Abstract
Bladder cancer (BCa) is the fourth most common cancer in men and one of the most common urinary tract cancers, especially in developed countries. The aim of this paper is to comprehensively analyze the biology of bladder cancer, including its epidemiology, etiology, histological types, risk factors, clinical symptoms, and diagnostic methods. The paper presents the dominant histological types of bladder cancer, such as transitional cell carcinoma (TCC), which accounts for 90–95% of cases, squamous cell carcinoma (SCC), and adenocarcinoma, which is much rarer. Risk factors, such as smoking, occupational exposure to chemicals, schistosomiasis, and genetic factors, which significantly affect the pathogenesis of bladder cancer, are also discussed. The paper focuses on modern diagnostic methods, including blue light cystoscopy (BLC) and computed tomography urography (CTU), which show increased sensitivity and specificity in detecting early neoplastic changes. The importance of TNM classification and the role of neoadjuvant chemotherapy in improving patient prognosis are also discussed. Based on a review of the scientific literature, the paper emphasizes the need for early diagnosis and an individualized therapeutic approach, which may contribute to improving the survival and quality of life of patients with bladder cancer. The potential for prevention, including quitting smoking and limiting exposure to harmful chemicals, has also been demonstrated to significantly reduce the risk of disease. Patient education and monitoring high-risk groups are key to reducing the incidence of bladder cancer.
Keywords:
bladder cancer; cancer biology; risk factors; clinical symptoms; diagnostic materials; clinical trials; diagnosis; treatment; prognosis; urological tumors; urine cytology; cystoscopy; biopsy; immunohistochemistry; molecular studies; tumor markers; TCC (transitional cell carcinoma); MIBC (muscle-invasive bladder cancer); NMIBC (non-muscle-invasive bladder cancer) 1. Introduction
Bladder cancer (BCa) is the most common cancer of the urinary system and is one of the most common cancers worldwide [1]. This common cancer affects both women and men, being the fourth most common cancer in men [2] after prostate cancer, lung cancer, and colon cancer [3]. Morbidity and mortality associated with bladder cancer vary geographically, which is a result of differences in the occurrence of risk factors for this disease, mainly related to tobacco smoking (Table 1) [4]. Bladder cancer is diagnosed mainly in men over 45 years of age (98% of cases). The highest incidence is observed in the age group of 80–84 years [5].

Table 1.
Bladder cancer incidence and mortality in 2022: top 10 countries.
At the time of diagnosis, in about 75–85% of patients, the cancer is limited to the urinary bladder. In the remaining 15–25%, the disease is diagnosed at the stage with distant metastases. Bladder cancer has a significantly higher incidence in geographical regions such as Europe, North America, and Australia, compared to lower incidence observed in Asia and Africa [6,7]. Currently, there is a downward trend in the incidence of this disease in highly developed countries [8]. It ranks 10th in the global ranking of cancers in terms of incidence, and data from 2021 indicated that approximately 573,000 new cases and 213,000 deaths were recorded [9]. It is worth noting that as many as 75% of cases are non-muscle-invasive bladder cancer (NMIBC), while the rest are classified as muscle-invasive bladder cancer (MIBC) [10]. These are significant data that emphasize the importance of monitoring, prevention, and effective treatment of this disease, which has a major impact on the world’s population. According to the World Cancer Research Fund International (WCRF), more than 614,298 new cases of bladder cancer were detected worldwide in 2022. Spain had the highest overall case rate, followed by Italy. Egypt had the highest overall case fatality rate, followed by Burkina Faso. The ten countries with the highest case rates and the highest number of deaths from bladder cancer in 2022 are shown in Table 1 below.
Statistics from the National Cancer Registry show that the incidence of bladder cancer in Poland has been increasing in both women and men over the years. In 2021, 7043 cases were detected, which means an increase of 543 cases compared to 2020 (Figure 1). Figure 1 shows the incidence of bladder cancer in Poland in 2011–2021. In the period from 2011 to 2018, a gradual increase in the number of new cases was observed, followed by a significant decrease in 2019–2020, and a renewed increase in 2021. The analyzed decrease in incidence in 2020 may be the result of the impact of the COVID-19 pandemic on the functioning of the healthcare system, including the diagnosis of neoplastic diseases. The COVID-19 pandemic has significantly disrupted access to medical services around the world, including in Poland. The introduction of numerous restrictions on the activities of medical facilities, resulting from the need to redirect healthcare system resources to combat the pandemic, could have significantly affected the reduction in the number of diagnostic tests performed, such as cystoscopy or imaging tests, which are key in the diagnosis of bladder cancer. In addition, restrictions to the availability of specialist consultations, including oncological ones, could have led to delays in the diagnosis of new cancer cases. The increase in the number of diagnosed bladder cancer cases in 2021 can be interpreted as a result of delayed diagnostics resulting from restrictions from the previous year. Patients who were unable to undergo appropriate tests in 2020 could only receive a diagnosis later, which contributed to the increase in the number of cases in 2021. Therefore, the observed decrease in incidence in 2020 does not reflect an actual decrease in the number of cases but may be the result of limited access to diagnostics and treatment as a result of the COVID-19 pandemic.
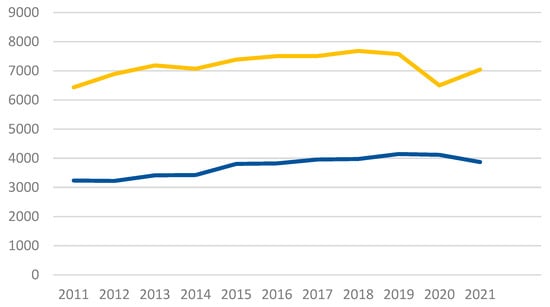
Figure 1.
Bladder cancer incidence (yellow line) and mortality (blue line) in Poland in both sexes.
Available data show that the mortality rate associated with bladder cancer in Poland is showing a tendency to stabilize at a relatively constant level. Although this relative stability is observed, one cannot ignore the fact that there is still a high percentage of deaths among people affected by this disease, as evidenced by data from 2021, where the mortality rate was 54.9%.
1.1. Anatomy of the Urinary Bladder
The urinary bladder is a flexible, hollow organ in the pelvic cavity that stores urine delivered by the ureters (Figure 2). When empty, it is located behind the pubic symphysis, and when filled, it rises into the abdominal cavity [11]. It has four surfaces: a superior, posterior (bladder floor), and two inferolateral surfaces. The apex of the bladder is connected to the umbilicus by the median umbilical ligament, and the lowest part, the bladder neck, contains the internal urethral opening [12]. In men, the bladder neck is located above the prostate, while in women it is connected to the pelvic floor [13]. The superior surface of the bladder is covered by the peritoneum, which in men forms the rectovesical pouch and in women extends to the isthmus of the uterus [14]. The bladder wall consists of four layers: the urothelium, the lamina propria, the detrusor muscle, and the serosa [15]. The urothelium forms an impermeable protective layer, and the detrusor muscle is responsible for bladder contraction [16].
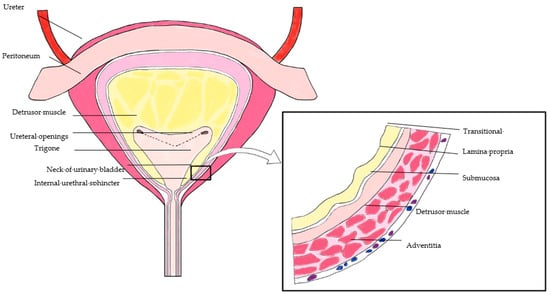
Figure 2.
Anatomy of the urinary bladder.
1.2. Physiology of the Urinary Bladder
The urinary bladder is responsible for storing and excreting urine, which is possible thanks to the flexible walls that allow it to stretch as it fills [17]. This process occurs in two phases: storage and emptying. In the storage phase, the detrusor muscle remains relaxed, and the urethral sphincters are closed, which prevents urine leakage. The capacity of the bladder is approximately 300–500 mL in adults [18]. The emptying phase, or micturition, is initiated when the bladder reaches the appropriate capacity, which causes the detrusor muscle to contract and the urethral sphincters to relax, allowing urine to be excreted [19]. The regulation of bladder function is achieved by the nervous system. The parasympathetic system, via acetylcholine, stimulates the contraction of the detrusor muscle, while the sympathetic system, via noradrenaline, inhibits its contraction and stimulates the contraction of the sphincters, allowing urine to be retained [20]. The somatic nervous system controls the external urethral sphincter, allowing for conscious control over micturition [21]. In a randomized phase III trial published in 2021, the efficacy of dose-dense MVAC (methotrexate, vinblastine, doxorubicin, and cisplatin) was compared to gemcitabine and cisplatin (GC) in the perioperative treatment of muscle-invasive bladder cancer (MIBC). A total of 437 patients received neoadjuvant chemotherapy, with 218 treated with dd-MVAC and 219 with GC. While the complete pathological response rate (ypT0N0) was higher in the dd-MVAC group (42% vs. 36%), this difference was not statistically significant (p = 0.2). However, dd-MVAC achieved a significantly higher rate of organ-confined disease (<ypT3N0) at 77%, compared to 63% for GC (p = 0.001), suggesting improved local tumor control. Toxicity profiles were similar in terms of hematological side effects, but dd-MVAC was associated with more frequent grade ≥3 gastrointestinal toxicities (p = 0.003) and asthenia (p < 0.001). Although dd-MVAC showed promising local control and tumor downstaging, progression-free survival data, expected in future analyses, are necessary to confirm these results. The final assessment will be critical in determining the superiority of dd-MVAC over GC in the perioperative setting for MIBC [21]. In addition to traditional diagnostic methods, such as cystoscopy, bladder cancer is now diagnosed using modern technologies, such as blue light cystoscopy (BLC) and computed tomography urography (CTU), which increase sensitivity and specificity in detecting neoplastic lesions. In addition, new treatment protocols, such as neoadjuvant chemotherapy, play a key role in improving patient outcomes, especially in cases of advanced invasive cancer. These technologies can contribute to significantly prolonging patient survival through early detection of lesions and an individualized approach to therapy.
2. Materials and Methods
The aim of this work was to thoroughly analyze available research on the biology of bladder cancer, taking into account risk factors, clinical symptoms, diagnostic materials, and available clinical trials. The analysis was aimed at identifying key aspects of the disease that may be important in the diagnosis, treatment, and prognosis of bladder cancer. In order to ensure the reliability and completeness of the analysis, a review of scientific literature available in databases, such as PubMed, Scopus, Research Gate, and Google Scholar, was conducted. The search was performed using the following keywords: “bladder cancer”, “cancer biology”, “risk factors”, “clinical features”, “diagnostic materials”, “clinical studies”, “diagnostics”, “treatment”, “prognosis”, “urological neoplasms”, “urine cytology”, “cystoscopy”, “biopsy”, “immunohistochemistry”, “molecular studies”, “tumor markers”, “TCC (transitional cell carcinoma)”, “MIBC (muscle-invasive bladder cancer)”, and “NMIBC (non-muscle-invasive bladder cancer)”.
2.1. Inclusion Criteria
Studies published in peer-reviewed journals that contained complete data on clinical, diagnostic, and therapeutic aspects of bladder cancer were included in the review. Only studies in the adult population (≥18 years) that provided complete methodological information, such as sample size, data collection, analysis methods, and study results, were included.
2.2. Exclusion Criteria
Incomplete text articles, such as conference abstracts and studies on cancers other than bladder cancer, were excluded. In addition, studies that did not provide complete data on methodology and outcomes were excluded from the review, in particular those that did not provide clear criteria for patient selection, diagnostic methods used, and assessment of treatment outcomes.
In addition, the following studies were excluded:
- Those that were focused on the same agents or therapies to avoid overemphasis on one method at the expense of others.
- Those that were stopped prematurely for various reasons, such as methodological difficulties or problems with patient recruitment.
- Those that did not produce significant results, i.e., did not show that the agents or therapies studied had an effect on the development, treatment, or prognosis of bladder cancer.
2.3. Selection Process
The literature selection process was conducted in several stages. Initially, databases were searched using a combination of the above-mentioned keywords. The results were filtered for full texts and publications based on clinical and experimental studies. Each article was then assessed for its methodological quality, the research methods used, and their relevance to the field of bladder cancer. Studies using a variety of diagnostic techniques were analyzed, including cystoscopy, molecular testing, immunohistochemistry, biopsies, and urine cytology. The results of the analyzed studies were presented in tables to facilitate comparison between different clinical and diagnostic approaches. Each study was assessed for its methodological quality, including sample size, data collection method, and statistical methods used to analyze the results. The results of the literature review allowed for the identification of key factors influencing the development, diagnosis, and treatment of bladder cancer.
3. Results
3.1. Types of Bladder Cancer
3.1.1. Transitional Cell Carcinoma
Transitional cell carcinoma (TCC), also known as urothelial carcinoma, accounts for over 90% of bladder cancer cases (Table 2) [22]. Figure 3, Figure 4 and Figure 5 presents examples of urothelial carcinoma. At diagnosis, approximately 70–85% of TCC cases are superficial (stages Ta, T1, and carcinoma in situ (CIS)) and are currently classified as non-muscle-invasive bladder cancer (NMIBC) [23]. In England and Wales, unlike in Europe or the USA, non-muscle-invasive tumors that do not penetrate the lamina propria (Ta and CIS) are not included in cancer registry statistics, leading to differences in the interpretation of epidemiological data worldwide [24]. Exclusion of muscle invasion is a key element in the diagnosis of bladder cancer, as the prognosis for patients with invasive TCC (T2–T4) is poor, with almost half of patients dying within five years of diagnosis [25]. In the Middle East and Africa, squamous cell carcinoma was previously more common, mainly due to Schistosoma haematobium infections [26]. However, with the increasing knowledge of schistosomiasis over the last three decades, the number of cases of this type of cancer has decreased significantly, resulting in TCC becoming the dominant type of bladder cancer in these regions as well [27].
Table 2.
Features of transitional cell carcinoma of the urinary bladder.
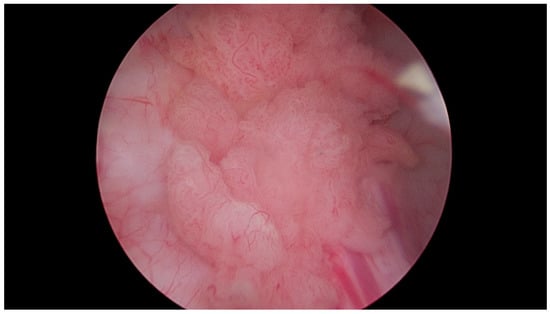
Figure 3.
Papillary urothelial carcinoma of the urinary bladder. Own study based on Ethical Approval of the University of Rzeszow, No. 29/05/2019. Titled 12. 2019, Evaluation of the efficacy of the in vitro photodynamic method in superficial bladder cancer, by M.D. Dominik Godlewski.
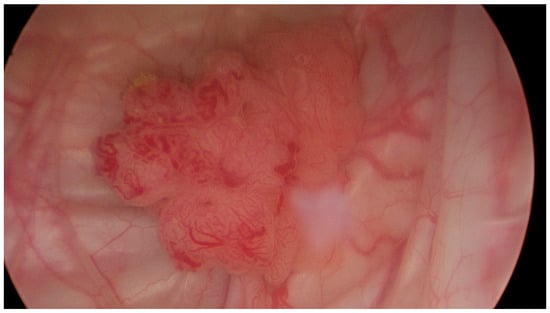
Figure 4.
Papillary urothelial carcinoma of the urinary bladder—visible pathological vascularization within the exophytic part of the tumor, as well as at its base. Own study based on Ethical Approval of the University of Rzeszow, No. 29/05/2019. Titled 12. 2019, Evaluation of the efficacy of the in vitro photodynamic method in superficial bladder cancer, by M.D. Dominik Godlewski.
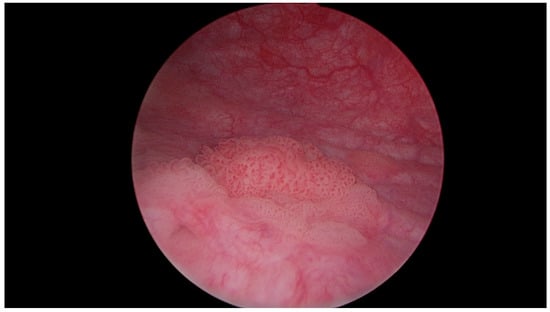
Figure 5.
Multiple papillary urothelial carcinoma of the urinary bladder—in the lower part of the image, at 8 o’clock, the vesical orifice of the right ureter is visible. Own study based on Ethical Approval of the University of Rzeszow, No. 29/05/2019. Titled 12. 2019, Evaluation of the efficacy of the in vitro photodynamic method in superficial bladder cancer, by M.D. Dominik Godlewski.
3.1.2. Squamous Cell Carcinoma
Squamous cell carcinoma (SCC) is the second most common malignancy, accounting for approximately 2–5% of all cases [28]. It can be divided into two major subtypes: SCC associated with schistosomiasis, referred to as B-SCC, and SCC not associated with bilharzia, referred to as NB-SCC (Table 3). The two subtypes differ in their epidemiology, natural history, and clinicopathologic features [29]. B-SCC is most common in regions endemic to schistosomiasis, such as the Middle East, Southeast Asia, and South America [30]. In the United States, NB-SCC is reported primarily in patients with spinal cord injury, particularly after long-term use of an indwelling catheter [31,32]. NB-SCC is usually diagnosed at a late stage, which is associated with a poor prognosis. Both B-SCC and NB-SCC are treated with radical cystectomy (RC); however, the efficacy of other treatment modalities, including neoadjuvant and adjuvant therapies in combination with RC, is not well documented.
Table 3.
Comparison of B-SCC and NB-SCC bladder SCC.
3.1.3. Adenocarcinoma
Primary bladder adenocarcinoma is a rare tumor that poses diagnostic challenges, especially when distinguished from adenocarcinomas of adjacent organs, such as the large intestine. It is characterized by a variable histological appearance and degree of differentiation. Bladder adenocarcinoma, originating from the urothelial lining, accounts for 0.5% to 2.0% of all malignant bladder tumors [33]. Histologically, it is divided into intestinal, indeterminate, mucinous, signet ring cell, clear cell, hepatoid, and mixed types [34]. It is often accompanied by changes, such as cystic and glandular cystitis or superficial glandular metaplasia. Molecular studies suggest that intestinal metaplasia may be a precursor lesion for adenocarcinoma. Adenocarcinomas constitute about 90% of tumors in the exstrophic bladder and are more common in schistosomiasis (Table 4). These tumors can arise anywhere in the bladder but most commonly involve the trigone and posterior wall. Approximately two-thirds of cases are solitary lesions, as opposed to multifocal urothelial carcinomas [35].
Table 4.
Features of bladder adenocarcinoma.
3.1.4. Sarcoma
Primary bladder carcinosarcoma is a rare and highly aggressive tumor, accounting for less than 1% of all bladder tumors (Table 5). There are no specific treatment guidelines for bladder carcinosarcoma, and most published cases are treated with surgery alone [36].
Table 5.
Features of bladder carcinosarcoma.
3.1.5. Small Cell Carcinoma
Small cell carcinoma (SCC) of the genitourinary (GU) system is a rare malignancy with high metastatic potential. The most common primary sites are the urinary bladder and prostate, but there are also reports of primary SCC in the kidney, ureter, and urethra (Table 6). SCC of the urinary bladder presents with lymph node involvement or metastases in most cases. Emerging data suggest that small cell carcinoma of the bladder and prostate develop from a common progenitor of conventional urothelial bladder carcinoma and prostatic adenocarcinoma [37].
Table 6.
Features of small cell bladder cancer.
3.2. Risk Factors
One of the most important factors of morbidity is the age of patients. According to the United Nations, the world population is expected to increase from its current level to 8.5 billion in 2030, and then exceed 9.7 billion in 2050. Currently, people over 60 years of age constitute about 13% of the world’s population, with Europe accounting for as much as 25% and, for comparison, only 5% in Africa. The data allow us to estimate that half of the increase in the global population will be reflected in the increase in the number of people over 60 years of age, which will increase from 960 million to 1.4 billion by 2030 and to 2.1 billion by 2050. These demographic changes will have a significant impact on the incidence of bladder cancer (as well as other late-onset diseases), which will consequently increase its incidence and mortality [38]. Another highly correlated risk factor associated with bladder cancer incidence is tobacco smoking. Data indicate that the risk of bladder cancer incidence associated with smoking is close to 50%. Hence, changes in the incidence of tobacco smoking will have a significant impact on the incidence of UBC, although with a delay of several decades [39]. A study of 52 analyses showed that the risk of bladder cancer increased proportionally with the intensity of smoking up to 20 cigarettes per day (risk ratio (RR): 2.52, 95% confidence interval (CI): 2.41–2.64 for 10 cigarettes per day, and RR: 3.27, 95% CI: 3.16–3.38 for 20 cigarettes per day), after which it did not increase and reached a plateau phase. However, the risk increased without reaching a plateau with the increasing duration of smoking. In other words, the chance of developing bladder cancer increased with the increasing duration of smoking [40]. Studies show that in countries with a lower level of social development, the percentage of smokers is higher than in more developed countries. However, it is worth noting that since 2015, the increasing number of people addicted to tobacco has started to slow down, and this is largely related to the policies of many countries. By conducting anti-smoking programs in more developed countries, a significant decrease in the number of people suffering from bladder cancer is expected, which cannot be said about less developed countries, where smoking tobacco products is still a huge problem and will probably contribute to a large extent to the growing number of cases of this cancer [41].
3.2.1. Opium and Its Role in Bladder Cancer
According to a 2020 study, opium use is positively correlated with the incidence of bladder cancer. A prospective cohort study was described, including 50,000 patients with a median follow-up of 10 years. It was found that people who had ever used opium—through smoking or other forms of dosing—showed a greater tendency to develop cancer than those who had never used this substance [42].
3.2.2. Occupational Exposure to Carcinogens
In countries with high industrial development, occupational exposure to carcinogens is a 5.7% risk factor for bladder cancer [43]. One of the professional groups exposed to large amounts of carcinogens, including sulfur dioxide, benzene, and ethylbenzene, is firefighters. All of these compounds are present in the smoke that firefighters involuntarily inhale during many interventions. A 2019 article proved that this professional group is at higher risk of developing cancer, including bladder cancer [44].
3.2.3. Potential Carcinogens in Daily Life
There are many studies on substances we come into contact with daily that have potential carcinogenic effects, but the results of these studies do not allow for a clear determination of their significant impact on cancer development. One of these substances is arsenic, which is present in drinking water. Although there is evidence supporting the thesis that high levels of arsenic in drinking water are positively correlated with the risk of bladder cancer, the concentration present in natural conditions in most places in the world does not show a significant increase in morbidity risk with increasing arsenic doses (by 10 mg/L), suggesting that its concentration is carcinogenic only at high levels [45]. Other substances whose concentration in drinking water did not show significant relationships between their content and the incidence of bladder cancer are nitrates and trihalomethanes [46].
3.2.4. Diet and Bladder Cancer Risk
Diet plays a significant role in bladder cancer risk. One of its key components is caffeine, as proven in 2020 when a pooled analysis of 12 cohorts, covering 501,604 patients, was conducted. It indicated an increased risk of bladder cancer with coffee consumption exceeding 500 mL per day (HR: 1.56, 95% CI: 1.38–1.77) and in the range of 180–500 mL per day (HR: 1.39, 95% CI: 1.23–1.58) compared to non-coffee drinkers. However, when the results were analyzed by gender and smoking status, it was found that this association occurred mainly among smoking men, suggesting the possibility of a residual confounding factor related to smoking [47]. As for alcohol consumption, studies conducted on the Japanese population have shown that high alcohol intake (more than 30 g of ethanol per day) significantly increases the risk of developing bladder cancer compared to those with moderate alcohol consumption (≤30 g of ethanol per day) [48]. In the case of vitamins, an increased risk of bladder cancer was found in people with excessive consumption of vitamin B1 (HR: 1.14, 95% CI: 1.01–1.29) compared to those with lower intake. However, this association was detected only in male subjects [49].
3.2.5. Protective Dietary Factors
In addition to dietary substances that increase the risk of bladder cancer, there are also those that reduce this risk. One of them is tea, as evidenced in 2022, when an article was published describing that higher tea consumption was associated with a reduced risk of bladder cancer in a pooled analysis of 12 cohort studies (HR: 0.84, 95% CI: 0.75–0.95 for high consumption). However, subgroup analysis did not show an association in women and never smokers, suggesting that this effect could be modulated by carcinogenic substances in tobacco [50]. Cow’s milk and dairy products also modulate bladder cancer risk in a favorable way. Studies conducted in Sweden in 2008 demonstrated a 38% risk reduction with the consumption of milk containing high levels of beneficial bacteria [51]. Moreover, in 2020, it was proven that moderate yogurt consumption reduces the incidence of bladder cancer (HR: 0.85, 95% CI: 0.75–0.96) [52]. Whole grain products have also been found to reduce bladder cancer risk. This was confirmed by a 2020 article that collected 13 cohort studies covering about 575,000 patients, which demonstrated a reduced risk of bladder cancer with higher consumption of whole grains (HR for the highest vs. lowest tertile: 0.87, 95% CI: 0.77–0.98). Similar results were also achieved for dietary fiber [53].
3.2.6. Genetic Factors and Bladder Cancer
Genetic factors play an important role in the development of bladder cancer. As previously mentioned, epidemiological studies have shown an association between cigarette smoking and the risk of urothelial cancer. Tobacco carcinogens cause DNA changes in the bladder mucosa, leading to common molecular changes, such as loss of alleles on chromosome 9, including the 9p region with the p16/ARF gene, which is often inactivated by LOH, deletion, or methylation. This locus also contains the IFN-α gene, whose inactivation may contribute to disease progression. LOH on 9q is one of the earliest events in the progression of bladder cancer [54]. Mapping of the entire bladder and analysis of its recombination markers on chromosomes 1–22 revealed six critical regions, including 3q22, 5q22–23, 9q21, 10q26, 13q14, and 17p13 [55].
3.3. Clinical Symptoms
Data published on 16 February 2023 by the National Cancer Institute indicated a diverse spectrum of bladder cancer symptoms, which can vary from patient to patient. The most commonly reported symptom is hematuria [56], which is the presence of blood in the urine, which can range from slightly rusty red to intense red. Hematuria is often episodic, and in some cases the amount of blood is so small that it does not cause a visible change in urine color, which means it can only be detected by microscopic examination (so-called microscopic hematuria). Approximately 1.3% of patients with asymptomatic microscopic hematuria (three or more red blood cells in the high-power field of view in a properly collected specimen, without an obvious benign cause) have bladder cancer, with estimates ranging from 0.4% to 6.5% [57]. Additional symptoms, such as frequent urination, pain or burning during urination, a feeling of incomplete emptying of the bladder, or an urgent need to urinate, are also common but not specific to bladder cancer (Figure 6). These symptoms, referred to as irritative urinary symptoms (including frequent urination, urgency, nocturia, or dysuria), may occur over the course of other, more common urinary tract conditions, such as infections, urolithiasis, or benign prostatic hyperplasia. However, due to the risk of cancer, it is necessary to perform appropriate diagnostic procedures to rule out bladder cancer. Obstructive symptoms, such as a weak or interrupted stream of urine, straining during urination, or a feeling of incomplete emptying of the bladder, may occur if the tumor is located near the bladder neck or urethra, which additionally affects the difficulty in urinating. In cases of advanced bladder cancer, symptoms may include those resulting from local disease advancement or the presence of metastases. These may include abdominal pain, difficulty urinating, anuria, lower back pain, and bone pain associated with bone metastases [58]. The most common sites of metastasis include the lymph nodes, bones, lungs, liver, and peritoneum [59]. Patients with advanced disease may also present with systemic symptoms, such as weight loss, loss of appetite, fatigue, and lower limb edema, which further complicates the clinical picture. In advanced stages of the disease, physical examination may reveal a palpable renal or bladder mass, indicating advanced disease or the presence of metastases.
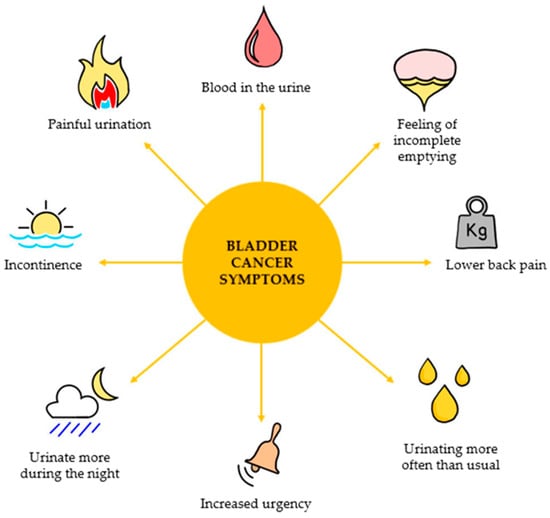
Figure 6.
Possible symptoms of bladder cancer.
3.4. Stages of Advancement
Cancer staging (Figure 7) refers to the extent to which the cancer has spread in the body, including the size of the tumor, the presence of metastases, and the extent of the spread from the primary site. Precise staging of bladder cancer is essential for developing an appropriate treatment plan. There are several staging systems in oncology. For bladder cancer, the most commonly used staging system is the Tumor-Node-Metastasis (TNM) system [60]. Pathology reports are based on the results of this system. The TNM staging system is used to determine the stage of the cancer, assigning it to one of the following stages: I, II, III, or IV (also recorded as stages 1, 2, 3, or 4) [61].
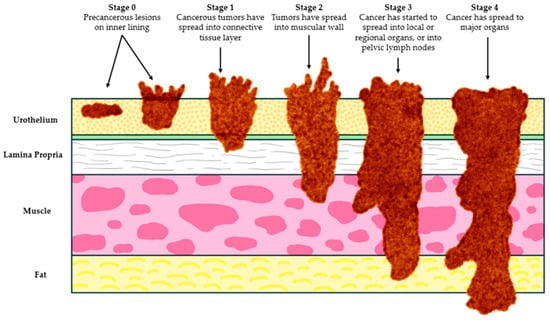
Figure 7.
Bladder cancer stages.
3.4.1. Stage pT0
pT0 bladder cancer refers to cases in which no residual urothelial cancer, either invasive or non-invasive, is found after cystectomy. In the past, the percentage of bladder cancer cases in the pT0 stage was approximately 10% [62], but with the increasing use of neoadjuvant chemotherapy (NAC), the incidence of this stage has been increasing, reaching values approaching 30% [63]. NAC is more effective in achieving a complete pathological response (pT0) than radical cystectomy alone, suggesting that its main advantage may be an increased chance of achieving the pT0 stage [64]. Nevertheless, most patients do not achieve pT0 after NAC. The prognosis for patients with pT0 bladder cancer is generally very good, especially when they achieve a complete pathological response (pT0N0M0), which is associated with better overall and relapse-free survival [65]. In one study, five-year relapse-free survival was 84%, cancer-specific survival 88%, and overall survival 84%. However, some patients may still experience relapse, especially in cases with prior extravesical spread [66]. Lymphatic and vascular invasion (LVI) and carcinoma in situ (CIS) in TUR specimens are significant prognostic factors for pT0 patients. Patients with LVI have a poorer prognosis, with a five-year overall survival of 70%, compared with 89% in patients without LVI. Although lymph node metastases in patients with pT0 bladder cancer are rare, they occur in 3–7% of cases, which may negatively impact prognosis [67].
Stage pTa
Approximately 70% to 80% of bladder cancers occur as non-invasive tumors of the bladder muscle. Of these, 60% to 70% are confined to the bladder mucosa, which corresponds to stage pTa [68]. It includes papillary neoplasms confined to the urothelium that do not show invasion of other layers of the bladder wall. Also known as non-invasive papillary carcinoma, it is characterized by the presence of papillary growths extending into the lumen of the bladder. This type of tumor can be low-grade or high-grade, depending on the degree of atypia of the cells seen under the microscope. According to the 8th edition of the AJCC Staging Manual, papillary urothelial carcinoma without invasion is classified as stage pTa. In stage pTa, the key prognostic factor is the histologic grade, which should be clearly stated in the pathology report. Any presence of invasion excludes the tumor from the pTa category and moves it to a more advanced stage. If a flat urothelial lesion, such as carcinoma in situ (CIS), is present, it should also be reported, as it has important prognostic implications. In cases where both papillary neoplasm and CIS are present, it is recommended to consider assigning both categories—pTa and pTis—to accurately reflect the complexity of the neoplastic lesions [69].
Stage pTis
Stage pTis, known as carcinoma in situ, is an early form of bladder cancer that is confined to the epithelium lining the bladder. Unlike other types of cancer, CIS does not invade deeper layers of tissue, remaining in the superficial layer. Although CIS is non-invasive, it is characterized by a high grade of malignancy. CIS is usually a flat, nonpapillary lesion composed of atypical urothelial cells that exhibit features such as enlarged nuclei, irregular nuclear shape, and increased mitotic activity. Due to its aggressive nature, CIS can be resistant to standard treatments, including chemotherapy, and tends to progress to more advanced, invasive forms of cancer if not treated appropriately [70]. Carcinoma in situ can occur alone or in association with other bladder neoplasms, such as invasive urothelial cancer. The clinical significance of CIS is that its presence in the pT0–pT2 stages (i.e., early stages of invasion) is associated with a poorer prognosis, as it increases the risk of disease recurrence and progression to more advanced stages. In more advanced stages of bladder cancer (pT3–pT4), however, the presence of CIS does not significantly affect the prognosis of patients [71]. Due to the risk of progression and the difficulty of treatment, the identification and monitoring of CIS is a key element of disease management in patients with bladder cancer.
3.4.2. pT1 Stage
Stage pT1 bladder cancer involves tumor invasion into the lamina propria without invasion of the muscularis propria. In patients at this stage, disease recurrence and progression occur in about 50% and 10% of cases, respectively, making the identification of patients at high risk of progression an important clinical goal and the subject of intensive research. The pT1 sub-staging, recognized as an important prognostic factor in the 2016 WHO classification of genitourinary cancers and in the 8th edition of the AJCC Staging Manual, aims to better differentiate patients by separating small foci of invasion from more extensive lesions. In clinical practice, the introduction of this sub-staging is recommended; however, the lack of a clearly recognized method of classification means that official sub-staging categories for the pT1 stage have not yet been established. Additionally, interobserver variability in pT1 staging and the associated diagnostic difficulties remain a significant challenge in pathology [72].
3.4.3. Stage pT2
Bladder cancer stage pT2 is characterized by tumor invasion of the muscularis propria layer of the bladder. Stage pT2 is divided into two sub-stages: pT2a, where the tumor invades the superficial muscularis propria (i.e., the inner half of this layer), and pT2b, where the tumor invades the deep muscularis propria (i.e., the outer half of this layer) [73]. Patients with deeper invasion (pT2b) were initially thought to have a poorer prognosis than those with shallower invasion (pT2a), as early studies suggested significant differences in survival between these sub-stages [74]. However, later studies have not confirmed these conclusions, indicating that the differences in survival between pT2a and pT2b may not be as significant. It has been found that tumor size may play a greater role in predicting the outcome in patients with pT2 bladder cancer [75]. Nevertheless, more recent analyses suggest that the pT2a and pT2b division may be clinically useful, especially in the context of relapse-free and cancer-specific survival [76]. The results of these studies indicate the need for further analyses to clearly assess the usefulness of this division and to examine other prognostic factors, such as tumor size.
3.4.4. Stage pT3
Stage 3 bladder cancer is an advanced stage of the disease, which is divided into two sub-stages: 3a and 3b. In stage 3a, the cancer has invaded through the muscle and wall of the bladder, reaching the surrounding fat layer, and potentially spreading to adjacent reproductive organs, such as the prostate, uterus, or vagina. However, it does not spread to lymph nodes. Alternatively, at this stage, the cancer may spread to one pelvic lymph node, provided that it is not close to the major iliac arteries. In stage 3b, the cancer has spread to more than one pelvic lymph node that is not close to the iliac arteries, or to one node in the immediate vicinity of the iliac arteries. The distinction between pT3a and pT3b has important prognostic implications, as pT3b is usually associated with poorer outcomes, especially in patients without lymph node metastases (pN0) [77]. Assessment of the degree of macroscopic infiltration is crucial for accurate staging of the disease, but this process can be difficult due to the irregular structure of the muscularis and surrounding adipose tissue. Precise diagnostics is, therefore, crucial for proper staging of the disease and for determining the optimal treatment strategy.
3.4.5. Stage pT4
Stage 4 bladder cancer is classified into subtypes 4a and 4b, depending on the stage of the disease and the extent of metastasis. In stage 4a, the cancer invades anatomical structures, such as the abdominal wall or pelvic wall. Alternatively, metastasis may occur in lymph nodes located above the main pelvic arteries, the common iliac arteries. In stage 4b, the tumor invades the pelvic wall or abdominal wall. This stage does not refer to generalized spread of the tumor to distant organs, but to local invasion of these key structures. It is important to emphasize that metastases to distant organs, such as lung, bone, or liver, are classified separately, in the “M” category (metastases) of the TNM classification (Table 7). An important aspect of cancer biology is the fact that cancer cells in metastatic foci retain the morphological and molecular characteristics of the primary tumor. For example, in cases where bladder cancer spreads to the lungs, the cancer cells in the lung remain bladder cancer cells, not lung cancer. For this reason, such spreads are classified as metastatic bladder cancer, not lung cancer. TNM classification for bladder cancer is presented in Table 7.
Table 7.
TNM classification for bladder cancer.
3.4.6. Prevention
Bladder cancer is a major health problem worldwide, not only because of its high incidence and associated mortality rates, but also because of the significant costs of its treatment. A significant proportion of bladder cancer cases, especially invasive forms, are strongly associated with preventable environmental factors. Recent meta-analyses have shown that up to 81.8% of bladder cancer cases between 1995 and 2015 could be attributed to known environmental causes. Tobacco smoking is the most important risk factor, accounting for 50–65% of all bladder cancer cases in developed countries. Quitting smoking reduces the risk of bladder cancer by about 40% within 1–4 years, and complete recovery to pre-smoking risk occurs after 20 years [78,79]. Quitting smoking is, therefore, one of the most effective preventive strategies. In addition to smoking, occupational exposure to carcinogens, particularly in manufacturing, transportation, and firefighting, is the second major preventable risk factor. In contrast, occupations such as farming and teaching, which have less exposure to toxic substances, are associated with lower risk. Protecting workers from exposure to harmful chemicals, such as aromatic amines, is key to reducing the incidence of bladder cancer. Other preventive strategies include eating a diet rich in fruits and vegetables, which, although controversial, may offer some protection. Physical activity, regardless of smoking status or body mass index (BMI), has also been shown to have a small but noticeable protective effect against bladder cancer. Despite the well-documented association between smoking, occupational exposures, and bladder cancer, urologists have traditionally played a limited role in prevention. However, as their involvement in men’s health grows, they are well positioned to play a more active role in cancer prevention, especially considering their regular contact with patients with bladder cancer. The World Urologic Oncology Federation (WUOF) leads a global effort to promote bladder cancer prevention through educational initiatives, anti-smoking campaigns, and work to reduce exposure to carcinogens in the workplace. This comprehensive approach to prevention is key to reducing the global burden of bladder cancer [78,79].
3.5. Bladder Cancer Diagnosis
The goal of screening and improving diagnostics for bladder cancer is to improve patient survival by detecting the cancer at an earlier, more curable stage of the disease. This allows for faster implementation of appropriate treatment, which can significantly reduce the risk of progression to more advanced stages, which are more difficult to treat and associated with a poorer prognosis. Various diagnostic methods aim to identify cancers before the patient becomes symptomatic, which can increase the chances of successful intervention and thus improve long-term treatment outcomes. There are many different methods that are multidisciplinary in their approach [80].
3.5.1. White Light Cystoscopy (WLC) and Blue Light Cystoscopy
Cystoscopy is a diagnostic procedure in which a doctor uses a cystoscope to visualize the inside of the bladder and urethra, allowing for the identification of potential pathologies. It is an important method in the diagnosis and treatment of bladder cancer, as well as other urological diseases. During the procedure, a cystoscope, a thin, tubular device equipped with a light and lens, is slowly inserted through the urethra into the bladder. The cystoscope may also have tools for removing small tumors or taking tissue samples for biopsy. Standard white light cystoscopy (WLC) has been used for years to detect and resection bladder tumors, but new technologies have been developed to improve the quality of cystoscopy and transurethral resection of bladder tumors (TURBT) to more effectively prevent recurrence and progression of the disease. Cystoscopy should be performed in all patients with macroscopic hematuria and in patients aged 35 years and older with microscopic hematuria. It may also be considered in younger patients with microscopic hematuria. In patients with hematuria and risk factors for bladder cancer, irritative symptoms during urination, or exposure to chemicals, cystoscopy should be performed regardless of age. Patients with abnormal bladder lavage cytology or pathologically abnormal tissue should undergo transurethral resection of the bladder tumor (TURBT). This procedure provides key histopathological information necessary for the final diagnosis, staging, and classification of the tumor, and allows for removal of visible tumor and sampling of surrounding muscle to assess the depth of tumor invasion [81].
PDD (photodynamic diagnostics) increases the detection of occult bladder tumors. This technique involves the introduction of a dye, such as 5-aminolevulinic acid (5-ALA) or its hexyl ester (HAL; Hexvix®; Photocure ASA), into the bladder. This dye accumulates in diseased tissues, making them sensitive to light. Diseased tissues glow red under blue light, while healthy tissues remain blue. PDD is recommended for diagnostics during initial transurethral resection of bladder tumors (TURBT), as well as in patients with positive urine cytology but negative results on standard cystoscopy (WLC). This method can also be used to evaluate recurrences in patients who have not previously been examined with PDD and to monitor patients with carcinoma in situ (CIS) or multifocal tumors. Analyses and studies show that blue light cystoscopy (BLC) detects more tumors than traditional WLC, including more high-risk tumors. The results of four randomized clinical trials (RCTs) confirmed that BLC with 5-ALA during TURBT allows for more thorough removal of tumors and prolongs the recurrence-free survival. However, differences in the use of additional intravesical therapy in these studies may have influenced the assessment of the benefits of PDD. To date, PDD has not been proven to prevent disease progression or prolong patient survival [82].
3.5.2. Computed Tomography of Urography
Computed tomography urography (CTU) is a valuable tool in detecting bladder cancer because it allows simultaneous imaging of the urinary tract, renal parenchyma, and other abdominal structures, which allows for the identification of lesions and determination of the stage of the neoplastic disease. Despite this, the accuracy of CTU in local staging of cancer is only 40–60%. CTU is performed for various indications, such as renal colic, urolithiasis, urinary tract obstruction, hydronephrosis, infections, urinary tract neoplasms, hematuria, or trauma, but this examination requires standardization, and further studies are necessary to achieve this. In doubtful cases or to better visualize defects in bladder filling and lower ureters, the excretory phase is used in the supine position. The sensitivity and specificity of CTU are 96.3% and 86.4%, respectively, which is confirmed by high agreement with the results of the literature. However, despite its high sensitivity, the specificity of CTU is limited, and false-negative results may be caused by the small size of the lesions (<5 mm). Some experts suggest that performing CT virtual cystoscopy, which has a diagnostic accuracy of 95%, could help to improve the results, although this method is invasive. Another limitation of CTU is the difficulty in differentiating between neoplastic and inflammatory changes in flat lesions, which may lead to false-positive results. Therefore, it is recommended to perform radiological examinations before cystoscopy to avoid false results. CTU can also help to guide cystoscopy in difficult-to-access areas of the bladder [83].
3.5.3. Intravenous Urography (IVP)
IVP, or intravenous urography, is an X-ray examination of the urinary tract that involves injecting a contrast agent into a vein and then taking a series of X-rays of the kidneys, ureters, and bladder to check for cancer. As the contrast agent moves through the urinary system, additional images are taken at specific times to assess urinary tract function and detect any signs of disease. IVP was the standard for urinary tract imaging from 1923 until about 2000, but with the introduction of computed tomography (CT), which became the gold standard for urinary tract diagnostics, its use was reduced. Despite this, IVP is still used, although its diagnostic capabilities are significantly inferior to CT. Studies have shown that IVP was most often used to evaluate kidney stones and lower back pain, but 48% of patients required additional imaging, underscoring its diagnostic limitations. CT is more sensitive and specific for detecting urinary tract pathology, including lumbar pain, nephrolithiasis, renal masses, and hematuria, and in the pregnant population with lumbar pain, ultrasonography is recommended as the first examination due to the lack of ionizing radiation. Painless hematuria also requires imaging, and contrast-enhanced CT is more effective in detecting urinary tract masses, especially small renal masses. After abdominopelvic surgery, evaluation of the urinary tract is crucial, especially if there is a risk of injury to the ureters or bladder. Although IVP can be used in emergency situations or where modern CT scanners are not available, CT is the preferred method for urological diagnostics due to its many advantages, despite some disadvantages, such as a higher radiation dose and cost [84].
3.5.4. Narrowband Imaging
Narrowband imaging (NBI) cystoscopy improves the visibility of small structures of the bladder mucosa surface without the use of dyes. Longer wavelengths of light allow for deeper tissue penetration. Unlike BLC (blue light cystoscopy), which requires preoperative administration of photosensitizing agents via a catheter, NBI cystoscopy does not require additional invasive procedures. It can also be performed using a flexible cystoscope, which makes it convenient in an outpatient setting. NBI cystoscopy improves the detection of recurrent non-muscle-invasive bladder cancer (NMIBC) compared to standard WLC cystoscopy, with a comparable false-positive rate. TURBT (transurethral resection of bladder tumor) performed using NBI reduces the risk of NMIBC recurrence by at least 10% after one year. However, there have been no clinical trials comparing NBI cystoscopy with WLC or BLC [85,86].
3.5.5. Urine Cytology
Urine cytology remains the standard for detecting high-grade malignancies, although available biomarkers often have low specificity and high false-positive rates, especially in mild inflammatory conditions. New genetic markers, although promising, also face similar challenges. The UroFollow study aims to reduce the intensity of monitoring low-grade malignancies with non-invasive methods, but for high-grade malignancies, urine cytology and cystoscopy are likely to remain the standard. The challenge is to effectively combine available biomarkers, considering their limitations. Systematic reviews show that single tests have limited diagnostic value, and multitarget markers may have better performance. Despite the increasing number of urinary biomarkers, no single method has replaced cystoscopy as the gold standard for diagnosing and monitoring bladder cancer. Issues with validation, different normative thresholds, and the complexity of biomarkers continue to challenge their development [87].
3.5.6. Biopsja Płynna
Liquid biopsy is a modern and promising diagnostic method that involves the analysis of various biological fluids, such as blood, urine, plasma, cerebrospinal fluid, or saliva, to detect cancers and monitor their progression. In the context of bladder cancer (BCa), liquid biopsies are particularly valuable because they enable a non-invasive examination that can detect the presence of the disease, its recurrence, progression, and response to treatment, without the need for invasive procedures, such as cystoscopy. Urine is a particularly attractive material for liquid biopsy in the diagnosis of bladder cancer because it contains nucleic acids from cancer cells, which are directly released into the urine, which minimizes the risk of contamination of the material. Thanks to this, genetic changes in urine can accurately reflect those occurring in urogenital tumors. Various diagnostic systems based on urine analysis have been developed, including the detection of specific biomarkers of genes, proteins, and metabolites that can identify bladder cancer even before the appearance of clinical symptoms. However, despite promising results in studies, further validation studies and standardization of sample collection and analysis procedures are necessary to ensure their effectiveness and broad clinical application. In advanced, metastatic bladder cancer, blood is becoming the preferred fluid for liquid biopsy because it allows for the identification of mutations and monitoring of disease progression, which can support therapeutic decisions. Although liquid biopsies offer great potential, there is still a need for large, prospective cohort studies to fully evaluate their clinical value and to implement them on a large scale as a standard in the diagnosis and monitoring of bladder cancer [88].
3.5.7. Protocols in Diagnosis
In European countries, the diagnosis of hematuria, both macroscopic and microscopic, plays a key role in the detection of urinary tract malignancies, including urothelial carcinoma (UCC) and renal cell carcinoma (RCC). Hematuria is often the first symptom leading to the detection of these malignancies, and patients usually undergo both cystoscopy and computed tomography of the urinary system (CTS). Depending on the country and the medical protocols used, the time to diagnosis and the structure of the studies may vary. In some countries, such as Norway, a three-phase CTU protocol is recommended, which includes corticomedullar, nephrographic, and excretory phases, to thoroughly examine both the kidneys and the urinary tract [89,90].
The most commonly used protocol is imaging in case of negative cystoscopy, which allows for the detection of upper urinary tract malignancies. Studies suggest that early detection of malignancies during the nephrographic phase is crucial. The time from the onset of symptoms, such as hematuria, to the initiation of diagnostic procedures is crucial for patient prognosis, and some European countries have guidelines that emphasize the importance of rapid diagnosis after the onset of symptoms.
3.5.8. The Role of Urinary Microbiome as a Biomarker
In the context of new diagnostic tools, the role of biomarkers is becoming increasingly important, and recent studies have increasingly drawn attention to the relationship between the urinary microbiome and bladder cancer. In 2023, an analysis of the urinary microbiome of patients with bladder cancer was carried out, using urine samples collected in the morning as a potential source of biomarkers for early cancer detection. The results of the study showed that patients with bladder cancer, especially men over 50 years of age, had a significantly increased number of bacteria from the genus Porphyromonas, and in particular Porphyromonas somerae. The increase in the number of these bacteria may be associated with chronic inflammation, which is one of the key mechanisms supporting the process of carcinogenesis. The presence of Porphyromonas somerae has also been identified as a specific biomarker of the risk of developing bladder cancer. An important aspect of this study was that morning urine samples (FM) were as effective as more invasive samples obtained by catheterization, making them a more practical and non-invasive tool for analyzing the urinary microbiome. This makes morning urine samples a useful tool for monitoring the risk of bladder cancer and potentially for early diagnosis. These findings have important implications for future research on biomarkers in bladder cancer. Analysis of the urine microbiome may provide non-invasive diagnostic methods that will enable early detection of the disease, which is crucial for improving patient outcomes. Furthermore, the study suggests that the presence of Porphyromonas may play a direct role in the pathogenesis of bladder cancer, which requires further investigation into the mechanisms that may lead to the development of this cancer via the microbiome [91].
3.5.9. Role of Systemic Inflammatory Index (SII) in Prognostic Assessment of Bladder Cancer
In addition to well-known prognostic factors, recent studies have shown that the Systemic Inflammatory Index (SII) may be a useful predictive marker of oncological outcomes in patients undergoing radical cystectomy for bladder cancer. A study conducted in 2023 showed that elevated preoperative SII values were strongly associated with a higher risk of nodal invasion, advanced pT stage of tumor, and poorer survival outcomes. The SII, calculated as the product of neutrophil count and platelet count divided by lymphocyte count, reflects the inflammatory status of the patient. The study found that a higher SII (>640.27) was an independent predictor of poorer relapse-free survival (RFS) and overall survival (OS). These results suggest that the SII may be useful in identifying patients at higher risk of relapse and allows for better tailoring of therapeutic strategies, including possible intensification of postoperative treatment, e.g., in the form of adjuvant chemotherapy [92].
Bladder cancer treatment is a complex process that requires an individual approach, taking into account the stage of the disease, the type of cancer, the patient’s general health, and their preferences. Depending on these factors, different therapeutic strategies are used. The key goal of treatment is not only to eliminate the cancer, but also to minimize the risk of recurrence and improve the patient’s quality of life. Early-stage bladder cancer can be effectively treated with less invasive procedures, while advanced cases often require more aggressive multimodal therapies [92]. Below is an overview of the different therapeutic approaches used in the treatment of bladder cancer.
Pembrolizumab, a PD-1 checkpoint inhibitor, is a promising treatment option for patients with non-muscle-invasive bladder cancer (NMIBC) who are not responding to Bacillus Calmette–Guérin (BCG) therapy, particularly those who are not candidates for or refuse cystectomy. The approval of pembrolizumab for this group of patients is based on the results of the KEYNOTE-057 trial, which demonstrated significant clinical efficacy. In that trial, pembrolizumab was evaluated in patients with high-risk NMIBC who had carcinoma in situ (CIS) or papillary tumors and who had not responded to BCG. In this group of patients, the complete response rate was approximately 41%, and the median duration of response was 16.2 months. These results suggest the potential of pembrolizumab as an alternative for patients who would otherwise require cystectomy [93]. The use of pembrolizumab in the treatment of NMIBC is important because it addresses the needs of patients who relapse or fail to respond to BCG therapy. Current intravesical therapies, such as valrubicin, have limited efficacy, and cystectomy, although effective, is associated with a high risk of complications. Pembrolizumab, by harnessing the body’s immune system, offers a less invasive approach that can preserve bladder function in a significant number of patients [94]. Considering these promising results, pembrolizumab is gaining importance as an important therapeutic option for the treatment of BCG-refractory NMIBC. Ongoing studies are aimed at confirming these results and exploring the possibility of using pembrolizumab in combination therapies, which may improve patient outcomes [95].
3.6. Bladder Cancer Treatment
3.6.1. Transurethral Resection of Bladder Tumor (TURBT)
Transurethral resection of bladder tumor (TURBT) is considered the gold standard in the diagnosis and treatment of non-invasive bladder cancer. This procedure aims not only to potentially cure selected bladder tumors but also to accurately determine the stage of the tumor, especially in high-risk tumors and muscle-invasive lesions that require additional therapy, such as radical cystectomy or chemoradiotherapy. Although TURBT is an effective treatment, its main challenge is the high recurrence rate, ranging from 35% to 70%, indicating the need for improvement of this technique. To improve the results, additional resection (re-TURBT) after 4–6 weeks or the use of photodynamic diagnostics (PDD) during the first procedure is often recommended. PDD allows for better detection and removal of tumors, which reduces the risk of residual tumors. Studies have shown that early re-TURBT can significantly reduce the recurrence rate by better estimating the risk of disease progression [96]. Although transurethral resection of bladder tumor (TURBT) has been the mainstay of bladder cancer treatment for decades, it has some challenges that require improvement. The traditional “incision and dispersion” technique fragments the tumor, which can increase the risk of tumor spread and complicate accurate histological assessment, as well as lead to incomplete resection. In addition, there is a risk of perioperative complications, such as bladder perforation and acute urinary retention. Due to the high risk of disease recurrence and progression, new resection techniques are gaining increasing attention, which may improve treatment outcomes. One of the most promising advances is en bloc resection of bladder tumor (ERBT), which allows for the removal of the tumor in its entirety, preserving its structure and margins. As a result, ERBT can provide better pathological assessment, reduce the risk of recurrence, and reduce the number of perioperative complications. Studies have shown that ERBT leads to high-quality resection, with the presence of the detrusor muscle in almost all cases, making this method a promising alternative to conventional TURBT and an important step forward in the treatment of bladder cancer [97].
3.6.2. Mycobacterium Bovis Bacillus Calmette–Guérin (BCG)
Mycobacterium bovis Bacillus Calmette–Guérin (BCG) is a bacterial strain that was created after 230 recultivations of pathogenic Mycobacterium bovis by Albert Calmette and Camille Guérin in 1921. BCG was initially developed as a vaccine against tuberculosis and remains the only commercially available vaccine against this disease to this day. In the 1970s, BCG began to be used in the treatment of bladder cancer, particularly in patients with non-muscle-invasive bladder cancer (NMIBC). Intravesical BCG infusions have become the standard of care for high-risk NMIBC, where they help prevent recurrence and progression of the disease after transurethral resection of the tumor (TURBT). The mechanism of action of BCG is based on the stimulation of a local immune response in the bladder, leading to the destruction of residual tumor cells. This therapy consists of an initial induction phase of six weeks, followed by maintenance therapy that can last from one to three years, depending on the risk of relapse. Although BCG is an effective therapy, it is not free from side effects. Many patients experience flu-like symptoms and bladder irritation, and in rare cases more serious complications can occur, such as systemic BCG infection, which requires intensive antibiotic treatment. It is also worth noting that there are differences in toxicity and efficacy between different BCG sub-strains. Comparative studies suggest that some sub-strains may cause more side effects than others, but the results are inconsistent. In the context of the global shortage of BCG that has occurred in recent years, medical guidelines have been adapted to optimally manage available resources, including the use of lower doses or alternative therapies in patients at intermediate risk. Despite these challenges, BCG remains the gold standard for the treatment of NMIBC, and new, personalized therapeutic approaches are being developed that may replace or complement this therapy in the future [98,99].
3.6.3. Cystectomy
Radical Cystectomy
Radical cystectomy, recommended by the National Comprehensive Cancer Network (NCCN), is considered the standard treatment for patients with muscle-invasive bladder cancer. This procedure involves the complete removal of the bladder and associated organs. In men, it involves the removal of the prostate, and in women, the uterus, ovaries, and part of the vagina. Cystectomy is a complex surgery that can take from 4 to 8 h, depending on the stage of the cancer and the extent of reconstruction of the urinary tract. The effectiveness of radical cystectomy is supported by studies showing that patients who undergo this procedure have significantly better survival rates compared with those who receive alternative therapies, such as chemotherapy, radiation therapy, or medical supervision. For example, the five-year survival rate after cystectomy ranges from 62% to 80% in patients with stage II cancer, whereas in patients with stage IV cancer, it ranges from 0% to 36% [100]. Although postoperative mortality has been significantly reduced compared to previous years, the postoperative morbidity rate remains high, which is due to the complexity of the procedure itself, especially in the case of advanced urinary diversion (UD) techniques. The success of the operation depends on the experience of the surgeon, and insufficient practice in different UD techniques may lead to a higher risk of complications. The most common complications after cystectomy include infections, bleeding, deep vein thrombosis, bowel injuries, and complications related to urinary diversion, such as anastomotic strictures or leaks. In the long term, patients may also suffer from metabolic disorders, bowel dysfunction, and urinary continence problems. Two key factors influencing improved outcomes are increasing the surgical volume (i.e., the number of surgeries performed) and reducing long-term postoperative complications. To achieve these goals, it is necessary to standardize the definitions of complications, standardize postoperative monitoring of patients, and collect prospective data, which will allow for further improvement of the results after cystectomy [101].
Partial Cystectomy
Partial cystectomy (PC) with bilateral pelvic lymph node dissection is being considered as an alternative treatment for muscle-invasive bladder cancer in carefully selected patients. Although PC is not a standard approach for the treatment of this type of cancer, it is an acceptable option for approximately 5–10% of patients who meet specific clinical criteria, such as unifocal disease without carcinoma in situ (CIS). There are case reports in the literature in which PC has been shown to be effective, with fewer complications compared to radical cystectomy (RC), making it a less burdensome alternative, especially for patients who cannot undergo RC due to the risk of high morbidity. Although retrospective data suggest that PC can lead to acceptable oncological outcomes, especially in the short term, its long-term efficacy compared to RC remains controversial. Therefore, PC is recommended only for appropriately selected patients, and further studies are needed to better define its role in the comprehensive treatment of bladder cancer [102].
Conservative techniques, such as trimodality therapy, are gaining popularity as an alternative to radical cystectomy for muscle-invasive bladder cancer (MIBC). Trimodality therapy, consisting of maximal transurethral resection (TURBT), radiotherapy, and chemotherapy, has been shown to be effective in carefully selected patients. A 2023 study showed that the five-year metastasis-free survival was about 75% with trimodality therapy, which is comparable to radical cystectomy. In a study of 722 patients, there was no significant difference in disease-specific survival or overall survival in the short term between patients who underwent trimodality therapy and those who underwent radical cystectomy. Furthermore, the five-year overall survival rate was 73% for patients who received trimodality therapy, suggesting that it is a valuable option for patients who do not wish to undergo or are unable to undergo cystectomy [103].
Other studies suggested that trimodality therapy may be further improved with modern radiotherapy techniques, such as intensity-modulated radiotherapy (IMRT), and the use of new drugs, such as immune checkpoint inhibitors [104].
These results show that trimodality therapy can be an effective option for selected patients, offering similar survival outcomes while preserving bladder function, although long-term comparisons suggest some advantage over radical cystectomy in terms of overall survival at 5 and 10 years [105].
3.6.4. Systemic Chemotherapy
Neoadjuvant (Preoperative) Chemotherapy
Platinum-based neoadjuvant chemotherapy (NCT) is considered the standard treatment strategy for muscle-invasive bladder cancer (MIBC). Its introduction before local-regional therapy, such as radical cystectomy, leads to a significant improvement in overall survival. Meta-analyses and the results of many randomized clinical trials confirmed that the use of cisplatin-based combination chemotherapy, especially in regimens such as methotrexate, vinblastine, doxorubicin, and cisplatin (MVAC) and gemcitabine and cisplatin/carboplatin (GC), contributes to a significant reduction in the risk of death compared with surgery alone. Although both regimens are effective in the neoadjuvant setting, current data suggest that MVAC may provide better survival outcomes compared to GC, although the differences in pathological response between these regimens are not statistically significant. Cisplatin-based NCT, with the appropriate dose and intensity of treatment, should be a common preoperative therapy, although further studies are needed to better define the optimal treatment regimen and its long-term benefits [106]. Newer studies from 2023 indicate that in patients who cannot receive cisplatin, the gemcitabine/carboplatin regimen (Gem/Carbo) is used. Although Gem/Carbo has less toxicity, it does not offer as large an overall survival benefit as cisplatin regimens [107].
Recent studies indicate that neoadjuvant chemotherapy for cT2–4, N0, and M0 disease can lead to a 5–10% increase in cancer-specific survival (CSS). NCT can also reduce the number of micro-metastases prior to surgical treatment. However, in some patients, this treatment may be ineffective, which may result in a delay in surgery with potentially serious consequences, while exposing them to the toxicity of the therapy [108].
Adjuvant Chemotherapy (Postoperative)
Adjuvant cisplatin-based chemotherapy is an important strategy in the treatment of muscle-invasive bladder cancer, leading to significant improvements in clinical outcomes. Results from ten randomized clinical trials (RCTs) indicated a 6% absolute benefit in overall survival at five years (from 50% to 56%), with an 18% reduction in the risk of death (HR = 0.82, 95% CI = 0.70–0.96, p = 0.02). Additionally, adjusted analyses for age, sex, pT stage, and pN stage showed an even larger survival benefit of 9% (from 50% to 59%). Adjuvant chemotherapy also improved relapse-free survival by 11%, locoregional relapse-free survival by 11%, and metastasis-free survival by 8%. The effect of treatment on these parameters confirms its efficacy in reducing the risk of relapse and metastasis, which translates into better long-term outcomes. Despite some limitations related to the diversity of chemotherapy protocols and the premature termination of some studies, the results of the meta-analysis indicated significant benefits of adjuvant chemotherapy, making it an important tool in the treatment of bladder cancer [109]. In 2019, a work was published, the aim of which was to compare the efficacy and parameters of the therapy data. The results of this article are presented below in the form of a table (Table 8).
Table 8.
Comparison of neoadjuvant and adjuvant therapy [110].
3.6.5. Radiotherapy
Radiotherapy plays an important role in both palliative and curative treatment of bladder cancer, although its use is associated with some technical challenges. These difficulties arise from problems with visualizing the tumor, as well as variability in the size and position of the bladder during treatment. To improve the accuracy and efficacy of radiotherapy, magnetic resonance imaging (MRI) is increasingly used, which provides better soft tissue contrast, allowing more precise localization of the tumor and assessment of disease severity. The introduction of hybrid MR-Linac systems, combining MRI scanning capabilities with a linear accelerator, allows for real-time adaptation of the treatment plan, which may benefit patients through more precise dose delivery and reduced radiation exposure to healthy tissue. Although MRgRT (magnetic-resonance-guided radiotherapy) has the potential to improve treatment outcomes, further studies are needed to confirm its clinical efficacy. Radiotherapy, as part of a multimodality strategy, achieves results comparable to radical cystectomy, and long-term bladder preservation is possible in a significant proportion of patients. However, before routinely implementing this technology, solid evidence from randomized controlled trials is needed to confirm its efficacy and benefits for patients with bladder cancer [111]. Additional studies are currently underway on the combination of radiotherapy with chemotherapy, as described in a study published in 2021. The article argues that radiotherapy combined with chemotherapy (cRT) has potential benefits in the treatment of patients with bladder cancer, especially after prior neoadjuvant chemotherapy. In a study of 117 patients, 74% of whom received gemcitabine with cisplatin or carboplatin, cRT improved locoregional control (LRC) compared with radiotherapy (RT) alone, although this difference was not statistically significant. There was no difference in overall survival (OS) between cRT and RT. Although grade ≥ 3 toxicity was higher in the cRT group (33% vs. 22% in the RT group), this difference also did not reach statistical significance. Importantly, radiotherapy combined with chemotherapy did not negatively affect the quality of life of patients. The results suggest that cRT may improve local disease control, but further studies with larger numbers of participants are needed to confirm these observations [112].
3.6.6. Immunotherapy
Immunotherapy is a modern and increasingly effective approach to treating bladder cancer, especially in advanced and metastatic cases. Unlike traditional methods, such as surgery, chemotherapy, or radiotherapy, immunotherapy works by mobilizing the patient’s immune system to fight cancer cells on its own. In recent years, immune checkpoint inhibitors (ICIs), such as PD-1/PD-L1 and CTLA-4 blockers, have played a key role in the treatment of advanced bladder cancer. Drugs, such as atezolizumab, nivolumab, pembrolizumab, and durvalumab, have been approved for both adjuvant and first-line treatment of patients with advanced disease. Particularly in the adjuvant context, immunotherapy is used after surgery in patients at high risk of disease recurrence. Clinical trials, such as the CheckMate 274 study, have confirmed that nivolumab, as an adjuvant therapy, can significantly reduce the risk of relapse in patients with advanced bladder cancer, especially in those with high PD-L1 expression. As a result, checkpoint inhibitors have become a key tool in the fight against disease relapse, improving long-term patient outcomes. Immunotherapy is also used in the first-line treatment of advanced bladder cancer, especially in patients who are not eligible for cisplatin-based chemotherapy. In such cases, PD-1/PD-L1 inhibitors, such as pembrolizumab and atezolizumab, can be used as first-line therapy. This has been confirmed in clinical trials, which have shown that checkpoint inhibitors in this group of patients lead to prolonged overall survival compared to traditional methods, especially in patients with PD-L1-positive tumors. In addition, maintenance immunotherapy after response to chemotherapy, e.g., with durvalumab, has been shown to be effective in patients who have shown an initial response to cisplatin or carboplatin. In patients whose disease has progressed after first-line cisplatin/carboplatin therapy, checkpoint inhibitors have shown significant efficacy. The use of pembrolizumab or atezolizumab in patients who have failed to respond to platinum-based chemotherapy leads to improved overall survival and prolonged progression-free survival [113]. This is particularly important for patients in whom previous treatment options have failed. Although immunotherapy is promising, its efficacy depends on many factors, including the PD-L1 expression level, tumor genetics, and the patient’s gut microbiome. High PD-L1 expression is strongly associated with a better response to checkpoint inhibitors, but not all patients with positive PD-L1 respond to treatment, indicating the need for further studies to better understand the mechanisms of resistance. Other factors, such as the patient’s general condition, comorbidities, and genetic and molecular characteristics of the tumor, may also affect the efficacy of immunotherapy. Currently, new immuno-oncology therapies are being investigated, including antibody conjugates, such as enfortumab vedotin, which may improve the efficacy of urothelial cancer treatment. These novel therapies, combining monoclonal antibodies with cytotoxic molecules, offer hope for further improving the efficacy of advanced bladder cancer treatment, especially in patients who have failed other treatments [114]. Enfortumab vedotin (EV) has been approved by the European Medicines Agency (EMA) as a third-line treatment for patients with advanced bladder cancer who have previously received platinum-based chemotherapy and immunotherapy with checkpoint inhibitors. EV, an antibody–drug conjugate, targets the Nectin-4 protein, which is highly expressed in bladder cancer cells, leading to selective killing of these cells. The approval of this drug was due to its efficacy in improving overall survival compared to standard chemotherapy and its tolerable safety profile in patients with advanced urothelial cancer who had previously received platinum therapy and PD-1/PD-L1 inhibitors. It is also worth mentioning the ongoing clinical trials, such as the EV-103 study, evaluating the use of enfortumab vedotin in the neoadjuvant setting. A study of patients with muscle-invasive bladder cancer (MIBC) who were cisplatin-ineligible has shown promising results. In the phase 1b/2 EV-103 (Cohort H) study, enfortumab vedotin was used as preoperative monotherapy in patients scheduled for radical cystectomy and lymph node dissection (RC+PLND). Patients who received three cycles of EV achieved a pathological complete response (pCR) rate of 36.4% and a pathological stage reduction rate (pDS) of 50%. Additionally, the event-free survival (EFS) rate at 12 months was 76.4%, confirming the efficacy of neoadjuvant EV therapy. The treatment was also well tolerated, with the most common adverse events being fatigue (45.5%), dysgeusia (36.4%), and alopecia (31.8%) [115].
3.7. Different Strategies Depending on the Level of Advancement—Summary
Bladder cancer treatment depends on the stage of the disease and includes a variety of approaches, from surgery to systemic therapies. For non-invasive bladder cancer (stage 0), the primary treatment is transurethral resection of the tumor (TURBT) with fulguration, often supplemented with intravesical chemotherapy or BCG immunotherapy to prevent recurrence. In stage I, treatment is also based on TURBT, but patients with recurrent disease may require partial or total cystectomy. In stages II and III, the main options are radical cystectomy or a combination of chemotherapy and radiotherapy. Chemotherapy is often administered before surgery to improve treatment outcomes. In stage IV, treatment consists of systemic chemotherapy, often combined with immunotherapy or palliative radiotherapy, depending on the extent of metastasis and the patient’s general condition. A significant advancement in the treatment of advanced bladder cancer is the use of avelumab maintenance therapy after first-line chemotherapy. Clinical data indicate that avelumab maintenance therapy provides a significant advantage in progression-free survival (PFS) and overall survival (OS) in patients with advanced disease who have achieved disease control after platinum-based chemotherapy. This therapy is becoming the new standard of care in this context. In the case of recurrent bladder cancer, treatment is adapted to previous therapies and may include chemotherapy, immunotherapy, or targeted therapy. In advanced stages and relapses, palliative therapy may also be a priority to improve the quality of life of patients [96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116].
3.8. Clinical Trials for Bladder Cancer
Historically, combining platinum-based therapies, such as cisplatin or carboplatin, with immunotherapy has not shown a clear OS advantage over chemotherapy alone. This is particularly true for the combination of these platinum drugs with checkpoint inhibitors in earlier-phase studies. However, recent clinical evidence suggests that the combination of cisplatin and nivolumab, especially as first-line therapy, has shown a significant improvement in OS compared with cisplatin alone. This finding represents a promising development in the optimization of treatment for advanced bladder cancer.
Despite numerous achievements in diagnostics and treatment, there is still an urgent need to develop new therapeutic strategies and optimize existing methods. Due to the dynamic development of oncology in recent years, we have observed an intensification of clinical trials on various forms of bladder cancer therapy, including immunotherapy, targeted therapies, and innovative approaches in chemotherapy and radiotherapy. The literature review from 2020 to 2024 includes both early-phase studies (I–II) and those in advanced stages (III–IV), which allows for a comprehensive understanding of current trends and perspectives in bladder cancer treatment. The presented clinical studies not only provide data on potential therapeutic benefits, but also shed light on possible side effects and limitations that may influence the selection of optimal therapy in everyday clinical practice. Figure 8 shows the number of clinical trials for bladder cancer published between 2020 and 2024, identified using the PubMed search engine. The search was performed using a combination of keywords, such as “bladder cancer”, “clinical trial”, and “therapy”. Data on the number of clinical trials were counted based on the PubMed search results, limiting them to the years 2020–2024.
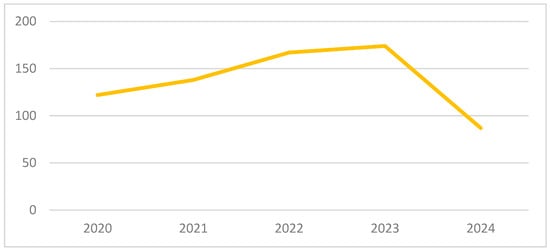
Figure 8.
Number of studies in PubMed for 2020–2024.
3.8.1. Selected Clinical Trials from 2020
The POUT trial, an open-label, randomized, controlled phase 3 clinical trial, was designed to evaluate the efficacy of adjuvant platinum-based chemotherapy in patients with upper urinary tract urothelial carcinoma (UTUC). The trial was conducted at 71 clinical sites in the United Kingdom. It included 261 patients who had undergone radical nephrectomy and had pT2-T4, pN0–N3 M0, or pTany N1–3 M0 UTUC. Participants were randomly assigned to one of two groups: observation, or 4, 21-day cycles of chemotherapy. Randomization was central and based on a random-effect minimization algorithm. The chemotherapy regimen included intravenous cisplatin (70 mg/m2) or carboplatin (AUC 4.5/AUC 5 for glomerular filtration rate < 50 mL/min) on day 1 of the cycle, and intravenous gemcitabine (1000 mg/m2) on days 1 and 8 of the cycle. Chemotherapy was initiated within 90 days of surgery. Monitoring included standard cystoscopic, radiological, and clinical examinations. The primary endpoint of the study was disease-free survival (DFS), analyzed according to the intention-to-treat principle using the Peto–Haybittle rule to assess treatment efficacy. The results of the study showed that adjuvant chemotherapy significantly improved disease-free survival (DFS) in patients with UTUC. The hazard ratio (HR) was 0.45 (95% CI 0.30–0.68, p = 0.0001) with a median follow-up of 30.3 months. The three-year event-free survival was estimated at 71% in the chemotherapy group, compared with 46% in the observation group. Of the 126 patients who started chemotherapy, 44% experienced grade 3 or higher acute adverse events, which was consistent with the expectations for the toxicity of the treatment regimen. In the observation group, only 4% of patients had grade 3 or higher acute adverse events. There were no treatment-related deaths in the study. The findings of the POUT study suggested that gemcitabine- and platinum-based chemotherapy initiated within 90 days after radical nephrectomy should be considered as the new standard of care for patients with locally advanced urothelial cancer of the upper urinary tract, as it significantly improved disease-free survival [117].
A phase 3 clinical trial in patients with locally advanced or metastatic urothelial cancer was designed to evaluate the efficacy of avelumab maintenance therapy in combination with the best supportive care versus supportive care alone. The trial included patients who had not progressed following first-line platinum-based chemotherapy (gemcitabine plus cisplatin or carboplatin). Participants were randomly assigned to receive avelumab or a control group that received supportive care alone. The primary endpoint of the study was overall survival, assessed both in the overall patient population and in the subgroup with positive PD-L1 status. The study results showed that the addition of avelumab to supportive care significantly prolonged overall survival compared with supportive care alone. In the overall population, the median overall survival was 21.4 months in the avelumab group, compared with 14.3 months in the control group (hazard ratio for death, 0.69). A significant improvement in overall survival was also observed in the PD-L1-positive population, with a one-year survival rate of 79.1% in the avelumab group, compared with 60.4% in the control group (hazard ratio for death, 0.56). The study also showed a benefit in terms of progression-free survival, with a median progression-free survival of 3.7 months in the avelumab group and 2.0 months in the control group in the overall population, and 5.7 months and 2.1 months, respectively, in the PD-L1-positive population. However, the adverse event rates were higher in the avelumab group, at 98.0%, compared with 77.7% in the control group. Grade 3 or higher adverse events occurred in 47.4% of patients in the avelumab group, compared with 25.2% in the control group. The results of this clinical trial indicate a significant benefit of avelumab as maintenance therapy in patients with advanced urothelial cancer who have not progressed after first-line chemotherapy. This therapy prolongs overall survival, especially in the PD-L1-positive population, although it is associated with a higher incidence of adverse events [118].
The multicenter, randomized HYBRIDBLUE clinical trial, conducted at six German academic centers, compared the efficacy of two surgical techniques for patients with non-muscle-invasive bladder cancer (NMIBC). The aim of the study was to determine whether transurethral en bloc resection with submucosal hydro-dissection (TUEB) was superior to standard transurethral resection of bladder tumors (TURBT) in terms of the quality of resection and the ability to accurately assess histopathological muscle invasion. The study included 305 patients who were randomly assigned to 1 of 2 treatment groups after initial screening: TUEB, in which resection was assisted by hexaminolevulinate (HAL), or TURBT, in which HAL was also used as an aid for visualization of lesions. The primary objective of the study was to compare the proportion of tissue samples that could be reliably assessed for the presence of muscularis propria and the margins of resection (R0 vs. R1), which are crucial for assessing the completeness of the procedure and planning further treatment. Additional aspects included completeness of resection, presence of muscularis propria in the specimens, recurrence rate, and the rate and type of postoperative complications. The final analysis included 115 patients, 56 of whom underwent TUEB and 59 TURBT. The results of the study showed that 86% of patients in the TUEB group had adequate histopathological slides to accurately assess muscle invasion, compared with 63% in the TURBT group (p = 0.006). Furthermore, complete tumor removal (R0) was confirmed in 57% of patients in the TUEB group, compared with only 9% in the TURBT group (p < 0.001). There were no major complications (class ≥III) in either group. At 3 months after the procedure, disease recurrence occurred in 3 patients in the TUEB group and 7 in the TURBT group, whereas at 1 year, this number increased to 19 and 11 patients, respectively (p = 0.33 and p = 0.08). In summary, the results of this study indicate that TUEB is a safe technique and provides better conditions for histopathological evaluation compared with standard TURBT resection. Although the differences in recurrence rates were not statistically significant, the results suggest that TUEB may reduce the need for early adjuvant resections. However, further studies are needed with recurrence-free survival as the primary endpoint, which will allow for a more precise assessment of the oncological efficacy of both methods [119].
The NCT03998371 clinical trial prospectively recruited patients with urothelial cancer and cancer-free controls. The aim of the study was to develop a non-invasive diagnostic method for urothelial cancer by low-coverage whole-genome sequencing of DNA from exfoliated urine cells. Analyses were performed using the Illumina HiSeq XTen system, followed by the use of a dedicated bioinformatics workflow, called Urine Exfoliated Cells Copy Number Aberration Detector (UroCAD), to identify chromosome copy number changes. In the discovery phase of the study, urine samples from 126 patients with urothelial cancer and 64 samples from non-cancer individuals were analyzed. Patients with cancer had multiple and characteristic chromosome copy number changes that were absent or much less pronounced in the control group. Based on these changes, a diagnostic model was developed, UroCAD, which included all autosomal chromosome changes. The model achieved an AUC of 0.92, with a 95% confidence interval ranging from 89.4% to 97.3%. At the optimal diagnostic threshold of |Z| ≥ 3.21, the model had a sensitivity, specificity, and accuracy of 82.5%, 96.9%, and 89.0%, respectively. A statistically significant correlation was also found between positive prediction and tumor stage (p = 0.01). External validation was performed in a further part of the study on 95 participants. The UroCAD test detected urothelial cancers with a sensitivity of 80.4%, a specificity of 94.9%, and an AUC of 0.91. These results were significantly better than those of traditional cytological tests, which had a sensitivity of only 33.9% (p < 0.001) with comparable specificity (94.9% vs. 100%, p = 0.49). The study suggests that UroCAD may be an effective and non-invasive diagnostic method for urothelial cancer, with better sensitivity than cytological tests, while maintaining similar specificity. It could potentially be used for both early detection of cancer and monitoring for recurrence, reducing the need for invasive diagnostic procedures, such as cystoscopy, which would significantly reduce the burden on patients [120].
To optimize the treatment of non-muscle-invasive bladder cancer (NMIBC), an application (APPv) was developed and evaluated in a prospective, double-blind, observational study of therapy compliance. The aim of the study was to assess the compliance of treatment prescriptions for NMIBC, including both overall compliance and adjustment for disease recurrence and progression rates, comparing APPv recommendations with clinical decisions made by urologists based on their experience. The study was conducted in a sample of 100 patients with histologically confirmed NMIBC, both at initial diagnosis and at later stages of disease. The study compared the therapy recommended by the application with the therapy recommended by the urologist to determine the degree of compliance between the two methods. The results showed that in 64% of cases, the treatment recommended by the urologist was consistent with that recommended by the application, as evidenced by a kappa score of 0.55 (p < 0.0001). Across risk subgroups, agreement was 77% for low-risk patients (kappa 0.55, p = 0.002), 63% for intermediate-risk patients (kappa 0.52, p < 0.0001), 17% for high-risk patients (kappa 0.143, p = 0.014), and 66% for very high-risk patients (kappa 0.71, p = 0.01). The efficacy analysis showed that patients who received adjuvant intravesical therapy according to the app recommendations remained free from relapses in 89.1% of cases, compared with 61.1% of patients who were noncompliant with the app (p = 0.0004), translating into a relative risk (RR) of 0.46 (95%CI: 0.25–0.86) versus RR of 2.4 (95%CI: 1.5–3.8, p = 0.001). Moreover, in the group of patients whose treatment was consistent with the app and urologist’s recommendations, all patients remained free from disease progression, whereas in the group where there was discordance, the percentage was 88.9% (p = 0.004), with an RR of 1 versus RR of 1.125 (95%CI: 1–1.26, p = 0.004). In summary, the results of the study suggest that the APPv app can effectively support adherence to treatment recommendations consistent with clinical guidelines, which may translate into better health outcomes in patients with NMIBC [121].
3.8.2. Selected Clinical Trials from 2023 (Table 9)
A global, randomized, phase 3 clinical trial was conducted to evaluate the efficacy of erdafitinib versus chemotherapy in patients with metastatic urothelial cancer harboring susceptible FGFR3 or FGFR2 alterations. The study population included patients whose disease had progressed after one or two prior therapies, including checkpoint inhibitors, such as anti-PD-1 or anti-PD-L1 antibodies. Participants were randomly assigned to one of two treatment groups: one group received erdafitinib and the other received chemotherapy of the investigator’s choice (docetaxel or vinflunine). The primary objective of the study was to compare overall survival (OS) between the groups. A total of 266 patients were included in the study, of whom 136 were assigned to receive erdafitinib and 130 to receive chemotherapy. The median follow-up time was 15.9 months. The study results showed that the median overall survival was significantly longer in the erdafitinib group (12.1 months) compared with the chemotherapy group (7.8 months). The hazard ratio for death was 0.64 (95% confidence interval 0.47–0.88, p = 0.005), indicating a 36% reduction in the risk of death in the erdafitinib group. In addition, the median progression-free survival (PFS) was also longer in the erdafitinib group (5.6 months) than in the chemotherapy group (2.7 months), with a hazard ratio for progression or death of 0.58 (95% CI 0.44–0.78, p < 0.001). In terms of safety, the incidence of grade 3 or 4 adverse events was similar in the two groups, at 45.9% and 46.4%, respectively. In contrast, treatment-related adverse events leading to death were less common in the erdafitinib group (0.7%) than in the chemotherapy group (5.4%). In summary, the results of the study showed that erdafitinib treatment resulted in significantly longer overall survival compared with chemotherapy in patients with metastatic urothelial cancer with FGFR alterations who had previously received checkpoint inhibitors [122]. A randomized clinical trial was conducted to assess the efficacy of selenium and vitamin E supplementation in preventing recurrence and progression of non-muscle-invasive bladder cancer (NMIBC). The study included 270 patients with newly diagnosed NMIBC, recruited from 10 secondary and tertiary care hospitals in the United Kingdom. Participants were randomly assigned to one of four groups to receive different combinations of supplements: selenium plus placebo, vitamin E plus placebo, selenium plus vitamin E, or placebo plus placebo. Recruitment to the study took place between 17 July 2007 and 10 October 2011, and participation was restricted to a diagnosis of NMIBC (stages Ta, T1, or Tis) and randomization within 12 months of the first transurethral resection of the tumor. The aim of the study was to investigate whether supplementation with selenium and/or vitamin E could reduce the risk of disease recurrence in patients with NMIBC. Patients received oral selenium (200 μg/day selenium-rich yeast), vitamin E (200 IU/day d-alpha-tocopherol), or matching placebo. The mean follow-up time was 5.5 years, and 84% of participants were followed for at least 5 years. The results of the study showed that selenium supplementation had no significant effect on reducing the risk of bladder cancer recurrence. Compared with the control group, there was no statistically significant difference in the relapse-free interval (RFI) in patients receiving selenium. In contrast, vitamin E supplementation was associated with a statistically significant increase in the risk of relapse. The hazard ratio values for vitamin E indicated an increased risk of relapse (1.46; 95% CI 1.02–2.09), suggesting that vitamin E may be potentially harmful for patients with NMIBC. Analyses did not show significant differences in the progression-free interval or overall survival for either group. A total of 1957 adverse events were recorded in the study, 85 of which were considered serious, but none of these events were attributed to the study treatment. Due to slow recruitment of participants, the study was prematurely terminated. The results suggested that vitamin E supplementation may not only not be beneficial but may even pose a risk to patients with NMIBC, which requires further investigation into the biological mechanisms of this phenomenon [123].
The SWOG S1314 study aimed to investigate the potential role of cell-free DNA (cfDNA) methylation as a predictive biomarker of response to neoadjuvant chemotherapy (NAC) in patients with muscle-invasive bladder cancer (MIBC). The study included 72 patients with MIBC (cT2-T4aN0M0, ≥5 mm viable tumor) who had blood samples collected before and during NAC treatment, as per the protocol. The aim of the study was to determine whether cfDNA methylation signatures in plasma could be associated with pathological response to NAC, as assessed by radical cystectomy. The study utilized the Infinium Methylation EPIC BeadChip technology to measure cfDNA methylation. Based on the analysis of differences in methylation between patients who achieved pathological response (≤pT1N0) and those who did not, a predictive classifier was developed using the Random Forest algorithm. The study results showed that cfDNA methylation level before chemotherapy was associated with treatment response, which allowed the development of a methylation response index (mR-score). Additionally, the mR-score obtained after the first cycle of NAC also showed a similar predictive ability. The study also calculated the fraction of circulating DNA from the bladder based on cfDNA methylation data, which proved to be an additional, independent predictor of treatment response. Combining the mR-score with the fraction of circulating bladder DNA correctly predicted pathological response in 79% of patients based on plasma samples collected both before and after the first cycle of NAC. Although the study provided evidence for the efficacy of cfDNA methylation as a predictive biomarker of response to NAC, its limitations included the relatively small number of participants and low levels of circulating bladder DNA in some cases. Nevertheless, the results of this study represent an important step toward personalizing NAC treatment in patients with bladder cancer, suggesting the potential for using cfDNA methylation as a tool to better tailor therapy to patients’ needs [124]. Another phase 1 study evaluated the safety, tolerability, and preliminary efficacy of the novel TAR-200 drug delivery system in patients with muscle-invasive bladder cancer who declined or were ineligible for curative-intent therapy. Muscle-invasive bladder cancer presents a significant therapeutic challenge, and many patients, particularly the elderly or frail ones, are unable to undergo standard curative-intent therapies. In response to this unmet need, TAR-200, a system that delivers gemcitabine directly to the bladder continuously over a 21-day dosing cycle, was developed. The study included patients with cT2-cT3bN0M0 urothelial bladder cancer who received four consecutive cycles of therapy for a total of 84 days. The primary endpoints of the study were the assessment of the safety and tolerability of TAR-200 at 84 days. Additionally, clinical complete and partial response rates were assessed, which were verified by cystoscopy, biopsy, and imaging techniques, as well as the duration of response and overall survival. The study included 35 patients, 68.6% of whom were male, with a median age of 84 years. Treatment-related adverse events occurred in 15 patients, 2 of whom required removal of TAR-200. After 3 months of treatment, a complete response was observed in 31.4% of patients and partial response in 8.6%, for a combined response rate of 40.0%. Median overall survival was 27.3 months, and the median duration of response was 14 months. In addition, the progression-free rate at 12 months was 70.5%. The results of this study suggest that TAR-200 is generally safe and well tolerated in older, frail patients and shows promising initial efficacy in a patient population with very limited treatment options [125].
A study investigating the effect of μ-opioid receptor agonists (MORA) on the progression and metastasis of bladder cancer (BCa) provided important insight into the potential mechanisms underlying these processes and suggested potential therapeutic directions. MORA, commonly used to relieve pain in BC patients both during surgery and for chronic pain management, has been shown to influence the generation of circulating tumor cells (CTCs), which in turn contributes to the enhancement of metastasis. This study used both preclinical models and patient studies to specifically investigate the effect of MORA on neoplastic processes. A novel microfluidic immunocapture microchip was used to detect changes in CTC numbers in both mouse models and BC patients. The results showed a significant increase in the number of CTCs with epithelial and/or mesenchymal features after MORA treatment. Using advanced bioinformatics methods, whole transcriptome sequencing, and molecular biology techniques, the MOR/PI3K/AKT/Slug signaling pathway was identified as a key mechanism responsible for this effect. Activation of this pathway promoted epithelial-to-mesenchymal transition (EMT) of cancer cells, which facilitated their migration and CTC formation. In turn, interventions blocking MOR, Slug, or PI3K inhibited EMT and reduced the number of CTCs, suggesting that the MOR/AKT/Slug axis may be a potential therapeutic target. The results of this study indicated that despite the benefits of the analgesic effects of MORAs, their use may contribute to an increased risk of metastasis by promoting the formation of circulating tumor cells. Therefore, in future clinical interventions, it would be possible to target the EMT-CTC pathway to reduce the negative effects of MORAs without losing their analgesic effects [126].
The RAIDER study evaluated the acute toxicity of different radiotherapy regimens used in the treatment of bladder cancer, focusing on the comparison of hypofractionated fractionation (55 Gy in 20 fractions) with conventional fractionation (64 Gy in 32 fractions) and the effect of concomitant (chemo)therapy. In the randomized clinical trial, patients with muscle-invasive bladder cancer stage T2–T4a N0 M0 were assigned to one of three groups: standard radiotherapy, standard-dose adaptive radiotherapy, or dose-increased adaptive radiotherapy. Neoadjuvant and concomitant chemotherapy were allowed, which allowed for the analysis of the effect of different treatment regimens on the occurrence of acute adverse events. The study included 345 patients, recruited from 46 centers, who received 20 or 32 fractions of radiotherapy. The median age of participants was 73 years, and 49% of patients had received prior neoadjuvant chemotherapy. Additionally, 71% of patients were treated with concurrent therapy, with the most common being 5-fluorouracil plus mitomycin C. Acute toxicity, graded using the Common Terminology Criteria for Adverse Events (CTCAE), was monitored weekly during radiotherapy and 10 weeks after treatment initiation. The results of the analysis showed that grade 2 or higher gastrointestinal toxicity was significantly higher in patients receiving concurrent therapy compared with radiotherapy alone in the 20-fraction cohort, but similar differences were not observed in the 32-fraction cohort. The highest gastrointestinal toxicity was observed in patients treated with gemcitabine, confirming the significant differences between treatment groups in the 32-fraction cohort. In terms of grade 2 or higher urinary tract toxicity, no significant differences were found between different concomitant therapy regimens in both the 20-fraction and 32-fraction cohorts. This study highlights that acute grade 2 or higher toxicity is a common phenomenon in radiotherapy for bladder cancer, and the adverse event profile varies depending on the concomitant therapy regimen used. In particular, gastrointestinal toxicity seems to be more severe in patients receiving gemcitabine, which indicates the need for further studies to optimize treatment in this group of patients [127].
Another clinical trial evaluated the safety and efficacy of OncoTherad® (MRB-CFI-1) nano-immunotherapy in patients with non-muscle-invasive bladder cancer (NMIBC) who had failed to respond to prior treatment with Bacillus Calmette–Guérin (BCG). This single-arm, phase I/II study included 44 patients, of whom 59.1% were BCG-resistant, 31.8% had relapsed disease, and 9.1% were BCG-intolerant. The primary efficacy measures were the pathological complete response (pCR) rate and relapse-free survival (RFS), while secondary measures included the duration of response and safety. After 24 months of follow-up, the pCR rate was 72.7% and the median RFS was 21.4 months. In the group of patients who achieved pCR, the median duration of response was 14.3 months. Of note, no patient developed muscle-invasive cancer or metastatic disease during treatment. Treatment-related adverse events were reported in 77.3% of patients, with mostly grade 1–2 adverse events, indicating good tolerability of the treatment. In terms of the mechanism of action, OncoTherad® demonstrated the ability to activate the innate immune system via the toll-like receptor 4 (TLR4) signaling pathway, which in turn led to increased activity of the interferon pathway. This activation was crucial for the stimulation of CX3CR1+ CD8 T cells, which was associated with reduced expression of immune checkpoint molecules and reversal of immunosuppression in the bladder tumor microenvironment. The results of the study suggest that OncoTherad® is a safe and effective treatment option for patients with NMIBC who are BCG-refractory and may also have potential benefits in preventing tumor relapse [128].
In a population-based study based on the Surveillance, Epidemiology, and End Results (SEER), and external validation using data from The Cancer Genome Atlas (TCGA), prognostic nomograms were developed and validated for patients with bladder cancer (BCa). The aim of the study was to compare the prognostic value of different lymph node metastasis (LNM) indices and to develop prognostic tools that could aid clinical treatment decisions. The study identified 10,093 patients with bladder cancer from the SEER database and 107 patients from the TCGA database. The data were used to create multivariate Cox regression models comparing the predictive performance of indices, such as N classification, number of positive lymph nodes (PLN), lymph node ratio (LNR), and log odds of positive lymph nodes (LODDS). The results of the analysis showed that the LODDS score had a higher prognostic performance than the other indices in terms of both overall survival (OS) and cause-specific survival (CSS). Based on the results, variables such as age, LODDS, and T and M classifications were included in the OS nomograms, while the CSS nomograms included gender, tumor stage, LODDS, and T and M classifications. These nomograms were validated for their prognostic accuracy and clinical utility in three independent cohorts. Furthermore, analysis of the tumor microenvironment revealed significant differences between risk groups, suggesting that different immune profiles may influence patient prognosis. In summary, the study demonstrated that the LODDS score is superior to traditional lymph node metastasis indices in terms of the prognostic value for patients with bladder cancer. The incorporation of LODDS into prognostic nomograms can significantly improve the accuracy of prognostication, thus supporting clinical decision-making [129]. The next study assessed the performance of radiomic signatures in detecting lymph node (LN) metastases in patients with bladder cancer (BCa), which is crucial for determining the optimal treatment plan. This study investigated the differences in diagnostic performance between manual and automated segmentation of LNs on computed tomography (CT) images. Among 1354 BC patients who underwent radical cystectomy with lymph node dissection, 391 patients were included in the study and had pathological determination of LN status (pN0: n = 297; pN+: n = 94). Patients were randomly divided into two groups: training (n = 274) and test (n = 117). Pelvic LN segmentation was performed both manually and automatically. From each node, 1004 radiomic features were extracted and used to train a machine learning model to predict lymph node (pN) status based on histopathological results. The results obtained by radiomic analysis based on manual and automated segmentation were compared with the assessment performed by radiologists. The receiver operating characteristic (ROC) curve method was used to assess sensitivity, specificity, and area under the curve (AUC). In the test group, manually segmented lymph nodes achieved an AUC of 0.80 (95% CI 0.69–0.91, p = 0.64), while automated segmentation achieved an AUC of 0.70 (95% CI 0.58–0.82, p = 0.17). These results were compared with the radiologist’s assessment, for which the AUC was 0.78 (95% CI 0.67–0.89). Combining the radiomic signature based on manual segmentation with the radiological assessment achieved an AUC of 0.81 (95% CI 0.71–0.92, p = 0.63). The study showed that the radiomic signature can be an effective tool for distinguishing lymph node status in BC patients, with manual segmentation outperforming the automated approach in terms of diagnostic accuracy. The results suggest that integrating radiomic techniques with traditional radiological assessment can lead to improved disease staging, which is important for further therapeutic decisions [130].
Another clinical trial aimed to evaluate the therapeutic effect of the combination of Kushen (CKI) and gemcitabine in postoperative patients with non-muscle-invasive bladder cancer (NMIBC) and to investigate the effect of this treatment on selected serum factors and the immune system. The study included 150 patients who were randomly divided into 2 groups. The control group (n = 75) received standard gemcitabine therapy, which consisted of 0.2 g of gemcitabine once a week for eight weeks after surgery, followed by continuation of treatment in a cycle every two weeks for eight subsequent applications. The observation group (n = 75) was treated with a CKI injection for 10 days in each of 3 cycles of therapy, in addition to gemcitabine. The study lasted two years, during which blood biochemical parameters, serum factor levels, and changes in T-cell subsets were monitored, as well as the safety of the therapy and the functioning of the immune system. The results indicated that patients in both groups had a significant increase in the levels of interferon-γ, interleukin-2 (IL-2), cell adhesion molecules (CAMs), hepatocyte CAMs, and cysteine proteinase-8 after the end of therapy. This increase was more pronounced in the observation group. At the same time, there was a significant decrease in the levels of tumor necrosis factor-α (TNF-α), C-reactive protein (CRP), IL-6, and other inflammatory and adhesion markers, such as metalloproteinases (MMP-9 and MMP-2), E-cadherin, epithelium-specific CAMs, soluble CAM-1, hepatic CAMs, vascular endothelial growth factor (VEGF), and fibroblast growth factor (FGF). The decrease in these parameters was also more pronounced in the group of patients receiving additional CKIs. Moreover, a significant decrease in the frequency of disease relapses and adverse events was observed in the observation group compared to the control group. The study results suggest that combining CKI therapy with gemcitabine may not only effectively alleviate clinical symptoms and reduce the inflammatory response, but also improve the safety of treatment, reducing the risk of adverse events and improving the overall efficacy of treatment in patients with NMIBC [131].
Table 9.
Summary of clinical trials in bladder cancer [117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136], 2020–2024.
Table 9.
Summary of clinical trials in bladder cancer [117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136], 2020–2024.
| Year | References | Study Phase | Key Findings |
|---|---|---|---|
| 2020 | [117] | Phase 3 | The POUT trial showed that adjuvant chemotherapy with gemcitabine and platinum initiated within 90 days post-nephrectomy significantly improved disease-free survival (DFS) in upper urinary tract urothelial carcinoma patients compared to observation. |
| 2020 | [118] | Phase 3 | Avelumab maintenance therapy significantly prolonged overall survival in advanced urothelial cancer patients who did not progress after first-line chemotherapy, particularly in PD-L1-positive patients. |
| 2020 | [119] | Randomized | The HYBRIDBLUE trial demonstrated that transurethral en bloc resection with submucosal hydro-dissection (TUEB) was superior to standard TURBT for histopathological assessment in non-muscle-invasive bladder cancer. TUEB achieved more accurate muscle invasion assessment and higher rates of complete tumor removal with fewer complications. |
| 2020 | [120] | Phase 1 | The SAKK 06/14 study of VPM1002BC for non-muscle-invasive bladder cancer patients who failed BCG therapy demonstrated safety and induced a strong immune response. |
| 2020 | [121] | Phase 1–2 | BioXmark® liquid markers demonstrated high visibility and positional stability during image-guided radiotherapy for invasive bladder cancer, improving treatment precision without related adverse events. |
| 2020 | [122] | Phase 3 | The use of intraoperative warmed fluids during robot-assisted radical cystectomy reduced the risk of hypothermia, decreased blood transfusions, and shortened hospitalization. |
| 2020 | [123] | Phase 2 | IMRT in patients with node-positive bladder cancer (NPBC) and high-risk node-negative bladder cancer (NNBC) was feasible, with low toxicity, low recurrence rates, and potential for long-term disease control. |
| 2020 | [124] | Phase 3 | The KEYNOTE-045 trial demonstrated durable antitumor activity of pembrolizumab in advanced urothelial cancer patients who failed prior platinum-based chemotherapy, with better tolerance and fewer adverse events compared to chemotherapy. |
| 2020 | [125] | Randomized | High-intensity interval training (HIIT) significantly improved exercise capacity (VO2AT) and reduced blood pressure in older patients before major urological surgery, suggesting better cardiovascular health and potential for improved surgical outcomes. |
| 2020 | [126] | Prospective | The NCT03998371 trial developed UroCAD, a non-invasive diagnostic method for urothelial cancer based on whole-genome sequencing of exfoliated urine cells, achieving better sensitivity and specificity than traditional cytological tests. |
| 2021 | [127] | Phase 3 | Nadofaragen firadenovec, a novel gene therapy, achieved a 53.4% complete response rate in BCG-refractory non-muscle-invasive bladder cancer patients within 3 months, offering a new treatment option. |
| 2021 | [128] | Phase 3 | The GETUG/AFU V05 VESPER trial showed that dose-escalated chemotherapy with dd-MVAC improved local control in muscle-invasive bladder cancer compared to the GC regimen, though it was associated with more severe toxicity. |
| 2021 | [129] | Observational | SNPs of lncRNA TINCR were associated with increased or decreased risk of bladder cancer, depending on the variant, with polymorphisms affecting the expression of miRNAs, indicating potential regulatory mechanisms. |
| 2021 | [130] | Randomized | HoLRBT was shown to be as effective as TURBT in treating NMIBC, with fewer complications and shorter catheterization and hospitalization times. |
| 2021 | [131] | Randomized | En bloc resection with green light laser was superior to traditional TURBT for non-muscular bladder cancer in reducing obturator reflex and blood loss, providing better-quality histopathological samples. |
| 2021 | [132] | Phase 3 | The VESPER trial compared GC and dd-MVAC chemotherapy regimens, showing that four cycles of cisplatin-based chemotherapy before cystectomy is sufficient for optimal pathological outcomes without significant deterioration in renal function. |
| 2021 | [133] | Phase 2 | RC48-ADC, a HER2-targeted antibody–drug conjugate, achieved a 51.2% ORR in HER2+ advanced urothelial cancer patients with a median OS of 13.9 months, showing promising efficacy and safety. |
| 2021 | [134] | Phase 3 | A 14-miRNA hypoxia signature was developed and validated, showing prognostic value in bladder cancer patients receiving carbogen and nicotinamide combined with radiotherapy, improving local recurrence-free survival. |
| 2021 | [135] | Retrospective | A predictive model for lymph node invasion (LNI) in extended lymph node dissection (PLND) was developed, showing moderate prediction accuracy (AUC 73%) and suggesting the need for better patient selection for extended PLND. |
| 2021 | [136] | Randomized | Plan-of-the-Day (POD) adaptive radiotherapy in muscle-invasive bladder cancer reduced severe nongenitourinary toxicity (6% vs. 13%) and achieved good local disease control at 3 months (81.3%). |
| 2022 | [137] | Phase 3 | The BC2001 study indicated that adding chemotherapy (fluorouracil and mitomycin C) to radiotherapy for muscle-invasive bladder cancer improves locoregional control and decreases the need for cystectomy. |
| 2022 | [138] | Randomized | Diabetic patients using metformin had better overall survival and disease-specific survival compared to non-metformin users and nondiabetic patients with non-muscle-invasive bladder cancer treated with BCG. |
| 2022 | [139] | Observational | APPv application for NMIBC treatment adherence showed improved treatment outcomes when its recommendations were followed, especially in high-risk and very high-risk patients. |
| 2022 | [140] | Prospective | The ADXBLADDER test effectively detected high-grade recurrence in low-grade non-muscle-invasive bladder cancer, potentially reducing the need for invasive surveillance cystoscopy. |
| 2022 | [141] | Randomized | Levofloxacin combined with intravesical BCG therapy reduced the severity of frequent urination and fever while improving long-term progression-free survival and cancer-specific survival in NMIBC patients. |
| 2022 | [142] | Phase 1/2 | LSAM-DTX showed promising safety, efficacy, and immune response in high-risk non-muscle-invasive bladder cancer patients, with prolonged recurrence-free survival in higher-dose groups and minimal systemic exposure. |
| 2022 | [143] | Phase 2b | The Optima II trial demonstrated that UGN-102, a chemoablative gel with mitomycin, was a safe and effective non-surgical treatment for NMIBC, with high patient satisfaction and no significant worsening of urinary symptoms. |
| 2022 | [144] | Randomized | Coated silicone catheters with biofilm-inhibiting technology showed lower bacterial colonization compared to standard Foley catheters in patients after radical cystectomy, though CAUTI rates were similar in both groups. |
| 2022 | [145] | Prospective | Low serum 25-hydroxyvitamin D levels were significantly associated with bladder cancer, especially the muscle-invasive form, but did not show significant prognostic value for recurrence in NMIBC. |
| 2022 | [146] | Phase 1 | Oncofid-P-B showed high safety and efficacy in patients with carcinoma in situ (CIS) of the bladder who did not respond to BCG treatment, with 75% achieving complete response (CR) after 12 weeks and 40% maintaining CR after 12 months. |
| 2023 | [147] | Phase 3 | Erdafitinib significantly improved overall survival and progression-free survival compared to chemotherapy in metastatic urothelial cancer patients with FGFR2/3 alterations who had previously received checkpoint inhibitors. |
| 2023 | [148] | Randomized | Vitamin E supplementation increased the risk of relapse in NMIBC patients, while selenium supplementation showed no significant effect in preventing recurrence or progression of the disease. |
| 2023 | [149] | Prospective | cfDNA methylation signatures were predictive of response to neoadjuvant chemotherapy in muscle-invasive bladder cancer, with a methylation response index (mR-score) correctly predicting pathological response in 79% of patients. |
| 2023 | [150] | Phase 1 | The TAR-200 drug delivery system demonstrated safety, tolerability, and a 40% response rate in patients with muscle-invasive bladder cancer who were ineligible for or declined curative-intent therapies. |
| 2023 | [151] | Preclinical/Patient study | μ-opioid receptor agonists (MORA) were shown to increase circulating tumor cells in bladder cancer patients, potentially promoting metastasis via the MOR/AKT/Slug signaling pathway. |
| 2023 | [152] | Randomized | The RAIDER study highlighted that acute grade 2 or higher toxicity is common during radiotherapy for bladder cancer. Gastrointestinal toxicity was more severe in patients receiving concurrent gemcitabine therapy compared to other regimens. No significant differences in urinary tract toxicity were found between regimens. |
| 2023 | [153] | Phase 1/2 | OncoTherad® (MRB-CFI-1) nanoimmunotherapy demonstrated a 72.7% pathological complete response (pCR) rate in BCG-refractory NMIBC patients, with a median relapse-free survival of 21.4 months. The treatment was well tolerated, with mostly mild to moderate adverse events. The mechanism of action involved activation of the TLR4 and interferon pathways, enhancing CD8+ T-cell activity and reversing immunosuppression in the tumor microenvironment. |
| 2023 | [154] | Population-based | A study based on SEER and TCGA databases developed and validated prognostic nomograms for bladder cancer patients. The LODDS (log odds of positive lymph nodes) score showed superior prognostic performance over traditional lymph node metastasis indices in predicting both overall survival (OS) and cause-specific survival (CSS). Incorporating LODDS into nomograms significantly improved the accuracy of prognostication and could aid in clinical decision-making. |
| 2023 | [155] | Diagnostic | A radiomics study assessing manual versus automated lymph node segmentation in bladder cancer patients found that manual segmentation outperformed automated segmentation, achieving an AUC of 0.80 compared to 0.70. Combining manual radiomic analysis with traditional radiological assessment improved lymph node metastasis detection, enhancing diagnostic accuracy and disease staging for further therapeutic decisions. |
| 2023 | [156] | Randomized | A clinical trial evaluating the combination of Kushen (CKI) and gemcitabine in postoperative NMIBC patients demonstrated a greater reduction in inflammatory markers (TNF-α, CRP, and IL-6) and a more pronounced increase in immune response markers (IFN-γ and IL-2) compared to gemcitabine alone. CKI also improved treatment safety, reduced the frequency of relapses, and alleviated clinical symptoms. |
| 2024 | [157] | Phase 2 | A phase II study investigating the COXEN gene expression model found that molecular subtypes of muscle-invasive bladder cancer (basal squamous, luminal, and neuronal) were modest predictors of pathological response to neoadjuvant chemotherapy, with limited impact on long-term outcomes, such as progression-free survival (PFS) and overall survival (OS). Further research is needed to understand their role as predictive biomarkers. |
| 2024 | [158] | Phase 1b | The PrECOG PrE0807 study evaluated the safety and efficacy of neoadjuvant nivolumab, with or without lirilumab, in cisplatin-ineligible patients with muscle-invasive bladder cancer (MIBC). Nivolumab-based neoadjuvant immunotherapy was well tolerated, with a 2-year relapse-free survival of 73–71% and overall survival of 82–89%. The combination therapy significantly increased CD8+ T-cell density, indicating potential immune activation. |
| 2024 | [159] | Phase 1 | A phase I study combining sacituzumab govitecan (SG) and enfortumab vedotin (EV) for metastatic urothelial cancer showed a 70% objective response rate, including three complete responses. Maximum tolerated doses were determined, and treatment was generally well tolerated with support from G-CSF. These promising results suggest potential for further studies. |
| 2024 | [160] | Phase 2 | Disitamab vedotin (RC48-ADC) demonstrated a 50.5% objective response rate in patients with HER2-positive locally advanced or metastatic urothelial cancer, with a median progression-free survival of 5.9 months and overall survival of 14.2 months. The treatment was well tolerated with manageable adverse events, making it a promising therapy for this patient population. |
| 2024 | [161] | Phase 2 | The LUX-Bladder 1 trial evaluated afatinib, an irreversible ErbB family inhibitor, in patients with ERBB1–3 mutations in advanced urothelial cancer. The objective response rate was 5.9–12.5%, and progression-free survival was 9.8–7.8 weeks. Tumors with ERBB2 amplification or the basal-squamous phenotype showed better responses. Common adverse events included diarrhea, with 9.5% of patients experiencing grade 3 events. |
3.8.3. Selected Clinical Trials from 2024
A phase II study evaluated the association of molecular subtypes with pathologic response, progression-free survival (PFS), and overall survival (OS) in patients with muscle-invasive bladder cancer treated with neoadjuvant chemotherapy (NAC). The aim of the study was to use the COXEN (Co-expression Extrapolation) gene expression model to identify patients who would best respond to NAC. The COXEN model included specific results for two chemotherapy regimens: methotrexate, vinblastine, adriamycin, and cisplatin (ddMVAC) and gemcitabine/cisplatin (GC). The study included 237 patients who were randomly assigned to receive 4 cycles of ddMVAC (51% of patients) or GC (49% of patients). Based on transcriptomic data obtained from the Affymetrix platform, patients were divided into molecular subtypes using three classifiers: TCGA (five subtypes), Consensus (six subtypes), and MD Anderson (three subtypes). The aim of the analysis was to assess whether molecular subtypes could predict response to NAC and whether they increased the predictive value of the COXEN model. Of the participants, 155 patients had available gene expression data, had received at least 3 of 4 NAC cycles, and underwent radical cystectomy, which allowed for the assessment of pathological response. The analysis noted that the TCGA classifier divided into three groups (basal squamous, neuronal, and luminal infiltrating) and the COXEN score for the GC regimen showed the highest values of the area under the curve (AUC) for complete pathological response (pT0). In contrast, the Consensus classifier, which had three subtype categories (basal squamous/neuroendocrine, luminal, and stroma-rich), slightly improved the prediction of pathological downstaging (<pT2). The AUC increased from 0.57 (using only stratification factors) to 0.61, suggesting a modest benefit from adding this classifier. Despite these results, no statistically significant associations were observed between molecular subtypes and progression-free survival (PFS) or overall survival (OS). The results of the study suggest that although molecular subtypes may have some prognostic value in terms of pathological response to chemotherapy, they do not show strong correlations with long-term clinical outcomes, such as PFS and OS. The conclusions of the study indicate the need for further research to better understand the role of molecular subtypes as predictive biomarkers in the treatment of bladder cancer [132].
The PrECOG PrE0807 study is a phase 1b study designed to evaluate the feasibility and safety of neoadjuvant nivolumab, either as monotherapy or in combination with lirilumab, in patients with muscle-invasive bladder cancer (MIBC) who are ineligible for or refuse cisplatin-based chemotherapy. Neoadjuvant cisplatin-based chemotherapy before radical cystectomy (RC) has been shown to improve overall survival in MIBC, but many patients are unable to receive this treatment, creating a need to seek alternative therapies. In the study, patients with cT2-4aN0-1M0 MIBC who were ineligible for cisplatin were administered two doses of nivolumab (480 mg) before RC. Patients were divided into two cohorts: the first received nivolumab alone, and the second received the combination of nivolumab with lirilumab (240 mg). The primary objective of the study was to determine the incidence of grade 3 or higher treatment-related adverse events (TRAEs) according to the Terminology Criteria for Adverse Events (CTCAE) version 5.0. Additionally, the proportion of patients who underwent RC more than 6 weeks after the last dose of treatment, changes in CD8+ T-cell density between transurethral resection of bladder tumor (TURBT) and RC, ypT0N0 and <ypT2N0 rates, and 2-year relapse-free survival (RFS) and overall survival (OS) were analyzed. The study included 43 patients, 41 of whom underwent planned RC. There was no grade 3 TRAE in the nivolumab monotherapy group, whereas grade 3 TRAEs occurred in 7% of patients in the combination group, but all of these events resolved, and no grade 4 or 5 TRAEs were reported. There were also no delays in RC beyond 6 weeks. The ypT0N0 rates were 17% and 21% in the two cohorts, respectively, and the <ypT2N0 rates were 25% and 32%. The two-year relapse-free survival was 73% and 71%, and the two-year overall survival was 82% and 89%, respectively. Importantly, a significant increase in CD8+ T-cell density was observed in the nivolumab plus lirilumab cohort. The study showed that nivolumab-based neoadjuvant immunotherapy was well tolerated and safe in patients with MIBC who were not eligible for cisplatin. Although the ypT0N0 rates were lower than in other studies, the two-year survival rates were comparable to those in other studies of neoadjuvant immunotherapy. These results suggest that nivolumab may be an effective alternative for patients who are ineligible for cisplatin-based chemotherapy, which is currently being studied in another clinical trial (NCT03661320) [133].
Another phase I study evaluated the safety and efficacy of combining two antibody–drug conjugates (ADCs): sacituzumab govitecan (SG) and enfortumab vedotin (EV), in the treatment of metastatic urothelial cancer (mUC). Both SG and EV are standard monotherapies in the treatment of mUC, but because of their different mechanisms of action and molecular targets, we decided to investigate whether their combination could provide additional clinical benefit. The study included patients with metastatic urothelial cancer who had disease progression despite prior platinum-based therapy and/or immunotherapy. A key inclusion criterion was having an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1, meaning that patients had to be in relatively good general condition. The therapy consisted of the administration of a combination of SG and EV on days 1 and 8 of a 21-day cycle. Treatment was continued until disease progression or toxicity that prevented further treatment. The primary objective of the study was to assess the incidence of dose-limiting toxicities (DLTs) during the first treatment cycle, with the aim of establishing the maximum tolerated dose (MTD) for this therapeutic regimen. The study used a Bayesian Optimal Interval model, which allows for flexible dose adjustments depending on adverse events. Response rates (ORR), progression-free survival (PFS), and overall survival (OS) were also assessed. Between May 2021 and April 2023, 24 patients were enrolled in the study, 23 of whom started therapy. The median age was 70 years, and 11 patients had received at least 3 prior lines of therapy. Grade 3 or higher adverse events occurred in 78% of patients (18/23) regardless of the assigned dose, including one fatal event (pneumonia, probably related to enfortumab vedotin). Based on the data obtained, the recommended doses for Phase II are 8 mg/kg for SG and 1.25 mg/kg for EV, respectively, with additional support from granulocyte-stimulating factor (G-CSF). The maximum tolerated doses were established at 10 mg/kg for SG and 1.25 mg/kg for EV. The objective response rate was 70%, with 16 patients achieving a response (95% confidence interval: 47–87%), including 3 complete responses. Three patients had disease progression as their best response. The median follow-up was 14 months, and 9 patients had ongoing responses, including 6 for more than 12 months. In conclusion, the combination of sacituzumab govitecan and enfortumab vedotin in the treatment of metastatic urothelial cancer showed promising results, especially in terms of high response rates and a significant number of complete clinical responses. These results suggest the therapeutic potential of this combination and indicate the need for further studies in subsequent clinical phases [134].
A clinical trial evaluated the efficacy and safety of disitamab vedotin (DV, RC48-ADC), a novel humanized antibody against human epidermal growth factor receptor 2 (HER2), in patients with locally advanced or metastatic urothelial cancer (UC) that overexpressed HER2. Disitamab vedotin, an antibody conjugate of the cytotoxic monomethyl auristatin E, was evaluated in two open-label, multicenter, single-arm phase II studies (RC48-C005 and RC48-C009). The studies included patients with HER2-positive urothelial cancer that had progressed after at least one line of systemic chemotherapy. HER2 positivity was defined as an immunohistochemical score of 3+ or 2+. Patients received DV at a dose of 2 mg/kg every other week as an intravenous infusion. The primary endpoint was the objective response rate (ORR), which was assessed by an independent expert review committee (BIRC). Additionally, progression-free survival (PFS), overall survival (OS), and the safety profile of the drug were analyzed. A total of 107 patients were included in the study. The ORR was confirmed to be 50.5% (95% CI 40.6–60.3), indicating promising efficacy of the drug. These results were consistent across subgroups, including patients with liver metastases and those previously treated with checkpoint inhibitors (PD-1/PD-L1). The median duration of response was 7.3 months (95% CI 5.7–10.8), and the median PFS and OS were 5.9 months (95% CI 4.3–7.2) and 14.2 months (95% CI 9.7–18.8), respectively. The most common treatment-related adverse events included peripheral sensory neuropathy (68.2%), leukopenia (50.5%), aspartate aminotransferase (AST) elevation (42.1%), and neutropenia (42.1%). Grade 3 or higher adverse events occurred in 54.2% of patients, with the most common being sensory neuropathy (18.7%) and neutropenia (12.1%). The study showed that disitamab vedotin has significant efficacy and an acceptable safety profile in the treatment of patients with locally advanced or metastatic HER2-positive urothelial cancer who had failed prior systemic therapies. The results suggest that DV may be an important treatment option in this group of patients [135]. A phase II clinical trial (LUX-Bladder 1, NCT02780687) evaluated the efficacy and safety of afatinib, an irreversible ErbB family inhibitor, in patients with advanced urothelial cancer with ERBB1–3 mutations. The study was open-label, single-arm, and participants received afatinib at a dose of 40 mg once daily as a second-line treatment. The primary objective of the study was to assess 6-month progression-free survival (PFS6) in patients with metastatic urothelial cancer. The study included 34 patients in cohort A and 8 patients in cohort B. The results showed that the PFS6 rate was 11.8% in cohort A and 12.5% in cohort B, respectively. The objective response rate (ORR) was 5.9% in cohort A and 12.5% in cohort B, and the disease control rate (DCR) was 50.0% and 25.0%, respectively. The median progression-free survival (PFS) was 9.8 weeks in cohort A and 7.8 weeks in cohort B, and the median overall survival (OS) was 30.1 weeks and 29.6 weeks, respectively. The study observed a partial response in three patients, two of whom had ERBB2 amplification in cohort A and one with EGFR amplification in cohort B. Despite promising results in some patients, phase 2 of the study in cohort A was not conducted due to lack of sufficient antitumor activity at interim analysis. In terms of safety, all patients experienced adverse events, most commonly diarrhea, which occurred in 76.2% of patients, 9.5% of whom had grade 3 diarrhea. Two treatment discontinuations were related to adverse events, and one adverse event resulted in death due to acute coronary syndrome, although this event was not considered treatment related. Biomarker analysis showed that tumors with a basal-squamous phenotype and those with ERBB2 amplification may have a better response to afatinib, suggesting the need for further investigation in these patient subgroups [136].
3.9. Analysis of Limitations and Challenges in Bladder Cancer Diagnosis and Treatment
Survival rates vary depending on the type of bladder cancer. Five-year survival is 96% for in situ carcinoma but drops to 5% for distant metastases (Table 10) [162].
Table 10.
Bladder cancer survival chart by stage.
3.9.1. Biomarkers
Biomarkers, such as FGFR3, TP53, NMP22, BTA, or UroVysion, are increasingly commonly used in bladder cancer diagnosis, but their effectiveness is not without drawbacks. For example, FGFR3 (fibroblast growth factor receptor 3) is one of the best-studied biomarkers associated with bladder cancer, but its effectiveness is mainly limited to low-grade tumors. This biomarker is rarely present in more aggressive, advanced forms of cancer, which makes its prognostic value limited. In addition, tests such as NMP22 and BTA are prone to false-positive results, especially in cases of urinary tract infection or inflammation. This limits their usefulness in routine diagnostics, especially in patients with comorbidities, where additional tests are necessary to confirm the diagnosis. UroVysion (FISH-based test), although precise, is expensive and time-consuming, which hinders its widespread use in clinical practice. Future research should focus on identifying panels of biomarkers that may include different molecular pathways, such as miRNA signaling or mutator gene expression. Combining several biomarkers could increase diagnostic sensitivity and specificity, as well as enable prediction of response to specific therapies, such as immunotherapy.
3.9.2. Therapies
Neoadjuvant chemotherapy, although the standard of care for muscle-invasive bladder cancer, is associated with numerous side effects and does not always lead to complete pathological response. Even patients who have successfully achieved pT0 disease may experience relapses. Furthermore, limited access to chemotherapy or immunotherapy may lead to inequalities in treatment outcomes, especially in less developed countries. The development of resistance to therapies, such as chemotherapy or immunotherapy, is also a major challenge. For example, immunotherapy with checkpoint inhibitors, such as atezolizumab or nivolumab, has shown promising results in patients with advanced bladder cancer, but not all patients respond to such treatments, and some develop resistance after an initial response. Emerging research should focus on identifying biomarkers of response to immunotherapy that can help predict which patients will benefit from this treatment. In the context of personalized therapies, genomic studies could enable better tailoring of treatment to specific cancer mutations. Targeted therapies, such as FGFR or PARP inhibitors, are promising areas that should be further explored in combination with other treatments.
3.9.3. Future Research Directions
In response to current challenges, future research should focus on several key areas:
- Development of non-invasive biomarker technologies, such as analysis of circulating tumor DNA (ctD-NA) in body fluids, which could enable monitoring of bladder cancer progression and assessment of therapy efficacy without the need for invasive procedures.
- Introduction of multi-agent therapies, which could include a combination of targeted therapies, immunotherapy, and radiotherapy to minimize tumor resistance.
- Studies of the tumor microenvironment (e.g., the role of regulatory T cells and tumor-associated macrophages), which could enable the development of new immunomodulatory therapies.
The application of omics (genomics, proteomics, and metabolomics) in bladder cancer research could lead to the identification of new therapeutic targets and diagnostic markers, which would significantly improve patient outcomes. Combined with developments in digital technologies, such as big data and machine learning, future research could enable a more individualized approach to the diagnosis and treatment of bladder cancer.
4. Conclusions
Bladder cancer (BCa) is the most common malignancy of the urinary system and the fourth most common cancer in men, especially after the age of 45, with the highest incidence in the age group of 80–84 years (Table 11).
Table 11.
Characterization of bladder cancer causes.
In 2021, approximately 573,000 new cases were diagnosed worldwide, of which 75% were non-muscle-invasive (NMIBC) and the remaining 25% were muscle-invasive (MIBC). Morbidity and mortality rates vary geographically, with higher rates in Europe, North America, and Australia and lower rates in Asia and Africa. High risk factors include tobacco smoking, chemical exposure, and chronic urinary tract infections. Tobacco smoking increases the risk of bladder cancer by about 50%, and long-term smoking increases this risk even further. Modern diagnostics are based on imaging methods, such as cystoscopy, computed tomography, or intravenous urography, as well as histopathological examinations obtained after transurethral resection of the tumor (TURBT). Early detection of the tumor is crucial for the effectiveness of treatment, which depends on the stage of the disease. Modern therapeutic approaches include surgery, chemotherapy, immunotherapy, and molecularly targeted therapies. In non-invasive forms of the disease (NMIBC), TURBT treatment is preferred, with the possibility of using intravesical therapy, such as BCG (Bacillus Calmette–Guérin). In advanced cases, especially in the muscle-invasive stage, radical cystectomy is often used in combination with neoadjuvant or adjuvant chemotherapy. In clinical trials on new methods of BCa treatment, special attention is paid to immunotherapy, including checkpoint inhibitors, which show promising results in improving the survival of patients with advanced disease. Molecularly targeted therapies based on specific genetic mutations are becoming increasingly common, offering hope for a more personalized approach to bladder cancer treatment. To further improve the prognosis and efficacy of bladder cancer treatment, it is crucial to focus on several strategic areas. First, the development of less invasive and more precise diagnostic tests, such as narrowband imaging (NBI) or photodynamic diagnostics (PDD), could contribute to wider use of screening, especially in high-risk groups, such as smokers. Second, improving the availability of modern therapies, such as immunotherapy and molecularly targeted therapies, especially in low-resource countries, could significantly improve survival rates. Also, introducing more widespread genetic testing for bladder cancer patients could contribute to better tailoring therapy to individual needs, which in turn would increase treatment efficacy and reduce side effects. In terms of prevention, continuing and intensifying anti-smoking programs, especially in developing countries, can significantly reduce the number of new cases. Future prospects include further development of new drugs, research on the effectiveness of combination therapies, and investment in biomarker research that can contribute to more precise diagnostics and monitoring of treatment responses. Improving international cooperation in clinical trials and better funding for research can bring significant progress in bladder cancer treatment on a global scale.
Author Contributions
Conceptualization, D.G., S.C., D.B.-A. and D.A.; methodology, D.G., S.C., D.B.-A. and D.A.; software, D.G., S.C., D.B.-A. and D.A.; validation, D.G., S.C., D.B.-A. and D.A.; formal analysis, D.G., S.C., D.B.-A. and D.A.; investigation, D.G., S.C., D.B.-A. and D.A.; resources, D.G., S.C., D.B.-A. and D.A.; data curation, D.G., S.C., D.B.-A. and D.A.; writing—original draft preparation, D.G., S.C., D.B.-A. and D.A.; writing—review and editing, D.G., S.C., D.B.-A. and D.A.; visualization, D.G., S.C., D.B.-A. and D.A.; supervision, D.G., S.C., D.B.-A. and D.A.; project administration, D.G., S.C., D.B.-A. and D.A.; funding acquisition, D.G., S.C., D.B.-A. and D.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Dobruch, J.; Oszczudłowski, M. Bladder Cancer: Current Challenges and Future Directions. Medicina 2021, 57, 749. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lenis, A.T.; Lec, P.M.; Chamie, K.; Mshs, M.D. Bladder Cancer: A Review. JAMA 2020, 324, 1980–1991. [Google Scholar] [CrossRef] [PubMed]
- Jin, L.; Chen, T.; Sun, H.; Dai, G.; Yao, Q.; Yuan, F.; Liu, X.; Xue, B. The clinical significance and anti-tumor role of PRKG1 in bladder cancer. Front Immunol. 2024, 15, 1442555. [Google Scholar] [CrossRef] [PubMed]
- Chavan, S.; Bray, F.; Lortet-Tieulent, J.; Goodman, M.; Jemal, A. International variations in bladder cancer incidence and mortality. Eur. Urol. 2014, 66, 59–73. [Google Scholar] [CrossRef] [PubMed]
- Cancer Research UK. Bladder Cancer Incidence Statistics. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/bladder-cancer/incidence (accessed on 1 September 2023).
- Letašiová, S.; Medveďová, A.; Šovčíková, A.; Dušinská, M.; Volkovová, K.; Mosoiu, C.; Bartonová, A. Bladder cancer, a review of the environmental risk factors. Environ. Health. 2012, 11 (Suppl. S1), S11. [Google Scholar] [CrossRef] [PubMed]
- Mahdavifar, N.; Ghoncheh, M.; Pakzad, R.; Momenimovahed, Z.; Salehiniya, H. Epidemiology, Incidence and Mortality of Bladder Cancer and their Relationship with the Development Index in the World. Asian Pac. J. Cancer Prev. 2016, 17, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Saad-Hussein, A.; Beshir, S.; Shaheen, W.; Saleh, I.A.; Elhamshary, M.; Mohammed, A.M.F. Integrated evaluation of workplace exposures and biomarkers of bladder cancer among textile dyeing workers. J Egypt Public Health Assoc. 2024, 99, 23. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F.; Bsc, M.F.B.; Me, J.F.; Soerjomataram, M.I.; et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, G.L.; Erikson, M.S.; Mogensen, K.; Rosthøj, S.; Hermann, G.G. Outpatient photodynamic diagnosis-guided laser destruction of bladder tumors is as good as conventional inpatient photodynamic diagnosis-guided transurethral tumor resection in patients with recurrent intermediate-risk low-grade Ta bladder tumors. A prospective random-ized noninferiority clinical trial. Eur. Urol. 2023, 83, 125–130. [Google Scholar] [CrossRef]
- Mahadevan, V. Anatomy of the lower urinary tract. Surgery 2016, 34, 318–325. [Google Scholar] [CrossRef]
- Moore, K.L.; Dalley, A.F. Clinically Oriented Anatomy; Wolters Kluwer India Pvt Ltd.: Gurugram, India, 2018. [Google Scholar]
- Woodburne, R.T. Anatomy of the bladder and bladder outlet. J. Urol. 1968, 100, 474–487. [Google Scholar] [CrossRef] [PubMed]
- Hallgrímsson, B.; Benediktsson, H.; Vize, P.D. Anatomy and histology of the human urinary system. In The Kidney; Academic Press: Cambridge, MA, USA, 2003; pp. 149–164. [Google Scholar]
- Keane, D.P.; O’Sullivan, S. Urinary incontinence: Anatomy, physiology and pathophysiology. Best. Pract. Res. Clin. Obstet. Gynaecol. 2000, 14, 207–226. [Google Scholar] [CrossRef] [PubMed]
- Pradidarcheep, W.; Wallner, C.; Dabhoiwala, N.F.; Lamers, W.H. Anatomy and histology of the lower urinary tract. In Urinary Tract; Springer: Berlin/Heidelberg, Germany, 2011; pp. 117–148. [Google Scholar] [CrossRef]
- Andersson, K.-E.; Arner, A. Urinary bladder contraction and relaxation: Physiology and pathophysiology. Physiol. Rev. 2004, 84, 935–986. [Google Scholar] [CrossRef] [PubMed]
- De Groat, W.C.; Booth, A.M. Physiology of the urinary bladder and urethra. Ann. Intern. Med. 1980, 92 Pt 2, 312–315. [Google Scholar] [CrossRef]
- Michel, M.C.; Barendrecht, M.M. Physiological and pathological regulation of the autonomic control of urinary blad-der contractility. Pharmacol. Ther. 2008, 117, 297–312. [Google Scholar] [CrossRef]
- Calvert, R.C.; Thompson, C.S.; Khan, M.A.; Mikhailidis, D.P.; Morgan, R.J.; Burnstock, G. Alterations in cholinergic and purinergic signaling in a model of the obstructed bladder. J. Urol. 2001, 166, 1530–1533. [Google Scholar] [CrossRef] [PubMed]
- Pfister, C.; Harter, V.; Allory, Y.; Radvanyi, F.; Culine, S.; VESPER Trial Investigators. Design of a randomized controlled phase III study of dose dense methotrexate, vinblastine, doxorubicin and cisplatin (dd-MVAC) or gemcitabine and cisplatin (GC) as peri-operative chemotherapy for patients with locally advanced transitional cell cancer of the bladder. The French GETUG/AFU V05 VESPER trial. Contemp Clin Trials Commun. 2020, 17, 100536. [Google Scholar] [CrossRef] [PubMed]
- Moyer, V.A.; US Preventive Services Task Force. Screening for bladder cancer: US Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2011, 155, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Keegan, K.A.; Resnick, M.J.; Clark, P.E. Multimodal therapies for muscle-invasive urothelial carcinoma of the bladder. Curr. Opin. Oncol. 2012, 24, 278–283. [Google Scholar] [CrossRef]
- British Association of Urological Surgeons, Section of Oncology. BAUS Cancer Registry, Analyses of Minimum Data Set for Urological Cancers, January to December 2009. October 2010. Available online: https://www.baus.org.uk/_userfiles/pages/files/publications/audit/2003finalanalyses.pdf (accessed on 6 January 2024).
- Yafi, F.A.; Aprikian, A.G.; Chin, J.L.; Fradet, Y.; Izawa, J.; Estey, E.; Fairey, A.; Rendon, R.; Cagiannos, I.; Lacombe, L.; et al. Contemporary outcomes of 2287 patients with bladder cancer who were treated with radical cystectomy: A Canadian multicentre experience. BJU Int. 2011, 108, 539–545. [Google Scholar] [CrossRef]
- Gouda, I.; Mokhtar, N.; Bilal, D.; El-Bolkainy, T.; El-Bolkainy, N.M. Bilharziasis and bladder cancer: A time trend analysis of 9843 patients. J. Egypt Natl. Canc. Inst. 2007, 19, 158–162. [Google Scholar] [PubMed]
- Felix, A.S.; Soliman, A.S.; Khaled, H.; Zaghloul, M.S.; Banerjee, M.; El-Baradie, M.; El-Kalawy, M.; Abd-Elsayed, A.A.; Ismail, K.; Hablas, A.; et al. The changing patterns of bladder cancer in Egypt over the past 26 years. Cancer Causes Control 2008, 19, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.W.; Carballido, E.M.; Ahmed, A.; Farhan, B.; Dutta, R.; Smith, C.; Youssef, R.F. Squamous cell carcinoma of the urinary bladder: Systematic review of clinical characteristics and therapeutic approaches. Arab. J. Urol. 2016, 14, 183–191. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Abol-Enein, H.; Kava, B.R.; Carmack, A.J. Nonurothelial cancer of the bladder. Urology 2007, 69 (Suppl. S1), 93–104. [Google Scholar] [CrossRef] [PubMed]
- Shokeir, A.A. Squamous cell carcinoma of the bladder: Pathology, diagnosis and treatment. BJU Int. 2004, 93, 216–220. [Google Scholar] [CrossRef]
- Welk, B.; McIntyre, A.; Teasell, R.; Potter, P.; Loh, E. Bladder cancer in individuals with spinal cord injuries. Spinal Cord 2013, 51, 516–521. [Google Scholar] [CrossRef]
- Kaufman, J.M.; Fam, B.; Jacobs, S.C.; Gabilondo, F.; Yalla, S.; Kane, J.P.; Rossier, A.B. Bladder Cancer and Squamous Metaplasia in Spinal Cord Injury Patients. J. Urol. 1977, 118, 967–971. [Google Scholar] [CrossRef]
- Grignon, D.J.; Ro, J.Y.; Ayala, A.G.; Johnson, D.E.; Ordóñez, N.G. Primary adenocarcinoma of the urinary bladder. A clinicopathologic analysis of 72 cases. Cancer 1991, 67, 2165–2172. [Google Scholar] [CrossRef]
- Epstein, J.I.; Amin, M.B.; Reuter, V.E. Glandular lesions. In Bladder Biopsy Interpretation, 2nd ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2010; pp. 180–213. [Google Scholar]
- Melicow, M.M. Tumors of the urinary bladder: A clinicopathological analysis of over 2500 specimens and biopsies. J. Urol. 1955, 74, 498–521. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.L.; Black, P.C.; Brown, G.A.; Porter, M.P.; Kamat, A.M.; Dinney, C.P.; Lin, D.W. Differences in survival among patients with sarcomatoid carcinoma, carcinosarcoma and urothelial carcinoma of the bladder. J. Urol. 2007, 178, 2302–2306. [Google Scholar] [CrossRef]
- Liao, R.S.; Ruan, H.T.; Jang, A.; Huynh, M.; Rios, R.N.; Hoffman-Censits, J.H.; Wei, S.; Mian, O.Y.; Barata, P.C. Emerging Insights in Small-Cell Carcinoma of the Genitourinary Tract: From Diagnosis to Novel Therapeutic Horizons. Am. Soc. Clin. Oncol. Educ. Book 2024, 44, e43336. [Google Scholar] [CrossRef]
- United Nations Department of Economic & Social Affairs. World Population Prospects, the 2017 Revision, Volume I: Comprehensive Tables; United Nations: New York, NY, USA, 2017.
- Freedman, N.D.; Silverman, D.T.; Hollenbeck, A.R.; Schatzkin, A.; Abnet, C.C. Association between smoking and risk of bladder cancer among men and women. JAMA 2011, 306, 737–745. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhao, X.; Wang, Y.; Liang, C. Cigarette smoking and risk of bladder cancer: A dose-response meta-analysis. Int. Urol. Nephrol. 2022, 54, 1169–1185. [Google Scholar] [CrossRef] [PubMed]
- Richters, A.; Aben, K.K.H.; Kiemeney, L.A.L.M. The global burden of urinary bladder cancer: An update. World J. Urol. 2020, 38, 1895–1904. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sheikh, M.; Poustchi, H.; Pourshams, A.; Etemadi, A.; Islami, F.; Khoshnia, M.; Gharavi, A.; Kamangar, F.; Rosh, G.; Hashemian, M.; et al. Opium use and subsequent incidence of cancer: Results from the Golestan Cohort Study. Lancet Glob. Health 2020, 8, e649–e660. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.F.; Rumgay, H.; Dunlop, C.; Ryan, M.; Quartly, F.; Cox, A.; Deas, A.; Elliss-Brookes, L.; Gavin, A.; Hounsome, L.; et al. The fraction of cancer attributable to modifiable risk factors in England, Wales, Scotland, Northern Ireland, and the United Kingdom in 2015. Br. J. Cancer 2018, 118, 1130–1141. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jalilian, H.; Ziaei, M.; Weiderpass, E.; Rueegg, C.S.; Kullberg, C.; Andersen, A.; Ljung, R.; Guha, N.; Poulot, D.; Byrnes, G.; et al. Cancer incidence and mortality among firefighters. Int. J. Cancer 2019, 145, 2639–2646. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Boffetta, P.; Borron, C. Low-level exposure to arsenic in drinking water and risk of lung and bladder cancer: A system-atic review and dose-response meta-analysis. Dose Response 2019, 17, 1559325819863634. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jubber, I.; Ong, S.; Bukavina, L.; Black, P.C.; Compérat, E.; Kamat, A.M.; Kiemeney, L.; Lawrentschuk, N.; Lerner, S.P.; Meeks, J.J.; et al. Epidemiology of Bladder Cancer in 2023: A Systematic Review of Risk Factors. Eur. Urol. 2023, 84, 176–190. [Google Scholar] [CrossRef] [PubMed]
- Yu, E.Y.; Granström, C.; Vermeulen, R.; Chow, W.H.; Rothman, N.; Chow, K.; Moore, L.E.; Steineck, G.; Pallon, J.; Golka, K.; et al. Coffee consumption and risk of bladder cancer: A pooled analysis of 501, 604 participants from 12 cohort studies in the BLadder Cancer Epidemiology and Nutritional Determinants (BLEND) international study. Eur. J. Epidemiol. 2020, 35, 523–535. [Google Scholar] [CrossRef]
- Vartolomei, M.D.; Iwata, T.; Roth, B.; Kimura, S.; Mathieu, R.; Ferro, M.; Shariat, S.F.; Seitz, C. Impact of alcohol consumption on the risk of developing bladder cancer: A systematic review and meta-analysis. World J. Urol. 2019, 37, 2313–2324. [Google Scholar] [CrossRef] [PubMed]
- Boot, I.W.A.; Schouten, L.J.; Linseisen, J.; Weiderpass, E.; van den Brandt, P.A.; Rinaldi, S.; Vineis, P.; Bueno-de-Mesquita, B.; Ros, M.; Tjønneland, A.; et al. Dietary B group vitamin intake and the bladder cancer risk: A pooled analysis of prospective cohort studies. Eur. J. Nutr. 2022, 61, 2397–2416. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Al-Zalabani, A.H.; Wesselius, A.; Yu, E.Y.-W.; Van Den Brandt, P.; Grant, E.J.; White, E.; Skeie, G.; Liedberg, F.; Weiderpass, E.; Zeegers, M.P. Tea consumption and risk of bladder cancer in the Bladder Cancer Epidemiology and Nutritional Determinants (BLEND) Study: Pooled analysis of 12 international cohort studies. Clin. Nutr. 2022, 41, 1122–1130. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Andersson, S.-O.; Johansson, J.-E.; Wolk, A. Cultured milk, yogurt, and dairy intake in relation to bladder cancer risk in a prospective study of Swedish women and men. Am. J. Clin. Nutr. 2008, 88, 1083–1087. [Google Scholar] [CrossRef] [PubMed]
- Acham, M.; Hess, T.; Rinaldi, S.; Weiderpass, E.; Ros, M.; Bueno-de-Mesquita, H.B.; Tjønnel, A.; Olsen, A.; Overvad, K.; Boutron-Ruault, M.C.; et al. Intake of milk and other dairy products and the risk of bladder cancer: A pooled analysis of 13 cohort studies. Eur. J. Clin. Nutr. 2020, 74, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Yu, E.Y.; Sinha, R.; Hung, R.J.; Zaridze, D.; Mukeria, A.; Navratilova, M.; Foretova, L.; Janout, V.; Holcatova, I.; Matejcic, M.; et al. Grain and dietary fiber intake and bladder cancer risk: A pooled analysis of prospective cohort studies. Am. J. Clin. Nutr. 2020, 112, 1252–1266. [Google Scholar] [CrossRef] [PubMed]
- McConkey, D.J.; Lee, S.; Choi, W.; Tran, M.; Majewski, T.; Lee, S.; Siefker-Radtke, A.; Dinney, C. Molecular genetics of bladder cancer: Emerging mechanisms of tumor initiation and progression. Urol. Oncol. 2010, 28, 429–440. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Papageorgiou, A.; Lashinger, L.; Millikan, R.; Grossman, H.B.; Benedict, W.; Dinney, C.P.N.; McConkey, D.J. Role of tumor necrosis factor-related apoptosis-inducing ligand in interferon-induced apoptosis in human bladder cancer cells. Cancer Res. 2004, 64, 8973–8979. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.; Jones, J.S.; Barocas, D.A.; Castle, E.P.; Lang, E.K.; Leveillee, R.J.; Messing, E.M.; Miller, S.D.; Peterson, A.C.; Turk, T.M.T.; et al. Diagnosis, evaluation and follow-up of asymptomatic microhematuria (AMH) in adults: AUA guideline. J. Urol. 2012, 188 (Suppl. S6), 2473–2481. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.C.; Chang, S.S.; Dalbagni, G.; Pruthi, R.S.; Seigne, J.D.; Skinner, E.C.; Wolf, J.S.; Schellhammer, P.F. Guideline for the management of nonmuscle invasive bladder cancer (stages Ta, T1, and Tis): 2007 update. J. Urol. 2007, 178, 2314–2330. [Google Scholar] [CrossRef] [PubMed]
- Pashos, C.L.; Botteman, M.F.; Laskin, B.L.; Redaelli, A. Bladder cancer: Epidemiology, diagnosis, and management. Cancer Pract. 2002, 10, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Shinagare, A.B.; Ramaiya, N.H.; Jagannathan, J.P.; Fennessy, F.M.; Taplin, M.-E.; Van Den Abbeele, A.D. Metastatic pattern of bladder cancer: Correlation with the characteristics of the primary tumor. Am. J. Roentgenol. 2011, 196, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Paner, G.P.; Stadler, W.M.; Hansel, D.E.; Montironi, R.; Lin, D.W.; Amin, M.B. Updates in the Eighth Edition of the Tu-mor-Node-Metastasis Staging Classification for Urologic Cancers. Eur. Urol. 2018, 73, 560–569. [Google Scholar] [CrossRef] [PubMed]
- Magers, M.J.; Beltran, A.L.; Montironi, R.; Williamson, S.R.; Kaimakliotis, H.Z.; Cheng, L. Staging of bladder cancer. Histopathology 2019, 74, 112–134. [Google Scholar] [CrossRef] [PubMed]
- Palapattu, G.S.; Shariat, S.F.; Karakiewicz, P.I.; Bastian, P.J.; Rogers, C.G.; Amiel, G.; Lotan, Y.; Vazina, A.; Gupta, A.; Sagalowsky, A.I.; et al. Cancer specific outcomes in patients with pT0 disease following radical cystectomy. J. Urol. 2006, 175, 1645–1649. [Google Scholar] [CrossRef]
- Kim, H.S.; Jeong, C.W.; Kwak, C.; Kim, H.H.; Ku, J.H. Pathological T0 following cisplatin-based neoadjuvant chemotherapy for muscle-invasive bladder cancer: A network meta-analysis. Clin. Cancer Res. 2016, 22, 1086–1094. [Google Scholar] [CrossRef] [PubMed]
- Lavery, H.J.; Stensland, K.D.; Niegisch, G.; Albers, P.; Droller, M.J. Pathological T0 following radical cystectomy with or without neoadjuvant chemotherapy: A useful surrogate. J. Urol. 2014, 191, 898–906. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Coinu, A.; Cabiddu, M.; Ghilardi, M.; Vavassori, I.; Barni, S. Correlation of pathologic complete response with survival after neoadjuvant chemotherapy in bladder cancer treated with cystectomy: A meta-analysis. Eur. Urol. 2014, 65, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Kassouf, W.; Spiess, P.E.; Brown, G.A.; Munsell, M.F.; Grossman, H.B.; Siefker-Radtke, A.; Dinney, C.P.N.; Kamat, A.M. P0 stage at radical cystectomy for bladder cancer is associated with improved outcome independent of traditional clinical risk factors. Eur. Urol. 2007, 52, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Volkmer, B.G.; Kuefer, R.; Bartsch, G., Jr.; Gschwend, J.E.; Hautmann, R.E.; Volkmer, B.G.; Kuefer, R.; Hautmann, R.E. Effect of a pT0 cystectomy specimen without neoadjuvant therapy on survival. Cancer 2005, 104, 2384–2391. [Google Scholar] [CrossRef]
- Aldousari, S.; Kassouf, W. Update on the management of non-muscle invasive bladder cancer. Can. Urol. Assoc. J. 2013, 4, 56–64. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Babjuk, M.; Böhle, A.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Hernández, V.; Kaasinen, E.; Palou, J.; Rouprêt, M.; et al. EAU Guidelines on non-muscle-invasive urothelial carcinoma of the bladder: Update 2016. Eur. Urol. 2017, 71, 447–461. [Google Scholar] [CrossRef] [PubMed]
- Moschini, M.; Shariat, S.F.; Abufaraj, M.; Soria, F.; Klatte, T.; La Croce, G.; Mattei, A.; Damiano, R.; Salonia, A.; Montorsi, F.; et al. The presence of carcinoma in situ at radical cystectomy increases the risk of urothelial recurrence: Implications for follow-up schemes. Urol. Oncol. 2017, 35, 151.e17–151.e23. [Google Scholar] [CrossRef] [PubMed]
- Raspollini, M.R.; Montironi, R.; Mazzucchelli, R.; Cimadamore, A.; Cheng, L.; Lopez-Beltran, A. PT1 high-grade bladder cancer: Histologic criteria, pitfalls in the assessment of invasion, and substaging. Virchows Arch. 2020, 477, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Montironi, R.; Davidson, D.D.; Lopez-Beltran, A. Staging and reporting of urothelial carcinoma of the urinary bladder. Mod. Pathol. 2009, 22 (Suppl. S2), S70–S95. [Google Scholar] [CrossRef] [PubMed]
- Jewett, H.J. Carcinoma of the bladder: Influence of depth of infiltration on the 5-year results following complete extirpation of the primary growth. J. Urol. 1952, 67, 672–676. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Neumann, R.M.; Scherer, B.G.; Weaver, A.L.; Leibovich, B.C.; Nehra, A.; Blute, M.L.; Zincke, H.; Bostwick, D.G. Tumor size predicts the survival of patients with pathologic stage T2 bladder carcinoma: A critical evaluation of the depth of muscle invasion. Cancer 1999, 85, 2638–2647. [Google Scholar] [CrossRef]
- Gakis, G.; Schilling, D.; Renninger, M.; Seibold, J.; Sievert, K.-D.; Stenzl, A. Comparison of the new American Joint Committee on Cancer substratification in node-negative pT2 urothelial carcinoma of the bladder: Analysis of patient outcomes in a contemporary series. BJU Int. 2011, 107, 919–923. [Google Scholar] [CrossRef] [PubMed]
- Tretter, E.M.; Ebel, J.J.; Pohar, K.S.; Zynger, D.L. Does the gross prosector impact pT3 subclassification or lymph node counts in bladder cancer? Hum. Pathol. 2017, 61, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Klotz, L.; Brausi, M.A. World Urologic Oncology Federation Bladder Cancer Prevention Program: A global initiative. Urol. Oncol. Semin. Orig. Investig. 2015, 33, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Saginala, K.; Barsouk, A.; Aluru, J.S.; Rawla, P.; Padala, S.A.; Barsouk, A. Epidemiology of Bladder Cancer. Med. Sci. 2020, 8, 15. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kirkali, Z.; Chan, T.; Manoharan, M.; Algaba, F.; Busch, C.; Cheng, L.; Kiemeney, L.; Kriegmair, M.; Montironi, R.; Murphy, W.M.; et al. Bladder cancer: Epidemiology, staging and grading, and diagnosis. Urology 2005, 66 (Suppl. S1), 4–34. [Google Scholar] [CrossRef] [PubMed]
- DeGeorge, K.C.; Holt, H.R.; Hodges, S.C. Bladder Cancer: Diagnosis and Treatment. Am. Fam. Physician 2017, 96, 507–514. [Google Scholar] [PubMed]
- Cheung, G.; Sahai, A.; Billia, M.; Dasgupta, P.; Khan, M.S. Recent advances in the diagnosis and treatment of bladder cancer. BMC Med. 2013, 11, 13. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Capalbo, E.; Kluzer, A.; Peli, M.; Cosentino, M.; Berti, E.; Cariati, M. Bladder cancer diagnosis: The role of CT urography. Tumori J. 2015, 101, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Hale, Z.; Hanna, E.; Miyake, M.; Rosser, C.J. Imaging the urologic patient: The utility of intravenous pyelogram in the CT scan era. World J. Urol. 2014, 32, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Naselli, A.; Introini, C.; Timossi, L.; Spina, B.; Fontana, V.; Pezzi, R.; Germinale, F.; Bertolotto, F.; Puppo, P. A randomized prospective trial to assess the impact of transurethral resection in narrow band imaging modality on non-muscle-invasive bladder cancer recurrence. Eur. Urol. 2012, 61, 908–913. [Google Scholar] [CrossRef] [PubMed]
- Herr, H.W.; Donat, S.M. A comparison of white-light cystoscopy and narrow-band imaging cystoscopy to detect bladder tumour recurrences. BJU Int. 2008, 102, 1111–1114. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.; Stenzl, A.; Sharma, A.; Vasdev, N. Urinary biomarkers in bladder cancer: A review of the current landscape and future directions. Urol. Oncol. Semin. Orig. Investig. 2021, 39, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Lodewijk, I.; Dueñas, M.; Rubio, C.; Munera-Maravilla, E.; Segovia, C.; Bernardini, A.; Teijeira, A.; Paramio, J.M.; Suárez-Cabrera, C. Liquid Biopsy Biomarkers in Bladder Cancer: A Current Need for Patient Diagnosis and Monitoring. Int. J. Mol. Sci. 2018, 19, 2514. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lopez-Beltran, A.; Cookson, M.S.; Guercio, B.J.; Cheng, L. Advances in diagnosis and treatment of bladder cancer. BMJ 2024, 384, e076743. [Google Scholar] [CrossRef] [PubMed]
- Rud, E.; Galtung, K.F.; Lauritzen, P.M.; Baco, E.; Flatabø, T.; Sandbæk, G. Examining the upper urinary tract in patients with hematuria-time to revise the CT urography protocol? Eur. Radiol. 2020, 30, 1664–1670. [Google Scholar] [CrossRef] [PubMed]
- Nardelli, C.; Aveta, A.; Pandolfo, S.D.; Tripodi, L.; Russo, F.; Imbimbo, C.; Castaldo, G.; Pastore, L. Microbiome Profiling in Bladder Cancer Patients Using the First-morning Urine Sample. Eur. Urol. Open Sci. 2024, 59, 18–26. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Russo, P.; Marino, F.; Rossi, F.; Bizzarri, F.P.; Ragonese, M.; Dibitetto, F.; Filomena, G.B.; Marafon, D.P.; Ciccarese, C.; Iacovelli, R.; et al. Is Systemic Immune-Inflammation Index a Real Non-Invasive Biomarker to Predict Oncological Outcomes in Patients Eligible for Radical Cystectomy? Medicina 2023, 59, 2063. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Necchi, A.; Roumiguié, M.; Esen, A.A.; Lebret, T.; Wit, R.D.; Shore, N.D.; Bajorin, D.F.; Krieger, L.E.M.; Kandori, S.; Uchio, E.M.; et al. Pembrolizumab (pembro) monotherapy for patients (pts) with high-risk non–muscle-invasive bladder cancer (HR NMIBC) unresponsive to bacillus Calmette–Guérin (BCG): Results from cohort B of the phase 2 KEYNOTE-057 trial. J. Clin. Oncol. 2023, 41, LBA442. [Google Scholar] [CrossRef]
- Rentsch, C.A.; Hayoz, S.; Cathomas, R. Pembrolizumab monotherapy for high-risk, non-muscle-invasive bladder cancer. Lancet Oncol. 2021, 22, e379. [Google Scholar] [CrossRef]
- Gill, J.; Prasad, V. Pembrolizumab for non–muscle-invasive bladder cancer—A costly therapy in search of evidence. JAMA Oncol. 2021, 7, 501–502. [Google Scholar] [CrossRef]
- Richterstetter, M.; Wullich, B.; Amann, K.; Haeberle, L.; Engehausen, D.G.; Goebell, P.J.; Krause, F.S. The value of extended transurethral resection of bladder tumour (TURBT) in the treatment of bladder cancer. BJU Int. 2012, 110 Pt 2, E76–E79. [Google Scholar] [CrossRef] [PubMed]
- Kim, L.H.C.; Patel, M.I. Transurethral resection of bladder tumour (TURBT). Transl. Androl. Urol. 2020, 9, 3056–3072. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guallar-Garrido, S.; Julián, E. Bacillus Calmette-Gurin (BCG) Therapy for Bladder Cancer: An Update. Immunotargets Ther. 2020, 9, 1–11. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pérez-Jacoiste Asín, M.A.; Fernández-Ruiz, M.; López-Medrano, F.; Lumbreras, C.; Tejido, A.; Juan, R.S.; Arrebola-Pajares, A.; Lizasoain, M.; Prieto, S.; Aguado, J.M. Bacillus Calmette-Guérin (BCG) infection following intravesical BCG administration as adjunctive therapy for bladder cancer: Incidence, risk factors, and outcome in a single-institution series and review of the literature. Medicine 2014, 93, 236–254. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gore, J.L.; Litwin, M.S.; Lai, J.; Yano, E.M.; Madison, R.; Setodji, C.; Adams, J.L.; Saigal, C.S. Urologic Diseases in America Pro-ject. Use of radical cystectomy for patients with invasive bladder cancer. J. Natl. Cancer Inst. 2010, 102, 802–811. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lawrentschuk, N.; Colombo, R.; Hakenberg, O.W.; Lerner, S.P.; Månsson, W.; Sagalowsky, A.; Wirth, M.P. Prevention and management of complications following radical cystectomy for bladder cancer. Eur. Urol. 2010, 57, 983–1001. [Google Scholar] [CrossRef] [PubMed]
- Peak, T.C.; Hemal, A. Partial cystectomy for muscle-invasive bladder cancer: A review of the literature. Transl. Androl. Urol. 2020, 9, 2938–2945. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zlotta, A.R.; Ballas, L.K.; Niemierko, A.; Lajkosz, K.; Kuk, C.; Miranda, G.; Drumm, M.; Mari, A.; Thio, E.; Fleshner, N.E. Radical cystectomy versus trimodality therapy for muscle-invasive bladder cancer: A multi-institutional propensity score matched and weighted analysis. Lancet Oncol. 2023, 24, 669–681. [Google Scholar] [CrossRef] [PubMed]
- Di Jiang, D.; Chung, P.; Kulkarni, G.S.; Sridhar, S.S. Trimodality Therapy for Muscle-Invasive Bladder Cancer: Recent Advances and Unanswered Questions. Curr. Oncol. Rep. 2020, 22, 14. [Google Scholar] [CrossRef]
- Su, X.; Dong, C.; Liao, W.; Liu, W. Oncological effectiveness of bladder-preserving trimodal therapy versus radical cystectomy for the treatment of muscle-invasive bladder cancer: A system review and meta-analysis. World J. Surg. Oncol. 2023, 21, 271. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yin, M.; Joshi, M.; Meijer, R.P.; Glantz, M.; Holder, S.; Harvey, H.A.; Kaag, M.; Van de Putte, E.E.F.; Horenblas, S.; Drabick, J.J. Neoadjuvant Chemotherapy for Muscle-Invasive Bladder Cancer: A Systematic Review and Two-Step Meta-Analysis. Oncologist 2016, 21, 708–715. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gupta, S.; Ballman, K.V.; Galsky, M.D.; Morris, M.J.; Sridhar, S.S.; Chen, R.C.; Chan, T.A.; Wen, Y.; Grivas, P.; Tan, A.; et al. MAIN-CAV: Phase III randomized trial of maintenance cabozantinib and avelumab versus avelumab after first-line platinum-based chemotherapy in patients (pts) with metastatic urothelial cancer (mUC.; Alliance A032001). J. Clin. Oncol. 2023, 41, TPS4609. [Google Scholar] [CrossRef]
- Motterle, G.; Andrews, J.R.; Morlacco, A.; Karnes, R.J. Predicting Response to Neoadjuvant Chemotherapy in Bladder Cancer. Eur. Urol. Focus 2020, 6, 642–649. [Google Scholar] [CrossRef] [PubMed]
- Advanced Bladder Cancer (ABC) Meta-analysis Collaborators Group. Adjuvant Chemotherapy for Muscle-invasive Bladder Cancer: A Systematic Review and Meta-analysis of Individual Participant Data from Randomised Controlled Trials. Eur. Urol. 2022, 81, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Del Bene, G.; Calabrò, F.; Giannarelli, D.; Plimack, E.R.; Harshman, L.C.; Yu, E.Y.; Crabb, S.J.; Pal, S.K.; Alva, A.S.; Powles, T.; et al. Neoadjuvant vs. Adjuvant Chemotherapy in Muscle Invasive Bladder Cancer (MIBC): Analysis From the RISC Database. Front. Oncol. 2018, 8, 463. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hijab, A.; Tocco, B.; Hanson, I.; Meijer, H.; Nyborg, C.J.; Bertelsen, A.S.; Smeenk, R.J.; Smith, G.; Michalski, J.; Baumann, B.C.; et al. MR-Guided Adaptive Radiotherapy for Bladder Cancer. Front. Oncol. 2021, 11, 637591. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hussain, S.A.; Porta, N.; Hall, E.; Salawu, A.; Lewis, R.; Sreenivasan, T.; Wallace, J.; Crundwell, M.; Jenkins, P.; Tremlett, J.; et al. Outcomes in Patients with Muscle-invasive Bladder Cancer Treated with Neoadjuvant Chemotherapy Followed by (Chemo)radiotherapy in the BC2001 Trial. Eur. Urol. 2021, 79, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Wołącewicz, M.; Hrynkiewicz, R.; Grywalska, E.; Suchojad, T.; Leksowski, T.; Roliński, J.; Niedźwiedzka-Rystwej, P. Immunotherapy in Bladder Cancer: Current Methods and Future Perspectives. Cancers 2020, 12, 1181. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rhea, L.P.; Mendez-Marti, S.; Kim, D.; Aragon-Ching, J.B. Role of immunotherapy in bladder cancer. Cancer Treat. Res. Commun. 2020, 26, 100296. [Google Scholar] [CrossRef] [PubMed]
- Flaig, T.W.; Rosenberg, J.E.; Hoimes, C.J.; O’Donnell, P.H.; Mar, N.; Gourdin, T.S.; Henry, S.; Bilen, M.A.; George, S.; Barata, P.C.; et al. Study EV-103: Neoadjuvant treatment with enfortumab vedotin monotherapy in cisplatin-ineligible patients (pts) with muscle invasive bladder cancer (MIBC): Updated results for Cohort H. J. Clin. Oncol. 2023, 41, 4595. [Google Scholar] [CrossRef]
- Wong, V.K.; Ganeshan, D.; Jensen, C.T.; Devine, C.E. Imaging and Management of Bladder Cancer. Cancers 2021, 13, 1396. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Birtle, A.; Johnson, M.; Chester, J.; Jones, R.; Dolling, D.; Bryan, R.T.; Harris, C.; Winterbottom, A.; Blacker, A.; Catto, J.W.F.; et al. Adjuvant chemotherapy in upper tract urothelial carcinoma (the POUT trial): A phase 3, open-label, randomised controlled trial. Lancet 2020, 395, 1268–1277. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Powles, T.; Park, S.H.; Voog, E.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Kalofonos, H.; Radulović, S.; Demey, W.; Ullén, A.; et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. N. Engl. J. Med. 2020, 383, 1218–1230. [Google Scholar] [CrossRef] [PubMed]
- Gakis, G.; Karl, A.; Bertz, S.; Burger, M.; Fritsche, H.; Hartmann, A.; Jokisch, F.; Kempkensteffen, C.; Miller, K.; Mundhenk, J.; et al. Transurethral en bloc submucosal hydrodissection vs conventional resection for resection of non-muscle-invasive bladder cancer (HYBRIDBLUE): A randomised, multicentre trial. BJU Int. 2020, 126, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Rentsch, C.A.; Bosshard, P.; Mayor, G.; Rieken, M.; Püschel, H.; Wirth, G.; Cathomas, R.; Parzmair, G.P.; Grode, L.; Eisele, B.; et al. Results of the phase I open label clinical trial SAKK 06/14 assessing safety of intravesical instillation of VPM1002BC, a recombinant mycobacterium Bacillus Calmette Guérin (BCG), in patients with non-muscle invasive bladder cancer and previous failure of conventional BCG therapy. Oncoimmunology 2020, 9, 1748981. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- De Ridder, M.; Gerbrandy, L.C.; De Reijke, T.M.; Hinnen, K.A.; Hulshof, M.C.C.M. BioXmark liquid fiducial markers for image-guided radiotherapy in muscle invasive bladder cancer: A safety and performance trial. Br. J. Radiol. 2020, 93, 20200241. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Luo, J.; Zhou, L.; Lin, S.; Yan, W.; Huang, L.; Liang, S. Beneficial effect of fluid warming in elderly patients with bladder cancer undergoing Da Vinci robotic-assisted laparoscopic radical cystectomy. Clinics 2020, 75, e1639. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tan, M.P.; Harris, V.; Warren-Oseni, K.; McDonald, F.; McNair, H.; Taylor, H.; Hansen, V.; Sharabiani, M.; Thomas, K.; Jones, K.; et al. The Intensity-Modulated Pelvic Node and Bladder Radiotherapy (IMPART) Trial: A Phase II Single-Centre Prospective Study. Clin. Oncol. 2020, 32, 93–100. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nishiyama, H.; Yamamoto, Y.; Sassa, N.; Nishimura, K.; Fujimoto, K.; Fukasawa, S.; Yokoyama, M.; Enokida, H.; Takahashi, K.; Tanaka, Y.; et al. Pembrolizumab versus chemotherapy in recurrent, advanced urothelial cancer in Japanese patients: A subgroup analysis of the phase 3 KEYNOTE-045 trial. Int. J. Clin. Oncol. 2020, 25, 165–174. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Blackwell, J.E.M.; Doleman, B.; Boereboom, C.L.; Morton, A.; Williams, S.; Atherton, P.; Smith, K.; Williams, J.P.; Phillips, B.E.; Lund, J.N. High-intensity interval training produces a significant improvement in fitness in less than 31 days before surgery for urological cancer: A randomised control trial. Prostate Cancer Prostatic Dis. 2020, 23, 696–704. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zeng, S.; Ying, Y.; Xing, N.; Wang, B.; Qian, Z.; Zhou, Z.; Zhang, Z.; Xu, W.; Wang, H.; Dai, L.; et al. Noninvasive Detection of Urothelial Carcinoma by Cost-effective Low-coverage Whole-genome Sequencing from Urine-Exfoliated Cell DNA. Clin. Cancer Res. 2020, 26, 5646–5654. [Google Scholar] [CrossRef] [PubMed]
- Boorjian, S.A.; Alemozaffar, M.; Konety, B.R.; Shore, N.D.; Gomella, L.G.; Kamat, A.M.; Bivalacqua, T.J.; Montgomery, J.S.; Lerner, S.P.; Busby, J.E.; et al. Intravesical nadofaragene firadenovec gene therapy for BCG-unresponsive non-muscle-invasive bladder cancer: A single-arm, open-label, repeat-dose clinical trial. Lancet Oncol. 2021, 22, 107–117. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pfister, C.; Gravis, G.; Fléchon, A.; Soulié, M.; Guy, L.; Laguerre, B.; Mottet, N.; Joly, F.; Allory, Y.; Harter, V.; et al. Randomized Phase III Trial of Dose-dense Methotrexate, Vinblastine, Doxorubicin, and Cisplatin, or Gemcitabine and Cisplatin as Perioperative Chemotherapy for Patients with Muscle-invasive Bladder Cancer. Analysis of the GETUG/AFU V05 VESPER Trial Secondary Endpoints: Chemotherapy Toxicity and Pathological Responses. Eur. Urol. 2021, 79, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Liu, M.; Jia, D.; Tao, T.; Hao, D. LncRNA TINCR SNPs and Expression Levels Are Associated with Bladder Cancer Susceptibility. Genet. Test. Mol. Biomark. 2021, 25, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Razzaghi, M.R.; Mazloomfard, M.M.; Yavar, M.; Malekian, S.; Mousapour, P. Holmium LASER in Comparison with Transurethral Resection of the Bladder Tumor for Non-muscle Invasive Bladder Cancer: Randomized Clinical Trial with 18-month Follow-up. Urol. J. 2021, 18, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Wu, K.; Zhang, N.; Yang, T.; Liu, N.; Jiang, Y.; Bai, X.; Wang, X.; He, D. Green-light laser en bloc resection versus conventional transurethral resection for initial non-muscle-invasive bladder cancer: A randomized controlled trial. Int. J. Urol. 2021, 28, 855–860. [Google Scholar] [CrossRef] [PubMed]
- Culine, S.; Harter, V.; Gravis, G.; Fléchon, A.; Chevreau, C.; Mahammedi, H.; Laguerre, B.; Guillot, A.; Joly, F.; Abadie-Lacourtoisie, S.; et al. Chemotherapy for Muscle-invasive Bladder Cancer: Impact of Cisplatin Delivery on Renal Function and Local Control Rate in the Randomized Phase III VESPER (GETUG-AFU V05) Trial. Clin. Genitourin. Cancer 2021, 19, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Sheng, X.; Yan, X.; Wang, L.; Shi, Y.; Yao, X.; Luo, H.; Shi, B.; Liu, J.; He, Z.; Yu, G.; et al. Open-label, Multicenter, Phase II Study of RC48-ADC, a HER2-Targeting Antibody-Drug Conjugate, in Patients with Locally Advanced or Metastatic Urothelial Carcinoma. Clin. Cancer Res. 2021, 27, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.T.; Irlam-Jones, J.J.; Pereira, R.R.; Lane, B.; Valentine, H.R.; Aragaki, K.; Dyrskjøt, L.; McConkey, D.J.; Hoskin, P.J.; Choudhury, A.; et al. A miRNA signature predicts benefit from addition of hypoxia-modifying therapy to radiation treatment in invasive sbladder cancer. Br. J. Cancer 2021, 125, 85–93. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Moschini, M.; Afferi, L.; Gandaglia, G.; D’Andrea, D.; Zamboni, S.; Di Bona, C.; Mordasini, L.; Mattei, A.; Baumeister, P.; Martini, A.; et al. Prediction of the Need for an Extended Lymphadenectomy at the Time of Radical Cystectomy in Patients with Bladder Cancer. Eur. Urol. Focus 2021, 7, 1067–1074. [Google Scholar] [CrossRef] [PubMed]
- Huddart, R.; Hafeez, S.; Lewis, R.; McNair, H.; Syndikus, I.; Henry, A.; Staffurth, J.; Dewan, M.; Vassallo-Bonner, C.; Moinuddin, S.A.; et al. Clinical Outcomes of a Randomized Trial of Adaptive Plan-of-the-Day Treatment in Patients Receiving Ultra-hypofractionated Weekly Radiation Therapy for Bladder Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 412–424. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hall, E.; Hussain, S.A.; Porta, N.; Lewis, R.; Crundwell, M.; Jenkins, P.; Rawlings, C.; Tremlett, J.; Sreenivasan, T.; Wallace, J.; et al. Chemoradiotherapy in Muscle-invasive Bladder Cancer: 10-yr Follow-up of the Phase 3 Randomised Controlled BC2001 Trial. Eur. Urol. 2022, 82, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Ong, W.; Shen, T.; Sng, J.; Lata, R.; Mahendran, R.; Kesavan, E.; Chiong, E. Beyond diabetes mellitus: Role of metformin in non-muscle-invasive bladder cancer. Singap. Med. J. 2022, 63, 209–213. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Beardo, P.; Pinto, R.; Ayerra, H.; Agüera, J.; Armijos, S.; Álvarez-Ossorio, J.L. Optimizing treatment for non muscle-invasive bladder cancer with an app. Actas Urol. Esp. Engl. Ed. 2022, 46, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Rouprêt, M.; Gontero, P.; McCracken, S.R.C.; Dudderidge, T.; Stockley, J.; Kennedy, A.; Rodriguez, O.; Sieverink, C.; Vanié, F.; Allasia, M.; et al. Reducing the Frequency of Follow-up Cystoscopy in Low-grade pTa Non-muscle-invasive Bladder Cancer Using the ADXBLADDER Biomarker. Eur. Urol. Focus 2022, 8, 1643–1649. [Google Scholar] [CrossRef] [PubMed]
- Numakura, K.; Kobayashi, M.; Ishida, T.; Okane, K.; Suzuki, K.; Shimoda, N.; Suzuki, T.; Kumazawa, T.; Sasaki, R.; Fukuda, H.; et al. Effect of Levofloxacin on the Efficacy and Adverse Events in Intravesical Bacillus Calmette-Guerin Treatment for Bladder Cancer: Results of a Ran-domized, Prospective, Multicenter Study. Eur. Urol. Focus 2022, 8, 1666–1672. [Google Scholar] [CrossRef] [PubMed]
- Kates, M.; Mansour, A.M.; Lamm, D.L.; Shore, N.; Maulhardt, H.; Wendt, A.; Verco, J.; Marin, A.; Dewnani, K.; Verco, S.; et al. Phase 1/2 Trial Results of a Large Surface Area Microparticle Docetaxel for the Treatment of High-Risk Nonmuscle-Invasive Bladder Cancer. J. Urol. 2022, 208, 821–829. [Google Scholar] [CrossRef] [PubMed]
- Stover, A.M.; Basak, R.; Mueller, D.; Lipman, R.; Teal, R.; Hilton, A.; Giannone, K.; Waheed, M.; Smith, A.B. Minimal Patient-Reported Side Effects for a Chemoablative Gel (UGN-102) Used as Frontline Treatment in Adults with Nonmuscle-Invasive Bladder Cancer. J. Urol. 2022, 208, 580–588. [Google Scholar] [CrossRef] [PubMed]
- Tae, B.S.; Oh, J.J.; Jeong, B.C.; Ku, J.H. Catheter-associated urinary tract infections in patients who have undergone radical cystectomy for bladder cancer: A prospective randomized clinical study of two silicone catheters (clinical benefit of antibiotic silicone material). Investig. Clin. Urol. 2022, 63, 334–340. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Abdelgawad, A.; Hashem, A.; Mosbah, A.; Eissa, L.A. A prospective trial investigating the role of Serum 25-Hydroxyvitamin D in diagnosis and prognosis of bladder cancer. PLoS ONE 2022, 17, e0266371. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hurle, R.; Guazzoni, G.; Colombo, P.; Santoro, A.; De Cobelli, O.; Di Trapani, E.; Nohales, G.; Carlos, L.; Duran-Merino, R.; Lazzeri, M. Oncofid-P-B: A novel treatment for BCG unresponsive carcinoma in situ (CIS) of the bladder: Results of a prospective European Multicentre study at 15 months from treatment start. Urol. Oncol. Semin. Orig. Investig. 2022, 40, 11.e9–11.e15. [Google Scholar] [CrossRef] [PubMed]
- Loriot, Y.; Matsubara, N.; Park, S.H.; Huddart, R.A.; Burgess, E.F.; Houede, N.; Banek, S.; Guadalupi, V.; Ku, J.H.; Valderrama, B.P.; et al. Erdafitinib or Chemotherapy in Advanced or Metastatic Urothelial Carcinoma. N. Engl. J. Med. 2023, 389, 1961–1971. [Google Scholar] [CrossRef] [PubMed]
- Bryan, R.T.; Pirrie, S.J.; Abbotts, B.; Maycock, S.; During, V.; Lewis, C.; Grant, M.; Bird, D.; Devall, A.J.; Wallace, D.M.A.; et al. Selenium and Vitamin E for Prevention of Non-Muscle-Invasive Bladder Cancer Recurrence and Progression: A Randomized Clinical Trial. JAMA Netw. Open 2023, 6, e2337494. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lu, Y.-T.; Plets, M.; Morrison, G.; Cunha, A.T.; Cen, S.Y.; Rhie, S.K.; Siegmund, K.D.; Daneshmand, S.; Quinn, D.I.; Meeks, J.J.; et al. Cell-free DNA Methylation as a Predictive Biomarker of Response to Neoadjuvant Chemotherapy for Patients with Muscle-invasive Bladder Cancer in SWOG S1314. Eur. Urol. Oncol. 2023, 6, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Tyson, M.D.; Morris, D.; Palou, J.; Rodriguez, O.; Mir, M.C.; Dickstein, R.J.; Guerrero-Ramos, F.; Scarpato, K.R.; Hafron, J.M.; Messing, E.M.; et al. Safety, Tolerability, and Preliminary Efficacy of TAR-200 in Patients With Muscle-invasive Bladder Cancer Who Refused or Were Unfit for Curative-intent Therapy: A Phase 1 Study. J. Urol. 2023, 209, 890–900. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhang, S.; Jin, D.; Luo, J.; Shi, Y.; Zhang, Y.; Wu, L.; Song, Y.; Su, D.; Pan, Z.; et al. μ-opioid receptor agonist facilitates circulating tumor cell formation in bladder cancer via the MOR/AKT/Slug pathway: A comprehensive study including randomized controlled trial. Cancer Commun. 2023, 43, 365–386. [Google Scholar] [CrossRef] [PubMed]
- Huddart, R.; Hafeez, S.; Omar, A.; Alonzi, R.; Birtle, A.; Cheung, K.C.; Choudhury, A.; Foroudi, F.; Gribble, H.; Henry, A.; et al. Acute Toxicity of Hypofractionated and Conventionally Fractionated (Chemo)Radiotherapy Regimens for Bladder Cancer: An Exploratory Analysis from the RAIDER Trial. Clin. Oncol. 2023, 35, 586–597. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.C.C.; De Souza, B.R.; Reis, I.B.; De Camargo, G.C.D.; De Oliveira, G.; De Salmazo, M.I.D.B.; Gonçalves, J.M.; De Roston, J.R.D.; Caria, P.H.F.; Da Santos, A.D.; et al. OncoTherad® (MRB-CFI-1) Nanoimmunotherapy: A Promising Strategy to Treat Bacillus Calmette-Guérin-Unresponsive Non-Muscle-Invasive Bladder Cancer: Crosstalk among T-Cell CX3CR1, Immune Checkpoints, and the Toll-Like Receptor 4 Signaling Pathway. Int. J. Mol. Sci. 2023, 24, 17535. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Wang, Y.; Hu, X. Prognostic nomogram based on the lymph node metastasis indicators for patients with bladder cancer: A SEER population-based study and external validation. Cancer Med. 2023, 12, 6853–6866. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gresser, E.; Woźnicki, P.; Messmer, K.; Schreier, A.; Kunz, W.G.; Ingrisch, M.; Stief, C.; Ricke, J.; Nörenberg, D.; Buchner, A.; et al. Radiomics Signature Using Manual Versus Automated Segmentation for Lymph Node Staging of Bladder Cancer. Eur. Urol. Focus 2022, 9, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.; Wang, Y.; Wang, S.; Li, C.; Zhang, M.; Hou, F. Clinical Effect of the Combination of Compound Kushen Injection and Gemcitabine on Postoperative Patients with Non-Muscle Invasive Bladder Cancer and Its Influence on Serum-Related Factors. Arch. Esp. Urol. 2023, 76, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Lerner, S.P.; McConkey, D.J.; Tangen, C.M.; Meeks, J.J.; Flaig, T.W.; Hua, X.; Daneshmand, S.; Alva, A.S.; Lucia, M.S.; Theodorescu, D.; et al. Association of Molecular Subtypes with Pathologic Response, PFS, and OS in a Phase II Study of COXEN with Neoadjuvant Chemotherapy for Muscle-invasive Bladder Cancer. Clin. Cancer Res. 2023, 30, 444–449. [Google Scholar] [CrossRef] [PubMed]
- Grivas, P.; Koshkin, V.S.; Chu, X.; Cole, S.; Jain, R.K.; Dreicer, R.; Cetnar, J.P.; Sundi, D.; Gartrell, B.A.; Galsky, M.D.; et al. PrECOG PrE0807: A Phase 1b Feasibility Trial of Neoadjuvant Nivolumab without and with Lirilumab in Patients with Muscle-invasive Bladder Cancer Ineligible for or Refusing Cisplatin-based Neoadjuvant Chemotherapy. Eur. Urol. Oncol. 2024, 7, 914–922. [Google Scholar] [CrossRef]
- McGregor, B.A.; Sonpavde, G.P.; Kwak, L.; Regan, M.M.; Gao, X.; Hvidsten, H.; Mantia, C.M.; Wei, X.X.; Berchuck, J.E.; Berg, S.A.; et al. The Double Antibody Drug Conjugate (DAD) phase I trial: Sacituzumab govitecan plus enfortumab vedotin for metastatic urothelial carcinoma. Ann. Oncol. 2024, 35, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Sheng, X.; Wang, L.; He, Z.; Shi, Y.; Luo, H.; Han, W.; Yao, X.; Shi, B.; Liu, J.; Hu, C.; et al. Efficacy and Safety of Disitamab Vedotin in Patients With Human Epidermal Growth Factor Receptor 2-Positive Locally Advanced or Metastatic Urothelial Carcinoma: A Combined Analysis of Two Phase II Clinical Trials. J. Clin. Oncol. 2024, 42, 1391–1402. [Google Scholar] [CrossRef] [PubMed]
- Font, A.; Mellado, B.; Climent, M.A.; Virizuela, J.A.; Oudar, D.S.; Puente, J.; Castellano, D.; González-Del-Alba, A.; Pinto, A.; Mo-rales-Barrera, R.; et al. Phase II trial of afatinib in patients with advanced urothelial carcinoma with genetic alterations in ERBB1-3 (LUX-Bladder 1). Br. J. Cancer 2024, 130, 434–441. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Cancer Stat Facts: Bladder Cancer. Available online: http://seer.cancer.gov/statfacts/html/urinb.html (accessed on 27 May 2016).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).