

Efficacy of a Food Supplement Based on Collagen and Magnesium Combined with Pelvic Floor Muscle Training Exercises in Women with Urinary Incontinence: A Double-Blind, Randomized, Pilot Clinical Trial

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Participants
2.3. Intervention, Randomization, and Compliance with Treatment
2.4. Primary and Secondary Endpoints
2.5. Outcomes
2.6. Statistics
3. Results
3.1. Subject Characteristics, Compliance with Treatment, and Tolerability
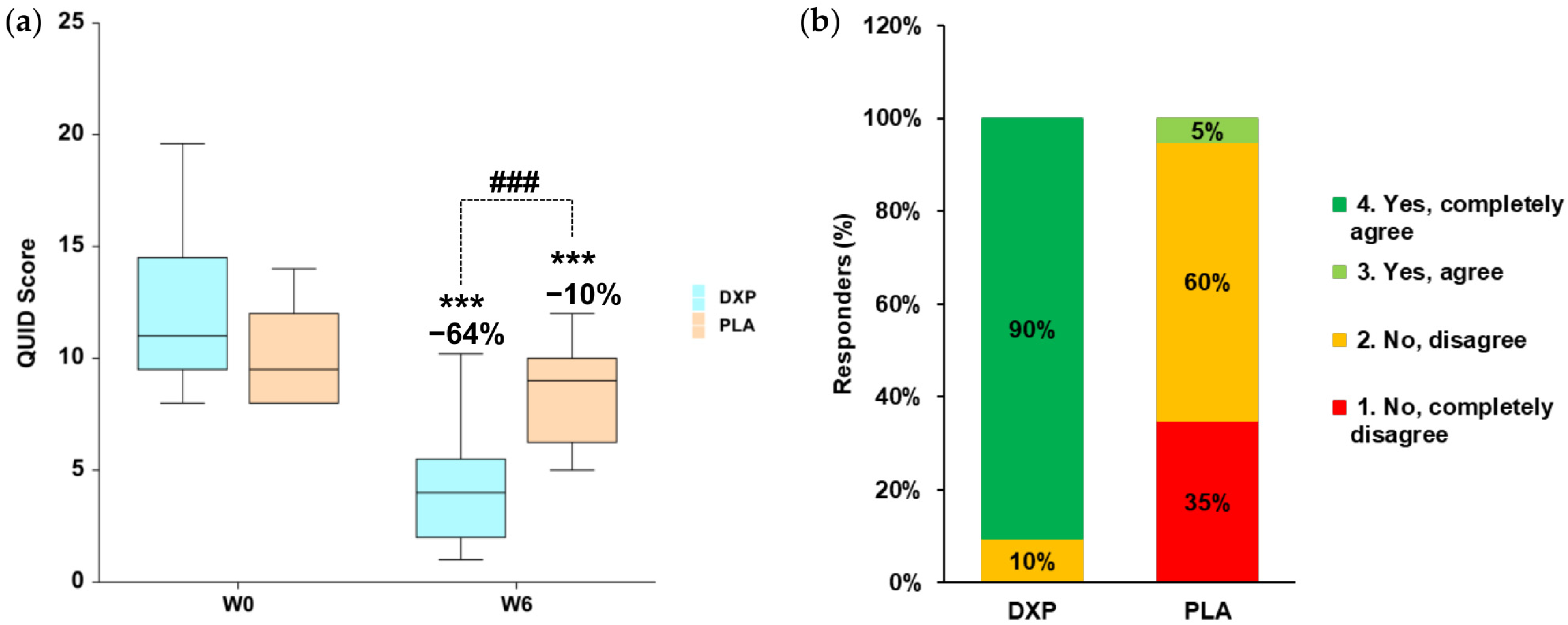
3.2. Primary Outcomes
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| UI | Urinary incontinence |
| PFMT | Pelvic floor muscle training |
| SUI | Stress urinary incontinence |
| UUI | Urge urinary incontinence |
| MUI | Mixed urinary incontinence |
| QUID | Questionnaire for urinary incontinence diagnosis |
| DPX | Active product |
| PLA | Placebo product |
| QoL | Quality of life |
| MMP | Matrix metalloproteinases |
| TIMP | Tissue inhibitors of metalloproteinases |
| VRS | Verbal rating scale |
| NRS | Numerical rating scale |
| ICOPE | Integrated care for older people |
| WHO | World health organization |
| EAU | European association of Urology |
| EC | Ethical committee |
References
- Haylen, B.T.; de Ridder, D.; Freeman, R.M.; Swift, S.E.; Berghmans, B.; Lee, J.; Monga, A.; Petri, E.; Rizk, D.E.; Sand, P.K.; et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) Joint Report on the Terminology for Female Pelvic Floor Dysfunction. Neurourol. Urodyn. 2010, 29, 4–20. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.; Cartwright, R.; Lapitan, M.C.; Milsom, I.; Nelson, R.; Sjöström, S.; Tikkinen, K.A.O. Epidemiology of Urinary Incontinence (UI) and Other Lower Urinary Tract Symptoms (LUTS), Pelvic Organ Prolapse (POP) and Anal Incontinence (AI). In Incontinence; Abrams, P., Cardozo, L., Wagg, A., Wein, A.J., Eds.; International Continence Society: Bristol, UK, 2017; pp. 1–141. [Google Scholar]
- Milsom, I.; Gyhagen, M. The Prevalence of Urinary Incontinence. Climacteric 2019, 22, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Mostafaei, H.; Sadeghi-Bazargani, H.; Hajebrahimi, S.; Salehi-Pourmehr, H.; Ghojazadeh, M.; Onur, R.; Al Mousa, R.T.; Oelke, M. Prevalence of Female Urinary Incontinence in the Developing World: A Systematic Review and Meta-Analysis-A Report from the Developing World Committee of the International Continence Society and Iranian Research Center for Evidence Based Medicine. Neurourol. Urodyn. 2020, 39, 1063–1086. [Google Scholar] [CrossRef]
- Milsom, I.; Coyne, K.S.; Nicholson, S.; Kvasz, M.; Chen, C.-I.; Wein, A.J. Global Prevalence and Economic Burden of Urgency Urinary Incontinence: A Systematic Review. Eur. Urol. 2014, 65, 79–95. [Google Scholar] [CrossRef]
- Russo, E.; Caretto, M.; Giannini, A.; Bitzer, J.; Cano, A.; Ceausu, I.; Chedraui, P.; Durmusoglu, F.; Erkkola, R.; Goulis, D.G.; et al. Management of Urinary Incontinence in Postmenopausal Women: An EMAS Clinical Guide. Maturitas 2021, 143, 223–230. [Google Scholar] [CrossRef]
- Dwyer, P.L. Differentiating Stress Urinary Incontinence from Urge Urinary Incontinence. Int. J. Gynaecol. Obstet. 2004, 86 (Suppl. S1), S17–S24. [Google Scholar] [CrossRef]
- Gacci, M.; Sakalis, V.I.; Karavitakis, M.; Cornu, J.-N.; Gratzke, C.; Herrmann, T.R.W.; Kyriazis, I.; Malde, S.; Mamoulakis, C.; Rieken, M.; et al. European Association of Urology Guidelines on Male Urinary Incontinence. Eur. Urol. 2022, 82, 387–398. [Google Scholar] [CrossRef]
- Sazonova, N.A.; Kiseleva, M.G.; Gadzhieva, Z.K.; Gvozdev, M.Y. Urinary incontinence in women and its impact on quality of life. Urologiia 2022, No. 2, 136–139. [Google Scholar] [CrossRef]
- Frigerio, M.; Barba, M.; Cola, A.; Braga, A.; Celardo, A.; Munno, G.M.; Schettino, M.T.; Vagnetti, P.; De Simone, F.; Di Lucia, A.; et al. Quality of Life, Psychological Wellbeing, and Sexuality in Women with Urinary Incontinence-Where Are We Now: A Narrative Review. Medicina 2022, 58, 525. [Google Scholar] [CrossRef]
- Walters, M.D.; Taylor, S.; Schoenfeld, L.S. Psychosexual Study of Women with Detrusor Instability. Obstet. Gynecol. 1990, 75, 22–26. [Google Scholar]
- Wagner, T.; Moore, K.; Subak, L.; De Wachter, S.; Dudding, T. Economics of urinary and faecal incontinence, and prolapse. In Incontinence, 6th ed.; Abrams, P., Cardozo, L., Wagg, A., Wein, A., Eds.; Health Publications Ltd.: Paris, France, 2016; pp. 17–24. [Google Scholar]
- Ekelund, P.; Grimby, A.; Milsom, I. Urinary Incontinence. Social and Financial Costs High. BMJ 1993, 306, 1344. [Google Scholar] [CrossRef]
- Uroweb. The Annual Economic Burden of Urinary Incontinence Could Reach €87 Billion in 2030 If No Action Is Taken. Available online: https://uroweb.org/press-releases/the-annual-economic-burden-of-urinary-incontinence-could-reach-87-billion-in-2030-if-no-action-is-taken (accessed on 2 January 2025).
- Morrison, A.; Levy, R. Fraction of Nursing Home Admissions Attributable to Urinary Incontinence. Value Health 2006, 9, 272–274. [Google Scholar] [CrossRef] [PubMed]
- Coyne, K.S.; Wein, A.; Nicholson, S.; Kvasz, M.; Chen, C.-I.; Milsom, I. Economic Burden of Urgency Urinary Incontinence in the United States: A Systematic Review. J. Manag. Care Pharm. 2014, 20, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Harris, S.; Leslie, S.W.; Riggs, J. Mixed Urinary Incontinence. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Talley, K.M.C.; Davis, N.J.; Peden-McAlpine, C.; Martin, C.L.; Weinfurter, E.V.; Wyman, J.F. Navigating through Incontinence: A Qualitative Systematic Review and Meta-Aggregation of the Experiences of Family Caregivers. Int. J. Nurs. Stud. 2021, 123, 104062. [Google Scholar] [CrossRef] [PubMed]
- Bektas Akpinar, N.; Unal, N.; Akpinar, C. Urinary Incontinence in Older Adults: Impact on Caregiver Burden. J. Gerontol. Nurs. 2023, 49, 39–46. [Google Scholar] [CrossRef]
- Gotoh, M.; Matsukawa, Y.; Yoshikawa, Y.; Funahashi, Y.; Kato, M.; Hattori, R. Impact of Urinary Incontinence on the Psychological Burden of Family Caregivers. Neurourol. Urodyn. 2009, 28, 492–496. [Google Scholar] [CrossRef]
- Schumpf, L.F.; Theill, N.; Scheiner, D.A.; Fink, D.; Riese, F.; Betschart, C. Urinary Incontinence and Its Association with Functional Physical and Cognitive Health among Female Nursing Home Residents in Switzerland. BMC Geriatr. 2017, 17, 17. [Google Scholar] [CrossRef]
- Gong, R.; Xia, Z. Collagen Changes in Pelvic Support Tissues in Women with Pelvic Organ Prolapse. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 234, 185–189. [Google Scholar] [CrossRef]
- Chen, B.H.; Wen, Y.; Li, H.; Polan, M.L. Collagen Metabolism and Turnover in Women with Stress Urinary Incontinence and Pelvic Prolapse. Int. Urogynecol. J. Pelvic Floor Dysfunct. 2002, 13, 80–87; discussion 87. [Google Scholar] [CrossRef]
- Li, C.; Yang, M.; Qu, Z.; Ruan, S.; Chen, B.; Ran, J.; Shu, W.; Chen, Y.; Hou, W. Effect of Electroacupuncture on the Degradation of Collagen in Pelvic Floor Supporting Tissue of Stress Urinary Incontinence Rats. Int. Urogynecol. J. 2022, 33, 2233–2240. [Google Scholar] [CrossRef]
- Patel, P.D.; Amrute, K.V.; Badlani, G.H. Pelvic Organ Prolapse and Stress Urinary Incontinence: A Review of Etiological Factors. Indian J. Urol. 2007, 23, 135. [Google Scholar] [CrossRef] [PubMed]
- Gordon, D.; Groutz, A.; Ascher-Landsberg, J.; Lessing, J.B.; David, M.P.; Razz, O. Double-Blind, Placebo-Controlled Study of Magnesium Hydroxide for Treatment of Sensory Urgency and Detrusor Instability: Preliminary Results. Br. J. Obstet. Gynaecol. 1998, 105, 667–669. [Google Scholar] [CrossRef]
- Jeitler, M.; Michalsen, A.; Schwiertz, A.; Kessler, C.S.; Koppold-Liebscher, D.; Grasme, J.; Kandil, F.I.; Steckhan, N. Effects of a Supplement Containing a Cranberry Extract on Recurrent Urinary Tract Infections and Intestinal Microbiota: A Prospective, Uncontrolled Exploratory Study. J. Integr. Complement. Med. 2022, 28, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Jepson, R.G.; Mihaljevic, L.; Craig, J. Cranberries for Preventing Urinary Tract Infections. Cochrane Database Syst. Rev. 2004, 4, CD001321. [Google Scholar] [CrossRef]
- Carneiro, D.; Jardim, T.; Araújo, Y.; Arantes, A.; de Sousa, A.; Barroso, W.; Sousa, A.; da Cunha, L.; Cirilo, H.; Bara, M.; et al. Equisetum Arvense: New Evidences Supports Medical Use in Daily Clinic. Pharmacogn. Rev. 2019, 13, 50–58. [Google Scholar] [CrossRef]
- Vaughan, C.P.; Tangpricha, V.; Motahar-Ford, N.; Goode, P.S.; Burgio, K.L.; Allman, R.M.; Daigle, S.G.; Redden, D.T.; Markland, A.D. Vitamin D and Incident Urinary Incontinence in Older Adults. Eur. J. Clin. Nutr. 2016, 70, 987–989. [Google Scholar] [CrossRef]
- Sharma, J.B.; Kakkad, V.; Kumar, S.; Roy, K.K. Cross-Sectional Study on Vitamin D Levels in Stress Urinary Incontinence in Women in a Tertiary Referral Center in India. Indian J. Endocrinol. Metab. 2019, 23, 623–627. [Google Scholar] [CrossRef]
- Ali, S.B.; Perdawood, D.; Abdulrahman, R.; Al Farraj, D.A.; Alkubaisi, N.A. Vitamin D Deficiency as a Risk Factor for Urinary Tract Infection in Women at Reproductive Age. Saudi J. Biol. Sci. 2020, 27, 2942–2947. [Google Scholar] [CrossRef]
- Raz, R. Postmenopausal Women with Recurrent UTI. Int. J. Antimicrob. Agents 2001, 17, 269–271. [Google Scholar] [CrossRef]
- El-Din, W.A.N. Role of Tibolone and Cimicifuga Racemosa on Urinary Bladder Alterations in Surgically Ovariectomized Adult Female Rats. Egypt. J. Anat. 2015, 38, 1–24. [Google Scholar]
- Bradley, C.S.; Rovner, E.S.; Morgan, M.A.; Berlin, M.; Novi, J.M.; Shea, J.A.; Arya, L.A. A New Questionnaire for Urinary Incontinence Diagnosis in Women: Development and Testing. Am. J. Obstet. Gynecol. 2005, 192, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Bradley, C.S.; Rahn, D.D.; Nygaard, I.E.; Barber, M.D.; Nager, C.W.; Kenton, K.S.; Siddiqui, N.Y.; Abel, R.B.; Spino, C.; Richter, H.E. The Questionnaire for Urinary Incontinence Diagnosis (QUID): Validity and Responsiveness to Change in Women Undergoing Non-Surgical Therapies for Treatment of Stress Predominant Urinary Incontinence. Neurourol. Urodyn. 2010, 29, 727–734. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Integrated Care for Older People (ICOPE): Guidelines on Community-Level Interventions to Manage Declines in Intrinsic Capacity: Evidence Profile: Urinary Incontinence. Available online: https://iris.who.int/handle/10665/342254 (accessed on 8 January 2025).
- Shogenji, M.; Yoshida, M.; Kakuchi, T.; Hirako, K. Factors Associated with Caregiver Burden of Toileting Assistance at Home versus in a Nursing Home: A Cross-Sectional Study. PLoS ONE 2024, 19, e0299721. [Google Scholar] [CrossRef] [PubMed]
- Kegel, A.H. Physiologic Therapy for Urinary Stress Incontinence. J. Am. Med. Assoc. 1951, 146, 915–917. [Google Scholar] [CrossRef]
- Riemsma, R.; Hagen, S.; Kirschner-Hermanns, R.; Norton, C.; Wijk, H.; Andersson, K.-E.; Chapple, C.; Spinks, J.; Wagg, A.; Hutt, E.; et al. Can Incontinence Be Cured? A Systematic Review of Cure Rates. BMC Med. 2017, 15, 63. [Google Scholar] [CrossRef]
- Hay-Smith, E.J.C.; Herderschee, R.; Dumoulin, C.; Herbison, G.P. Comparisons of Approaches to Pelvic Floor Muscle Training for Urinary Incontinence in Women. Cochrane Database Syst. Rev. 2011, CD009508. [Google Scholar] [CrossRef]
- Curillo-Aguirre, C.A.; Gea-Izquierdo, E. Effectiveness of Pelvic Floor Muscle Training on Quality of Life in Women with Urinary Incontinence: A Systematic Review and Meta-Analysis. Medicina 2023, 59, 1004. [Google Scholar] [CrossRef]
- Bent, A. ACOG Practice Bulletin No. 155: Urinary Incontinence in Women. Obstet. Gynecol. 2015, 126, e66–e81. [Google Scholar] [CrossRef]
- Vignesh, A.; Amal, T.C.; Sarvalingam, A.; Vasanth, K. A Review on the Influence of Nutraceuticals and Functional Foods on Health. Food Chem. Adv. 2024, 5, 100749. [Google Scholar] [CrossRef]
- Takacs, P.; Pákozdy, K.; Koroknai, E.; Erdődi, B.; Krasznai, Z.; Kozma, B. A Randomized Controlled Pilot Trial to Assess the Effectiveness of a Specially Formulated Food Supplement and Pelvic Floor Muscle Training in Women with Stress-Predominant Urinary Incontinence. BMC Women’s Health 2023, 23, 321. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| DPX (n = 21) | PLA (n = 20) | p Value 1 | |
|---|---|---|---|
| Age (years) | 58.6 ± 1.7 | 53.7 ± 1.3 | 0.060036 |
| UI diagnosis | |||
| Stress (SUI) | 7 (33%) | 11 (52%) | n.a. |
| Urge (UUI) | 3 (14%) | 1 (5%) | n.a. |
| Mixed (MUI) | 11 (52%) | 8 (38%) | n.a. |
| QUID score | 11 (10–14) | 10 (8–12) | 0.079650 |
| No. | Items | DXP | PLA | |||||
|---|---|---|---|---|---|---|---|---|
| W0 | W6 | DW6 | W0 | W6 | DW6 | p value 1 | ||
| 01 | Physical activities | 5 (4–7) | 1 (1–3) | −80% | 5 (4–6) | 4 (3–5) | −20% | <0.001 |
| 02 | Social activities | 4 (3–6) | 1 (0–3) | −75% | 4 (3–6) | 4 (3–5) | 0% | <0.001 |
| 03 | Relationships/interactions | 4 (3–5) | 1 (0–2) | −75% | 4 (3–6) | 4 (3–5) | 0% | <0.001 |
| 04 | Outdoor activities | 4 (3–5) | 1 (1–3) | −75% | 5 (3–6) | 4 (3–6) | −20% | <0.001 |
| 05 | Activities at home | 3 (2–5) | 0 (0–1) | −100% | 4 (2–4) | 4 (2–4) | 0% | <0.001 |
| 06 | Productivity | 4 (2–5) | 1 (0–2) | −75% | 4 (4–5) | 4 (2–5) | 0% | <0.001 |
| 07 | Ability to travel | 5 (4–6) | 2 (1–3) | −60% | 5 (3–6) | 5 (3–6) | 0% | <0.01 |
| 08 | Feeling stressed | 5 (3–6) | 1 (1–2) | −80% | 4 (4–5) | 4 (2–5) | 0% | <0.001 |
| 09 | Feeling sad | 4 (3–5) | 1 (1–1) | −75% | 4 (3–5) | 4 (2–5) | 0% | <0.001 |
| 10 | Feeling embarrassed | 5 (4–6) | 1 (1–3) | −80% | 5 (4–7) | 5 (3–6) | 0% | <0.001 |
| Overall | 45 (32–52) | 11 (9–19) | −76% | 43 (37–55) | 42 (31–50) | −2% | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nobile, V.; Villa, R.; Micieli, M.; Amone, F.; D’Ambrosio, E.; Pulitano, G.; Schinzari, C.; Di Campi, E.; Carati, D. Efficacy of a Food Supplement Based on Collagen and Magnesium Combined with Pelvic Floor Muscle Training Exercises in Women with Urinary Incontinence: A Double-Blind, Randomized, Pilot Clinical Trial. Uro 2025, 5, 7. https://doi.org/10.3390/uro5020007
Nobile V, Villa R, Micieli M, Amone F, D’Ambrosio E, Pulitano G, Schinzari C, Di Campi E, Carati D. Efficacy of a Food Supplement Based on Collagen and Magnesium Combined with Pelvic Floor Muscle Training Exercises in Women with Urinary Incontinence: A Double-Blind, Randomized, Pilot Clinical Trial. Uro. 2025; 5(2):7. https://doi.org/10.3390/uro5020007
Chicago/Turabian StyleNobile, Vincenzo, Roberta Villa, Mariella Micieli, Fabio Amone, Erminia D’Ambrosio, Giuseppe Pulitano, Camilla Schinzari, Eleonora Di Campi, and Davide Carati. 2025. "Efficacy of a Food Supplement Based on Collagen and Magnesium Combined with Pelvic Floor Muscle Training Exercises in Women with Urinary Incontinence: A Double-Blind, Randomized, Pilot Clinical Trial" Uro 5, no. 2: 7. https://doi.org/10.3390/uro5020007
APA StyleNobile, V., Villa, R., Micieli, M., Amone, F., D’Ambrosio, E., Pulitano, G., Schinzari, C., Di Campi, E., & Carati, D. (2025). Efficacy of a Food Supplement Based on Collagen and Magnesium Combined with Pelvic Floor Muscle Training Exercises in Women with Urinary Incontinence: A Double-Blind, Randomized, Pilot Clinical Trial. Uro, 5(2), 7. https://doi.org/10.3390/uro5020007