
Living with COVID-19 and Sustaining a Tourism Recovery—Adopting a Front-Line Collaborative Response between the Tourism Industry and Community Pharmacists


Abstract
:1. Introduction
“(…) no work in the tourism literature appears to have integrated a medical or health sciences perspective to reveal theoretical and practical insight for the tourism and hospitality industry. Interdisciplinary research is thus strongly encouraged in this vein, particularly with regard to the current pandemic.”Wen et al. (2021, p. 312)
2. Background and the Macao Context
2.1. COVID-19 Containment, Travel Corridor, and Tourism Revival in Macao
2.2. The Role of CPs during the Pandemic in Macao
3. Literature Review
3.1. The Relevance of Cross-Disciplinary Research during COVID-19
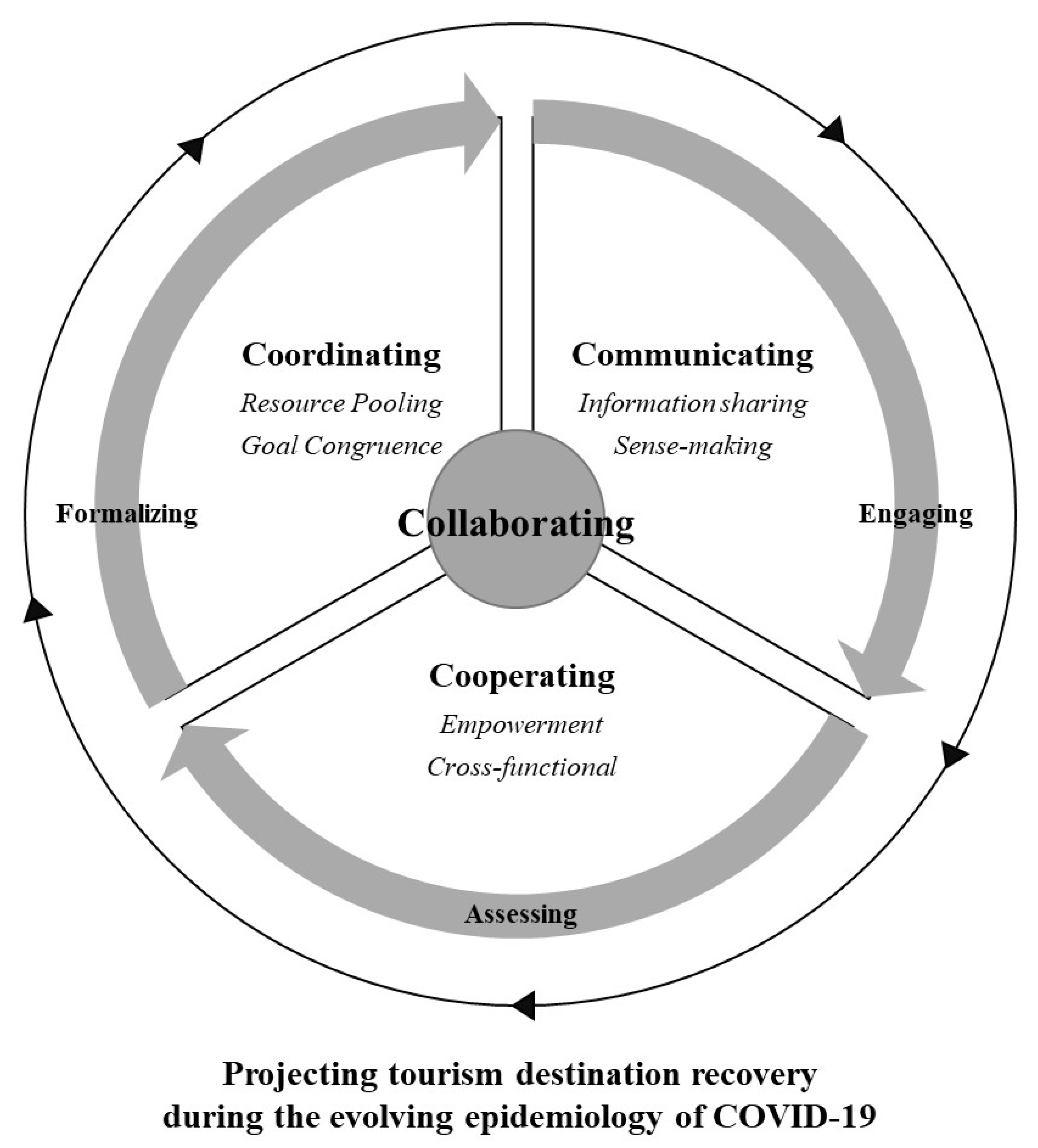
3.2. Development of the Theoretical Framework
3.3. CPs and Tourism Collaboration
3.4. Cooperation between CPs and the Tourism Sector
3.5. Communication between CPs and the Tourism Sector
3.6. Cooperation between CPs and the Tourism Sector
4. Methodology

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question | Probes | Literature | |
|---|---|---|---|
| 1 | What are the values and expectations of cross-industry collaboration to the COVID-19 management? | What is the value and contribution of a network of pharmacists to the recovery strategy of tourism industry? What resources can be part of this collaboration (such as information sharing, skills and knowledge exchange). | [71] Cioccio and Michael; [72] Fyall, Garrod and Wang; [73] Holmes et al. |
| 2 | What are the challenges that you see impeding the cross-industry collaboration? | How is the network established? Who adopts the leadership role? How is trust established in the collaboration? How are data shared? | [74] Jamal and Getz; [75] Graci; [76] Scarpino and Gretzel; [61] Novelli, Burgress, Jones, and Ritchie. |
| 3 | What are the enablers that will help facilitate the cross-disciplinary collaboration for Macao COVID-19 tourism recovery strategy? | What are the shared views or goals? What incentives are provided to enable and sustain collaboration? | [77] Ansell and Gash, [78] Kumar and Banerjee. |
| 4 | What is the priority of actions by pharmacists/tourism to create the strategy that builds the collaboration? | What does the action plan look like to help foster a collaborative relationship between the tourism industry and pharmacists? What is the role of government? Who is responsible for doing what? What is the format of the collaboration efforts (taskforce, regular meeting)? | [79] Ritchie; [67] Jiang and Ritchie. |
| 5 | How should the collaborative relationship be monitored and evaluated? | Who takes the leadership role in this new collaborative mechanism? Who provides the financing and follow-up actions? | [76] Scarpino and Gretzel; [61] Novelli, Burgress, Jones, and Ritche. |
| 6 | If the collaborative relationship is to be sustained even after COVID-19, how should this be done? | How should the collaborative relationship be sustained, and if so, for how long? Will informal or shadow networks emerge to influence and control? Will safe spaces be created to allow people to learn together, with a common understanding of a crisis, to permit collaborative resilience to form? | [80] Jamal and Stronza; [81] Bullock, Armitage and Mitchell; [82] Goldstein. |
5. Results
5.1. Respondents’ Demographic Backgrounds
5.2. The Expectations of Cross-Industry Collaboration towards COVID-19 Management
‘Macao could become a short-term vaccination destination with the best option of vaccines available’(TE5)
‘Pharmacists should have an app with multi-lingual live updates by the minute providing info to hotels so they may direct guests and international travellers to the right place’(TE8)
‘Testing and speed of results are crucial to tourism recovery. Once a resident or tourist of a destination is tested positive, the drugs and therapeutics must be targeted to these individuals as soon as possible to stop any further spread of the virus’(TE7)
‘The cross-over between the tourism industry and the community pharmacy is nothing new. Tourists come to Macao for leisure, but many tourists are also very interested in what we sell in the pharmacy. It is still a common perception that what we sell in pharmacy in Macao is of high-quality assurance compared to what is available in their hometown. So, there is a general trust in the practice’s reliability in the pharmacy in Macao among the tourists’(PH1)
‘It is a matter of building trust for the tourists, and we pharmacists should be a part of it. To this end, we need to be more innovative in adjusting to this new norm. I hope that the interface between our profession and the tourist industry brings us new opportunities to become more than just a retail sales person’(PH3)
‘With our distribution all over Macao, we can become a strong safety net offering advice, education and assurance for people we serve…. However, we need a mechanism to move the pharmacies as a joint force instead of individual business operations. The collaboration with the tourist industry, if well structured and well orchestrated, will be a great opportunity for us to continue being a positive factor in protecting the public, including the tourists’(PH5)
5.3. The Challenges Impeding Cross-Industry Collaboration
‘The local government is risk averse; hence, their key concern is that tourists will not transmit the COVID-19 disease to residents, yet the tourism industry is coming to a crossroads on survival, and with that, there will be conflict and friction because the tourism industry and the health authorities may desire different outcomes’(TE3)
‘Yes, business and revenue are important, but the perspective here is to create a service model together that addresses the concerns and needs of the potential travellers. For this, I am afraid that neither we nor the tourist industry has a lot of insights so far’(PH6)
‘I can see many positive outcomes through closer collaboration with the tourist industry, but the problem here is how to get it started? We hardly have any formal or professional industry-to-industry communication before. How can we, people from both sides, come to a consensus about the goals we want to achieve and how? I find the idea very meaningful but novel. That means we need strong leadership here to help both sides come together, talk in the same language and work together’(PH2)
‘One relies on the Macao Government to do something to prevent COVID-19; therefore, lending themselves to wait and expect that the government do whatever is necessary because of the belief that this is beyond their reach to have an impact. There is no initiative to talk with different stakeholders. There is a lack of dialogue and thinking that others can do their job on their behalf. If the dialogue was not easy when business was running high, now that business is running low, everyone says that they are too busy to stop and reflect’(TE8)
‘I know my professional responsibilities should extend towards the tourists. I guess I need to have a “blueprint” about what is expected of me and how I should practise meeting the expectations. However, the more troublesome experiences are about the tourists themselves. Many of them do not use us as healthcare professionals but just salespersons. They are probably not aware that we are trained and licensed health professionals’(PH3)
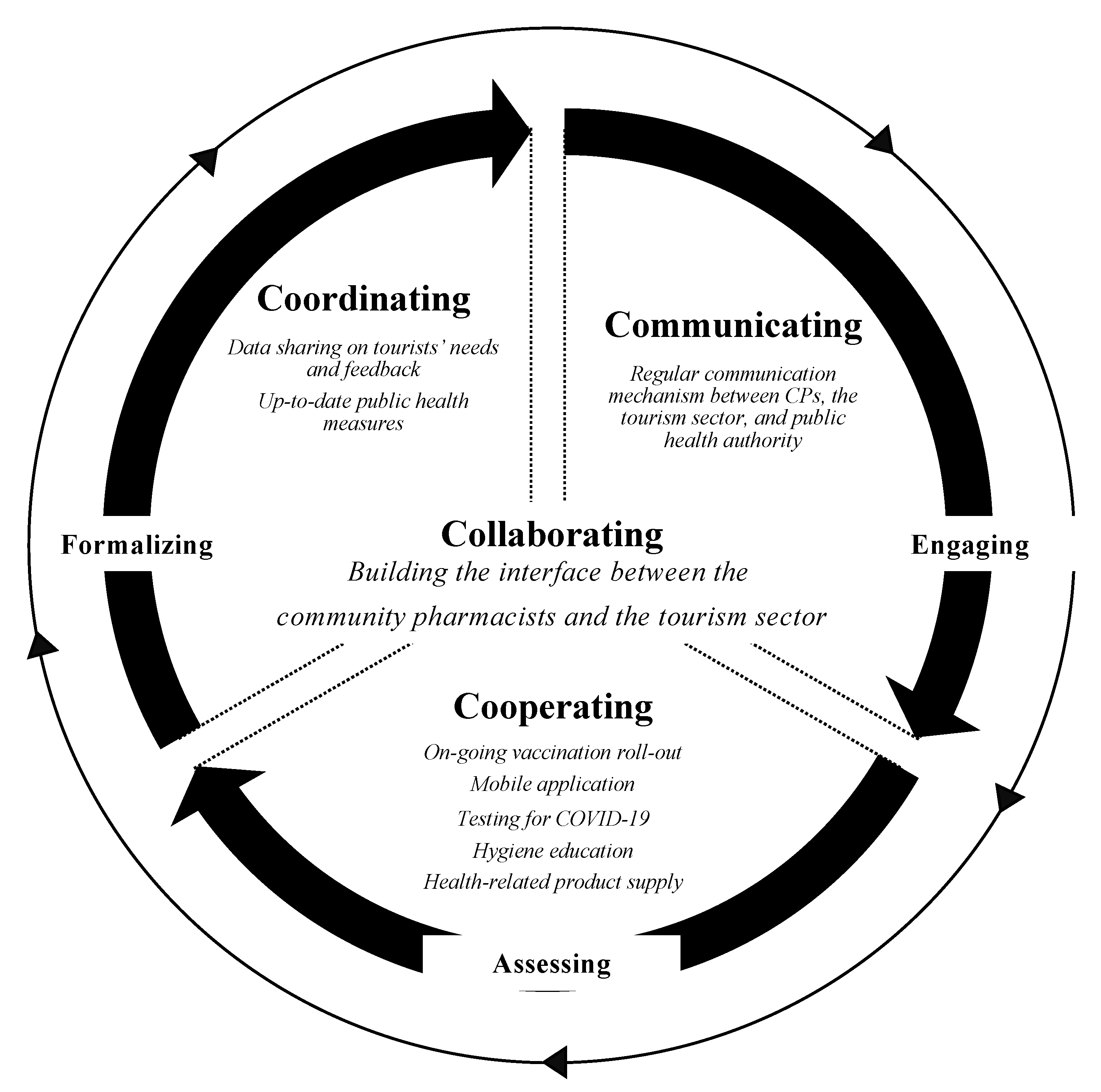
5.4. The 4C’s for a Macao COVID-19 Tourism Recovery Strategy
‘Maybe some of them are not confident enough to know when and how to make referrals. That needs to be reinforced. At the same time, the public and the tourists need to be educated about us as a health resource at the community level who they can turn to in case of any concerns about the pandemic. Such awareness should be raised so that they know where to look for help and support’(PH4)
‘I guess we need to have some sort of initiative to kick start the realisation of this conceptual idea. Pharmacists or pharmacies alone may not be in the position to initiate such communication and further collaboration. Representatives from the tourist industry should take a more proactive role in the initial stage’(PH2)
‘I guess this should be a coordinated effort somehow under the government’s leadership as this is, after all, an issue of public health and economic recovery for Macao. Based on the past nine months’ outbreak experiences, the government has a pivotal role in coordinating different sectors. The government must recognise such collaborative effort’(PH5)
‘There should be an internationally recognised certification of testing, results, drugs and therapeutics in Macao’(TE7)
‘The government needs to arrange a certification process to qualify pharmacists to do vaccination, but this is not consensual because these new vaccines are more unpredictable than the ones previously developed over the decades. The government needs to address this to the medical community so that the Universities and main accreditation bodies are involved’(TE1)
‘The use of Macao as a mass vaccination destination should be considered… VIP gaming facilities have in-house hospitals to provide gamblers and their families with a vaccine as part of the package. Casinos could reinvent themselves to become mass “vaccination” (vaccination + visitation) points’(TE5)
5.5. Collaboration That Creates Actions by Pharmacists and Tourism Professionals
‘There is currently a lack of transparency between the two, a lack of involvement by each party, and a lack of information shared by each party’(TE2)
‘Transparency is always key to this type of strategy, both internally and externally’(TE7)
‘The expectations from each side should be communicated clearly, and an action plan should be designed and followed through. I guess we can try a pilot by engaging one or two chain pharmacy companies in the project. This should proceed quickly as the borders are opening up already, and it will be some time before the key messages can get to the tourists’(PH1)
‘It is important for the tourist industry to be committed in terms of communication with the pharmacy sector and provide the support needed. Education, meetings, lobbying, accreditation, and promotion are all actions consuming resources. Really, I don’t think pharmacies can bear all the costs nor would they be in any position to provide the resources needed’(PH4)
‘There should be awareness that the pharmacies are the places to get actual medication versus overpriced supplements’(TE4)
‘We need to ensure the authorities overseeing the pharmaceutical industry determine the best COVID-19 vaccines to be imported to the city’(TE5)
5.6. How the Collaborative Relationship Should Be Monitored and Evaluated
‘An independent medical professional body that collaborates with WHO and a regional CDC (like the USA) could review what the Macao authorities are doing in comparison to how the region is handling the evolution of the pandemic, as well as monitoring the new vaccine effectiveness through time’(TE6)
‘As I mention before, the design of the collaboration should have an evaluation mechanism built in already. In the health sector, the use of an ECHO model is common when testing any new interventions. ECHO stands for the economic, clinical and humanistic outcomes. I think the easiest way to evaluate is to monitor the humanistic outcome of the collaboration. For example, using a survey and simply randomly asking the tourists about their experience with certain services provided out of the collaboration would be feasible’(PH5)
‘The outcome for us is really about how many more tourists the collaborative services can drive to our pharmacy and how it translates into our business performance. I am trying to be practical here. Eventually, the community pharmacy is a business…. A professional image is one, but it is not tangible. Positive impact on the business is core. With good services and good promotion through the tourism network, I believe there are many advantages for pharmacies to participate’(PH4)
5.7. How the Collaborative Relationship Should Be Sustained, even after COVID-19
‘First, there should be legislation or reinforcement on the existing one for pharmacists—an official government certification system which recognises highly qualified pharmacist professionals’(TE5)
‘They (pharmacists) need a good public relations campaign to revamp their image: from shops that have sprung up to benefit from Chinese tourism to shops that we can trust actually to sell us what we need’(TE4)
‘Any outreach to CPs should not cannibalise on resources needed to combat COVID-19’(TE1)
6. Major Contribution
6.1. Theoretical Contribution
6.2. Practical Contribution
6.2.1. Active Surveillance and Orientation
6.2.2. Tourist and Public Education
6.2.3. Provision of Medicines and Other Quality Health-Related Products
7. Discussion
8. Results Recommendations
9. Conclusions
10. Limitations and Future Scope
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hernández, J.M. SARS-CoV-2 Risk Misclassification Explains Poor COVID-19 Management. Lancet Lond. Engl. 2020, 396, 1733–1734. [Google Scholar] [CrossRef]
- Rodríguez-Antón, J.M.; Alonso-Almeida, M. del M. COVID-19 Impacts and Recovery Strategies: The Case of the Hospitality Industry in Spain. Sustainability 2020, 12, 8599. [Google Scholar] [CrossRef]
- Atalan, A. Is the Lockdown Important to Prevent the COVID-19 Pandemic? Effects on Psychology, Environment and Economy-Perspective. Ann. Med. Surg. 2020, 56, 38–42. [Google Scholar] [CrossRef]
- Oraby, T.; Tyshenko, M.G.; Maldonado, J.C.; Vatcheva, K.; Elsaadany, S.; Alali, W.Q.; Longenecker, J.C.; Al-Zoughool, M. Modeling the Effect of Lockdown Timing as a COVID-19 Control Measure in Countries with Differing Social Contacts. Sci. Rep. 2021, 11, 3354. [Google Scholar] [CrossRef] [PubMed]
- Vinceti, M.; Filippini, T.; Rothman, K.J.; Ferrari, F.; Goffi, A.; Maffeis, G.; Orsini, N. Lockdown Timing and Efficacy in Controlling COVID-19 Using Mobile Phone Tracking. EClinicalMedicine 2020, 25, 100457. [Google Scholar] [CrossRef]
- Plümper, T.; Neumayer, E. Lockdown Policies and the Dynamics of the First Wave of the SARS-CoV-2 Pandemic in Europe. J. Eur. Public Policy 2020, 27, 1–21. [Google Scholar] [CrossRef]
- Duan, L.; Zhu, G. Psychological Interventions for People Affected by the COVID-19 Epidemic. Lancet Psychiatry 2020, 7, 300–302. [Google Scholar] [CrossRef]
- Bausch, T.; Gartner, W.C.; Ortanderl, F. How to Avoid a COVID-19 Research Paper Tsunami? A Tourism System Approach. J. Travel Res. 2021, 60, 467–485. [Google Scholar] [CrossRef]
- Purcell, W.M.; Burns, O.; Voss, A. COVID-19 and Sustainable Tourism. In COVID-19: Paving the Way for a More Sustainable World; Leal Filho, W., Ed.; World Sustainability Series; Springer International Publishing: Cham, Switzerland, 2021; pp. 163–184. ISBN 978-3-030-69284-1. [Google Scholar]
- Helble, M.; Park, C.-Y.; Cho, W.H.; Cortes, S.F. Can Vaccination Help Restart Tourism? ADB Briefs; Asian Development Bank: Manila, Philippines, 2021. [Google Scholar]
- Wang, M.; Kunasekaran, P.; Rasoolimanesh, S.M. What Influences People’s Willingness to Receive the COVID-19 Vaccine for International Travel? Curr. Issues Tour. 2021, 1–6. [Google Scholar] [CrossRef]
- McCartney, G.; Pinto, J. Macao’s COVID-19 Responses: From Virus Elimination Success to Vaccination Rollout Challenges. Lancet Reg. Health-West. Pac. 2021, 11, 100169. [Google Scholar] [CrossRef]
- Wen, J.; Wang, W.; Kozak, M.; Liu, X.; Hou, H. Many Brains Are Better than One: The Importance of Interdisciplinary Studies on COVID-19 in and beyond Tourism. Tour. Recreat. Res. 2021, 46, 310–313. [Google Scholar] [CrossRef]
- Koch, S.; Yoon, L.; Gils, B. From the Exposome to the Socioexposome in COVID-19 Research—A Call for More Multidisciplinary Research. JAMA Netw. Open 2020, 3, e2032287. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Hotopf, M.; Worthman, C.M.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; et al. Multidisciplinary Research Priorities for the COVID-19 Pandemic—Authors’ Reply. Lancet Psychiatry 2020, 7, e44–e45. [Google Scholar] [CrossRef]
- Parajuli, R.R.; Mishra, B.; Banstola, A.; Ghimire, B.R.; Poudel, S.; Sharma, K.; Dixit, S.M.; Sah, S.K.; Simkhada, P.; van Teijlingen, E. Multidisciplinary Approach to COVID-19 Risk Communication: A Framework and Tool for Individual and Regional Risk Assessment. Sci. Rep. 2020, 10, 21650. [Google Scholar] [CrossRef]
- Arencibia-Jorge, R.; García-García, L.; Galban-Rodriguez, E.; Carrillo-Calvet, H. The Multidisciplinary Nature of COVID-19 Research. Iberoam. J. Sci. Meas. Commun. 2021, 1, 394312. [Google Scholar] [CrossRef]
- Dawoud, D. Emerging from the Other End: Key Measures for a Successful COVID-19 Lockdown Exit Strategy and the Potential Contribution of Pharmacists. Res. Soc. Adm. Pharm. 2021, 17, 1950–1953. [Google Scholar] [CrossRef]
- Peto, J.; Alwan, N.A.; Godfrey, K.M.; Burgess, R.A.; Hunter, D.J.; Riboli, E.; Romer, P.; Buchan, I.; Colbourn, T.; Costelloe, C.; et al. Universal Weekly Testing as the UK COVID-19 Lockdown Exit Strategy. Lancet 2020, 395, 1420–1421. [Google Scholar] [CrossRef]
- Ung, C.O.L. Community Pharmacist in Public Health Emergencies: Quick to Action against the Coronavirus 2019-NCoV Outbreak. Res. Soc. Adm. Pharm. RSAP 2020, 16, 583–586. [Google Scholar] [CrossRef]
- McCartney, G.; Pinto, J.; Liu, M. City Resilience and Recovery from COVID-19: The Case of Macao. Cities 2021, 112, 103130. [Google Scholar] [CrossRef]
- Macao SAR Government. Statistics and Census Service Statistics -- Statistics and Census Service. Available online: https://www.dsec.gov.mo/en-US/Statistic?id=402 (accessed on 14 December 2021).
- Macao SAR Government Tourism Office. Measures and Important Notes for Tourists Visiting Macao—Macao Government Tourism Office. Available online: https://www.macaotourism.gov.mo/en/article/notice/covid19-notice (accessed on 15 December 2021).
- World Travel and Tourism Council. Travel & Tourism Economic Impact | World Travel & Tourism Council (WTTC). Available online: https://wttc.org/Research/Economic-Impact (accessed on 14 December 2021).
- Macao SAR Government. Health Bureau News. Available online: https://www.ssm.gov.mo/Portal/portal.aspx?lang=pt (accessed on 23 March 2021).
- Zhang, M.Y.; Chong, W.K.; Hu, H.; Wang, Y. Pharmacy-Perceived Consumer Preferences: A Survey of Community Pharmacies in Macau. J. Med. Mark. 2014, 14, 41–48. [Google Scholar] [CrossRef]
- Macao SAR Government. Cartography and Cadastre Bureau Cartography and Cadastre Bureau. Available online: https://www.dscc.gov.mo/en/geographical_typeMap.html (accessed on 14 December 2021).
- Brüning, H. Over 200 Million ‘Government Masks’ Sold in Macau. Macau Post Dly. 2021, 112, 103130. [Google Scholar]
- Choi, B.; Pak, A. Multidisciplinarity, Interdisciplinarity and Transdisciplinarity in Health Research, Services, Education and Policy: 1. Definitions, Objectives, and Evidence of Effectiveness. Clin. Investig. Med. Médecine Clin. Exp. 2007, 29, 351–364. [Google Scholar]
- Iskander, J.K.; Bianchi, K.M. Changes in the Scientific Information Environment During the COVID-19 Pandemic: The Importance of Scientific Situational Awareness in Responding to the Infodemic. Health Secur. 2021, 19, 82–87. [Google Scholar] [CrossRef]
- Yang, S.; Carlson, J.R.; Chen, S. How Augmented Reality Affects Advertising Effectiveness: The Mediating Effects of Curiosity and Attention toward the Ad. J. Retail. Consum. Serv. 2020, 54, 102020. [Google Scholar] [CrossRef]
- Peek, L.; Guikema, S. Interdisciplinary Theory, Methods, and Approaches for Hazards and Disaster Research: An Introduction to the Special Issue. Risk Anal. Off. Publ. Soc. Risk Anal. 2021, 41, 1047–1058. [Google Scholar] [CrossRef]
- Sharma, G.D.; Thomas, A.; Paul, J. Reviving Tourism Industry Post-COVID-19: A Resilience-Based Framework. Tour. Manag. Perspect. 2021, 37, 100786. [Google Scholar] [CrossRef] [PubMed]
- Robina-Ramírez, R.; Sánchez, M.S.-O.; Jiménez-Naranjo, H.V.; Castro-Serrano, J. Tourism Governance during the COVID-19 Pandemic Crisis: A Proposal for a Sustainable Model to Restore the Tourism Industry. Environ. Dev. Sustain. 2021, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.A.; Gonzalez, M.C.; Haegeman, K.; Rainoldi, A. Behavioural Changes in Tourism in Times of COVID-19. The Joint Research Centre Science for Policy Report; European Commission: Brussels, Belgium, 2020. [Google Scholar]
- Bedwell, W.L.; Wildman, J.L.; DiazGranados, D.; Salazar, M.; Kramer, W.S.; Salas, E. Collaboration at Work: An Integrative Multilevel Conceptualization. Hum. Resour. Manag. Rev. 2012, 22, 128–145. [Google Scholar] [CrossRef]
- Martin, R.; Sunley, P.; Gardiner, B.; Tyler, P. How Regions React to Recessions: Resilience and the Role of Economic Structure. Reg. Stud. 2016, 50, 561–585. [Google Scholar] [CrossRef] [Green Version]
- Kapucu, N.; Garayev, V. Collaborative Decision-Making in Emergency and Disaster Management. Int. J. Public Adm. 2011, 34, 366–375. [Google Scholar] [CrossRef]
- Clarke, A.; Crane, A. Cross-Sector Partnerships for Systemic Change: Systematized Literature Review and Agenda for Further Research. J. Bus. Ethics 2018, 150, 303–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuh, G.; Potente, T.; Varandani, R.; Hausberg, C.; Fränken, B. Collaboration Moves Productivity to the Next Level. Procedia CIRP 2014, 17, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Rice, R.; Atkin, C. Public Communication Campaigns, 3rd ed.; SAGE Knowledge: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- Flanagin, A.J.; Bator, M. The Utility of Information and Communication Technologies in Organizational Knowledge Management. In Communication and Organizational Knowledge; Routledge: London, UK, 2010; ISBN 978-0-203-87450-9. [Google Scholar]
- Porter, M.E. Clusters and the New Economics of Competition. Harv. Bus. Rev. 1998, 76 6, 77–90. [Google Scholar]
- Kohn, A. No Contest: The Case Against Competition; Houghton Mifflin Harcourt: Boston, MA, USA, 1992; ISBN 978-0-395-63125-6. [Google Scholar]
- Han, E.; Tan, M.M.J.; Turk, E.; Sridhar, D.; Leung, G.M.; Shibuya, K.; Asgari, N.; Oh, J.; García-Basteiro, A.L.; Hanefeld, J.; et al. Lessons Learnt from Easing COVID-19 Restrictions: An Analysis of Countries and Regions in Asia Pacific and Europe. Lancet 2020, 396, 1525–1534. [Google Scholar] [CrossRef]
- Cadogan, C.A.; Hughes, C.M. On the Frontline against COVID-19: Community Pharmacists’ Contribution during a Public Health Crisis. Res. Soc. Adm. Pharm. RSAP 2021, 17, 2032–2035. [Google Scholar] [CrossRef] [PubMed]
- Visacri, M.B.; Figueiredo, I.V.; Lima, T.d.M. Role of Pharmacist during the COVID-19 Pandemic: A Scoping Review. Res. Soc. Adm. Pharm. RSAP 2021, 17, 1799–1806. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services Trump Administration Partners with Chain and Independent Community Pharmacies to Increase Access to Future COVID-19 Vaccines. Available online: https://www.hhs.gov/about/news/2020/11/12/trump-administration-partners-chain-independent-community-pharmacies-increase-access-future-covid-19-vaccines.html (accessed on 28 April 2021).
- CDC-Center for Disease Control Influenza Vaccinations Administered to Adults in Pharmacies and Physician Medical Offices, United States | FluVaxView | Seasonal Influenza (Flu) | CDC. Available online: https://www.cdc.gov/flu/fluvaxview/dashboard/vaccination-administered.html (accessed on 28 April 2021).
- Lau, Y. Looking beyond COVID-19 as a Pandemic. HONG KONG Med. J. 2021, 27, 88–89. [Google Scholar] [CrossRef]
- Kaushal, V.; Srivastava, S. Hospitality and Tourism Industry amid COVID-19 Pandemic: Perspectives on Challenges and Learnings from India. Int. J. Hosp. Manag. 2021, 92, 102707. [Google Scholar] [CrossRef]
- Uğur, N.G.; Akbıyık, A. Impacts of COVID-19 on Global Tourism Industry: A Cross-Regional Comparison. Tour. Manag. Perspect. 2020, 36, 100744. [Google Scholar] [CrossRef]
- Chang, C.-L.; McAleer, M.; Ramos, V. A Charter for Sustainable Tourism after COVID-19. Sustainability 2020, 12, 3671. [Google Scholar] [CrossRef]
- French Government Ministry of Solidarity and Health How to obtain a health pass in case of vaccination abroad? Available online: https://www.sante.fr/how-to-obtain-a-french-health-pass (accessed on 15 December 2021).
- Governo Regional da Madeira. Resolução n.o 1208/2021 da Presidência do Governo Regional da Madeira; Journal Oficial da Região Autónoma da Madeira: Madeira, Portugal, 2021.
- Mukattash, T.L.; Jarab, A.S.; Mukattash, I.; Nusair, M.B.; Farha, R.A.; Bisharat, M.; Basheti, I.A. Pharmacists’ Perception of Their Role during COVID-19: A Qualitative Content Analysis of Posts on Facebook Pharmacy Groups in Jordan. Pharm. Pract. 2020, 18, 1900. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. Pharmacy: A Way Forward for Public Health, Opportunities for Action through Pharmacy for Public Health; Public Health England: Londok, UK, 2017; p. 53.
- WHO. W.H.O. Coronavirus Disease (COVID-19)—World Health Organization. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 8 August 2021).
- Daszak, P.; Olival, K.J.; Li, H. A Strategy to Prevent Future Epidemics Similar to the 2019-NCoV Outbreak. Biosaf. Health 2020, 2, 6–8. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.G.P.; Crowe, S.M.; Tyndall, M.W. Planning for the Next Global Pandemic. Int. J. Infect. Dis. 2015, 38, 89–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novelli, M.; Gussing Burgess, L.; Jones, A.; Ritchie, B.W. ‘No Ebola…still Doomed’—The Ebola-Induced Tourism Crisis. Ann. Tour. Res. 2018, 70, 76–87. [Google Scholar] [CrossRef]
- Saker, L.; Lee, K.; Cannito, B.; Gilmore, A.; Campbell-Lendrum, D. Globalization and Infectious Diseases: A Review of the Linkages; Special Topics No. 3; World Health Organization on Behalf of the Special Programme for research and training in Tropical Diseases -TDR Steering Committee for Social; Economic and Behavioral Research: Geneva, Switzerland, 2004; p. 67. [Google Scholar]
- Ayeh, J.K.; Leung, D.; Au, N.; Law, R. Perceptions and Strategies of Hospitality and Tourism Practitioners on Social Media: An Exploratory Study. In Proceedings of the Information and Communication Technologies in Tourism 2012, Helsingborg, Sweden, 25-27 January 2012; Fuchs, M., Ricci, F., Cantoni, L., Eds.; Springer: Vienna, Austria, 2012; pp. 1–12. [Google Scholar]
- Granville, F.; Mehta, A.; Pike, S. Destinations, Disasters and Public Relations: Stakeholder Engagement in Multi-Phase Disaster Management. J. Hosp. Tour. Manag. 2016, 28, 73–79. [Google Scholar] [CrossRef]
- Radic, A.; Lück, M.; Al-Ansi, A.; Chua, B.-L.; Seeler, S.; Han, H. Cruise Ship Dining Experiencescape: The Perspective of Female Cruise Travelers in the Midst of the COVID-19 Pandemic. Int. J. Hosp. Manag. 2021, 95, 102923. [Google Scholar] [CrossRef]
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample Size in Qualitative Interview Studies: Guided by Information Power. Qual. Health Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef]
- Jiang, Y.; Ritchie, B.W. Disaster Collaboration in Tourism: Motives, Impediments and Success Factors. J. Hosp. Tour. Manag. 2017, 31, 70–82. [Google Scholar] [CrossRef]
- Bryant, A.; Charmaz, K. The SAGE Handbook of Grounded Theory; SAGE: Thousand Oaks, CA, USA, 2007; ISBN 978-1-4462-7572-6. [Google Scholar]
- Glaser, B.G.; Strauss, A.L. The Discovery of Grounded Theory: Strategies for Qualitative Research; 4. paperback printing; Aldine Publishing: New Brunswick, NJ, USA, 2009; ISBN 978-0-202-30260-7. [Google Scholar]
- Lai, I.K.W.; Wong, J.W.C. Comparing Crisis Management Practices in the Hotel Industry between Initial and Pandemic Stages of COVID-19. Int. J. Contemp. Hosp. Manag. 2020, 32, 3135–3156. [Google Scholar] [CrossRef]
- Cioccio, L.; Michael, E.J. Hazard or Disaster: Tourism Management for the Inevitable in Northeast Victoria. Tour. Manag. 2007, 28, 1–11. [Google Scholar] [CrossRef]
- Fyall, A.; Garrod, B.; Wang, Y. Destination Collaboration: A Critical Review of Theoretical Approaches to a Multi-Dimensional Phenomenon. J. Destin. Mark. Manag. 2012, 1, 10–26. [Google Scholar] [CrossRef]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary Research Priorities for the COVID-19 Pandemic: A Call for Action for Mental Health Science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Jamal, T.B.; Getz, D. Collaboration Theory and Community Tourism Planning. Ann. Tour. Res. 1995, 22, 186–204. [Google Scholar] [CrossRef]
- Graci, S. Collaboration and Partnership Development for Sustainable Tourism. Tour. Geogr. 2013, 15, 25–42. [Google Scholar] [CrossRef]
- Scarpino, M.R.; Gretzel, U. Conceptualizing Organizational Resilience in Tourism Crisis Management. Tour. Crisis Disaster Manag. Asia-Pac. 2014, 1, 15. [Google Scholar]
- Ansell, C.; Gash, A. Collaborative Platforms as a Governance Strategy. J. Public Adm. Res. Theory 2018, 28, 16–32. [Google Scholar] [CrossRef]
- Kumar, G.; Nath Banerjee, R. Collaboration in Supply Chain: An Assessment of Hierarchical Model Using Partial Least Squares (PLS). Int. J. Product. Perform. Manag. 2012, 61, 897–918. [Google Scholar] [CrossRef]
- Ritchie, B.W. Chaos, Crises and Disasters: A Strategic Approach to Crisis Management in the Tourism Industry. Tour. Manag. 2004, 25, 669–683. [Google Scholar] [CrossRef]
- Jamal, T.; Stronza, A. Collaboration Theory and Tourism Practice in Protected Areas: Stakeholders, Structuring and Sustainability. J. Sustain. Tour. 2009, 17, 169–189. [Google Scholar] [CrossRef]
- Bullock, R.; Armitage, D.; Mitchell, B. Shadow Networks, Social Learning, and Collaborating through Crisis: In Collaborative Resilience; Moving Through Crisis to Opportunity; Goldstein, B.E., Ed.; The MIT Press: Cambridge, MA, USA, 2012; pp. 309–338. ISBN 978-0-262-51645-7. [Google Scholar]
- Goldstein, B.E. Collaborative Resilience: Moving Through Crisis to Opportunity; The MIT Press: Cambridge, MA, USA, 2012; ISBN 978-0-262-51645-7. [Google Scholar]
- Al-Quteimat, O.M.; Amer, A.M. SARS-CoV-2 Outbreak: How Can Pharmacists Help? Res. Soc. Adm. Pharm. RSAP 2021, 17, 480–482. [Google Scholar] [CrossRef]
- American Pharmacists Association Advocacy Issues. Available online: https://pharmacist.com/Advocacy/Issues (accessed on 28 April 2021).
- Bregoli, I.; Del Chiappa, G. Coordinating Relationships Among Destination Stakeholders: Evidence from Edinburgh (UK). Tour. Anal. 2013, 18, 145–155. [Google Scholar] [CrossRef]
- Hartman, S. Resilient Tourism Destinations? Governance Implications of Bringing Theories of Resilience and Adaptive Capacity to Tourism Practice; Routledge: Oxfordshire, UK, 2018; pp. 66–76. ISBN 978-0-203-70190-4. [Google Scholar]
- Johnson, R.; McGowan, M.; Turner, L. Grounded Theory in Practice: Is It Inherently a Mixed Method? Psychol. Sch. 2010, 13, 65–78. [Google Scholar]
- Elbeddini, A.; Prabaharan, T.; Almasalkhi, S.; Tran, C. Pharmacists and COVID-19. J. Pharm. Policy Pract. 2020, 13, 36. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Luo, P.; Tang, M.; Hu, Q.; Polidoro, J.P.; Sun, S.; Gong, Z. Providing Pharmacy Services during the Coronavirus Pandemic. Int. J. Clin. Pharm. 2020, 42, 299–304. [Google Scholar] [CrossRef] [Green Version]
- Hansson, S.; Orru, K.; Torpan, S.; Bäck, A.; Kazemekaityte, A.; Meyer, S.F.; Ludvigsen, J.; Savadori, L.; Galvagni, A.; Pigrée, A. COVID-19 Information Disorder: Six Types of Harmful Information during the Pandemic in Europe. J. Risk Res. 2021, 24, 1–14. [Google Scholar] [CrossRef]
- Gao, Y.; Cai, G.-Y.; Fang, W.; Li, H.-Y.; Wang, S.-Y.; Chen, L.; Yu, Y.; Liu, D.; Xu, S.; Cui, P.-F.; et al. Machine Learning Based Early Warning System Enables Accurate Mortality Risk Prediction for COVID-19. Nat. Commun. 2020, 11, 5033. [Google Scholar] [CrossRef]
- Campiranon, K.; Scott, N. Critical Success Factors for Crisis Recovery Management: A Case Study of Phuket Hotels. J. Travel Tour. Mark. 2014, 31, 313–326. [Google Scholar] [CrossRef] [Green Version]
- Mahase, E. COVID-19: “Mix and Match” Primary Vaccines Are Safe and Effective, Study Finds. BMJ 2021, 375, n3030. [Google Scholar] [CrossRef]
- Zheng, S.; Yang, L.; Zhou, P.; Li, H.; Liu, F.; Zhao, R. Recommendations and Guidance for Providing Pharmaceutical Care Services during COVID-19 Pandemic: A China Perspective. Res. Soc. Adm. Pharm. 2021, 17, 1819–1824. [Google Scholar] [CrossRef]
- Indar, L.; Hospedales, C.J.; Asin-Oostburg, V. Developing Policy to Support Novel Caribbean Tourism and Health Surveillance Program. Online J. Public Health Inform. 2018, 10, e72. [Google Scholar] [CrossRef] [Green Version]
- Haider, N.; Yavlinsky, A.; Simons, D.; Osman, A.Y.; Ntoumi, F.; Zumla, A.; Kock, R. Passengers’ Destinations from China: Low Risk of Novel Coronavirus (2019-NCoV) Transmission into Africa and South America. Epidemiol. Infect. 2020, 148, e41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Pharmaceutical Federation COVID-19 Hub. Available online: https://www.fip.org//coronavirus (accessed on 15 December 2021).
- UNWTO. COVID-19 Tourism Recovery Techincal Assistance Package. Available online: https://www.unwto.org/tourism-covid-19 (accessed on 13 January 2022).
- Blackman, D.; Kennedy, M.; Ritchie, B. Knowledge Management: The Missing Link in DMO Crisis Management? Curr. Issues Tour. 2011, 14, 337–354. [Google Scholar] [CrossRef]

| Interviewees (Code) | Age (Years) | Gender | Role |
|---|---|---|---|
| PH1 | 45–54 | M | Owner of a community pharmacy |
| PH2 | 45–54 | F | Manager of a chain pharmacy company |
| PH3 | 35–44 | M | Community pharmacist |
| PH4 | 55–64 | F | Representative of a pharmacy association |
| PH5 | 35–44 | M | Representative of a pharmacist profession organisation |
| PH6 | 55–64 | M | Manager of a chain pharmacy company |
| TE1 | 55–64 | M | Managing Director, Integrated Resort Advisor |
| TE2 | 45–54 | F | Managing Director, Integrated Resort Advisor |
| TE3 | 35–44 | F | Airline CEO |
| TE4 | 45–54 | M | Executive Director, Front Office Operations |
| TE5 | 45–54 | M | Managing Director of Destination Management Company |
| TE6 | 45–54 | M | Senior Vice President of Conventions and Exhibitions |
| TE7 | 35–44 | M | Executive Director of Food and Beverage |
| TE8 | 35–44 | F | Managing Director of Travel Agency |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McCartney, G.; Ung, C.O.L.; Pinto, J.F. Living with COVID-19 and Sustaining a Tourism Recovery—Adopting a Front-Line Collaborative Response between the Tourism Industry and Community Pharmacists. Tour. Hosp. 2022, 3, 47-68. https://doi.org/10.3390/tourhosp3010004
McCartney G, Ung COL, Pinto JF. Living with COVID-19 and Sustaining a Tourism Recovery—Adopting a Front-Line Collaborative Response between the Tourism Industry and Community Pharmacists. Tourism and Hospitality. 2022; 3(1):47-68. https://doi.org/10.3390/tourhosp3010004
Chicago/Turabian StyleMcCartney, Glenn, Carolina Oi Lam Ung, and José Ferreira Pinto. 2022. "Living with COVID-19 and Sustaining a Tourism Recovery—Adopting a Front-Line Collaborative Response between the Tourism Industry and Community Pharmacists" Tourism and Hospitality 3, no. 1: 47-68. https://doi.org/10.3390/tourhosp3010004
APA StyleMcCartney, G., Ung, C. O. L., & Pinto, J. F. (2022). Living with COVID-19 and Sustaining a Tourism Recovery—Adopting a Front-Line Collaborative Response between the Tourism Industry and Community Pharmacists. Tourism and Hospitality, 3(1), 47-68. https://doi.org/10.3390/tourhosp3010004