


Recent Case Reveals a Nineteenth Century Trauma Analysis and Presentation of a Skull as Evidence in a Homicide Trial


Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Case Report
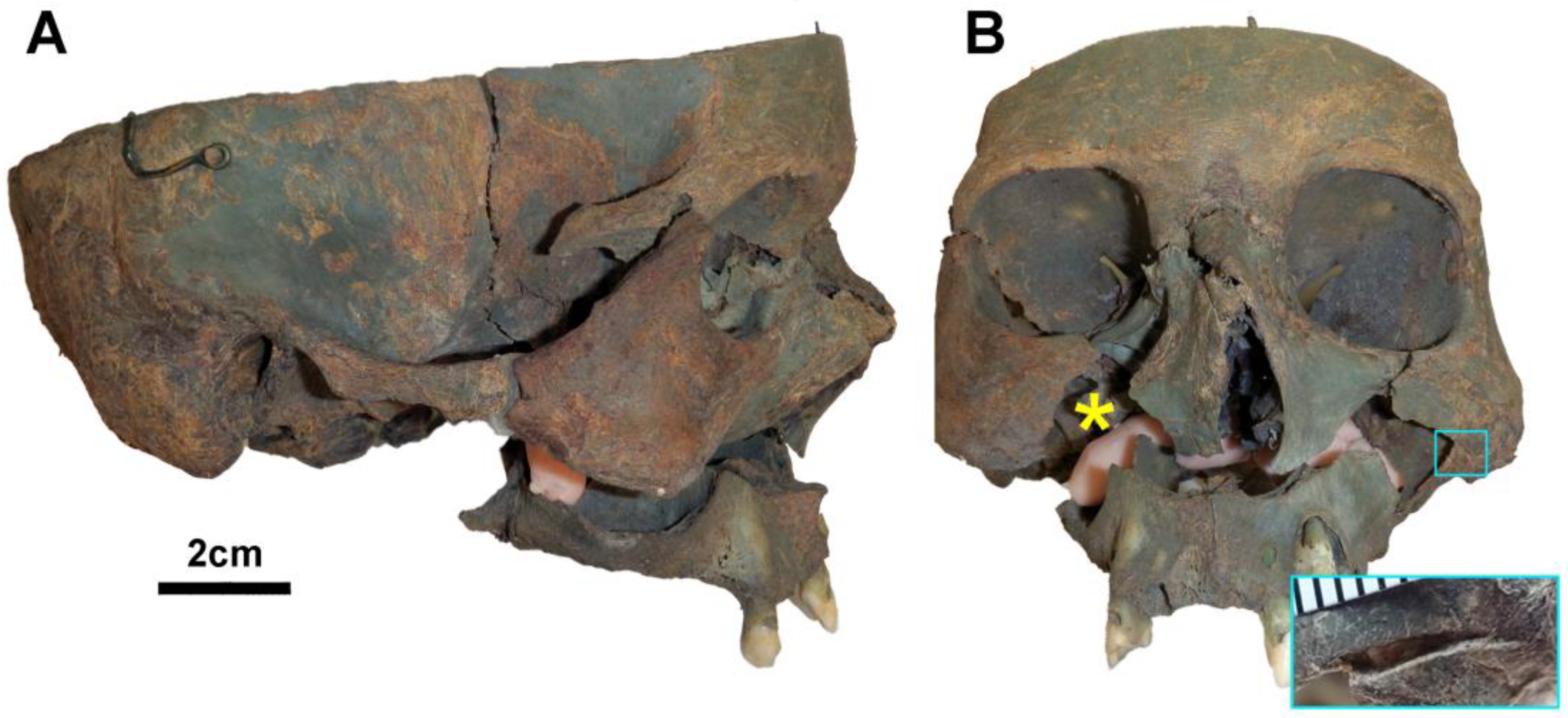
2.1. Forensic Anthropological Assessment
2.1.1. Associated Material Artifacts
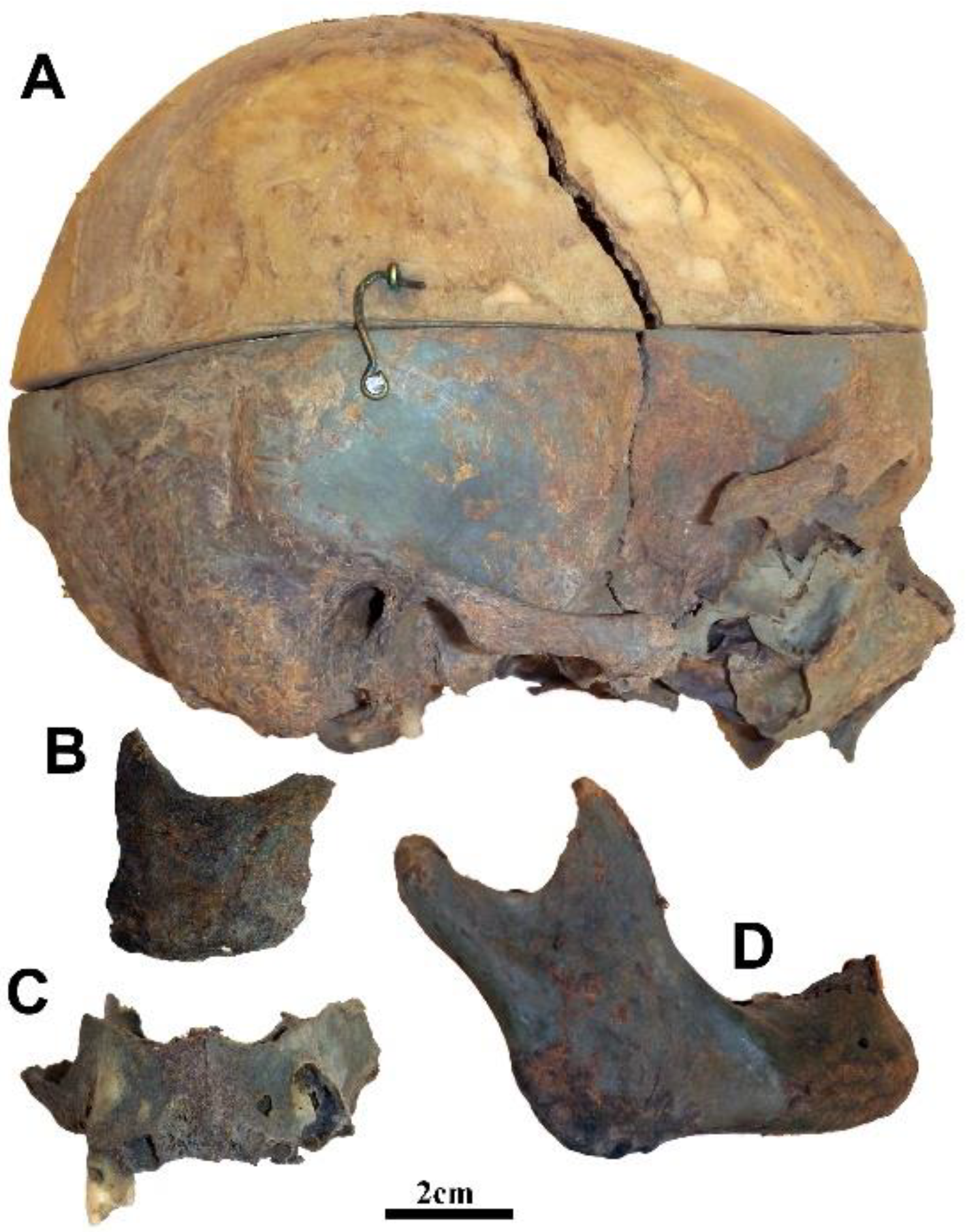
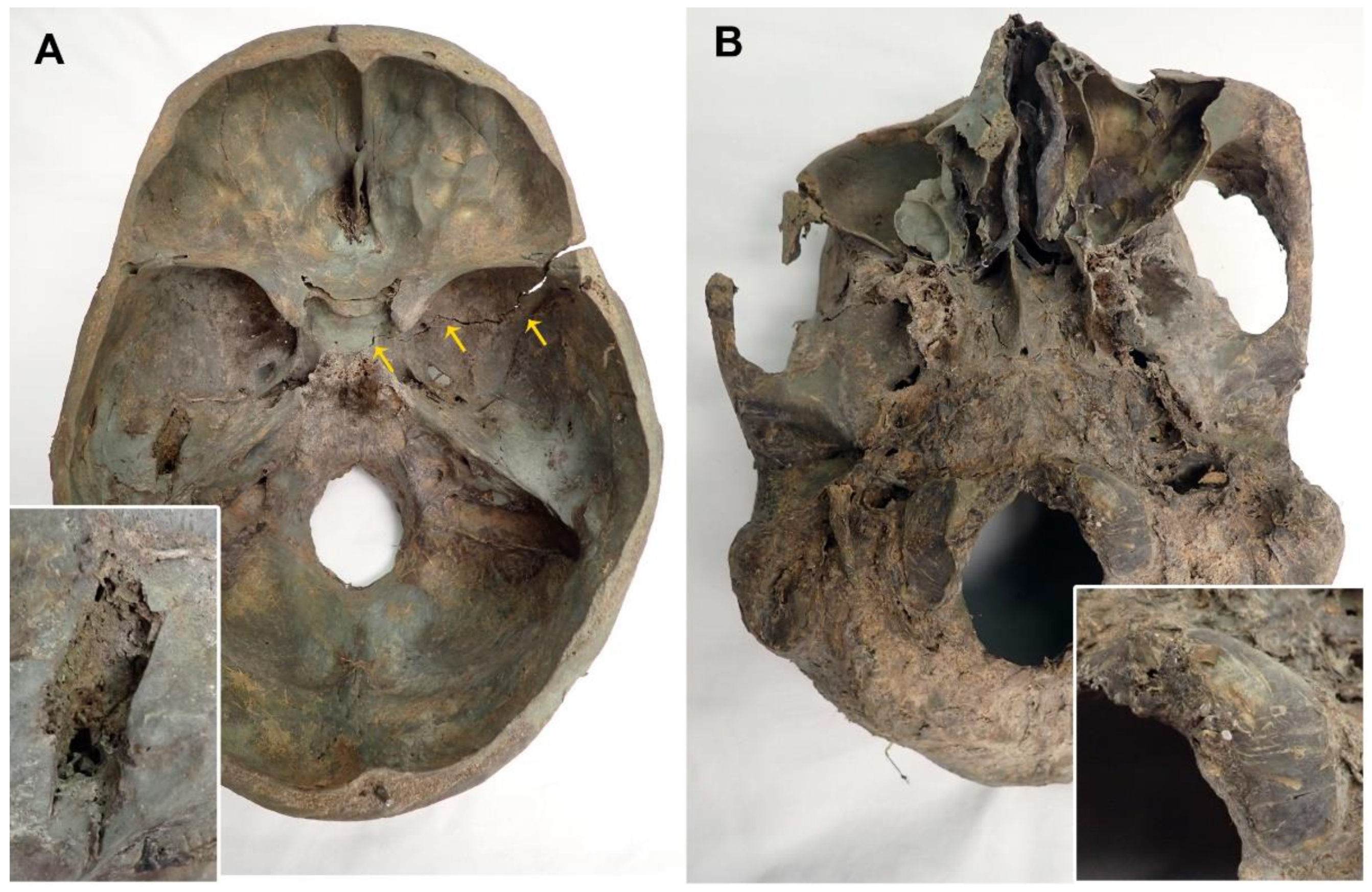
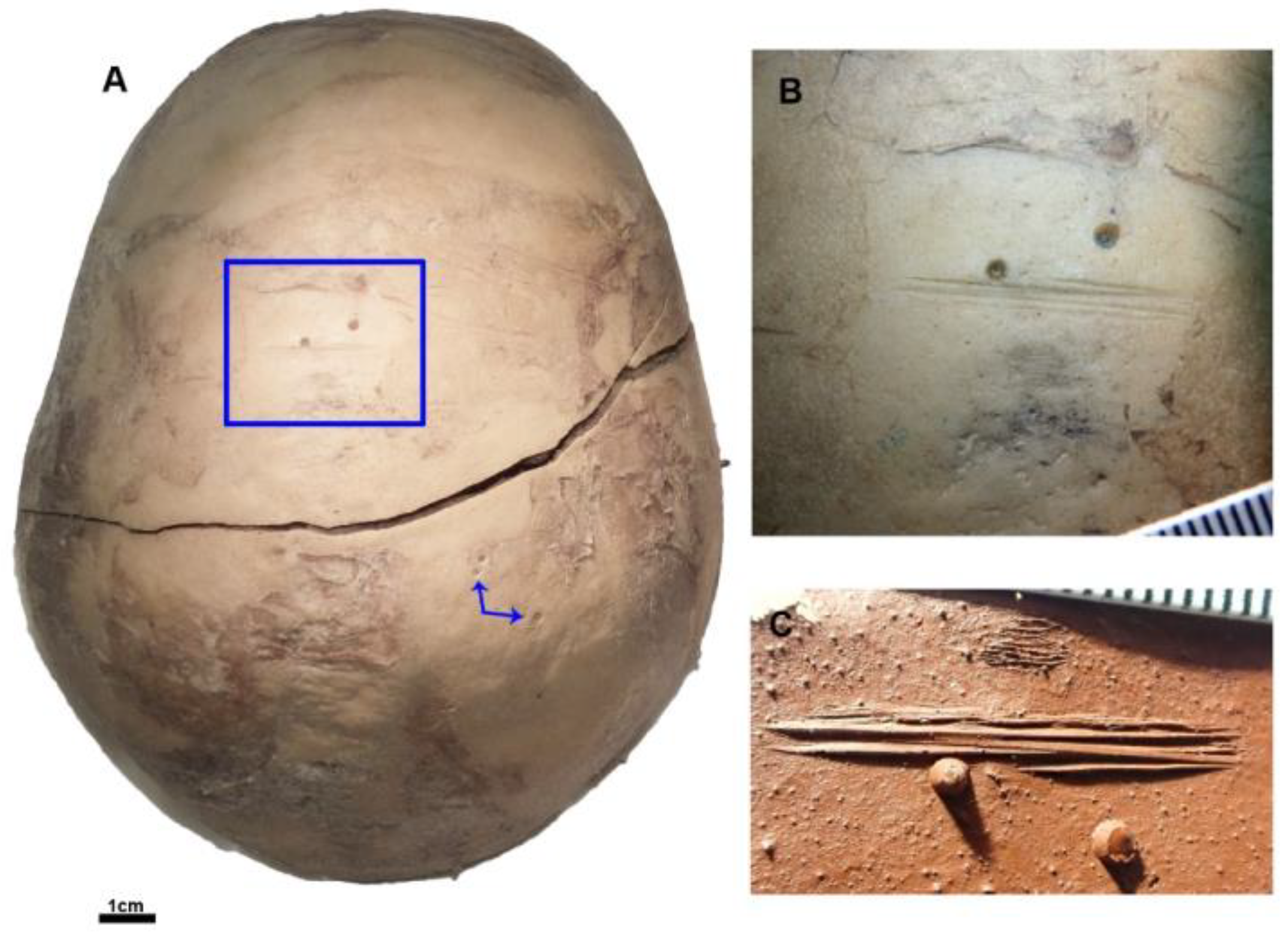
2.1.2. Taphonomic Modifications
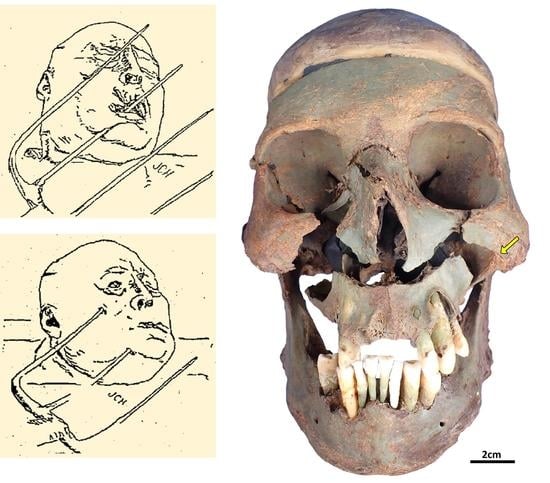
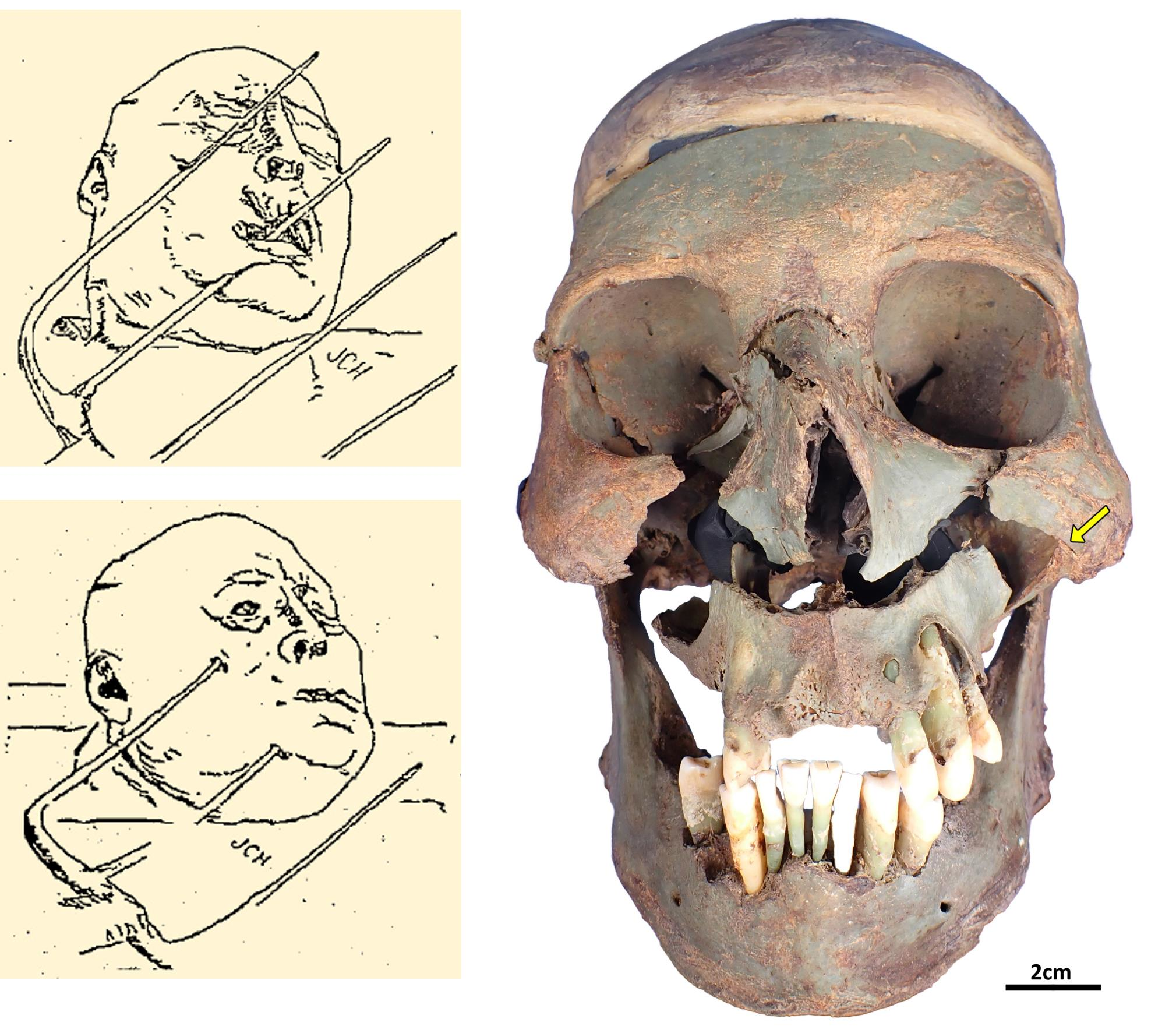
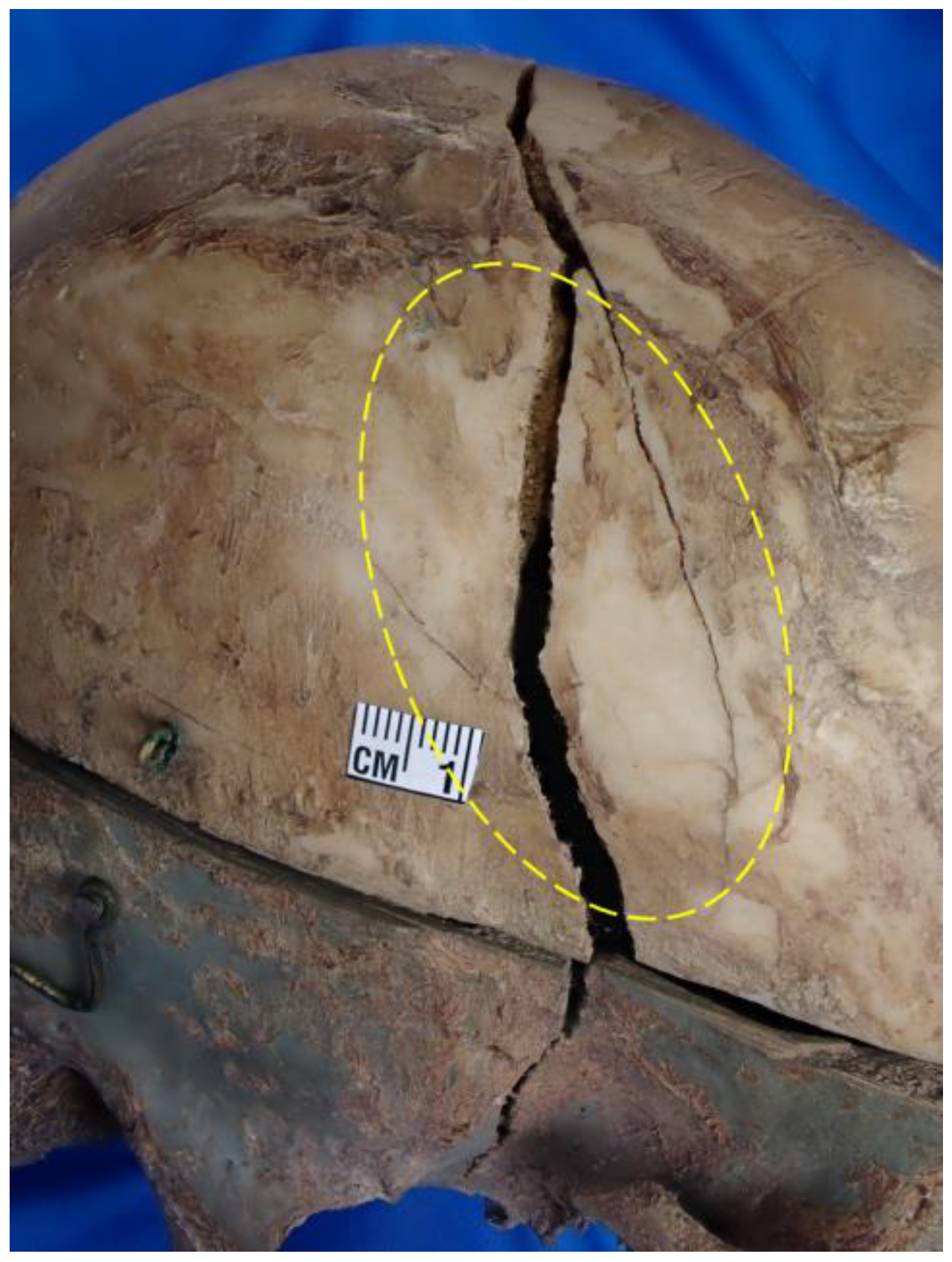
2.1.3. Trauma
2.1.4. Biological Profile
2.1.5. Conclusions
2.2. Historical Investigation
2.2.1. G.B. Ward
2.2.2. State of Iowa v. Charles Adams (1895)—Black Hawk County
3. Discussion
3.1. Identification
3.2. Historical Precedence
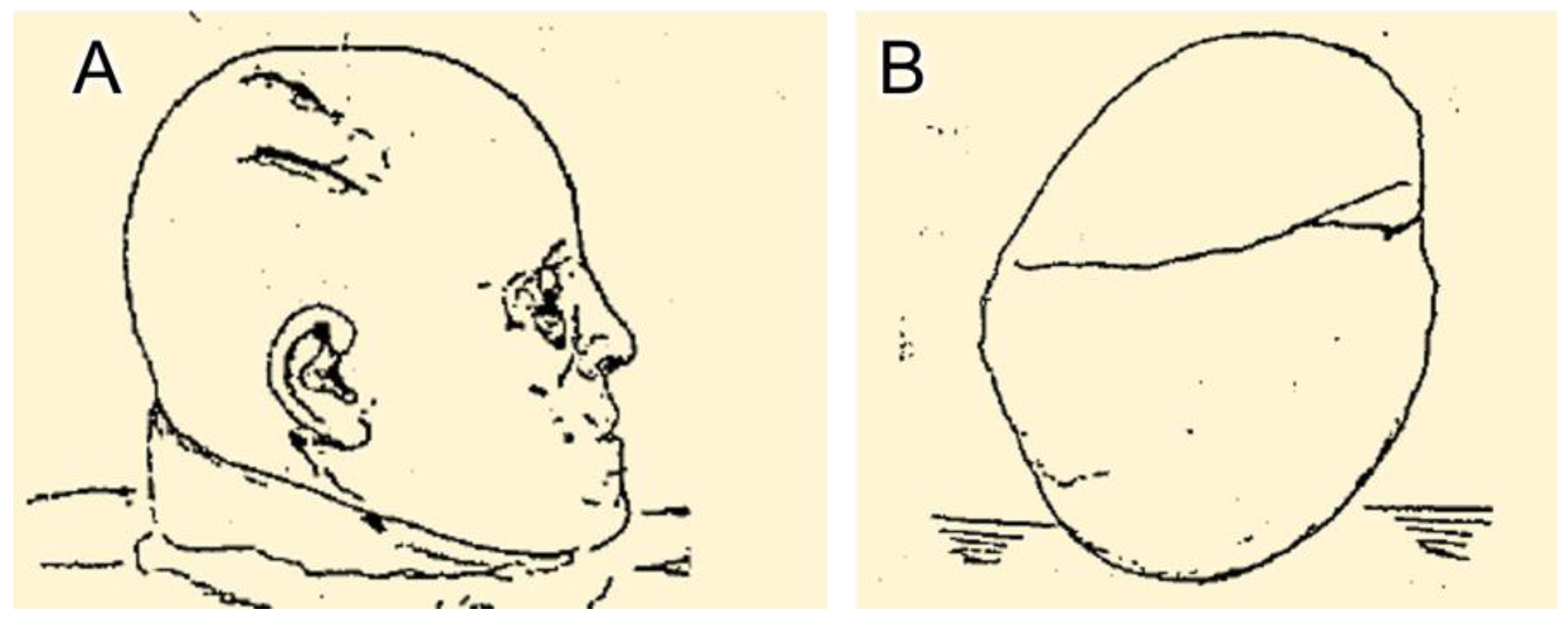
3.3. Mechanism of Trauma
4. Impact Statement
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ubelaker, D.H. A history of forensic anthropology. Am. J. Phys. Anthropol. 2018, 165, 915–923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Symes, S.A. Morphology of Saw Marks in Human Bone: Identification of Class Characteristics. Ph.D. Dissertation, University of Tennessee, Knoxville, Tennessee, 1992. [Google Scholar]
- Symes, S.A.; Chapman, M.S.; Rainwater, C.W.; Cabo, L.L.; Muster, S.M.T. Knife and Saw Tool-Mark Analysis on Bone: A Manual Designed for the Examination of Criminal Mutilation and Dismemberment; National Institute of Justice Report: Washington, DC, USA, 2010. [Google Scholar]
- Paolello, J.M.; Klales, A.R. Contemporary cultural alterations to bone. In Manual of Forensic Taphonomy; Pokines, J., Symes, S.A., Eds.; CRC Press: Boca Raton, FL, USA, 2013; pp. 181–199. [Google Scholar]
- Tank, P.W. Grants Dissector, 13th ed.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2005; pp. 208–209. [Google Scholar]
- Keleman, G. Removal of the petrous bone from the cranial base for macro- and microscopic investigation: Historical and technical considerations. Ann. Otol. Rhinol. 1952, 61, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Pokines, J.T. Taphonomic characteristics of former anatomical teaching specimens received at a Medical Examiner’s Office. J. Forensic. Identif. 2015, 65, 173–195. [Google Scholar]
- Pokines, J.T.; Appel, N.; Pollock, C.; Eck, C.J.; Maki, A.G.; Joseph, A.S.; Cadwell, L.; Young, C.D. Anatomical Taphonomy at the source: Alterations to a sample of 84 teaching skulls at a medical school. J. Forensic. Identif. 2017, 67, 600–632. [Google Scholar]
- Galloway, A.; Zephro, L.; Wedel, V.L. Diagnostic criteria for the determination of timing and fracture mechanism. In Broken Bones: Anthropological Analysis of Blunt Force Trauma, 2nd ed.; Wedel, V.L., Galloway, A., Charles, C., Eds.; Thomas: Springfield, IL, USA, 2014; pp. 47–58. [Google Scholar]
- Meindl, R.S.; Lovejoy, C.O. Ectocranial suture closure: A revised method for the determination of skeletal age at death based on the latera-anterior sutures. Am. J. Phys. Anthropol. 1985, 68, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Shirley, J.; Jantz, R.B. Spheno-occipital synchondrosis fusion in modern Americans. J. Forensic. Sci. 2011, 56, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Walker, P.L. Sexing skulls using discriminant function analysis of visually assessed traits. Am. J. Phys. Anthropol. 2008, 136, 36–50. [Google Scholar] [CrossRef] [PubMed]
- Hefner, J.T. Cranial nonmetric variation and estimating ancestry. J. Forensic. Sci. 2009, 54, 985–995. [Google Scholar] [CrossRef] [PubMed]
- Coelho, J.; Navega, D. hefneR. Available online: https://osteomics.com/hefneR/ (accessed on 3 December 2020).
- Thompson, L. Ward Family Has Served Medical Needs of Fairbank for 100 Years. Waterloo Sunday Courier. 29 September 1946, p. 14. Available online: https://waterloo.newspaperarchive.com (accessed on 3 March 2020).
- Was He Quarrelsome? Waterloo Daily Courier. 25 March 1895, p. 5. Available online: https://waterloo.newspaperarchive.com/crime-clipping-mar-25-1895-1579768/ (accessed on 4 March 2020).
- The Way It Was Done. Waterloo Daily Courier. 6 December 1894, p. 3. Available online: https://waterloo.newspaperarchive.com/crime-clipping-dec-06-1894-1579646/ (accessed on 4 March 2020).
- The Howard Murder. Waterloo Daily Courier. 16 November 1894, p. 3. Available online: https://newspaperarchive.com/waterloo-daily-courier-nov-16-1894-p-3/ (accessed on 4 March 2020).
- Charged with Murder. Waterloo Daily Courier. 16 January 1895, p. 4. Available online: https://newspaperarchive.com/waterloo-daily-courier-jan-16-1895-p-4/ (accessed on 4 March 2020).
- Afraid of Lynchers. Waterloo Daily Courier. 15 November 1894, p. 3. Available online: https://waterloo.newspaperarchive.com/crime-clipping-nov-15-1894-1579623/ (accessed on 4 March 2020).
- The Jury Empanelled. Waterloo Daily Courier. 13 March 1895, p. 5. Available online: https://newspaperarchive.com/waterloo-daily-courier-mar-13-1895-p-5/ (accessed on 4 March 2020).
- Adams Tells His Story. Waterloo Daily Courier. 27 March 1895, p. 5. Available online: https://newspaperarchive.com/waterloo-daily-courier-mar-27-1895-p-5/ (accessed on 4 March 2020).
- He Made Them Laugh. Waterloo Daily Courier. 15 March 1895, p. 5. Available online: https://waterloo.newspaperarchive.com/crime-clipping-mar-15-1895-1579733/ (accessed on 4 March 2020).
- Experts are Ruled Out. Waterloo Daily Courier. 28 March 1895, p. 5. Available online: https://newspaperarchive.com/waterloo-daily-courier-mar-28-1895-p-5/ (accessed on 4 March 2020).
- A Struggle of Giants. Waterloo Daily Courier. 19 March 1895, p. 5. Available online: https://newspaperarchive.com/waterloo-daily-courier-mar-29-1895-p-5/ (accessed on 4 March 2020).
- Goes to Jury Monday. Waterloo Daily Courier. 30 March 1895, p. 5. Available online: https://newspaperarchive.com/waterloo-daily-courier-mar-30-1895-p-5/ (accessed on 4 March 2020).
- The Pitchfork Theory. Waterloo Daily Courier. 16 March 1895, p. 5. Available online: https://newspaperarchive.com/waterloo-daily-courier-mar-16-1895-p-5/ (accessed on 4 March 2020).
- Most Ghastly Evidence. Waterloo Daily Courier. 18 March 1895, p. 5. Available online: https://newspaperarchive.com/waterloo-daily-courier-mar-18-1895-p-5/ (accessed on 4 March 2020).
- Says Del Swore False. Waterloo Daily Courier. 8 December 1894, p. 5. Available online: https://waterloo.newspaperarchive.com/crime-clipping-dec-08-1894-1579655/ (accessed on 4 March 2020).
- Will Be Tried. Waterloo Daily Courier. 4 February 1895, p. 5. Available online: https://newspaperarchive.com/waterloo-daily-courier-feb-04-1895-p-5/ (accessed on 4 March 2020).
- State Rests Its Case. Waterloo Daily Courier. 20 March 1895, p. 5. Available online: https://newspaperarchive.com/waterloo-daily-courier-mar-20-1895-p-5/ (accessed on 4 March 2020).
- Might Have Been a Club. Waterloo Daily Courier. 19 March 1895, p. 5. Available online: https://waterloo.newspaperarchive.com/crime-clipping-mar-19-1895-1579751/ (accessed on 4 March 2020).
- Doctor Versus Doctor. Waterloo Daily Courier. 21 March 1895, p. 5. Available online: https://newspaperarchive.com/waterloo-daily-courier-mar-21-1895-p-5/ (accessed on 4 March 2020).
- What Will the Jury Do? Waterloo Daily Courier. 1 April 1895, p. 5. Available online: https://newspaperarchive.com/waterloo-daily-courier-apr-01-1895-p-5/ (accessed on 4 March 2020).
- It Was Manslaughter. Waterloo Daily Courier. 2 April 1895, p. 5. Available online: https://newspaperarchive.com/waterloo-daily-courier-apr-02-1895-p-5/ (accessed on 4 March 2020).
- Applied for Pardon. Waterloo Daily Courier. 3 August 1895, p. 5. Available online: https://waterloo.newspaperarchive.com/crime-clipping-aug-03-1895-1579811/ (accessed on 4 March 2020).
- Wants to Come Back. Waterloo Daily Courier. 28 September 1897, p. 4. Available online: https://waterloo.newspaperarchive.com/crime-clipping-sep-28-1897-1579834/ (accessed on 4 March 2020).
- Kling, D.; Phillips, C.; Kennett, D.; Tillmar, A. Investigative genetic geneology: Current methods, knowledge and practice. Forensic. Sci. Int. 2021, 52, 102474. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, C. The emerging discipline of forensic genetic genealogy. In Forensic Genetic Approaches for Identification of Human Skeletal Remains: Challenges, Best Practices, and Emerging Technologies, 1st ed.; Ambers, A., Ed.; Academic Press: Cambridge, MA, USA, 2022; pp. 459–488. [Google Scholar]
- Widdows, H. Lizzie Andrew Borden Virtual Museum and Library Primary Source Documents, Trial Transcript Vol. 1. 2001. Available online: https://lizzieandrewborden.com/primary-source-documents-borden-case.htm (accessed on 25 January 2023).
- Brenner, E. Human body preservation—Old and new techniques. J. Anat. 2014, 224, 316–344. [Google Scholar] [CrossRef] [PubMed]
- Crowder, C.M.; Wiersema, J.M.; Adams, B.J.; Austin, D.E.; Love, J.C. The utility of forensic anthropology in the Medical Examiner’s Office. Acad. Forensic Pathol. 2016, 6, 349–360. [Google Scholar] [CrossRef] [PubMed]
- Phillips, B.J.; Turco, L.M. Le Fort fractures: A collective review. Bull. Emerg. Trauma 2017, 5, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Galloway, A.; Wedel, V.L. Bones of the skull, the dentition, and osseous structures of the throat. In Broken Bones: Anthropological Analysis of Blunt Force Trauma, 2nd ed.; Wedel, V.L., Galloway, A., Charles, C., Eds.; Thomas: Springfield, IL, USA, 2014; pp. 133–160. [Google Scholar]
- Rose, F.C. The history of head injuries: An overview. J. His. Neurosci. 1997, 6, 154–180. [Google Scholar] [CrossRef] [PubMed]
- Payne, W.N.; De Jesus, O.; Payne, A.N. Countrecoup Brain Injury; StatPearls Publishing, LLC.: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK536965/#_NBK536965_pubdet_ (accessed on 28 February 2023).
- Allen, F.J. The mechanism of contre-coup and of certain other forms of intracranial injury. Br. Med. J. 1896, 1, 1196–1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DiMaio, V.J.; DiMaio, D. Forensic Pathology: Practical Aspects of Criminal and Forensic Investigations, 2nd ed.; CRC Press: Boca Raton, FL, USA, 2001; pp. 104–106. [Google Scholar]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garvin, H.; Hohulin, L.; VanBaarle, A.; Wilson, A. Recent Case Reveals a Nineteenth Century Trauma Analysis and Presentation of a Skull as Evidence in a Homicide Trial. Forensic Sci. 2023, 3, 245-257. https://doi.org/10.3390/forensicsci3020018
Garvin H, Hohulin L, VanBaarle A, Wilson A. Recent Case Reveals a Nineteenth Century Trauma Analysis and Presentation of a Skull as Evidence in a Homicide Trial. Forensic Sciences. 2023; 3(2):245-257. https://doi.org/10.3390/forensicsci3020018
Chicago/Turabian StyleGarvin, Heather, Lindsey Hohulin, Alexis VanBaarle, and Andrew Wilson. 2023. "Recent Case Reveals a Nineteenth Century Trauma Analysis and Presentation of a Skull as Evidence in a Homicide Trial" Forensic Sciences 3, no. 2: 245-257. https://doi.org/10.3390/forensicsci3020018
APA StyleGarvin, H., Hohulin, L., VanBaarle, A., & Wilson, A. (2023). Recent Case Reveals a Nineteenth Century Trauma Analysis and Presentation of a Skull as Evidence in a Homicide Trial. Forensic Sciences, 3(2), 245-257. https://doi.org/10.3390/forensicsci3020018