Abstract
COVID-19 is a pandemic that has affected health care personnel worldwide. Dentists have a high risk of contracting COVID-19 given the face-to-face contact required in daily interactions with their patients. This study aimed to determine the stressors experienced by academic dentists due to the COVID-19 situation in Trinidad and Jamaica. All academic staff at the University of the West Indies (UWI) dental schools (St. Augustine and Mona campuses) were invited to complete a self-reported questionnaire, which was conducted for one month from May to June 2020. Thirty-two dental academics responded and the response rate was 61.54%. More than a third (34.4%) were in the 25–35 age group, 71.9% were females. The most common speciality (20.7%) was restorative dentistry. Just over one-third (38.7%) had been in academia for 5–10 years. Most (40.6%) were apprehensive about infecting their family. When the locus of control was determined, just over half (53.1%) felt they were in control of protecting themselves while 34.4% felt that external factors controlled their lives. The findings suggest that academic staff at UWI dental schools (Trinidad and Jamaica) were stressed by the COVID-19 situation. The vast majority were worried about infecting their families.
1. Introduction
The coronavirus disease of 2019, known as COVID-19, is caused by a novel coronavirus termed SARS-CoV-2 [1]. The virus can spread from person to person, includes a range of respiratory symptoms and its incubation period varies from 3 to 14 days and is more contagious than the seasonal flu [1]. The initial outbreak of the novel coronavirus COVID-19 began in Wuhan, China, towards the end of 2019 and soon became a pandemic in March 2020 [1]. There are many types of human coronaviruses that cause varying degrees of respiratory illness. This is one of the newest strains of human coronaviruses and is spread through droplet infection [2], aerosols and cross-contamination from objects to persons’ faces [1]. Moreover, there has been confirmation of transmission via persons with little to no symptoms [3]. The virus affects all persons including children and infants, however, to date, the elderly and persons with preexisting medical conditions have been more likely to be infected by the virus and develop severe symptoms as a result [2].
This study was conducted in May 2020, before the existence of vaccines and credible preventive medicines to counteract the disease, which were only available from November 2020 [2]. Vaccines have now passed the stage of clinical trials and received emergency approval, however, no vaccine is currently available in Trinidad and Tobago as of February 2021. The WHO continues to recommend social distancing of 3 to 6 m apart to prevent transmission of the virus [1]. However, this is impossible in the dental setting, given the varying risk of infection, based on whether or not aerosols are generated during treatment, which requires in-person communication and frequent contact with bodily fluids [4]. Research on fear and anxiety among dental health care professionals of being infected, given the mode of transmission, has found that 66% of dentists globally wanted to close their practices until there was a decline in the number of COVID-19 cases [5]. Additionally, in a recent publication in the New York Times [6], dentists were described as being at a high risk of contracting COVID-19, compared to other health care providers who were on the front line.
Governments worldwide attempted to reduce the burden on the health systems by implementing social measures, such as physical isolation, to “flatten the epidemiologic curve” which largely proved effective when executed early [7]. In Trinidad and Tobago, our first reported case was imported and subsequently, the government attempted to reduce the spread of infection via social distancing measures and a reduction in the movement of non-essential workers in the public [8]. These measures extended to the practice of dentistry, whereby, only emergency treatment was deemed necessary from March 2020 and all elective procedures were delayed until June 2020 [9]. The University of the West Indies (UWI) school of dentistry in Trinidad followed the guidelines set out by the Ministry of Health and closed the school in March 2020, until routine procedures were allowed and reopened in July 2020 [10]. These written guidelines involved social distancing practices, sanitization procedures and the use of PPE. During this period the academic staff continued to teach via online classes, whilst there was an uncertainty regarding the resumption of clinical teaching.
Currently, Trinidad and Tobago has 250 active cases, 135 deaths and a total of 7607 positive results for COVID-19 as of 4 February 2021 [10]. This is worrisome, given that the UN stated that the COVID-19 related deaths, per 100,000, in Trinidad and Tobago were similar to the mortality rates of the hardest hit European countries in April 2020 [11], when the number of deaths was at eight. The islands in the West Indies such as Trinidad and Tobago, as well as Jamaica, are at significant risk of negative economic consequences given the substantial health and economic risks to these islands which are largely dependent on some developed economies for tourism and imported goods [11]. The present pandemic has brought about mental distress among people due to the economic downturn; recent publications have opined that the level of mental distress due to the high levels of unemployment would lead to an increase in mental health issues [12]. Furthermore, during stressful periods persons may display symptoms of anxiety and depression, there are new concerns about the mental health of health care workers who have had to limit physical interaction with families as a result of the current pandemic [13].
During stressful periods such as a pandemic with a highly contagious virus, it is important to understand coping mechanisms, and in this study, the locus of control of the participants was assessed using a global scale which was validated previously [14]. The concept of locus of control was initially developed in 1966 by Rotter, who theorized that a person’s belief regarding the reasons for causative occurrences in that person’s life [14]. In other words, it defines whether or not a person believes that they can determine their outcome in various situations in life, or if it is as a fatalistic result of an external factor.
Given that this is a novel virus, the information on the dynamics of this infection is rapidly evolving. New information and research brought varying suggested guidelines and protocols for dentists [15], this in itself may have caused further stress to the academic dental staff at UWI and the authors felt that it was imperative to understand the reasons for stress and determine the locus of control amongst the academic staff at the UWI. This group of staff was chosen given the new demands to teach online, as well as their role as academics, in educating students, colleagues and supporting staff, regarding the transmission of the virus in a dental setting.
This study aimed to determine the stressors of academics, their demographics and the factors that affect the locus of control of the participants at the dental schools in the University of the West Indies (UWI).
2. Methods
An ethics waiver of consent was obtained from the UWI ethics committee and approval granted (CREC-SA.0357/05/2020), as the research did not involve any invasive procedures and was carried as per the Helsinki declaration. This study was cross-sectional and was conducted among the teaching staff at the UWI Schools of dentistry via an online platform for one month from April to May 2020. The questions were based on a review of the literature available at the time, on the fear and stress faced by dental academics. Face validity was performed on the questionnaire which was pilot tested on ten (10) participants and adjusted after comments on the questions were made by the subjects, to improve the comprehension of the questions. Therefore, any questions which were ambiguous or did not convey the exact meaning were rephrased. A link was sent to all academic staff of both dental schools via email which invited the participants to respond to the anonymous questionnaire, data were collected over one month. Participants were given a time frame to respond and were reminded to respond at fortnightly intervals.
The questionnaire was comprised of a total of 39 questions in total, 16 of which were closed-ended questions which included questions on demographics, internal and external locus of control, coping patterns and infection control practices in the dental setting, as well as questions on the highest level of qualifications, years spent in dental academia and experience in training dental students. Additionally, the remaining 23 questions used a 5-point Likert scale from 1—strongly disagree to 5—strongly agree on questions related to the pandemic and locus of control, as well as a 5-point Likert scale from 1—not worried at all to 5—very worried on various concerns in daily life. Data were organized and entered using Microsoft Excel (Microsoft Corp., Redwood, WA, USA) which was analyzed using SPSS (software package version 22, IBM, Armonk, NY, USA). Descriptive analyses, cross-tabulations and Pearson’s correlation were assessed for the multiple variables to determine the association between the variables.
3. Results
The population of academic staff members was comprised of 52 persons, there were 32 respondents, with a response rate of 61.54%, of these, 87.5% were stressed about the COVID-19 situation. More than a third (34.4%) were in the 25–35 age group, 71.9% were females (Table 1). The most common speciality was restorative dentistry (20.7%) however, most (44.8%) stated “other” for their speciality. More than half of the participants had postgraduate qualifications (Table 1). Just over one-third, (38.7%) had been in academia for 5–10 years (Table 1). In addition, 76.7% stated that they triaged their patients and 56.3% had received online training on dealing with the COVID-19 situation. Moreover, the vast majority (92.9%) of our participants stated that they use personal protective equipment. There were no exposure and outcome variables as in the study and hence the study was largely descriptive in nature. There were no statistically significant differences between the variables in the demographics and the locus of control (Table 2).

Table 1.
Demographics of participants.
Table 2.
Locus of control of participants and p values.
Most (87.5%) stated that they were stressed about the COVID-19 situation in the West Indies. When asked about the level of concern the participants experienced regarding infecting their family, 40.6% were often worried followed by 37.5% who worried all the time (Table 3). Additionally, over one-third (34.4%) of respondents were worried all the time about getting infected from emergency clinics at UWI/private practice.
Table 3.
Levels of concern among participants.
The vast majority (96.9%) received social support and of these, most (64.5%) stated that they received the greatest support from their parents and relatives followed by 61.3% from both their spouse and children, as well as from their friends and university colleagues. Calling friends and colleagues over the phone/video call was the most common coping mechanism, used by 83.9% of the participants (Table 4).
Table 4.
Ways of coping.
The questions on external and internal locus of control (Figure 1 and Figure 2 respectively) showed that more than half (53.1%) of the respondents strongly agreed that COVID-19 changed their life to a new normal and three-quarters (75%) strongly agreed that they now practice social distancing. The vast majority (92.9%) stated that they use personal protective equipment such as dental goggles, masks, and gloves which was closely followed by most (89.3%) participants stating that “All health staff members wear protective clothing” (Table 5).
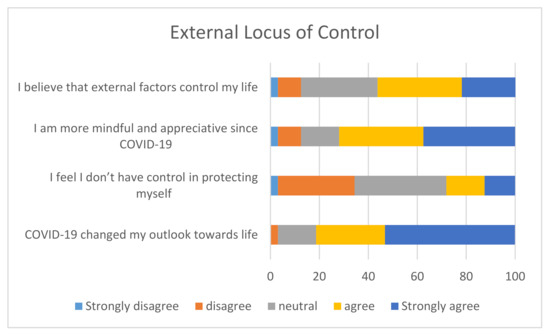
Figure 1.
External locus of control.
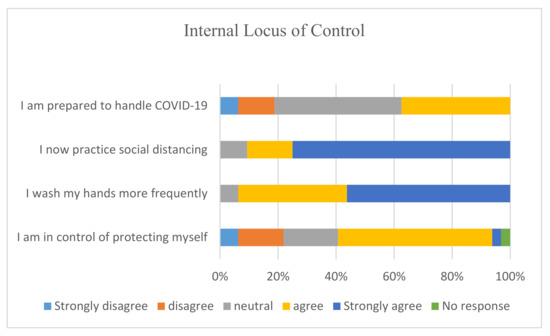
Figure 2.
Internal locus of control.
Table 5.
What participants practice, since COVID-19 *.
4. Discussion
This is a pilot study and is exploratory in nature which suggests cautiousness in interpreting the results given that the sample was comprised of only 32 persons. However, its strengths are that the UWI dental schools generally have small numbers of academics due to a small student intake and it is the first of its kind, regionally. The data were collected during the early stages of the pandemic and this research provides an insight into the levels of stress experienced by dental educators during the COVID-19 pandemic. The latter and its concomitant practices of physical isolation are believed to end in a variety of challenges both in the mental health and psychosocial spheres [16].
In a similar study, which also used an online-based questionnaire (Kwiksurveys) researchers found that the vast majority of their participants were afraid of infecting their families [5], which is comparable to our findings. Our results showed that most participants’ speciality was that of restorative dentistry, which may account for this concern of transmitting COVID-19. Since this virus has the potential to be transmitted via droplets and aerosols from infected patients in dental settings, adherence to strict infection control measures is of utmost importance in the prevention of its spread [4].
A recent study that used a self-administered questionnaire to assess the anxiety, knowledge and attitudes of dental professionals during the Swine flu pandemic, found that one-third of them were more reluctant to treat infected patients compared to their medical colleagues, even though there is a vaccine available for that virus [17]. Similarly, just over one-third of our participants were often worried about patient-to-patient transmission. However, it is important to provide dental care in emergency situations to reduce the patient load of healthcare organisations and hospitals which would already be inundated with patients [18]. This may also be a source of additional stress, related to the intensification of the responsibilities as a result of the rise in dental emergencies and virtual consultations required by academic dentists [19].
Another area which participants of this study felt stressed about was the ability of other islands in the Caribbean to be able to cope with COVID-19, which may be related to the expected reduction in the economies due to the global pandemic [11]. This concern may also have an impact on the participants’ fear of being laid off from work. Moreover, when the government of Trinidad and Tobago lifted restrictions on a phased basis, the public saw an incremental increase in the number of positive cases [10], this was similar to the findings of recent research which observed a rebound in the epidemic when interventions ended [7]. However, two months later, certain restrictions were reinstated by the government of Trinidad and Tobago to reduce the spread of the disease [20], although a return to the full measures of restriction cannot be expected given that it is economically unsustainable.
Furthermore, participants have ensured that all health staff members wear protective clothing but were concerned about the shortage of daily essentials, which is understandable, given the importance of personal protective equipment in reducing the risk of transmission of the virus. The consensus is that dentists who are currently treating patients should follow triaging protocols of checking patients’ temperatures and asking specific questions that assess the level of risk of exposure to the virus in addition to following infection control practices [21]. At the UWI, the dental school has implemented the triaging of all patients before their attendance at the clinics and installed sinks and hand sanitisers for the patients and staff before they enter the school. Additionally, all procedures are now performed in various zones according to their level of risk, for instance, those in which aerosols are generated are done in a separate zone from those without aerosols and require that personnel use extra PPE.
Coping mechanisms and social support are important factors in dealing with stress. This study found that while the majority of participants were stressed about the COVID-19 situation, they had social support systems and mechanisms to deal with the stress. In a recent study on the psychological experience of nurses of patients with COVID-19, their authors advocated for early psychological intervention and encouragement of social support to support psychological health, especially during an epidemic [22].
Further research has also shown that persons with a high external locus of control tend to have poorer survival after Acute Coronary Syndromes (ACS) and predictable coping mechanisms [16]. This research assessed the loci of control of dental academics who stated that they were stressed by the COVID-19 situation and gave the first insight into the areas in which the participants felt stressed. These findings may be useful when the university looks at strategies to reduce the levels of stress of its staff with appropriate coping mechanisms, based on the individual’s locus of control.
5. Limitations
- The data were collected during a period of the pandemic and the views of the participants may have changed based on various factors such as the prevalence of COVID-19 and dental protocols. However, the authors are currently conducting a large-scale data collection for a multinational study in Caribbean countries.
- A larger sample size may have been necessary to determine any statistically significant correlations between the parameters and the locus of control.
6. Suggestions
This is an evolving situation and more studies are needed to determine the levels of stress by their staff and ways in which the staff may be assisted in coping with the psychological consequences of the effects of the COVID-19 pandemic.
UWI may be able to provide further programs to reduce the stress of academics and probably improve mental health via meditation, counselling and health promotion seminars.
7. Conclusions
The findings suggest that dental academics are stressed by the COVID-19 situation and most are worried about infecting their families. Many participants had both coping mechanisms and social support. Provision of programs that focus on the locus of control may be useful in reducing mental stress during the COVID-19 pandemic.
Author Contributions
Conceptualisation, M.B. and R.B.; methodology and data collection, R.B., S.M. and W.S.; software, R.B., and W.S.; validation, R.B. and M.B.; formal analysis, R.B., M.B. and W.S.; writing—original draft preparation, R.B., M.B., S.M. and W.S.; writing-review and editing R.B., M.B., S.M. and W.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
The authors would like to thank Thaon Jones, Head of School of Dentistry, Mona, for his assistance with the coordination of this study and the staff at both dental schools who participated in the research.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Coronavirus Disease (COVID-19). 2020. Available online: https://www.who.int/news-room/q-a-detail/coronavirus-disease-covid-19 (accessed on 29 January 2021).
- How It Spreads|Coronavirus FAQ. 2020. Available online: https://faq.coronavirus.gov/spread/#how-does-the-virus-spread (accessed on 4 August 2020).
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Janke, C.; Guggemos, W.; et al. Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany. N. Engl. J. Med. 2020, 382, 970–971. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission routes of 2019-nCoV and controls in dental practice. Int. J. Oral Sci. 2020, 12, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.A.; Jouhar, R.; Ahmed, N.; Adnan, S.; Aftab, M.; Zafar, M.S.; Khurshid, Z. Fear and Practice Modifications among Dentists to Combat Novel Coronavirus Disease (COVID-19) Outbreak. Int. J. Environ. Res. Public Heal. 2020, 17, 2821. [Google Scholar] [CrossRef] [PubMed]
- Gamio, L. Reported Coronavirus Cases Top 5 Million Worldwide. 2020. Available online: https://www.nytimes.com/interactive/2020/03/15/business/economy/coronavirus-worker-risk.html?action=click&module=Top+Stories&pgtype=Homepage (accessed on 2 August 2020).
- Matrajt, L.; Leung, T. Evaluating the Effectiveness of Social Distancing Interventions to Delay or Flatten the Epidemic Curve of Coronavirus Disease. Emerg. Infect. Dis. 2020, 26, 1740–1748. [Google Scholar] [CrossRef] [PubMed]
- Editor. Non-Essential-Workers-Stay-Home. 2020. Available online: https://trinidadexpress.com/coronavirus/timeline/non-essential-workers-stay-home/article_2207a2da-8b46-11ea-9299-6b3a93f21586.html (accessed on 7 August 2020).
- Dental Council of Trinidad and Tobago 2020. Available online: https://dctt.org.tt/media_images/Covid%2019%20-%20Update%2010.pdf (accessed on 10 August 2020).
- Ministry of Health. Available online: https://health.gov.tt/covid-19 (accessed on 4 February 2021).
- The COVID-19 Pandemic puts Small Island Developing Economies in Dire Straits. Economic Analysis & Policy Division|Dept of Economic & Social Affairs|United Nations. 2020. Available online: https://www.un.org/development/desa/dpad/publication/un-desa-policy-brief-64-the-covid-19-pandemic-puts-small-island-developing-economies-in-dire-straits/#:~:text=1%20May%202020,The%20COVID%2D19%20pandemic%20puts%20Small%20island%20developing%20economies (accessed on 4 August 2020).
- Kawohl, W.; Nordt, C. COVID-19, unemployment, and suicide. Lancet Psychiatry 2020, 7, 389–390. [Google Scholar] [CrossRef]
- The Lancet Psychiatry. Isolation and Inclusion. Lancet Psychiatry 2020, 7, 371. [Google Scholar] [CrossRef]
- Rotter, J.B. Generalized expectancies for internal versus external control of reinforcement. Psychol. Monogr. Gen. Appl. 1966, 80, 1–28. [Google Scholar] [CrossRef]
- Alharbi, A.; Alharbi, S.; Alqaidi, S. Guidelines for dental care provision during the COVID-19 pandemic. Saudi Dent. J. 2020, 32, 181–186. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, A.; Nicholls, S.J.; Redfern, J.; Brown, A.; Hare, D.L. Mental Health and Psychosocial Challenges in the COVID-19 Pandemic: Food for Thought for Cardiovascular Health Care Professionals. Hear. Lung Circ. 2020, 29, 960–963. [Google Scholar] [CrossRef] [PubMed]
- Mishra, P.; Bhadauria, U.S.; Dasar, P.L.; Kumar, S.; Lalani, A.; Sarkar, P.; Chauhan, A.; Godha, S.; Vyas, S. Knowledge, attitude and anxiety towards pandemic flu a potential bio weapon among health professionals in Indore City. Prz. Epidemiol. 2016, 70, 41–127. [Google Scholar]
- Dave, M.; Seoudi, N.; Coulthard, P. Urgent dental care for patients during the COVID-19 pandemic. Lancet 2020, 395, 1257. [Google Scholar] [CrossRef]
- Wu, K.; Wu, D.; Nguyen, T.; Tran, S. COVID-19’s impact on private practice and academic dentistry in North America. Oral Dis. 2020, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Kissoon, C. T&T Begins Closing down Again: Masks to Become Mandatory. Trinidad Express Newspapers. 2020. Available online: https://trinidadexpress.com/newsextra/t-t-begins-closing-down-again-masks-to-become-mandatory/article_73b9821a-df29-11ea-aaec-33aa3d8edd62.html (accessed on 7 August 2020).
- Spagnuolo, G.; De Vito, D.; Rengo, S.; Tatullo, M. COVID-19 Outbreak: An Overview on Dentistry. Int. J. Environ. Res. Public Health 2020, 17, 2094. [Google Scholar] [CrossRef] [PubMed]
- Sun, N.; Wei, L.; Shi, S.; Jiao, D.; Song, R.; Ma, L.; Wang, H.; Wang, C.; Wang, Z.; You, Y.; et al. A qualitative study on the psychological experience of caregivers of COVID-19 patients. Am. J. Infect. Control. 2020, 48, 592–598. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).