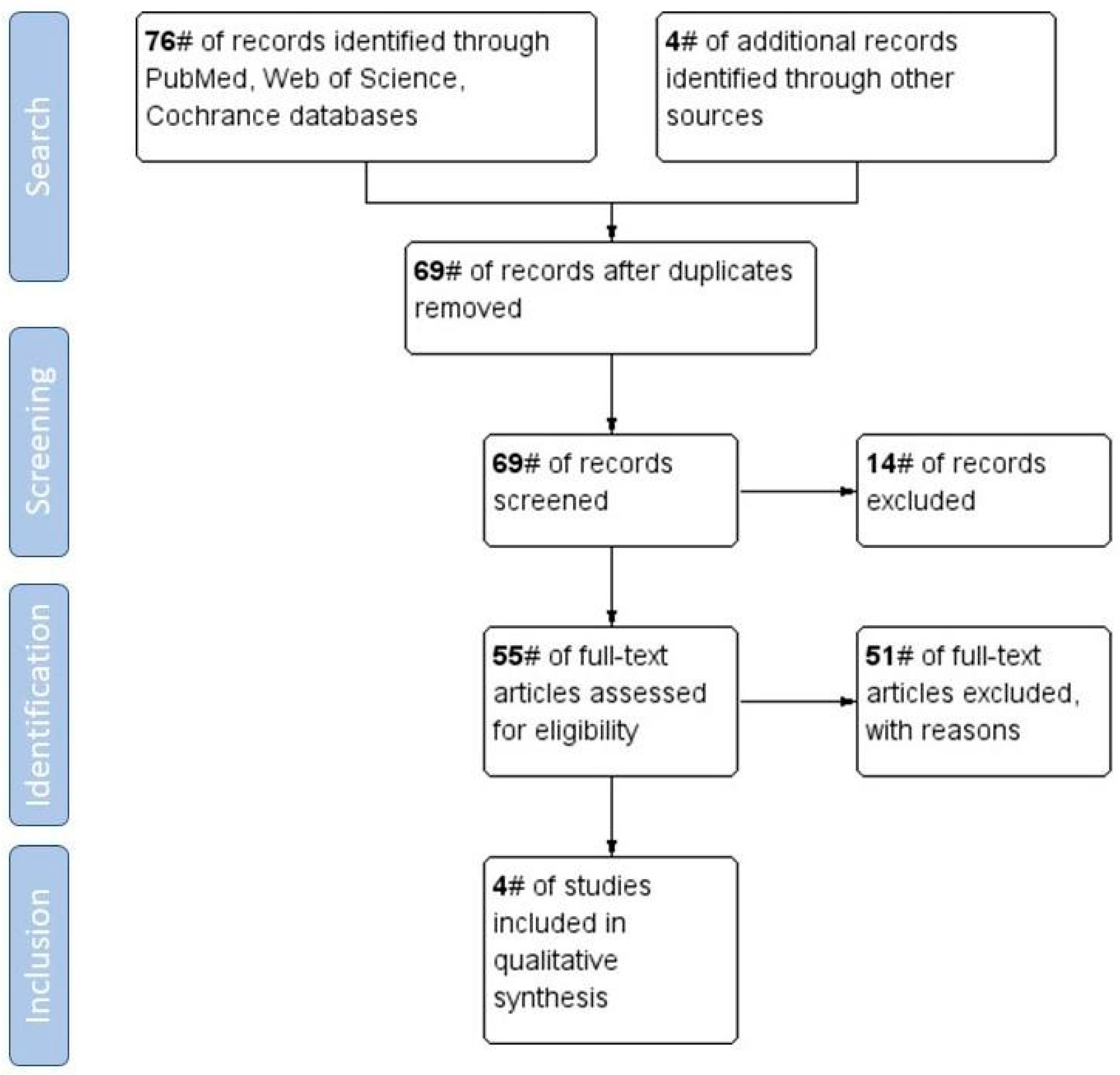
3.1. Search Strategy and Study Selection
3.2. Geographical Distribution of the Included Studies
3.3. Methodological Index for Non-Randomized Studies (MINORS)
3.4. Patient Characteristics
3.5. Patient Outcomes with DMCs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Helmick, C.G.; Felson, D.T.; Lawrence, R.C.; Gabriel, S.; Hirsch, R.; Kwoh, C.K.; Liang, M.H.; Kremers, H.M.; Mayes, M.D.; Merkel, P.A.; et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part I. Arthritis Rheum. 2008, 58, 15–25. [Google Scholar] [CrossRef]
- An, V.V.; Phan, K.; Sivakumar, B.S.; Mobbs, R.J.; Bruce, W.J. Prior Lumbar Spinal Fusion is Associated with an Increased Risk of Dislocation and Revision in Total Hip Arthroplasty: A Meta-Analysis. J. Arthroplast. 2018, 33, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Malkani, A.L.; Himschoot, K.J.; Ong, K.L.; Lau, E.C.; Baykal, D.; Dimar, J.R.; Glassman, S.D.; Berry, D.J. Does Timing of Primary Total Hip Arthroplasty Prior to or After Lumbar Spine Fusion Have an Effect on Dislocation and Revision Rates? J. Arthroplast. 2019, 34, 907–911. [Google Scholar] [CrossRef] [PubMed]
- Barry, J.J.; Sing, D.C.; Vail, T.P.; Hansen, E.N. Early Outcomes of Primary Total Hip Arthroplasty after Prior Lumbar Spinal Fusion. J. Arthroplast. 2017, 32, 470–474. [Google Scholar] [CrossRef] [PubMed]
- Mononen, H.; Sund, R.; Halme, J.; Kröger, H.; Sirola, J. Following total hip arthroplasty: Femoral head component diameter of 32 mm or larger is associated with lower risk of dislocation in patients with a prior lumbar fusion. Bone Jt. J. 2020, 102-B, 1003–1009. [Google Scholar] [CrossRef]
- Dagneaux, L.; Marouby, S.; Maillot, C.; Canovas, F.; Rivière, C. Dual mobility device reduces the risk of prosthetic hip instability for patients with degenerated spine: A case-control study. Orthop. Traumatol. Surg. Res. 2019, 105, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, B.P.; Syku, M.; Sculco, T.P.; Jerabek, S.A.; Mayman, D.J.; Westrich, G.H. Dual-Mobility Constructs in Primary Total Hip Arthroplasty in High-Risk Patients with Spinal Fusions: Our Institutional Experience. Arthroplast. Today 2020, 6, 749–754. [Google Scholar] [CrossRef] [PubMed]
- Malkani, A.L.; Sachdeva, S.; Nessler, J.P.; Westrich, G.; Harwin, S.F.; Mayman, D.; Jerabek, S. Use of dual mobility cups in patients undergoing primary total hip arthroplasty with prior lumbar spine fusion. Int. Orthop. 2020, 44, 857–862. [Google Scholar] [CrossRef]
- Plummer, D.R.; Haughom, B.D.; Della Valle, C.J. Dual mobility in total hip arthroplasty. Orthop. Clin. N. Am. 2014, 45, 1–8. [Google Scholar] [CrossRef]
- De Martino, I.; Triantafyllopoulos, G.K.; Sculco, P.K.; Sculco, T.P. Dual mobility cups in total hip arthroplasty. World J. Orthop. 2014, 5, 180–187. [Google Scholar] [CrossRef]
- Malik, A.; Maheshwari, A.; Dorr, L.D. Impingement with Total Hip Replacement. J. Bone Jt. Surg. 2007, 89, 1832–1842. [Google Scholar] [CrossRef]
- Aguado-Maestro, I.; de Blas-Sanz, I.; Sanz-Peñas, A.E.; Campesino-Nieto, S.V.; Diez-Rodríguez, J.; Valle-López, S.; Espinel-Riol, A.; Fernández-Díez, D.; García-Alonso, M. Dual Mobility Cups as the Routine Choice in Total Hip Arthroplasty. Medicina 2022, 58, 528. [Google Scholar] [CrossRef]
- Huten, D.; Fournier, Y.; Gicquel, T.; Bertho, P.; Basselot, F.; Hamadouche, M. Risk factors for dislocation after revision total hip arthroplasty with a dual-mobility cup. Matched case-control study (16 cases vs. 48 controls). Orthop. Traumatol. Surg. Res. 2019, 105, 1303–1309. [Google Scholar] [CrossRef]
- Assi, C.; Mansour, J.; Prudhon, J.L.; Caton, J.; Yammine, K. Dual-mobility cups could yield lesser infections than conventional cups: A meta-analysis of comparative studies. Int. Orthop. 2021, 45, 1961–1969. [Google Scholar] [CrossRef]
- Schmidt, A.; Batailler, C.; Fary, C.; Servien, E.; Lustig, S. Dual Mobility Cups in Revision Total Hip Arthroplasty: Efficient Strategy to Decrease Dislocation Risk. J. Arthroplast. 2020, 35, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Mohaddes, M.; Cnudde, P.; Rolfson, O.; Wall, A.; Kärrholm, J. Use of dual-mobility cup in revision hip arthroplasty reduces the risk for further dislocation: Analysis of seven hundred and ninety one first-time revisions performed due to dislocation, reported to the Swedish Hip Arthroplasty Register. Int. Orthop. 2017, 41, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Prudhon, J.L.; Desmarchelier, R.; Hamadouche, M.; Delaunay, C.; Verdier, R. Is dual mobility associated with an increased risk of revision for infection? Matched cohort of 231 cases of dual-mobility cups and 231 fixed cups. HIP Int. 2018, 28, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Viricel, C.; Boyer, B.; Philippot, R.; Farizon, F.; Neri, T. Survival and complications of total hip arthroplasty using third-generation dual-mobility cups with non-cross-linked polyethylene liners in patients younger than 55 years. Orthop. Traumatol. Surg. Res. 2022, 108, 103208. [Google Scholar] [CrossRef] [PubMed]
- Patil, N.; Deshmane, P.; Deshmukh, A.; Mow, C. Dual Mobility in Total Hip Arthroplasty: Biomechanics, Indications and Complications–Current Concepts. Indian J. Orthop. 2021, 55, 1202–1207. [Google Scholar] [CrossRef] [PubMed]
- Harwin, S.F.; Sodhi, N.; Ehiorobo, J.; Khlopas, A.; Sultan, A.A.; Mont, M.A. Outcomes of Dual Mobility Acetabular Cups in Total Hip Arthroplasty Patients. Surg. Technol. Int. 2019, 15, 367–370. [Google Scholar]
- Rudy, H.L.; Padilla, J.A.; Gabor, J.A.; Iorio, R.; Schwarzkopf, R.; Vigdorchik, J. Cost-Effectiveness of Dual Mobility and a Value-Based Algorithm of Utilization. Orthop. Clin. N. Am. 2019, 50, 151–158. [Google Scholar] [CrossRef]
- Khoshbin, A.; Haddad, F.S.; Ward, S.; Heireamhoin, S.O.; Wu, J.; Nherera, L.; Atrey, A. A cost-effectiveness assessment of dual-mobility bearings in revision hip arthroplasty. Bone Jt. J. 2020, 102-B, 1128–1135. [Google Scholar] [CrossRef]
- Cochrane. Cochrane Handbook for Systematic Reviews of Interventions, Version 6.1. 2020. Available online: https://training.cochrane.org/handbook/archive/v6.1 (accessed on 23 January 2022).
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (MINORS): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Wright, J.G.; Swiontkowski, M.F.; Heckman, J.D. Introducing levels of evidence to the journal. J. Bone Joint. Surg. Am. 2003, 85, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Bedard, N.A.; Martin, C.T.; Slaven, S.E.; Pugely, A.J.; Mendoza-Lattes, S.A.; Callaghan, J.J. Abnormally High Dislocation Rates of Total Hip Arthroplasty After Spinal Deformity Surgery. J. Arthroplast. 2016, 31, 2884–2885. [Google Scholar] [CrossRef] [PubMed]
- Perfetti, D.C.; Schwarzkopf, R.; Buckland, A.J.; Paulino, C.B.; Vigdorchik, J.M. Prosthetic Dislocation and Revision after Primary Total Hip Arthroplasty in Lumbar Fusion Patients: A Propensity Score Matched-Pair Analysis. J. Arthroplast. 2017, 32, 1635–1640.e1. [Google Scholar] [CrossRef]
- Malkani, A.L.; Garber, A.T.; Ong, K.L.; Dimar, J.R.; Baykal, D.; Glassman, S.D.; Cochran, A.R.; Berry, D.J. Total Hip Arthroplasty in Patients with Previous Lumbar Fusion Surgery: Are There More Dislocations and Revisions? J. Arthroplast. 2018, 33, 1189–1193. [Google Scholar] [CrossRef] [PubMed]
- Bala, A.; Chona, D.V.; Amanatullah, D.F.; Hu, S.S.; Wood, K.B.; Alamin, T.F.; Cheng, I. Timing of Lumbar Spinal Fusion Affects Total Hip Arthroplasty Outcomes. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2019, 3, e00133. [Google Scholar] [CrossRef] [PubMed]
- Legaye, J.; Duval-Beaupère, C.; Hecquet, J.; Marty, C. Pelvic incidence: A fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur. Spine J. 1998, 7, 99–103. [Google Scholar] [CrossRef]
- Roussouly, P.; Pinheiro-Franco, J.L. Biomechanical analysis of the spino-pelvic organization and adaptation in pathology. Eur. Spine J. 2011, 20, 609–618. [Google Scholar] [CrossRef]
- Buckland, A.J.; Burapachaisri, A.; Stekas, N.; Vasquez-Montes, D.; Protopsaltis, T.; Vigdorchik, J. Obesity Alters Spinopelvic Alignment Changes from Standing to Relaxed Sitting: The Influence of the Soft-tissue Envelope. Arthroplast. Today 2020, 6, 590–595.e1. [Google Scholar] [CrossRef]
- Phan, D.; Bederman, S.S.; Schwarzkopf, R. The influence of sagittal spinal deformity on anteversion of the acetabular component in total hip arthroplasty. Bone Jt. J. 2015, 97-B, 1017–1023. [Google Scholar] [CrossRef]
- Lewinnek, G.E.; Lewis, J.L.; Tarr, R.; Compere, C.L.; Zimmerman, J.R. Dislocations after total hip-replacement arthroplasties. J. Bone Jt. Surg. 1978, 60, 217–220. [Google Scholar] [CrossRef]
- Dorr, L.D.; Callaghan, J.J. Death of the Lewinnek “Safe Zone”. J. Arthroplast. 2019, 34, 1–2. [Google Scholar] [CrossRef]
- Blizzard, D.J.; Nickel, B.T.; Seyler, T.M.; Bolognesi, M.P. The Impact of Lumbar Spine Disease and Deformity on Total Hip Arthroplasty Outcomes. Orthop. Clin. N. Am. 2016, 47, 19–28. [Google Scholar] [CrossRef]
- Bolland, B.J.; Whitehouse, S.L.; Timperley, A.J. Indications for Early Hip Revision Surgery in the UK—A Re-Analysis of Njr Data. HIP Int. 2012, 22, 145–152. [Google Scholar] [CrossRef]
- Morrison, A.; Polisena, J.; Husereau, D.; Moulton, K.; Clark, M.; Fiander, M.; Mierzwinski-Urban, M.; Clifford, T.; Hutton, B.; Rabb, D. The effect of English-language restriction on systematic review-based meta-analyses: A systematic review of empirical studies. Int. J. Technol. Assess. Health Care 2012, 28, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Pham, B.; Klassen, T.P.; Lawson, M.L.; Moher, D. Language of publication restrictions in systematic reviews gave different results depending on whether the intervention was conventional or complementary. J. Clin. Epidemiol. 2005, 58, 769–776.e2. [Google Scholar] [CrossRef] [PubMed]
- Cochrane. Cochrane Handbook for Systematic Reviews of Interventions, Version 6. 2019. Available online: https://training.cochrane.org/handbook/archive/v6 (accessed on 23 January 2022).


{kind=link}
| Quality Assessment for Non-Randomized Studies (MINORS) | Mean | SD | MIN | MAX |
|---|---|---|---|---|
| (1) A clearly stated aim | 1.75 | 0.5 | 1 | 2 |
| (2) Inclusion of consecutive patients | 0.75 | 0.95 | 0 | 2 |
| (3) Prospective collection of data | 0 | 0 | 0 | 0 |
| (4) Endpoints appropriate to the aim of the study | 1.75 | 0.5 | 1 | 2 |
| (5) Unbiased assessment of the study endpoint | 1.25 | 0.5 | 1 | 2 |
| (6) Follow-up period appropriate to the aim of the study | 1 | 1.15 | 0 | 2 |
| (7) Loss to follow-up less than 5% | 2 | 0 | 2 | 2 |
| (8) Prospective calculation of the study size | 0 | 0 | 0 | 0 |
| Total for non-comparative (=16) | 8.5 | 3.10 | 5 | 12 |
| (9) An adequate control group | 0.5 | 1 | 0 | 2 |
| (10) Contemporary groups | 0.5 | 1 | 0 | 2 |
| (11) Baseline equivalence analyses | 0.5 | 1 | 0 | 2 |
| (12) Adequate statistical | 0.5 | 1 | 0 | 2 |
| Total (=24) | 10.5 | 5.80 | 5 | 18 |
| Author | Country | Study Design | Level of Evidence | Patient Number | Sex F/M | Use of Robotic THA | Spinal Surgery | Mean Age (Years) | BMI | Follow-Up (Months) |
|---|---|---|---|---|---|---|---|---|---|---|
| Nessler 2020 | USA | Case series | IV | 93 | 56/47 | robotic (65%) | LSF | 66 | 30 | 32.4 |
| Chalmers 2020 | USA | Case series | IV | 80 | 57/23 | robotic (33%) | LSF | 69 | 28 | 36 |
| Dagneaux 2019 | France | Case-control | III | 82 | 49/33 | N/A | DJD or LSF | 70.4 | 26 | N/A |
| Mononen 2020 | Finland | Retrospective | III | 29 | N/A | N/A | LSF or Discectomy | 67.5 | N/A | N/A |
| Author | Acetabular Shell | Acetabular Cup | Type of Dual-Mobility Cup | Acetabular Anteversion | Acetabular Inclination | Dislocation Rate |
|---|---|---|---|---|---|---|
| Nessler 2020 | 44–62 mm | 36–48 mm | 14% ADM 86% MDM | ~20° | ~45° | 0% |
| Chalmers 2020 | 52 (44–62) mm | 42 (36–52) mm | 35% ADM 65% MDM | 24° | 44° | 0% |
| Dagneaux 2019 | N/A | N/A | N/A | N/A | N/A | N/A |
| Mononen 2020 | N/A | 32 mm | N/A | 13° | 46° | 0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Issa, T.Z.; Pearl, A.; Moore, E.; Maqsood, H.A.; Saleh, K.J. Dual-Mobility Cups in Patients Undergoing Primary Total Hip Arthroplasty with Prior Lumbar Spine Fusion: A Systematic Review. Surgeries 2024, 5, 125-134. https://doi.org/10.3390/surgeries5020014
Issa TZ, Pearl A, Moore E, Maqsood HA, Saleh KJ. Dual-Mobility Cups in Patients Undergoing Primary Total Hip Arthroplasty with Prior Lumbar Spine Fusion: A Systematic Review. Surgeries. 2024; 5(2):125-134. https://doi.org/10.3390/surgeries5020014
Chicago/Turabian StyleIssa, Tariq Ziad, Adam Pearl, Emelia Moore, Hannan Ahmad Maqsood, and Khaled J. Saleh. 2024. "Dual-Mobility Cups in Patients Undergoing Primary Total Hip Arthroplasty with Prior Lumbar Spine Fusion: A Systematic Review" Surgeries 5, no. 2: 125-134. https://doi.org/10.3390/surgeries5020014
APA StyleIssa, T. Z., Pearl, A., Moore, E., Maqsood, H. A., & Saleh, K. J. (2024). Dual-Mobility Cups in Patients Undergoing Primary Total Hip Arthroplasty with Prior Lumbar Spine Fusion: A Systematic Review. Surgeries, 5(2), 125-134. https://doi.org/10.3390/surgeries5020014