Abstract
Defense wounds generally occur when a victim attempts to protect vital organs and blood vessels during an assault, and are therefore typically located on the forearms or hands. Gunshot-induced defense wounds are less frequent compared to stab wounds, which have been extensively described in the literature. We present three cases where victims unsuccessfully attempted to defend themselves from gunshots, and where the detailed description of injuries played a key role in the reconstruction of the crime scenes. In the first case, a man was shot with a smooth-bore shotgun, presenting a “through-and-through” gunshot wound on the lateral surface of the left forearm and a large gaping wound on the posterior surface of the same forearm. The second and third cases involved two men who were shot with handguns. The first displayed an entrance wound on the dorsal surface of the right hand, with burned edges and smoke soiling, and an exit wound on the palmar surface. The second case involved two wounds on the left hand: one on the dorsum and the other on the palm. To the best of our knowledge, few studies in the literature emphasize the role of gunshot defense wounds in aiding the reconstruction of crime dynamics. The cases presented in this study highlight the importance of precisely defining the pathological and morphological features of the wounds, as well as the bullet trajectories, to accurately identify defense wounds. These findings are valuable for reconstructing the dynamics of the assault and providing critical information to the public prosecutor.
1. Introduction
Defense wounds are injuries that occur when victims try to protect themselves during an attack, typically noted in cases where the assault happened at close range. As such, they can be crucial in reconstructing a crime [1]. The natural response of a victim to any type of assault is to raise their upper limbs to protect vital organs and vessels in the head, neck, and chest. Consequently, forearms, hands, elbows, and legs are instinctively raised, making these body parts more likely to sustain injuries, such as abrasions, contusions, lacerations, or incised wounds [1,2]. There is a higher frequency of defense injuries in women, as they may be more prone to being involved in prolonged domestic disputes, where self-defense becomes necessary [3,4].
Classic defense injuries are often associated with knife attacks, as the victim typically attempts to fend off the thrusts by grabbing the weapon [5]. When the victim grasps the sharp weapon or tries to deflect the attack, injuries occur on the flexor or palmar surfaces of the hand, or between the fingers; these are referred to as “active” defense wounds. Another common “active” defense wound is found in the webbing between the thumb and index finger. In contrast, when the victim places the dorsal or extensor surface of the forearm or hand between the weapon and their body in an attempt to protect themselves, these wounds are classified as “passive” [1,6,7].
Traditionally, defense wounds are described as injuries on the back and ulnar aspect of the forearms. However, a recent study has shown a predominance of injuries on the anterior surface of the upper limbs over the posterior surface [4]. Rarely, defense wounds can also be found on the feet or legs, which may occur when the individual attempts to kick away the weapon or curls up to protect vital areas with their legs [8].
Defense wounds hold significant medico-legal value, as they can assist in reconstructing a crime scene [9]. Generally, stab or sharp force defense wounds suggest that the victim was conscious, at least partially mobile, and in some cases, not taken by surprise. Therefore, the absence of defense wounds may be indicative of a single, unexpected fatal blow [5,7,10]. Moreover, the presence or absence of defense wounds can depend on several factors, including the duration of the attack (for instance, in a pre-existing conflict) and whether the victim was able to move their hands effectively [11].
The examination of defense wounds can provide insight into the relative positions of the assailant and victim, aiding the prosecutor in evaluating the perpetrator’s statements. It has been suggested that defense wounds predominantly occur on the left forearm and hand, as during a frontal attack by a right-handed assailant, the left arm is closer to the assailant and can react more quickly to grasp or deflect the attack [4,7,10]. However, the literature does not consistently support this predominance, with some studies indicating an equal distribution of defense wounds between the right and left limbs [7,12,13].
In forensic pathology, defense stab wounds are well classified and described. In contrast, gunshot-related defense wounds are less well-documented. This case series presents three deaths caused by gunshot wounds, where the study of defense wounds was instrumental in reconstructing the crime scene, thereby assisting the prosecution in establishing a plausible sequence of events. The cases are followed by a review of the literature on gunshot-related defense wounds
2. Case Reports
2.1. First Case
A 50-year-old man was killed by his son in a public square, shot with a smooth-bore shotgun. A sawed-off shotgun and two shotgun cartridges were found next to the body. External examination of the victim revealed multiple gunshot injuries. On the face, there was a cluster of wounds surrounded by abrasion collars. In the occipital region, there was a superficial and irregular hole, with numerous small metal pellets found in the scalp. Additionally, a circular “rat hole” wound measuring 3.5 cm in diameter was observed on the left scapular region, surrounded by an abrasion collar and pellet holes around the periphery.
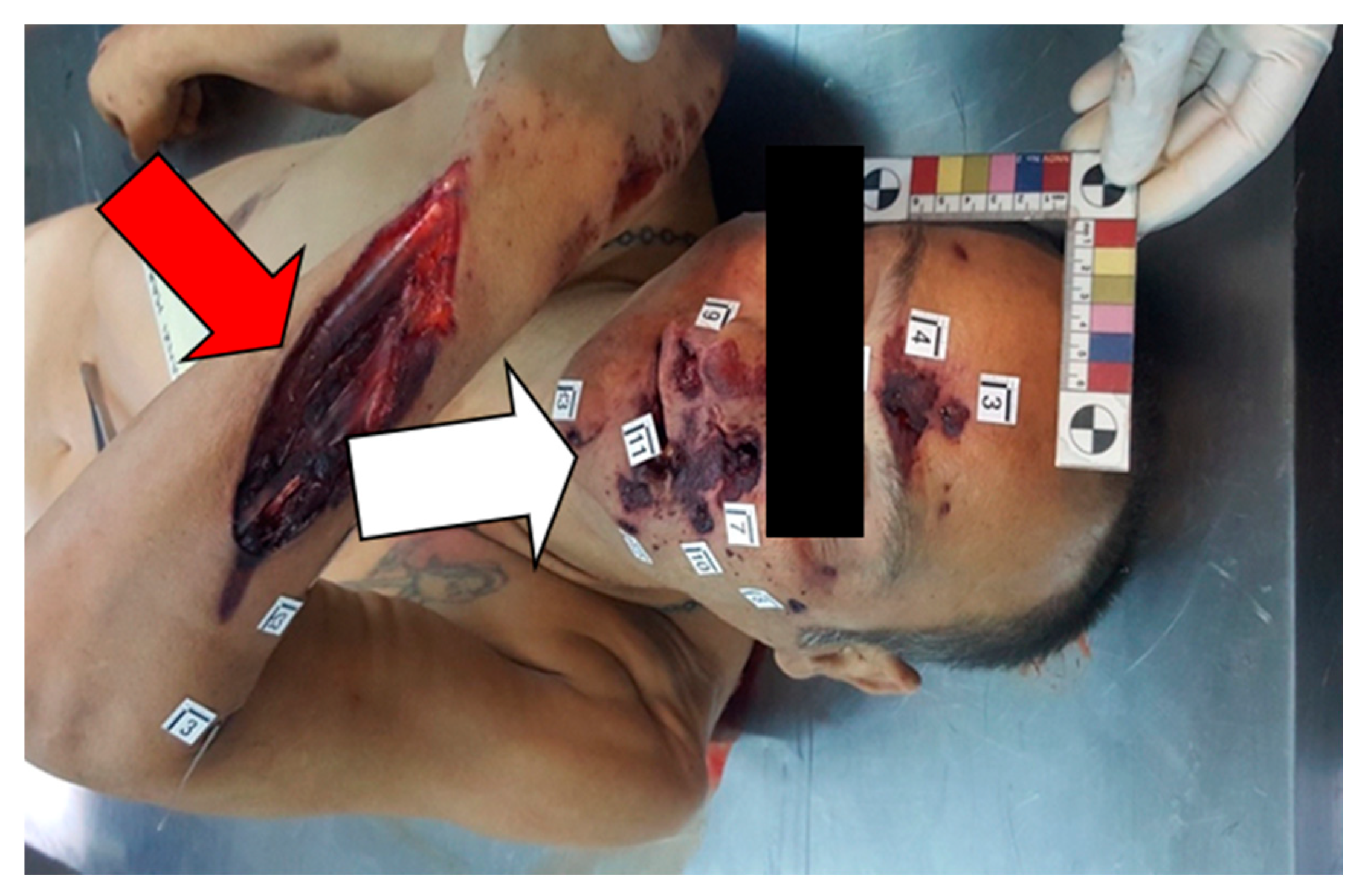
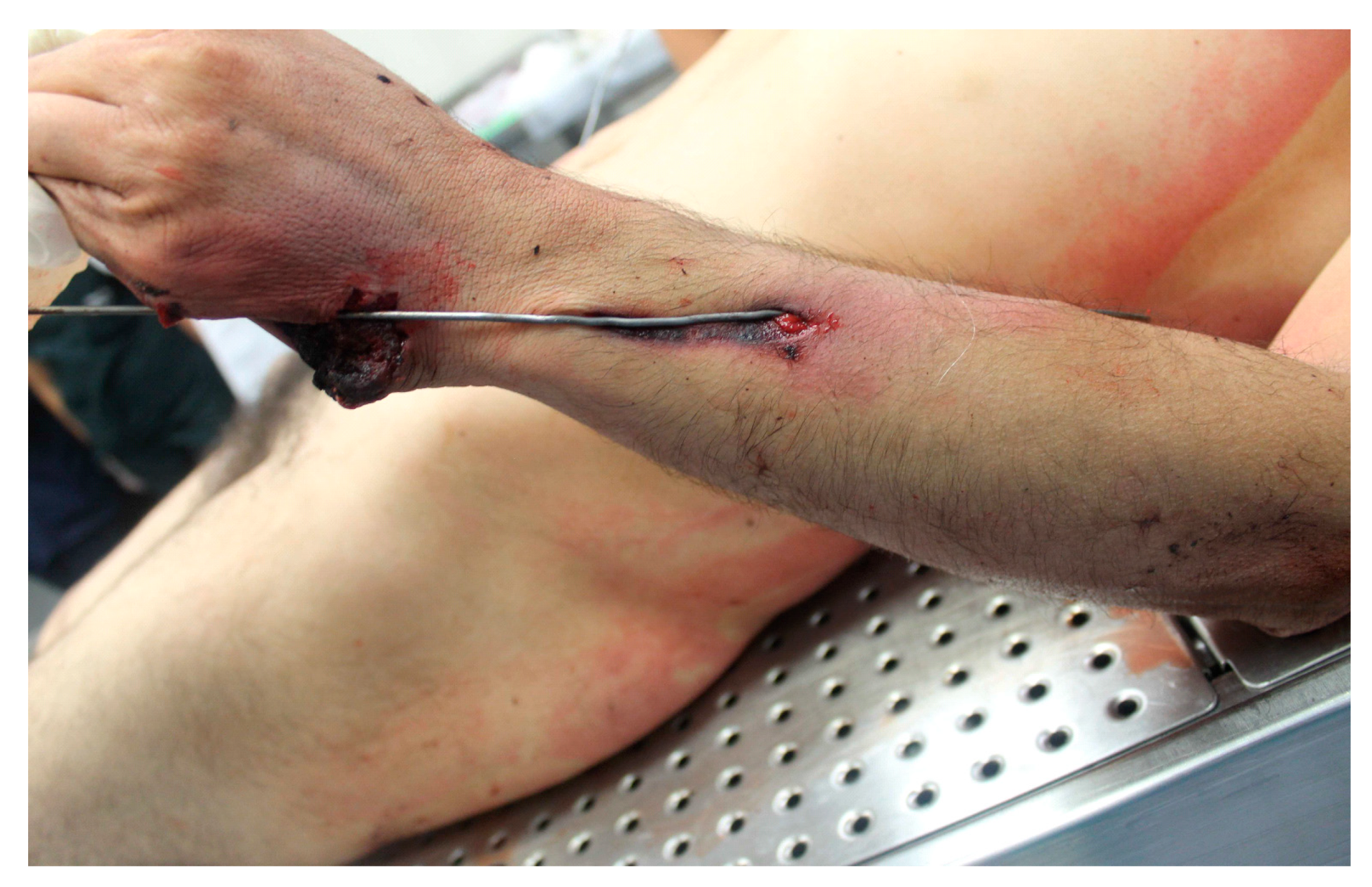
On the lateral surface of the left forearm, a “through-and-through” gunshot wound was noted, surrounded by an abrasion collar. Finally, a large gaping wound, also surrounded by an abrasion collar, was present on the posterior surface of the left forearm (Figure 1 and Figure 2).
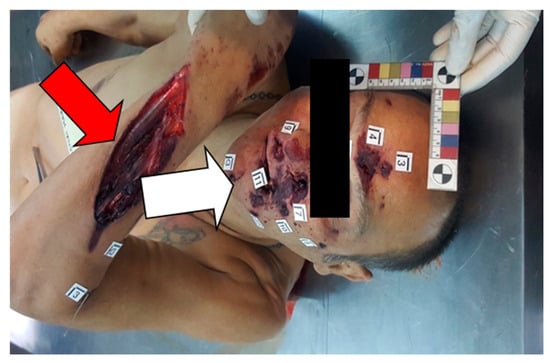
Figure 1.
First case. Red arrow: large gaping wound on the posterior surface of the left forearm. White arrow: the cluster of holes surrounded by abrasion collars. The coroner reconstructed the victim’s position, suggesting that the left forearm was bent to protect the face.

Figure 2.
First case. The “through-and-through” gunshot wound on the lateral surface of the left forearm surrounded by an abrasion collar.
The autopsy revealed the presence of small metal pellets in the injuries to the face and left side of the thorax. During the autopsy, a plastic wad was discovered lodged between the second and third left ribs, both of which were fractured. Another plastic wad was found on the left sleeve of the victim’s jacket. The cause of death was determined to be a transection of the thoracic aorta caused by gunshot wounds. In this first case, the authors proposed three bullet trajectories.
Two gunshots struck the left forearm before impacting the face and occipital region. The first injury was a “through-and-through” wound on the lateral surface of the left forearm, with closely situated entrance and exit wounds. The second was a large gaping wound on the posterior surface of the left forearm, resulting from a tangential bullet trajectory, which subsequently impacted the cephalic region.
These superficial wounds with tangential trajectories can be classified as “passive” gunshot defense injuries, sustained when the victim raises their forearm to protect their face and head. The fatal gunshot passed through the left scapula, perforating the left lung lobe, the thoracic aorta, and the second and third ribs. The firing distance was estimated to be approximately 1 m, based on the characteristics of the gunshot entrance wounds, particularly the “rat hole” wound in the left scapular region. It was hypothesized that the victim saw the attacker armed with the weapon and consequently attempted to defend themselves from the shots.
2.2. Second Case
A 33-year-old man was killed in the garden of his apartment. External examination revealed multiple gunshot injuries. An entry wound was identified on the dorsal surface of the right hand. On the palmar surface of the right hand, a cluster of wounds with smoke soiling was observed: one on the fourth metacarpal bone with a “star-shaped” pattern and irregular edges (with a nearby superficial wound), and two on the proximal phalanx of the first finger, both with irregular shapes and edges. Additionally, a graze wound was noted on the posterior surface of the left forearm.
On the hypothenar eminence of the left hand, a significant breach in the skin was surrounded by burning and smoke soiling.
The autopsy revealed a wound to the pectoral muscle, a fracture of the fourth left rib, and two wounds to the left lung. Two metal ogive bullets were recovered near the aorta and sacrum.
In this second case, the authors identified three distinct gunshot trajectories. The injuries to the right hand were interpreted as passive defense wounds, resulting from the victim’s attempt to shield his abdomen. The wounds to the left hand were considered active defense wounds, likely sustained when the victim attempted to grasp the firearm.
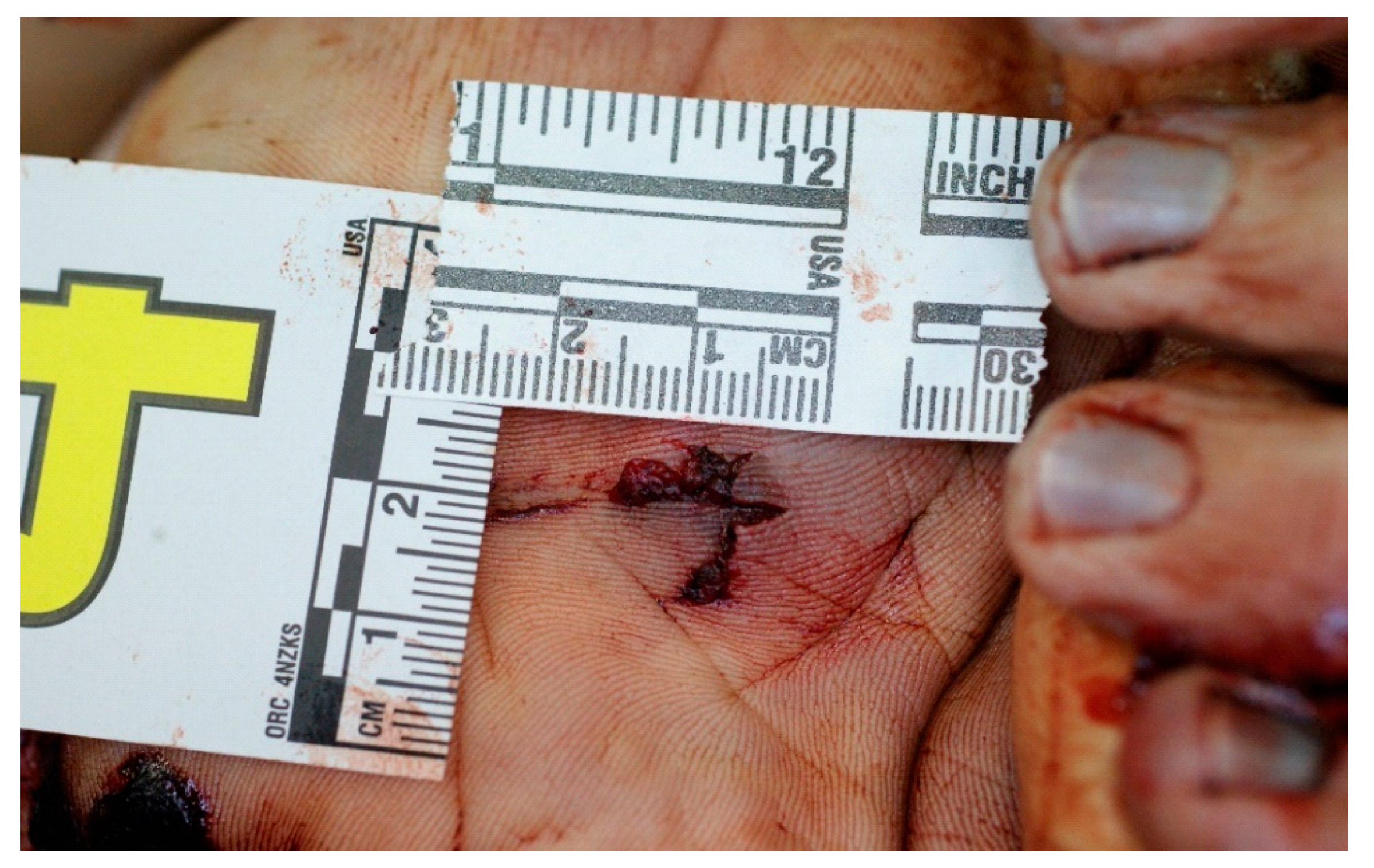
Specifically, the first gunshot penetrated the dorsal surface of the right hand, exited through the palmar surface, and created a re-entry wound by perforating the proximal phalanx of the first finger on the right hand. The bullet then impacted the mesogastric region, penetrated it, and lodged in the sacrum (Figure 3 and Figure 4).

Figure 3.
Second case. Right hand wound on the palmar surface, with reconstruction of the trajectory.

Figure 4.
Second case. The trajectory of the passive gunshot defense wound resulting from the victim’s attempt to protect the abdomen.
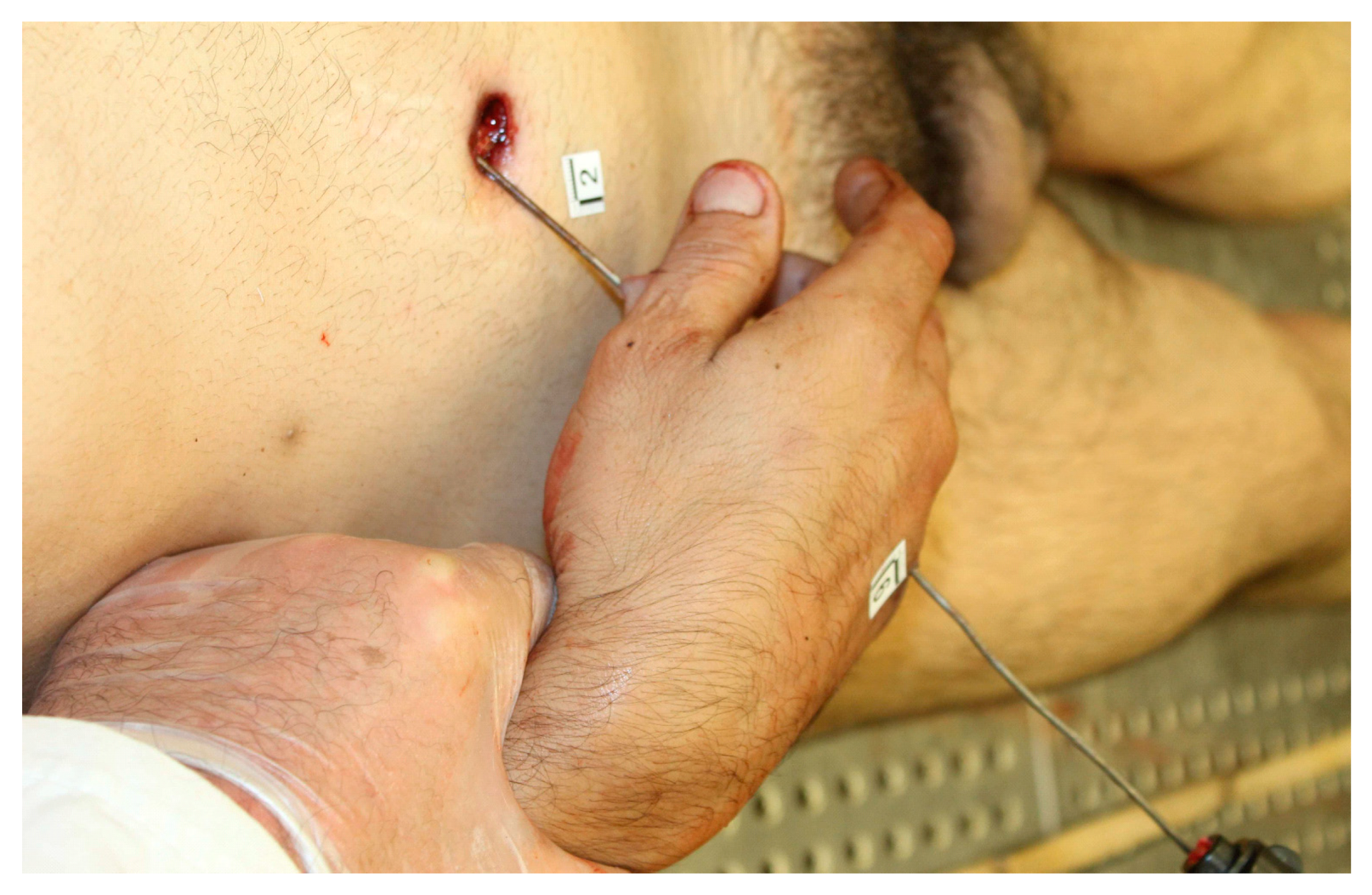
The second gunshot struck the hypothenar eminence of the left hand. Subsequently, the bullet tangentially impacted the left forearm, causing a graze wound—an elongated abrasion without skin perforation, characterized by irregular and bruised edges (Figure 5, Figure 6 and Figure 7). The characteristics of both injuries suggest that the shots were fired from a distance of less than 15 cm. This injury is considered an active defense wound, as it likely occurred while the victim attempted to grasp the weapon.

Figure 5.
Second case. Reconstruction of the trajectory of the active gunshot defense wounds resulting from the victim’s attempt to grasp the weapon.

Figure 6.
Second case. Detail of the graze wound on the posterior surface of the left hand.

Figure 7.
Second case. Detail on the left hand skin breach surrounded by burning and smoke soiling.
The fatal gunshot was the one that entered the left side of the thorax, perforating the left lung, heart, and abdominal aorta.
The pattern of gunshot defense wounds suggests that the attacker may not have initially intended to shoot the victim. The incident could have occurred following an argument, during which the victim had an opportunity to grab the weapon to distract the assailant. The police investigation revealed that the victim engaged in a struggle with the shooter and attempted to seize the gun.
2.3. Third Case
The third case concerns a 36-year-old man who was shot twice on a public street near his home, becoming the first victim in a triple murder. The attacker, a neighbor, subsequently fired additional shots at the victim’s father and aunt, both of whom also died. The weapon found at the crime scene was a Smith & Wesson revolver chambered in 0.357 Magnum. External examination of the victim revealed four gunshot injuries: a circular entrance wound on the left side of the temporal region with leakage of blood and brain matter; two wounds were observed on the left hand: one on the dorsum between the II and III metacarpals (entry wound), and the other on the palmar surface (exit wound). In addition, there were abrasions and fractures at the distal phalanges of the fourth and fifth fingers of the left hand. A fourth circular re-entry wound was found in the thorax (Figure 8, Figure 9, Figure 10 and Figure 11).

Figure 8.
Third case. The round injury on the dorsal surface of the left hand with an abrasion collar.
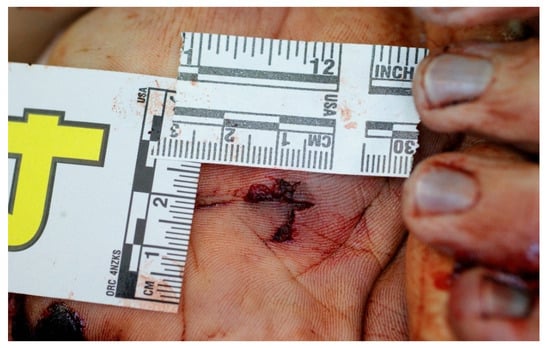
Figure 9.
Third case. The left hand’s palmar wound with irregular edges.

Figure 10.
Third case. The effects of the destructive action of the bullet, abrasions, and fractures on the distal phalanges of the fourth and fifth rays of the left hand.

Figure 11.
Third case. Oval-shaped thoracic skin lesion with an abrasive collar and bruised edges (re-entry wound).
The autopsy revealed a fracture at the base of the skull. The brain showed hemorrhagic infiltration in the left temporoparietal region, with evidence of a bullet path extending from the frontal to the occipital surface.
The left thoracic muscles showed hemorrhagic infiltration, with a wound in continuity with the thoracic skin lesion. The right lung exhibited a laceration of the upper lobe, accompanied by a massive hemothorax.
Two metal ogive bullets were recovered: one from the subcutaneous tissue of the extracranial region and the other from the subcutaneous tissue in the thoracic region, corresponding to the right sixth rib. The cause of death was cerebral collapse and hemothorax resulting from open trauma to the skull and thorax.
In this case, the rounded shape of the wound on the left hand suggests an approximately orthogonal firing angle. The exit wound on the palm and the re-entry wound on the left side of the thorax indicate that the victim assumed a defensive “avoidance/protection” posture, flexing the left upper limb or hand to shield themselves from the firearm. This is consistent with a passive defense wound caused by an attempt to protect the thorax.
None of the injuries showed signs of burning, soot, or stippling, suggesting that all shots were fired from a distance of more than 40–50 cm. Regarding the chronology of the shots, it is likely that the first bullet struck the victim in the thorax, while the second bullet, with the most immediately lethal effect, penetrated the cranial vault, causing cerebral collapse.
It is conceivable that the victim had enough time to see the attacker, the weapon, and the imminent shot. The killer confessed to surprising the victim in a car with his partner, making the partner leave, and then shooting the man, confirming that the victim had time to realize what was happening.
3. Gunshot Defense Wounds: A Literature Review
We reviewed current and recent textbooks, and the primary literature through hardcopy materials and PubMed literature searches. Textbooks were examined using the index and table of contents to locate sections on defense wounds, gunshot wounds, and ballistic injuries. Literature searches were conducted without filters using the following keywords: gunshot wounds, defense wounds, ballistic injury, and gunshot defense wounds. All publications with relevant content were reviewed.
The textbooks analyzed did not contain specific descriptions or references to gunshot defense wounds. There was only a brief mention that defense wounds can occur in firearm injuries, where an arm is raised in a desperate attempt to shield the trunk or head from the blast, similar to other types of injuries. This is exemplified by certain shooting deaths where entrance and exit wounds are found in the upper arm, with the projectile(s) then penetrating the trunk [5].
Textbooks provided references to defense wounds from stab or sharp weapons, with detailed descriptions of their characteristics. Similar results were found in PubMed searches, with little to no references to gunshot defense wounds. These scarce findings can be attributed to the low incidence of firearm-related defense injuries. Unlike stab defense wounds, gunshot defense wounds are rare because the shooter typically does not need to be close to the victim. When present, they resemble those seen in knife attacks [14].
A few studies of interest to our inquiry focus on injury patterns in gunshot wound cases. Some studies highlight the frequent involvement of the upper limbs in firearm injuries. An Italian study demonstrated that a high percentage of limb injuries (21.5%) (both upper and lower limbs) were associated with other lethal firearm wounds in homicide fatalities [15]. A more recent American study confirmed that the upper extremities are more frequently involved in homicides than in suicides [16].
Unfortunately, most of the significant literature addresses clinical gunshot wounds with an emphasis on wound management. However, these studies also provide useful data. Studies reporting on emergency department data show that many firearm injuries to the limbs result from accidents, such as during weapon cleaning. Other studies suggest that most firearm injuries are not accidental but rather result from fights or aggression, indicating some inconsistency in the data [17,18,19]. There is limited information on gunshot defense wounds in the scientific literature.
4. Discussion
As with other defense injuries, gunshot defense wounds can occur when the victim instinctively raises an arm or hand in a desperate attempt to shield the trunk or head from the blast [5].
This work presents three murder cases in which forensic pathologists detected multiple gunshot wounds on the forearms and hands, allowing them to reconstruct the dynamics of the assault by focusing on the pathological and morphological aspects of the wounds.
In these cases, gunshot defense wounds played a critical role in reconstructing the event, particularly in determining whether the victim had the opportunity and time to see the attacker and understand what was about to happen.
The presence of gunshot defense wounds is a key element in crime scene investigations and autopsies and warrants similar attention to that given to sharp or stab defense wounds. Furthermore, gunshot defense wounds may prompt investigators to explore the relationship between the victim and the shooter more deeply, considering the possibility that the killing was not premeditated but occurred during an argument or an attempt by the victim to grab the weapon.
Identifying gunshot defense wounds is crucial for reconstructing the dynamics of the assault, determining the bullet trajectory, and assessing the consistency of testimonies related to the attack. It is not uncommon for the perpetrator to claim that the gun was drawn only to frighten the victim, with a struggle ensuing afterward. As is well known, the first step in reconstructing bullet trajectories is identifying the entrance and exit wounds and their characteristics, which helps determine the shooting distance.
5. Conclusions
These three cases illustrate the importance of identifying defensive injuries. Despite their rarity, gunshot defense wounds should be studied and defined with the same rigor as defense wounds from sharp or stab weapons, with active and passive wounds being distinguishable in such cases. The study of defensive injuries can be decisive in reconstructing the crime scene and determining the manner of death in gunshot fatalities. Accurate crime scene reconstruction is a vital component of judicial and law enforcement investigations, as it can confirm or challenge statements and influence the charges against the offender with the expert contribution of forensic pathologists.
Author Contributions
L.A. and S.N., writing—original draft; M.B., writing—review and editing; D.F. and R.V., methodology and investigation; B.S., supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study did not require ethical approval as it did not involve humans. As stated in Recital 27 of the GDPR: “This Regulation does not apply to the personal data of deceased persons” (https://gdpr-info.eu/recitals/no-27/, accessed on 1 July 2024).
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Chattopadhyay, S.; Sukul, B. Pattern of defence injuries among homicidal victims. Egypt. J. Forensic Sci. 2013, 3, 81–84. [Google Scholar] [CrossRef]
- Deepali, P.; Mohite, P.M.M. Autopsy Evaluation of Defence Wounds in Homicidal Death in Central India. J. Forensic Res. 2013, 4, 5. Available online: https://www.omicsonline.org/autopsy-evaluation-of-defence-wounds-in-homicidal-death-in-central-india-2157-7145.1000205.php?aid=20742 (accessed on 11 April 2024).
- Shkrum, M.J.; Ramsay, D.A. Forensic Pathology of Thrauma, Common Problem for The Pathologist; Humana Press: Totowa, NJ, USA, 2007; p. 377. [Google Scholar]
- Racette, S.; Kremer, C.; Desjarlais, A.; Sauvageau, A. Suicidal and homicidal sharp force injury: A 5-year retrospective comparative study of hesitation marks and defense wounds. Forensic Sci. Med. Pathol. 2008, 4, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Saukko, P.; Knight, B. Knight’s Forensic Pathology, 3rd ed.; Hodder Arnold: London, UK, 2004; pp. 165–166. [Google Scholar]
- Katkici, Ü.; Özkök, M.S.; Örsal, M. An autopsy evaluation of defence wounds in 195 homicidal deaths due to stabbing. J. Forensic Sci. Soc. 1994, 34, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Pollak, S.; Saukko, P.J. Clinical forensic medicine|Defense Wounds. Encycl. Forensic Sci. 2000, 374–378. Available online: https://linkinghub.elsevier.com/retrieve/pii/B0122272153004388 (accessed on 11 April 2024).
- DiMaio, V.; DiMaio, D. Forensic Pathology, 2nd ed.; CRC Press: Boca Renton, FL, USA, 2001; p. 216. [Google Scholar]
- Hugar, B.S.; Harish, S.; Girish Chandra, Y.P.; Praveen, S.; Jayanth, S.H. Study of defence injuries in homicidal deaths—An autopsy study. J. Forensic Leg. Med. 2012, 19, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, M.K.; Panigrahi, M.K.; Mohanty, S.; Dash, J.K.; Dash, S.K. Self-defense injuries in homicidal deaths. J. Forensic Leg. Med. 2007, 14, 213–215. [Google Scholar] [CrossRef] [PubMed]
- Ambade, V.N.; Godbole, H.V. Comparison of wound patterns in homicide by sharp and blunt force. Forensic Sci. Int. 2006, 156, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, U.; Pollak, S. Sharp force injuries in clinical forensic medicine-findings in victims and perpetrator. Forensic Sci. Int. 2006, 159, 113–118. [Google Scholar] [CrossRef]
- O’Donovan, S.; Langlois, N.E.I.; Byard, R.W. “Defense” type wounds in suicide. Forensic Sci. Med. Pathol. 2018, 14, 402–405. [Google Scholar] [CrossRef]
- Rouse, D.; Dunn, L. Firearm fatalities. Forensic Sci. Int. 1992, 56, 59–64. [Google Scholar] [CrossRef]
- Solarino, B.; Nicoletti, E.M.; Di Vella, G. Fatal firearm wounds: A retrospective study in Bari (Italy) between 1988 and 2003. Forensic Sci. Int. 2007, 168, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Gitto, L.; Arunkumar, P.; Segovia, A.; Filkins, J.A.; Formica, M.K.; Serinelli, S. Anatomical distribution and autopsy features of gunshot injuries to support the manner of death. J. Forensic Leg. Med. 2021, 79, 102135. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, A.J.; Kusnezov, N.A.; Dunn, J.C.; Rensing, N.; Prabhakar, G.; Pirela-Cruz, M.A. Epidemiology of gunshot wounds to the hand. Hand Surg. Rehabil. 2019, 38, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Toston, R.J.; Graf, A.R.; Dawes, A.M.; Farley, K.X.; Hurt, J.T.; Karzon, A.; Ojemakinde, A.A.; Gottschalk, M.B.; Wagner, E.R. Upper extremity firearm injuries: Epidemiology and factors predicting hospital admission. Eur. J. Orthop. Surg. Traumatol. 2023, 33, 1173–1178. [Google Scholar] [CrossRef] [PubMed]
- Anantavorasakul, N.; Westenberg, R.F.; Serebrakian, A.T.; Zamri, M.; Chen, N.C.; Eberlin, K.R. Gunshot Injuries of the Hand: Incidence, Treatment Characteristics, and Factors Associated With Healthcare Utilization. Hand 2023, 18, 158–166. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).