
Relationship Between the Anteroposterior Acceleration of Lower Lumbar Spine and Pelvic Tilt Movements During Running

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
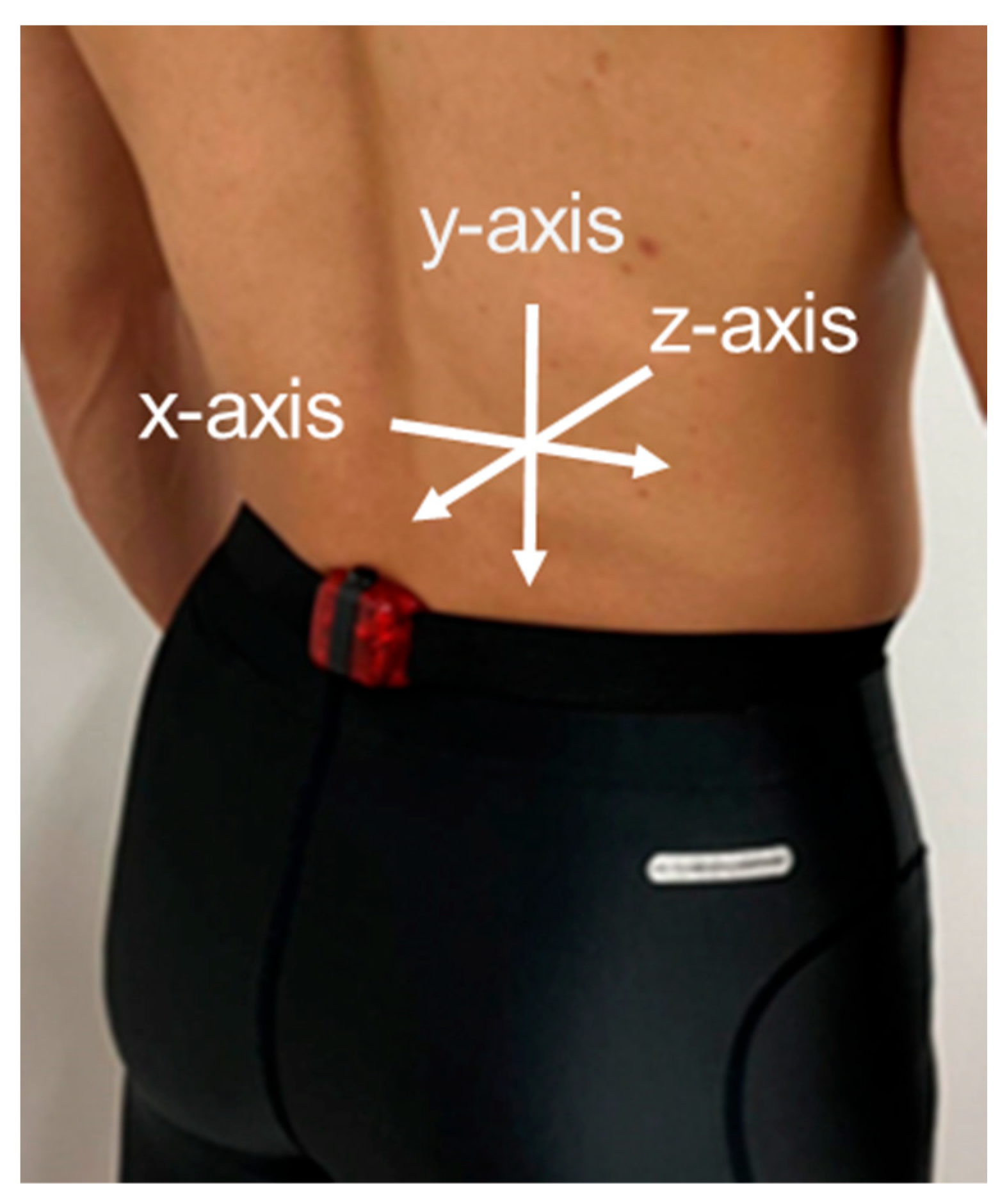
2.2. Procedures
2.3. Data Analysis
2.4. Statistical Analysis
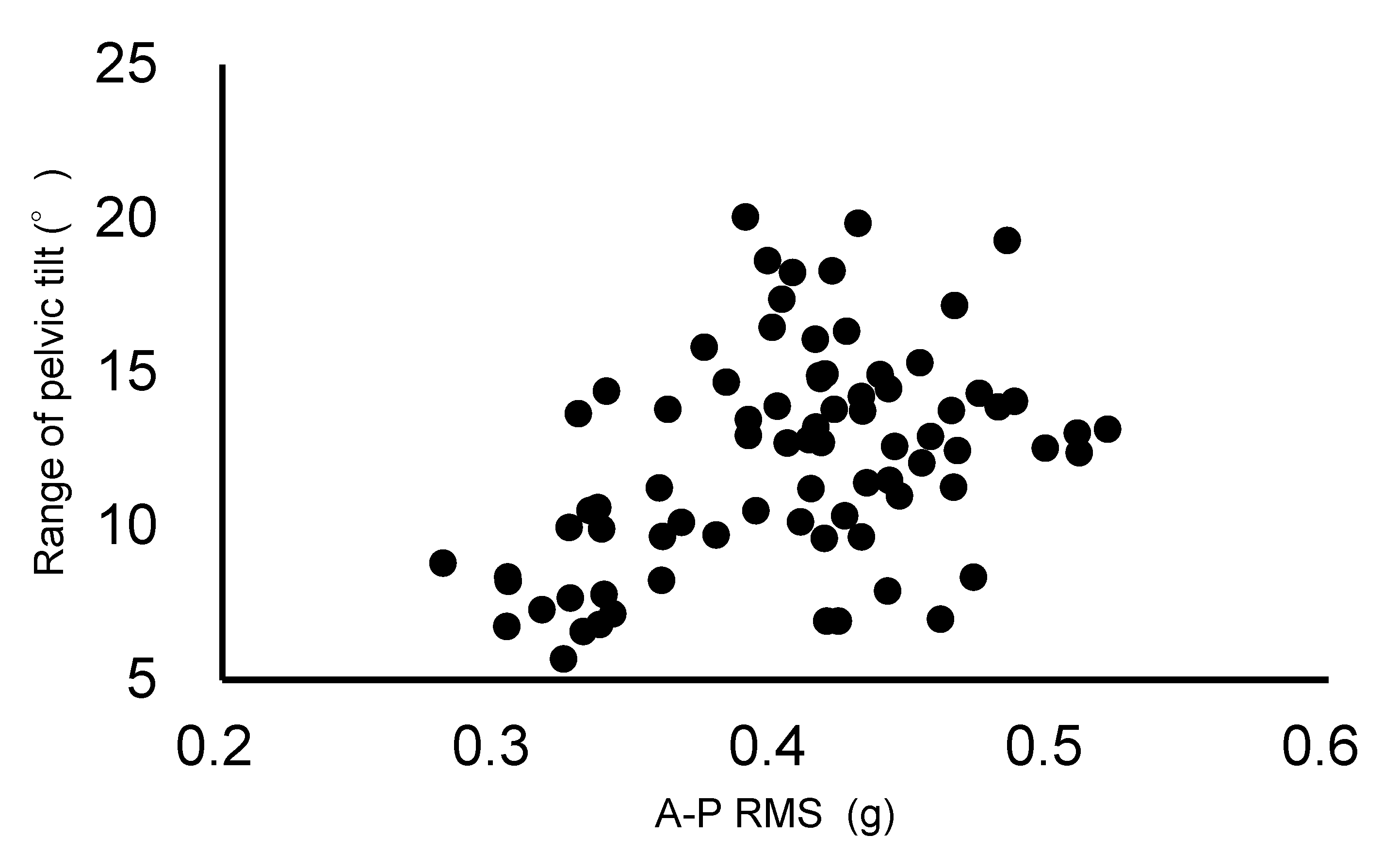
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Min, S.K.; Nakazato, K.; Yamamoto, Y.; Gushiken, K.; Fujimoto, H.; Fujishiro, H.; Kobayakawa, Y.; Hiranuma, K. Cartilage intermediate layer protein gene is associated with lumbar disc degeneration in male, but not female, collegiate athletes. Am. J. Sports Med. 2010, 38, 2552–2557. [Google Scholar] [CrossRef] [PubMed]
- Hangai, M.; Kaneoka, K.; Hinotsu, S.; Shimizu, K.; Okubo, Y.; Miyakawa, S.; Mukai, N.; Sakane, M.; Ochiai, N. Lumbar intervertebral disk degeneration in athletes. Am. J. Sports Med. 2009, 37, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Koyama, K.; Nakazato, K.; Hiranuma, K. Etiology and nature of intervertebral disc degeneration and its correlation with low back pain. J. Phys. Fit. Sports Med. 2015, 4, 63–72. [Google Scholar] [CrossRef]
- Chan, S.C.; Ferguson, S.J.; Gantenbein-Ritter, B. The effects of dynamic loading on the intervertebral disc. Eur. Spine J. 2011, 20, 1796–1812. [Google Scholar] [CrossRef] [PubMed]
- Belavy, D.L.; Albracht, K.; Bruggemann, G.P.; Vergroesen, P.P.; Van Dieen, J.H. Can Exercise Positively Influence the Intervertebral Disc? Sports Med. 2016, 46, 473–485. [Google Scholar] [CrossRef] [PubMed]
- Belavy, D.L.; Quittner, M.J.; Ridgers, N.; Ling, Y.; Connell, D.; Rantalainen, T. Running exercise strengthens the intervertebral disc. Sci. Rep. 2017, 7, 45975. [Google Scholar] [CrossRef] [PubMed]
- Kawabata, M.; Goto, K.; Fukusaki, C.; Sasaki, K.; Hihara, E.; Mizushina, T.; Ishii, N. Acceleration patterns in the lower and upper trunk during running. J. Sports Sci. 2013, 31, 1841–1853. [Google Scholar] [CrossRef] [PubMed]
- Takatalo, J.; Karppinen, J.; Niinimaki, J.; Taimela, S.; Nayha, S.; Jarvelin, M.R.; Kyllonen, E.; Tervonen, O. Prevalence of degenerative imaging findings in lumbar magnetic resonance imaging among young adults. Spine 2009, 34, 1716–1721. [Google Scholar] [CrossRef]
- Wilke, H.; Neef, P.; Hinz, B.; Seidel, H.; Claes, L. Intradiscal pressure together with anthropometric data—A data set for the validation of models. Clin. Biomech. 2001, 16 (Suppl. S1), S111–S126. [Google Scholar] [CrossRef]
- Lindsay, T.R.; Yaggie, J.A.; McGregor, S.J. Contributions of lower extremity kinematics to trunk accelerations during moderate treadmill running. J. Neuroeng. Rehabil. 2014, 11, 162. [Google Scholar] [CrossRef]
- Franz, J.R.; Paylo, K.W.; Dicharry, J.; Riley, P.O.; Kerrigan, D.C. Changes in the coordination of hip and pelvis kinematics with mode of locomotion. Gait Posture 2009, 29, 494–498. [Google Scholar] [CrossRef]
- Schache, A.G.; Blanch, P.; Rath, D.; Wrigley, T.; Bennell, K. Three-dimensional angular kinematics of the lumbar spine and pelvis during running. Hum. Mov. Sci. 2002, 21, 273–293. [Google Scholar] [CrossRef] [PubMed]
- Takatalo, J.; Karppinen, J.; Nayha, S.; Taimela, S.; Niinimaki, J.; Blanco, S.R.; Tammelin, T.; Auvinen, J.; Tervonen, O. Association between adolescent sport activities and lumbar disk degeneration among young adults. Scand. J. Med. Sci. Sports 2017, 27, 1993–2001. [Google Scholar] [CrossRef] [PubMed]
- Sekine, C.; Matsunaga, N.; Kaneoka, K. Changes in Lumbopelvic Motion and Trunk Muscle Activity during 2000 m Rowing Ergometer Trial. Int. J. Sport Health Sci. 2021, 19, 47–57. [Google Scholar] [CrossRef]
- Schache, A.G.; Blanch, P.D.; Murphy, A.T. Relation of anterior pelvic tilt during running to clinical and kinematic measures of hip extension. Br. J. Sports Med. 2000, 34, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, A.; Takeshita, T.; Yanagiya, T. Differences in sprinting performance and kinematics between preadolescent boys who are fore/mid and rear foot strikers. PLoS ONE 2018, 13, e0205906. [Google Scholar] [CrossRef] [PubMed]
- Wundersitz, D.W.; Gastin, P.B.; Richter, C.; Robertson, S.J.; Netto, K.J. Validity of a trunk-mounted accelerometer to assess peak accelerations during walking, jogging and running. Eur. J. Sport Sci. 2015, 15, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Crosbie, J.; Vachalathiti, R.; Smith, R. Patterns of spinal motion during walking. Gait Posture 1997, 5, 6–12. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kubo, Y.; Koyama, K.; Kimura, T. Relationship Between the Anteroposterior Acceleration of Lower Lumbar Spine and Pelvic Tilt Movements During Running. Biomechanics 2024, 4, 765-772. https://doi.org/10.3390/biomechanics4040056
Kubo Y, Koyama K, Kimura T. Relationship Between the Anteroposterior Acceleration of Lower Lumbar Spine and Pelvic Tilt Movements During Running. Biomechanics. 2024; 4(4):765-772. https://doi.org/10.3390/biomechanics4040056
Chicago/Turabian StyleKubo, Yoshiaki, Koji Koyama, and Taichi Kimura. 2024. "Relationship Between the Anteroposterior Acceleration of Lower Lumbar Spine and Pelvic Tilt Movements During Running" Biomechanics 4, no. 4: 765-772. https://doi.org/10.3390/biomechanics4040056
APA StyleKubo, Y., Koyama, K., & Kimura, T. (2024). Relationship Between the Anteroposterior Acceleration of Lower Lumbar Spine and Pelvic Tilt Movements During Running. Biomechanics, 4(4), 765-772. https://doi.org/10.3390/biomechanics4040056