Abstract
(1) Background: The aim of this study was to compare the histopathological features of syndromic and non-syndromic odontogenic keratocysts (OKs) using conventional and Confocal Laser Scanning Microscopy (CLSM) with their biological behaviour. (2) Methods: Data from the medical records of 113 patients with histological diagnosis of (single and/or multiple) OKs were collected. Globally, 213 OKs (120 syndromic and 93 sporadic) were retrieved, and their histological slides were re-evaluated with conventional H&E staining and with autofluorescence on the same slides using CLSM (Nikon Eclipse E600 microscope). (3) Results: Syndromic OKs showed more satellite cysts than sporadic cases, as well as a basophilic layer in the basement membrane, which was absent in sporadic OKs; both were highlighted with CLSM. The basement membrane in syndromic OKs appeared amorphous and fragile, thus possibly being responsible for the epithelial detachment and collapse, with scalloped features. Furthermore, the basal epithelial layers in such cases also showed increased cellularity and proliferative activity. All these histological features may possibly justify their higher tendency to recur. (4) Conclusions: CLSM is useful advanced technology that could help to quickly and easily discriminate between syndromic and non-syndromic OKs and to more accurately predict their biological behaviour in order to set fitter clinico-radiological follow-ups for individual patients.
1. Introduction
The odontogenic keratocyst (OK) was first described in 1956 by Philpsen as an odontogenic cyst with keratinized epithelium [1], and later, because of its aggressive behaviour, high recurrence rates, and specific histological characteristics [2], it was re-classified as “a benign uni- or multi-cystic, intra-osseus tumour of odontogenic origin (Keratocystic odontogenic tumour-KCOT), with a characteristic lining of para-keratinized stratified squamous epithelium and potential for aggressive, infiltrative behaviour” by the World Health Organization (WHO) in 2005 [3]. In the 2017 classification of head and neck tumours, this pathological entity was reverted back from tumour to the original and well-accepted terminology of odontogenetic keratocyst [4], because despite the characteristics of aggressive growth, post-operative recurrence, the rare reports of solid variants of OKs, and mutations in the PTCH gene, there was not sufficient evidence to support the classification as a tumour [5].
In the newest 2022 edition of the WHO classification of head and neck tumours, the OK continues to be part of the cyst classification [6].
It may be solitary or multiple and occur synchronously or metachronously in one or both jaws, the latter being considered as one stigmata of the inherited Nevoid Basal-Cell Carcinoma Syndrome (NBCCS) [3]. NBCCS is a rare genetic condition with an autosomal-dominant inheritance pattern, showing variable expressiveness and complete penetrance, firstly defined in 1960 by Gorlin and Goltz as a condition including multiple basal-cell nevi, multiple OKs, and skeletal abnormalities [7].
OKs can occur in wide age range, with a peak in the third and fourth decades and a second smaller peak in the elderly with a slight male predilection [8] (the reported male–female ratio is 1.6:1 [2]). OKs are believed to arise from the dental lamina or its remnants, which include the pre-functional lamina, not involved in tooth formation [9], and occasionally, from the basal layers of the overlying mucosa [10].
Several studies have highlighted the role of the PTCH1 gene in the aetiology of both syndromic and sporadic OKs. The PTCH1 gene, mapped on chromosome 9q22.3-q31, encodes for a transmembrane receptor for Sonic Hedgehog (SHH). The PTCH–SHH pathway is involved in the pathogenesis of sporadic and syndromic tumours (associated with NBCCS), such as OKs, basal-cell carcinomas, medulloblastomas, and trichoepitheliomas [11].
OKs more frequently involve the angle of the mandible (the mandible–maxilla ratio is 2:1) [12]. These tumours may reach a large size prior to identification, and patients may complain of pain, swelling, or discharge in almost 60% of the cases [13]. Radiographically, an OK may appear as a small and round unilocular radiolucency or may be larger and multilocular with scalloped margins. In 25–40% of cases, OKs may be present in association with impacted or displaced teeth, whereas dental root erosion rarely occurs [14].
Typically, histologic findings of OKs show a para-keratinized stratified squamous epithelium, usually 5–8-cell-layer thick, which demarcates a cystic lumen filled with desquamated keratin [2]. There is a well-defined, often palisaded, basal layer of columnar or cuboidal cells, whereas the parakeratotic cells in the upper layers often show a corrugated surface. Satellite cysts may be seen in the surrounding fibrous connective tissues. Occasionally, epithelial dysplasia may be present, but the malignant transformation to squamous-cell carcinoma is exceedingly rare [4].
Another, less frequent histologic variant was described, i.e., the orthokeratinized odontogenic keratocyst [15]. In this case, histology is characterized by thin, uniform, orthokeratinized lining epithelium with an onion-skin-like luminal surface keratinization, prominent stratum granulosum, and low cuboidal or flattened basal-cell layer with little tendency of nuclear palisading [16].
When OKs show features such as small satellite cysts or solid islands in the cystic wall or budding of the basal layer, they are generally associated with NBCCS [4].
Patients with syndromic keratocysts may be at greater risk for developing more numerous and severe BCCs and other neoplastic growths, including ovarian fibromas [17].
The aim of this study was to report on novel histopathological findings, as detected with Confocal Laser Scanning Microscopy (CLSM), and to compare such findings with the biological behaviour of both syndromic and sporadic OKs in order to determine specific features that could facilitate the early diagnosis of NBCCS in those patients where the first manifestation is that of OKs.
2. Materials and Methods
This retrospective study was performed at Odontostomatology and Surgery Unit of University of Bari Aldo Moro.
The current study was carried out in accordance with the principles of the Declaration of Helsinki; in addition, it was approved by the institutional review board (study No. 4599, Prot. 1528/C.E.); patients released informed consent for diagnostic/therapeutic procedures and for the possible use of the biologic samples for research purposes.
In the period between 1979 and 2020, a total number of 126 patients were histologically diagnosed with 228 syndromic and sporadic OKs. All patients provided written informed consent before any study-related procedure was started.
All samples were fixed in 10% neutral-buffered formalin, paraffin-embedded, thin-sectioned at 3–4 μm, and stained with haematoxylin–eosin. All histological slides were re-evaluated using a Nikon Eclipse E600 microscope (Nikon Corporation, Tokio, Japan), equipped with argon and helium–neon lasers emitting at 488–543-nm wavelengths, which allowed us to perform both optical and Confocal Laser Scanning Microscope (CLSM) analyses. Nikon EZ C1 software (ver. 2.10; Nikon Corporation, Coord Automatizing) was used for bidimensional image processing. For each sample, ten 512 × 512 × 12-bit bidimensional images were acquired.
Following histological re-evaluation, 13 patients harbouring 15 OKs were excluded due to equivocal morphologic presentation, which did not allow us to definitely rule out cysts of other types. Overall, 213 OKs from 113 patients were included in this study. The collected data included gender, age at diagnosis, familiarity in syndromic patients, site, size, multiplicity, maxillary-sinus involvement, associated impacted teeth, treatment modalities, and recurrence rate. The chi-squared test (χ²) was used to detect associations between the several analysed variables using a 95% significance level (p < 0.05).
3. Results
The main clinic–radiological features of the investigated patients are summarized in Table 1. Overall, 31 patients were affected by NBCCS (group 1), while the remaining 82 patients presented sporadic (non-syndromic) lesions (group 2). In group 1, the age range was 3.5–53 years, whereas in group 2, it was 9–86 years. Interestingly, OKs were detected in a larger cohort of paediatric patients (18 years old or younger) (n = 11/31 = 35.48%) of group 1 in comparison with those of group 2 (n = 9/82 = 10.98%), this difference being statistically significant (χ² = 9.28; p = 0.0023).

Table 1.
Clinical data of the 113 patients included in this study.
The male–female ratio was almost 1.5:1 in both groups. Both sporadic and syndromic OKs preferentially involved the mandible rather than the maxilla (the mandible–maxilla ratio was 1.9:1 in syndromic OKs and 5.8:1 in sporadic lesions), and 20.19% of the lesions were associated with impacted teeth.
Within group 1, 74.19% of the patients presented multiple lesions (81 OKs = 3.52/patient), while no multiple lesions were identified among patients of group 2 (χ² = 76.39; p < 0.0001).
In addition, following conservative surgery, 12 syndromic patients experienced 26 recurrences (38.71%; n = 12/31), as opposed to 8 patients with sporadic OKs who presented 11 recurrences (9.76%; n = 8/82) (χ² = 12.95; p = 0.0003).
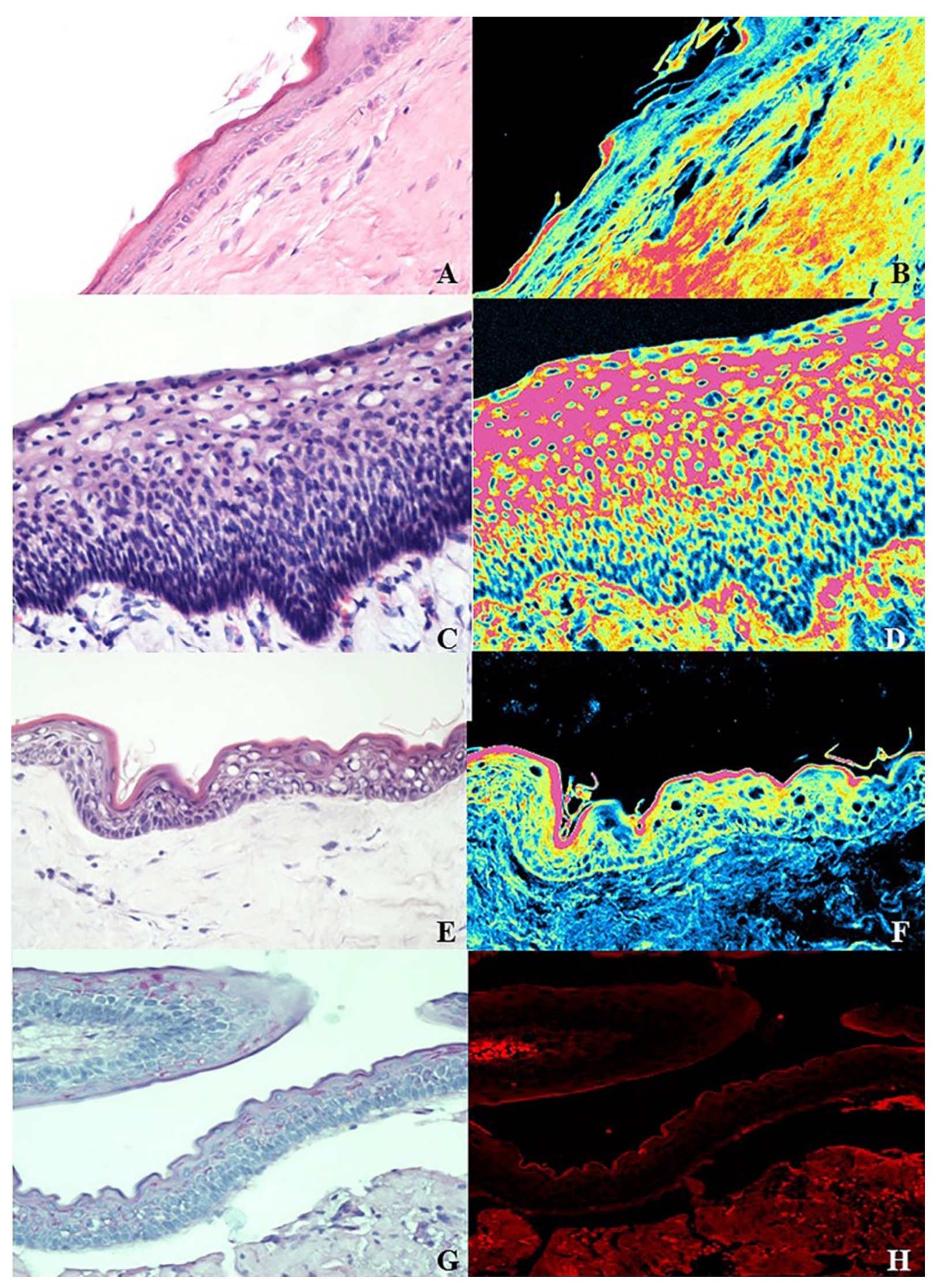
The histological findings are summarized in Table 2. Syndromic OKs analysed with CLSM presented more numerous satellite cysts, due to the budding of the basal-cell layers in the underlying connective tissue, than sporadic lesions (Figure 1A,B). Furthermore, the epithelial layers appeared more densely cellular and more intensely mitotically active in syndromic OKs, in comparison with sporadic cases. Interestingly, a subepithelial basophilic layer was clearly detectable in syndromic OKs (Figure 1C,D) and absent in non-syndromic OKs (Figure 1E,F). Moreover, the basement membrane in syndromic OKs resulted amorphous and fragile, this feature being possibly responsible for the detachment of the epithelial component, which appeared collapsed and ramified, with a scalloped and corrugated aspect (Figure 1G,H).
Table 2.
CLSM typical features of 120 syndromic and 93 sporadic OKs.
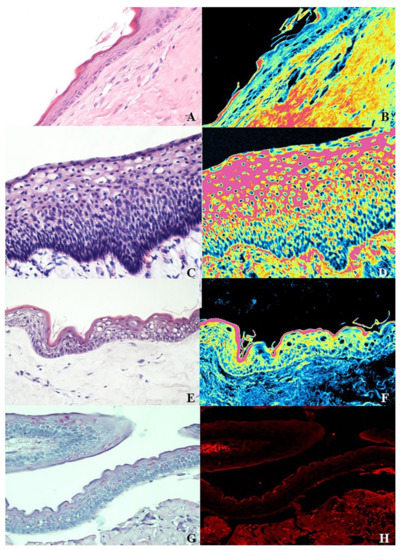
Figure 1.
(A,B) Morphologic appearance of the epithelium in sporadic KOTs with traditional microscopy (haematoxylin–eosin staining) and the same field in Confocal Laser Scanning Microscopy with a double laser inducing fluorescence (green and red) (original magnification of ×20). (C,D) Higher cellular density with subepithelial basophilic layers of syndromic KOTs in traditional microscopy (haematoxylin–eosin staining) and the same field in Confocal Laser Scanning Microscopy with a double laser inducing fluorescence (green and red) (original magnification of ×20). (E,F) Low cellular density without subepithelial basophilic layers of sporadic KOTs in traditional microscopy (haematoxylin–eosin staining) and the same field in Confocal Laser Scanning Microscopy with a double laser inducing fluorescence (green and red) (original magnification of ×20). (G,H) Epithelial detachment in syndromic KOTs due to the amorphous and fragile basement membrane in traditional microscopy (haematoxylin–eosin staining) and the same field in Confocal Laser Scanning Microscopy with a red laser inducing fluorescence (original magnification of ×20).
4. Discussion
Following its initial designation as a cyst of odontogenic origin, some authors postulated that OKs would have been more appropriately considered neoplasms, in view of their locally destructive and aggressive behaviour, high recurrence rates after simple enucleation, histological appearance, expression of tumour markers, and for the occurrence of the mutation of the PTCH1 gene [2,3,9,14]. Such tentative re-classification of OKs as neoplastic lesions (keratocystic odontogenic tumour) was included in the WHO classifications of 2005 of odontogenic tumours to highlight its virtually aggressive nature and to emphasize the need for more aggressive therapeutic interventions [18]. Nevertheless, no unanimous consensus was reached in this regard, and in the updated WHO classifications, OKs were re-included among the odontogenic cysts, with a note of caution as to its possible aggressive behaviour [4,5,6].
In close agreement with most reports in the literature, the mean age of NBCCS patients in the current series was lower than that of patients harbouring non-syndromic OKs; the male–female ratio was almost 1.5:1, thus confirming the slight male predominance generally reported by several investigators [2]. Most reports concur that OKs affect the mandible more frequently than the maxilla, with the mandibular posterior region being the most commonly affected site, as confirmed by our analyses, which also support the prevalence of mandibular OKs in sporadic lesions.
While we detected a relatively smaller percentage (20.19%) of OKs associated with impacted teeth than what reported in the literature [19], our data confirm that multiple OKs were mostly detected within NBCCS patients, who also experienced higher recurrence rates and larger sizes of the lesions. Quite interestingly, the recurrence rate of OKs in non-syndromic patients included in the current series was lower than the one reported in the literature, with analogous treatment modalities [19,20,21,22].
Biological differences between sporadic and syndromic keratocysts were studied performing an immunohistochemical evaluation of the Sonic-Hedgehog-signalling-pathway protein expression (Shh, Ptch1, Ptch2, Smo, Gli1, Gli2, and Gli3), and it emerged that in the syndromic OKs, there was an increase in the expression of Shh, Smo, and Gli1 proteins when compared to that of sporadic cysts [23].
Some novel findings of this study resulted from the CLSM examination of the histological samples using autofluorescence. CLSM was demonstrated to be a major advance in biological imaging and in many fields of dental medicine [24,25], as well as in general medicine [25,26]. It may be considered an intermediate step between optical and electronic microscopy and uses a bi-chromatic punctiform laser source, the resulting emission energy being detected by a spatially filtered optical system, the pinhole, which eliminates light signals arising from out-of-focus planes [24]. Samples do not need any specific staining procedure, as conventional H&E-stained sections provide excellent results. Overall, CLSM produces intensely stained and high-resolution images, with clearly visible borders, without noise or otherwise disturbing signals from the surrounding tissues.
In the current study, CLSM allowed us to perform more accurate analyses of the morphological and cellular features of the lesions, in particular, the detection of amorphous and fragile basement membranes, detached and collapsed epithelial layers, and higher cellular density in the basal epithelial layers with increased proliferative activity in syndromic OKs as compared with sporadic lesions. Such features may at least in part justify the higher tendency of syndromic OKs to recur, in view of the lower mechanical resistance of the peripheral layers of the cysts towards the expansion of the proliferating epithelial compartment.
Our study has limitations, such as the lack of discrimination between orthokeratinized and parakeratinized keratocysts and the absence of a correlation with an immunohistochemical analysis.
In addition, considering CLSM as a quick and easily manageable technique in oral pathology, it may be adopted as a supplementary tool, along with immunohistochemistry and molecular biology, to tell apart syndromic from sporadic OKs, especially in cases in which the surgical samples may result insufficient for extensive morphologic evaluation [27,28].
Author Contributions
Conceptualization, G.F. and L.L.; methodology, G.F. and E.M.; software, E.M.; validation, F.S. and A.T.; formal analysis, S.C.; investigation, E.M.; resources, A.T.; data curation, L.L.; writing—original draft preparation, G.F.; writing—review and editing, F.S. and L.L.M.; visualization, E.L.M.; supervision, L.L.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research study received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the institutional review board (study No. 4599, Prot. 1528/C.E).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
This work was supported by Consorzio Interuniversitario Nazionale per la Bio-Oncologia (CINBO), Italy.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Philipsen, H.P. Om keratocystedr (Kolesteratomer) and kaeberne. Tandlaegebladet 1956, 60, 963–971. [Google Scholar]
- Bhargava, D.; Deshpande, A.; Pogrel, M.A. Keratocystic odontogenic tumour (KCOT)-a cyst to a tumour. Oral Maxillofac. Surg. 2012, 16, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Barnes, L.; Eveson, J.W.; Reichart, P.; Sidransky, D. Pathology and Genetics of Head and Neck Tumours; IARC Press: Lyon, France, 2005. [Google Scholar]
- Speight, P.; Devilliers, P.; Li, T.-J.; Odell, E.W.; Wright, J.M. Odontogenic keratocyst. In WHO Classification of Head and Neck Tumours, 4th ed.; El-Naggar, A.K., Chan, J.K.C., Grandis, J.R., Takata, T., Slootweg, P., Eds.; IARC Press: Lyon, France, 2017. [Google Scholar]
- Bhargava, D. Odontogenic keratocyst (OKC)-reverting back from tumour to cyst: Keratocystic odontogenic tumour (KCOT)-a cyst to a tumour. Oral Maxillofac. Surg. 2012, 16, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Vered, M.; Wright, J.M. Update from the 5th Edition of the World Health Organization Classification of Head and Neck Tumors: Odontogenic and Maxillofacial Bone Tumours. Head Neck Pathol. 2022, 16, 63–75. [Google Scholar] [CrossRef]
- Gorlin, R.J.; Goltz, R.W. Multiple nevoid basal-cell epithelioma, jaw cysts and bifid rib. A syndrome. N. Engl. J. Med. 1960, 262, 908–912. [Google Scholar] [CrossRef]
- Soluk-Tekkesin, M.; Wright, J.M. The World Health Organization Classification of Odontogenic Lesions: A Summary of the Changes of the 2022 (5th) Edition. Turk. Patoloji. Derg. 2022, 38, 168–184. [Google Scholar] [CrossRef]
- Pogrel, M.A. The keratocystic odontogenic tumor. Oral Maxillofac. Surg. Clin. N. Am. 2013, 25, 21–30. [Google Scholar] [CrossRef]
- Stoelinga, P.J. Etiology and pathogenesis of keratocysts. Oral Maxillofac. Surg. Clin. N. Am. 2003, 15, 317–324. [Google Scholar] [CrossRef]
- Gorlin, R.J. Nevoid basal cell carcinoma syndrome. Dermatol. Clin. 1995, 13, 113–125. [Google Scholar] [CrossRef]
- Eryilmaz, T.; Ozmen, S.; Findikcioglu, K.; Kandal, S.; Aral, M. Odontogenic keratocyst: An unusual location and review of the literature. Ann. Plast. Surg. 2009, 62, 210–212. [Google Scholar] [CrossRef]
- Stoelinga, P.J. Long-term follow-up on keratocysts treated according to a defined protocol. Int. J. Oral Maxillofac. Surg. 2001, 30, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, W.A. Surgical treatment of keratocystic odontogenic tumour: A review article. Saudi Dent. J. 2011, 23, 61–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravi, J.; Wadhwan, V.; Gotur, S.P. Orthokeratinized versus parakeratinized odontogenic keratocyst: Our institutional experience. J. Oral. Maxillofac. Pathol. 2022, 26, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Selvamani, M.; Devi, A.Y.; Basandi, P.S.; Madhushankari, G.S. Prevalence and clinicopathological comparison of kerotocystic odontogenic tumor and orthokeratinized odontogenic cyst in South Indian sample population: A retrospective study over 13 years. J. Pharm. Bioallied. Sci. 2014, 6, S127–S130. [Google Scholar] [CrossRef]
- Betancourt, N.J.; Qian, M.F.; Pickford, J.R.; Bailey-Healy, I.; Tang, J.Y.; Teng, J.M.C. Gorlin Syndrome: Assessing Genotype-Phenotype Correlations and Analysis of Early Clinical Characteristics as Risk Factors for Disease Severity. J. Clin. Oncol. 2022, 40, 2119–2127. [Google Scholar] [CrossRef]
- Madras, J.; Lapointe, H. Keratocystic odontogenic tumour: Reclassification of the odontogenic keratocyst from cyst to tumour. J. Can. Dent. Assoc. 2008, 74, 165. [Google Scholar]
- Chirapathomsakul, D.; Sastravaha, P.; Jansisyanont, P. A review of odontogenic keratocysts and the behavior of recurrences. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, 5–9. [Google Scholar] [CrossRef]
- Bataineh, A.B.; al Qudah, M. Treatment of mandibular odontogenic keratocysts. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 86, 42–47. [Google Scholar] [CrossRef]
- Driemel, O.; Rieder, J.; Morsczeck, C.; Schwarz, S.; Hakim, S.G.; Muller-Richter, U.; Reichert, T.E.; Kosmehl, H. Comparison of clinical immunohistochemical findings in keratocystic odontogenic tumours and ameloblastomas considering their risk of recurrence. Mund-Kiefer-Gesichtschirurgie MKG 2007, 11, 221–231. [Google Scholar] [CrossRef]
- Habibi, A.; Saghravanian, N.; Habibi, M.; Mellati, E.; Habibi, M. Keratocystic odontogenic tumor: A 10-year retrospective study of 83 cases in an Iranian population. J. Oral Sci. 2007, 49, 229–235. [Google Scholar] [CrossRef] [Green Version]
- Hoyos Cadavid, A.M.; Kaminagakura, E.; Rodrigues, M.; Pinto, C.A.L.; Teshima, T.H.N.; Alves, F.A. Immunohistochemical evaluation of Sonic Hedgehog signaling pathway proteins (Shh, Ptch1, Ptch2, Smo, Gli1, Gli2, and Gli3) in sporadic and syndromic odontogenic keratocysts. Clin. Oral. Investig. 2019, 23, 153–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zucker, R.M.; Price, O. Evaluation of confocal microscopy system performance. Cytometry 2001, 44, 273–294. [Google Scholar] [CrossRef]
- Watson, T.F. Applications of confocal scanning optical microscopy to dentistry. Br. Dent. J. 1991, 171, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Zucker, R.M.; Price, O.T. Practical confocal microscopy and the evaluation of system performance. Methods 1999, 18, 447–458. [Google Scholar] [CrossRef] [PubMed]
- Cserni, D.; Zombori, T.; Stajer, A.; Rimovszki, A.; Cserni, G.; Barath, Z. Immunohistochemical Characterization of Reactive Epithelial Changes in Odontogenic Keratocysts. Pathol. Oncol. Res. 2020, 26, 1717–1724. [Google Scholar] [CrossRef] [Green Version]
- Vered, M.; Peleg, O.; Taicher, S.; Buchner, A. The immunoprofile of odontogenic keratocyst (keratocystic odontogenic tumor) that includes expression of PTCH, SMO, GLI-1 and bcl-2 is similar to ameloblastoma but different from odontogenic cysts. J. Oral Pathol. Med. 2009, 38, 597–604. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).