
Gynecological Health Concerns in Women with Schizophrenia and Related Disorders: A Narrative Review of Recent Studies

 ,
,  ,
, 
 and
and 
Abstract
:1. Introduction
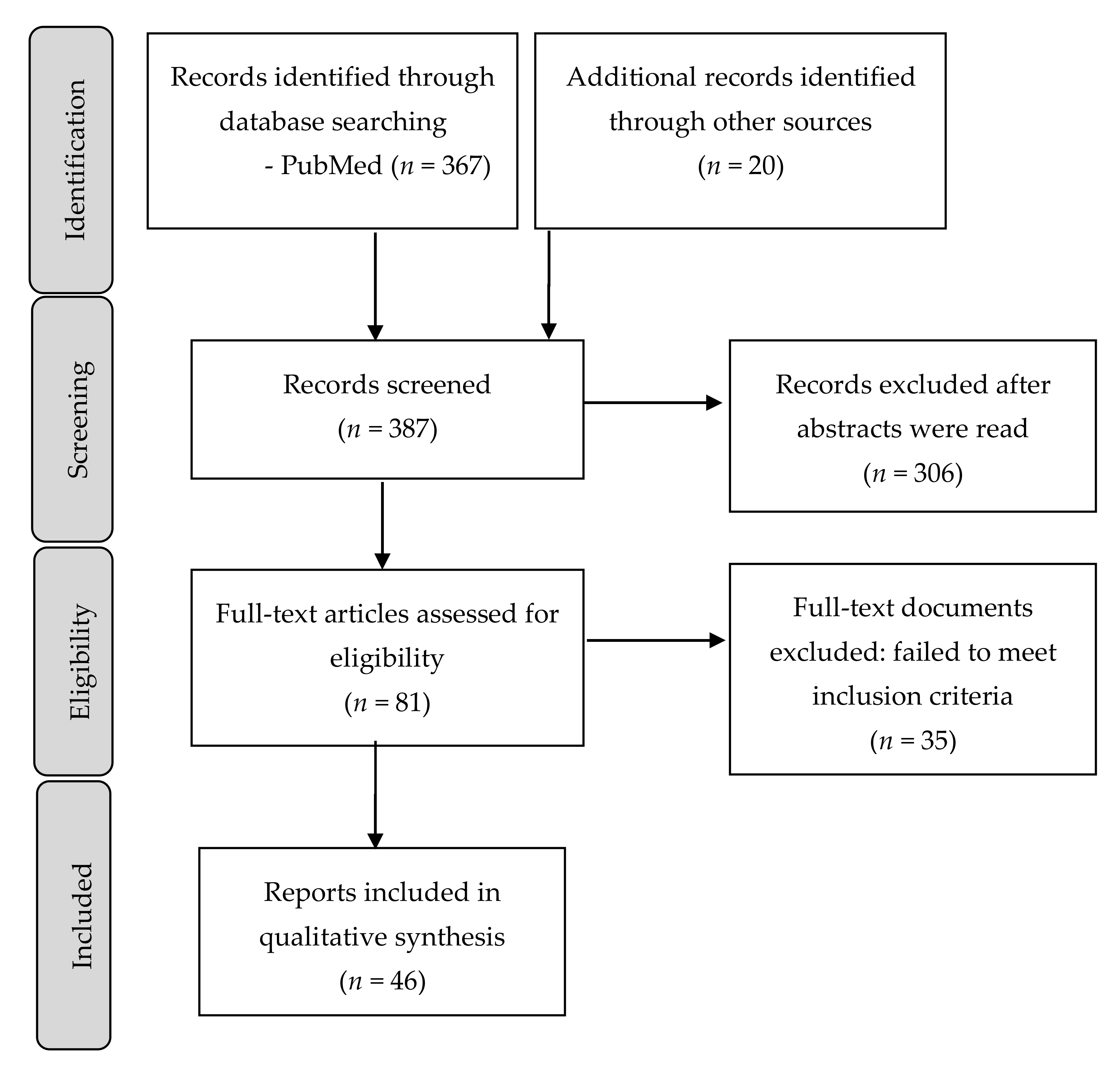
2. Methods
3. Results
3.1. Prevalence of Gynecological Disorders in Women with Schizophrenia and Delusional Disorder
3.2. Risk Factors for Gynecological Disorders in Women with Schizophrenia and Delusional Disorder
- Symptom and stigma-related stress;
- Long term use of prolactin-raising and weight-inducing antipsychotics;
- Nulliparity;
- Relative lack of breastfeeding;
- High rates of smoking;
- Alcohol use;
- Sedentary lifestyle.
3.3. Prevalence of Malignant versus Non-Malignant Gynecological Disease in Schizophrenia and Delusional Disorders
3.4. Cancer Screening and Mortality in Schizophrenia and Delusional Disorder
3.5. Menopause in Women with Schizophrenia and Delusional Disorder and How It Affects Gynecologic Health
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Regitz-Zagrosek, V. Sex and gender differences in health. Science & Society Series on Sex and Science. EMBO Rep. 2012, 13, 596–603. [Google Scholar]
- Jáuregui, B. Biology, Culture and Society, Factors Configuring Health from a Gender Perspective. Has Cardiology Overcome the Challenge? Rev. Esp. Cardiol. 2019, 72, 800–802. [Google Scholar] [CrossRef]
- The Lancet Psychiatry. Sex and gender in psychiatry. Lancet Psychiatry 2016, 3, 999. [Google Scholar] [CrossRef] [Green Version]
- Ochoa, S.; Usall, J.; Cobo, J.; Labad, X.; Kulkarni, J. Gender differences in schizophrenia and first-episode psychosis: A comprehensive literature review. Schizophr. Res. Treatment. 2012, 2012, 916198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Rodríguez, A.; Guàrdia, A.; Monreal, J.A. Peri- and Post-Menopausal Women with Schizophrenia and Related Disorders Are a Population with Specific Needs: A Narrative Review of Current Theories. J. Pers. Med. 2021, 11, 849. [Google Scholar] [CrossRef]
- Seeman, M.V.; González-Rodríguez, A. Stratification by sex and hormone level when contrasting men and women in schizophrenia trials will improve personalized treatment. J. Pers. Med. 2021, 11, 929. [Google Scholar] [CrossRef]
- Szeliga, A.; Stefanowski, B.; Meczekalski, B.; Snopek, M.; Kostrzak, A.; Smolarczyk, R.; Bala, G.; Duszewska, A.; Smolarczyk, K.; Maciejewska-Jeske, M. Menopause in women with schizophrenia, schizoaffective disorder and bipolar disorder. Maturitas 2021, 152, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Barker, M.G. Psychiatric illness after hysterectomy. Br. Med. J. 1968, 2, 91–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gath, D.; Osborn, M.; Bungay, G.; Iles, S.; Day, A.; Bond, A.; Passingham, C. Psychiatric disorder and gynaecological symptoms in middle aged women: A community survey. Br. Med. J. 1987, 294, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Warner, P. Psychiatric disorder and gynaecological symptoms in middle aged women. Br. Med. J. 1987, 294, 1033–1034. [Google Scholar] [CrossRef] [Green Version]
- González-Rodríguez, A.; Seeman, M.V.; Álvarez, A.; Guàrdia, A.; Sanz, N.; Fucho, G.F.; Palao, D.J.; Labad, J. Care for Women with Delusional Disorder: Towards a Specialized Approach. Women 2021, 1, 46–59. [Google Scholar] [CrossRef]
- Mariano, A.; Di Lorenzo, G.; Jannini, T.B.; Santini, R.; Bertinelli, E.; Siracusano, A.; Niolu, C. Medical Comorbidities in 181 Patients with Bipolar Disorder vs. Schizophrenia and Related Psychotic Disorders: Findings from a Single-Center, Retrospective Study From an Acute Inpatients Psychiatric Unit. Front. Psychiatry 2021, 12, 702789. [Google Scholar] [CrossRef]
- Pettersson, D.; Gissler, M.; Hällgren, J.; Ösby, U.; Westman, J.; Bobo, W.V. The overall and sex- and age-group specific incidence rates of cancer in people with schizophrenia: A population-based cohort study. Epidemiol. Psychiatr. Sci. 2020, 29, e132. [Google Scholar] [CrossRef] [PubMed]
- Taipale, H.; Solmi, M.; Lähteenvuo, M.; Tanskanen, A.; Correll, C.U.; Tiihonen, J. Antipsychotic use and risk of breast cancer in women with schizophrenia: A nationwide nested case-control study in Finland. Lancet Psychiatry 2021, 8, 883–891. [Google Scholar] [CrossRef]
- De Hert, M.; Peuskens, J.; Sabbe, T.; Mitchell, A.J.; Stubbs, B.; Neven, P.; Wildiers, H.; Detraux, J. Relationship between prolactin, breast cancer risk, and antipsychotics in patients with schizophrenia: A critical review. Acta Psychiatr. Scand. 2016, 133, 5–22. [Google Scholar] [CrossRef] [PubMed]
- Xiping, Z.; Shuai, Z.; Feijiang, Y.; Bo, C.; Shifeng, Y.; Qihui, C. Meta-analysis of the Correlation Between Schizophrenia and Breast Cancer. Clin. Breast Cancer 2019, 19, e172–e185. [Google Scholar] [CrossRef] [Green Version]
- Zhuo, C.; Triplett, P.T. Association of Schizophrenia with the Risk of Breast Cancer Incidence: A Meta-analysis. JAMA Psychiatry 2018, 75, 363–369. [Google Scholar] [CrossRef]
- Lu, D.; Song, J.; Lu, Y.; Fall, K.; Chen, X.; Fang, F.; Landén, M.; Hultman, C.M.; Czene, K.; Sullivan, P.; et al. A shared genetic contribution to breast cancer and schizophrenia. Nat. Commun. 2020, 11, 4637. [Google Scholar] [CrossRef]
- Lu, D.; Andersson, T.M.; Fall, K.; Hultman, C.M.; Czene, K.; Valdimarsdóttir, U.; Fang, F. Clinical Diagnosis of Mental Disorders Immediately Before and After Cancer Diagnosis: A Nationwide Matched Cohort Study in Sweden. JAMA Oncol. 2016, 2, 1188–1196. [Google Scholar] [CrossRef]
- Si, S.; Li, J.; Tewara, M.A.; Li, H.; Liu, X.; Li, Y.; Chen, X.; Liu, C.; Yuan, T.; Li, W.; et al. Identifying causality, genetic correlation, priority and pathways of large-scale complex exposures of breast and ovarian cancers. Br. J. Cancer. 2021, 125, 1570–1581. [Google Scholar] [CrossRef]
- Shi, J.; Wu, L.; Zheng, W.; Wen, W.; Wang, S.; Shu, X.; Long, J.; Shen, C.Y.; Wu, P.E.; Saloustros, E.; et al. Genetic Evidence for the Association between Schizophrenia and Breast Cancer. J. Psychiatr. Brain. Sci. 2018, 3, 7. [Google Scholar] [PubMed] [Green Version]
- Byrne, E.M.; Ferreira, M.A.R.; Xue, A.; Lindström, S.; Jiang, X.; Yang, J.; Easton, D.F.; Wray, N.R.; Chenevix-Trench, G. Is Schizophrenia a Risk Factor for Breast Cancer?-Evidence From Genetic Data. Schizophr. Bull. 2019, 45, 1251–1256. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, Y.; Tsuji, I.; Mizoue, T.; Inoue, M.; Sawada, N.; Matsuo, K.; Ito, H.; Naito, M.; Nagata, C.; Kitamura, Y.; et al. Cigarette smoking and cervical cancer risk: An evaluation based on a systematic review and meta-analysis among Japanese women. Jpn. J. Clin. Oncol. 2019, 49, 77–86. [Google Scholar] [CrossRef]
- Chen, J.; Bacanu, S.A.; Yu, H.; Zhao, Z.; Jia, P.; Kendler, K.S.; Kranzler, H.R.; Gelernter, J.; Farrer, L.; Minica, C.; et al. Genetic Relationship between Schizophrenia and Nicotine Dependence. Sci. Rep. 2016, 6, 25671. [Google Scholar] [CrossRef] [Green Version]
- Grassi, L.; Caruso, R.; Biancosino, B.; Belvederi Murri, M.; Riba, M.; Meggiolaro, E.; Ruffilli, F.; Palagini, L.; Nanni, M.G.; Zavatta, S.; et al. Knowledge about risk factors for cancer and cancer risk behavior among patients with severe mental illness. Psychooncology 2021, 30, 2077–2081. [Google Scholar] [CrossRef] [PubMed]
- Adams, C.D.; Neuhausen, S.L. Bi-directional Mendelian randomization of epithelial ovarian cancer and schizophrenia and uni-directional Mendelian randomization of schizophrenia on circulating 1- or 2-glycerophosphocholine metabolites. Mol. Genet. Metab. Rep. 2019, 21, 100539. [Google Scholar] [CrossRef]
- Jin, L.; Yu, J.; Chen, Y.; Pang, H.; Sheng, J.; Huang, H. Polycystic Ovary Syndrome and Risk of Five Common Psychiatric Disorders Among European Women: A Two-Sample Mendelian Randomization Study. Front. Genet. 2021, 12, 689897. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Deng, Q.; Stener-Victorin, E. Is there a shared genetic basis and causal relationship between polycystic ovary syndrome and psychiatric disorders: Evidence from a comprehensive genetic analysis. Hum. Reprod. 2021, 36, 2382–2391. [Google Scholar] [CrossRef]
- Chen, S.F.; Yang, Y.C.; Hsu, C.Y.; Shen, Y.C. Risk of schizophrenia in patients with polycystic ovary syndrome: A nationwide population-based cohort study from Taiwan. J. Psychosom. Obstet. Gynaecol. 2021, 42, 272–278. [Google Scholar] [CrossRef]
- Cesta, C.E.; Månsson, M.; Palm, C.; Lichtenstein, P.; Iliadou, A.N.; Landén, M. Polycystic ovary syndrome and psychiatric disorders: Co-morbidity and heritability in a nationwide Swedish cohort. Psychoneuroendocrinology 2016, 73, 196–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douglas, K.M.; Fenton, A.J.; Eggleston, K.; Porter, R.J. Rate of polycystic ovary syndrome in mental health disorders: A systematic review. Arch. Womens Ment. Health 2021. [Google Scholar] [CrossRef]
- Gao, M.; Koupil, I.; Sjöqvist, H.; Karlsson, H.; Lalitkumar, S.; Dalman, C.; Kosidou, K. Psychiatric comorbidity among women with endometriosis: Nationwide cohort study in Sweden. Am. J. Obstet. Gynecol. 2020, 223, 415.e1–415.e16. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.A.; Caraballo-Rivera, E.J.; Isola, S.; Oraka, K.; Akter, S.; Verma, S.; Patel, R.S. Demographics and Hospital Outcomes in American Women with Endometriosis and Psychiatric Comorbidities. Cureus 2020, 12, e9935. [Google Scholar] [CrossRef] [PubMed]
- Delanerolle, G.; Ramakrishnan, R.; Hapangama, D.; Zeng, Y.; Shetty, A.; Elneil, S.; Chong, S.; Hirsch, M.; Oyewole, M.; Phiri, P.; et al. A systematic review and meta-analysis of the Endometriosis and Mental-Health Sequelae; The ELEMI Project. Womens Health 2021, 17, 17455065211019717. [Google Scholar] [CrossRef]
- Solmi, M.; Firth, J.; Miola, A.; Fornaro, M.; Frison, E.; Fusar-Poli, P.; Dragioti, E.; Shin, J.I.; Carvalho, A.F.; Stubbs, B.; et al. Disparities in cancer screening in people with mental illness across the world versus the general population: Prevalence and comparative meta-analysis including 4,717,839 people. Lancet Psychiatry 2020, 7, 52–63. [Google Scholar] [CrossRef]
- González-Rodríguez, A.; Labad, J.; Seeman, M.V. Schizophrenia and cancer. Curr. Opin. Support. Palliat. Care. 2020, 14, 232–238. [Google Scholar] [CrossRef]
- Murphy, K.A.; Daumit, G.L.; McGinty, E.E.; Stone, E.M.; Kennedy-Hendricks, A. Predictors of cancer screening among Black and White Maryland Medicaid enrollees with serious mental illness. Psychooncology 2021, 30, 2092–2098. [Google Scholar] [CrossRef] [PubMed]
- Hwong, A.; Wang, K.; Bent, S.; Mangurian, C. Breast Cancer Screening in Women with Schizophrenia: A Systematic Review and Meta-Analysis. Psychiatr. Serv. 2020, 71, 263–268. [Google Scholar] [CrossRef]
- Woodhead, C.; Cunningham, R.; Ashworth, M.; Barley, E.; Stewart, R.J.; Henderson, M.J. Cervical and breast cancer screening uptake among women with serious mental illness: A data linkage study. BMC Cancer 2016, 16, 819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harder, E.; Thomsen, L.T.; Hertzum-Larsen, R.; Albieri, V.; Hessner, M.V.; Juul, K.E.; Bonde, J.; Frederiksen, K.; Kjaer, S.K. Determinants for Participation in Human Papillomavirus Self-Sampling among Nonattenders to Cervical Cancer Screening in Denmark. Cancer Epidemiol. Biomark. Prev. 2018, 27, 1342–1351. [Google Scholar] [CrossRef] [Green Version]
- Hertzum-Larsen, R.; Kjær, S.K.; Frederiksen, K.; Thomsen, L.T. Participation in cervical cancer screening among immigrants and Danish-born women in Denmark. Prev. Med. 2019, 123, 55–64. [Google Scholar] [CrossRef]
- Tamauchi, S.; Kajiyama, H.; Moriyama, Y.; Yoshihara, M.; Ikeda, Y.; Yoshikawa, N.; Nishino, K.; Niimi, K.; Suzuki, S.; Kikkawa, F. Relationship between preexisting mental disorders and prognosis of gynecologic cancers: A case-control study. J. Obstet. Gynaecol. Res. 2019, 45, 2082–2087. [Google Scholar] [CrossRef]
- Ouk, M.; Edwards, J.D.; Colby-Milley, J.; Kiss, A.; Swardfager, W.; Law, M. Psychiatric morbidity and cervical cancer screening: A retrospective population-based case-cohort study. CMAJ Open 2020, 8, E134–E141. [Google Scholar] [CrossRef] [Green Version]
- Inagaki, M.; Fujiwara, M.; Nakaya, N.; Fujimori, M.; Higuchi, Y.; Hayashibara, C.; So, R.; Kakeda, K.; Kodama, M.; Uchitomi, Y.; et al. Low Cancer Screening Rates among Japanese People with Schizophrenia: A Cross-Sectional Study. Tohoku J. Exp. Med. 2018, 244, 209–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujiwara, M.; Inagaki, M.; Nakaya, N.; Fujimori, M.; Higuchi, Y.; Hayashibara, C.; So, R.; Kakeda, K.; Kodama, M.; Uchitomi, Y.; et al. Cancer screening participation in schizophrenic outpatients and the influence of their functional disability on the screening rate: A cross-sectional study in Japan. Psychiatry Clin. Neurosci. 2017, 71, 813–825. [Google Scholar] [CrossRef]
- Lindamer, L.A.; Buse, D.C.; Auslander, L.; Unützer, J.; Bartels, S.J.; Jeste, D.V. A comparison of gynecological variables and service use among older women with and without schizophrenia. Psychiatr. Serv. 2003, 54, 902–904. [Google Scholar] [CrossRef]
- González-Rodríguez, A.; Molina-Andreu, O.; Penadés Rubio, R.; Catalán Campos, R.; Bernardo Arroyo, M. Reproductive variables and gynaecological service use in delusional disorder outpatients. Rev. Psiquiatr. Salud. Ment. 2015, 8, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Ni, L.; Wu, J.; Long, Y.; Tao, J.; Xu, J.; Yuan, X.; Yu, N.; Wu, R.; Zhang, Y. Mortality of site-specific cancer in patients with schizophrenia: A systematic review and meta-analysis. BMC Psychiatry 2019, 19, 323. [Google Scholar] [CrossRef] [Green Version]
- Lawrence, W.R.; Kuliszewski, M.G.; Hosler, A.S.; Leinung, M.C.; Zhang, X.; Zhang, W.; Du, Z.; Schymura, M.J.; Boscoe, F.P. Association between preexisting mental illnesses and mortality among medicaid-insured women diagnosed with breast cancer. Soc. Sci. Med. 2021, 270, 113643. [Google Scholar] [CrossRef]
- Dalton, S.O.; Suppli, N.P.; Ewertz, M.; Kroman, N.; Grassi, L.; Johansen, C. Impact of schizophrenia and related disorders on mortality from breast cancer: A population-based cohort study in Denmark, 1995–2011. Breast 2018, 40, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Iglay, K.; Santorelli, M.L.; Hirshfield, K.M.; Williams, J.M.; Rhoads, G.G.; Lin, Y.; Demissie, K. Impact of Preexisting Mental Illness on All-Cause and Breast Cancer-Specific Mortality in Elderly Patients with Breast Cancer. J. Clin. Oncol. 2017, 35, 4012–4018. [Google Scholar] [CrossRef]
- Konishi, T.; Fujiogi, M.; Michihata, N.; Tanaka-Mizutani, H.; Morita, K.; Matsui, H.; Fushimi, K.; Tanabe, M.; Seto, Y.; Yasunaga, H. Breast cancer surgery in patients with schizophrenia: Short-term outcomes from a nationwide cohort. Br. J. Surg. 2021, 108, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Fond, G.; Pauly, V.; Duba, A.; Salas, S.; Viprey, M.; Baumstarck, K.; Orleans, V.; Llorca, P.M.; Lancon, C.; Auquier, P.; et al. End of life breast cancer care in women with severe mental illnesses. Sci. Rep. 2021, 11, 10167. [Google Scholar] [CrossRef]
- Haskins, C.B.; McDowell, B.D.; Carnahan, R.M.; Fiedorowicz, J.G.; Wallace, R.B.; Smith, B.J.; Chrischilles, E.A. Impact of preexisting mental illness on breast cancer endocrine therapy adherence. Breast. Cancer Res. Treat. 2019, 174, 197–208. [Google Scholar] [CrossRef]
- Irwin, K.E.; Park, E.R.; Shin, J.A.; Fields, L.E.; Jacobs, J.M.; Greer, J.A.; Taylor, J.B.; Taghian, A.G.; Freudenreich, O.; Ryan, D.P.; et al. Predictors of disruptions in breast cancer care for individuals with schizophrenia. Oncologist 2017, 22, 1374–1382. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.-J.; Lin, C.-H.; Lane, H.-Y. From menopause to neurodegeneration—molecular basis and potential therapy. Int. J. Mol. Sci. 2021, 22, 8654. [Google Scholar] [CrossRef] [PubMed]
- Taipale, H.; Mittendorfer-Rutz, E.; Alexanderson, K.; Majak, M.; Mehtälä, J.; Hoti, F.; Jedenius, E.; Enkusson, D.; Leval, A.; Sermon, J.; et al. Antipsychotics and mortality in a nationwide cohort of 29,823 patients with schizophrenia. Schizophr. Res. 2018, 197, 274–280. [Google Scholar] [CrossRef]
- Irwin, K.E.; Park, E.R.; Fields, L.E.; Corveleyn, A.E.; Greer, J.A.; Perez, G.K.; Callaway, C.A.; Jacobs, J.M.; Nierenberg, A.A.; Temel, J.S.; et al. Bridge: Person-Centered Collaborative Care for Patients with Serious Mental Illness and Cancer. Oncologist 2019, 24, 901–910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Rodríguez, A.; Guàrdia, A.; Álvarez Pedrero, A.; Betriu, M.; Cobo, J.; Acebillo, S.; Monreal, J.A.; Seeman, M.V.; Palao, D.; Labad, J. Women with schizophrenia over the life span: Health promotion, treatment and outcomes. Int. J. Environ. Res. Public Health 2020, 17, 5594. [Google Scholar] [CrossRef]


{kind=link}
| Gynecological Cancer | Findings | Reference |
|---|---|---|
| Breast cancer | Higher incidence compared to the general population. | [13,16,17] |
| Exposure for 5 or more years to prolactin-raising drugs associated with increased incidence. | [14] | |
| Other risk factors contribute to the risks: obesity, alcohol use, smoking, diabetes mellitus, stress. | [15] | |
| Cervical cancer | Smoking is associated with schizophrenia and risk for cervical cancer. | [24,25] |
| Ovarian cancer | Schizophrenia associated with weakly increased risk for epithelial ovarian cancer. | [26] |
| Overall gynecological cancers | Genetic and lifestyle factors associated with increased risk: weight gain, metabolic syndrome. | [23,24] |
| Cancer Type | Findings | References |
|---|---|---|
| Overall Cancer Screening | Cancer screening rates are lower in patients with severe mental illness compared to the general population | [35] |
| Primary care use and long duration of Medicaid enrolment were associated with higher cancer screening rates | [37] | |
| Comorbid substance use disorders were associated with lower rates of cancer screening | [37] | |
| Gynecological cancers | Women with schizophrenia were less likely to receive breast and cervical cancer screening | [39] |
| The frequency of primary care visits influences cancer screening | [40] | |
| Breast cancer | Women with schizophrenia and delusional disorders were less likely to receive mammography | [38,39] |
| Cervical cancer | Low income, smoking, obesity, schizophrenia, and substance use disorders were associated with low participation in cancer screening | [41] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Rodríguez, A.; Seeman, M.V.; Guàrdia, A.; Natividad, M.; Marín, M.; Labad, J.; Monreal, J.A. Gynecological Health Concerns in Women with Schizophrenia and Related Disorders: A Narrative Review of Recent Studies. Women 2022, 2, 1-14. https://doi.org/10.3390/women2010001
González-Rodríguez A, Seeman MV, Guàrdia A, Natividad M, Marín M, Labad J, Monreal JA. Gynecological Health Concerns in Women with Schizophrenia and Related Disorders: A Narrative Review of Recent Studies. Women. 2022; 2(1):1-14. https://doi.org/10.3390/women2010001
Chicago/Turabian StyleGonzález-Rodríguez, Alexandre, Mary V. Seeman, Armand Guàrdia, Mentxu Natividad, Marta Marín, Javier Labad, and José Antonio Monreal. 2022. "Gynecological Health Concerns in Women with Schizophrenia and Related Disorders: A Narrative Review of Recent Studies" Women 2, no. 1: 1-14. https://doi.org/10.3390/women2010001
APA StyleGonzález-Rodríguez, A., Seeman, M. V., Guàrdia, A., Natividad, M., Marín, M., Labad, J., & Monreal, J. A. (2022). Gynecological Health Concerns in Women with Schizophrenia and Related Disorders: A Narrative Review of Recent Studies. Women, 2(1), 1-14. https://doi.org/10.3390/women2010001