
Conceptual Models of Disability: The Development of the Consideration of Non-Biomedical Aspects

Abstract
:
1. Introduction
2. On Models
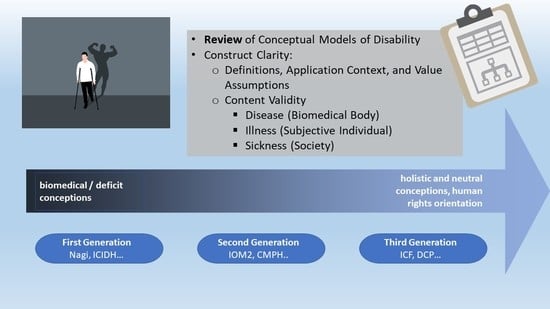
3. Methodological Approach
- Definitions
- Application Context and Value Assumptions
- Content Validity
- Disease (Biomedical Body)
- Illness (Subjective Individual)
- Sickness (Society)
4. Conceptual Models
4.1. First Generation (1965–1994)
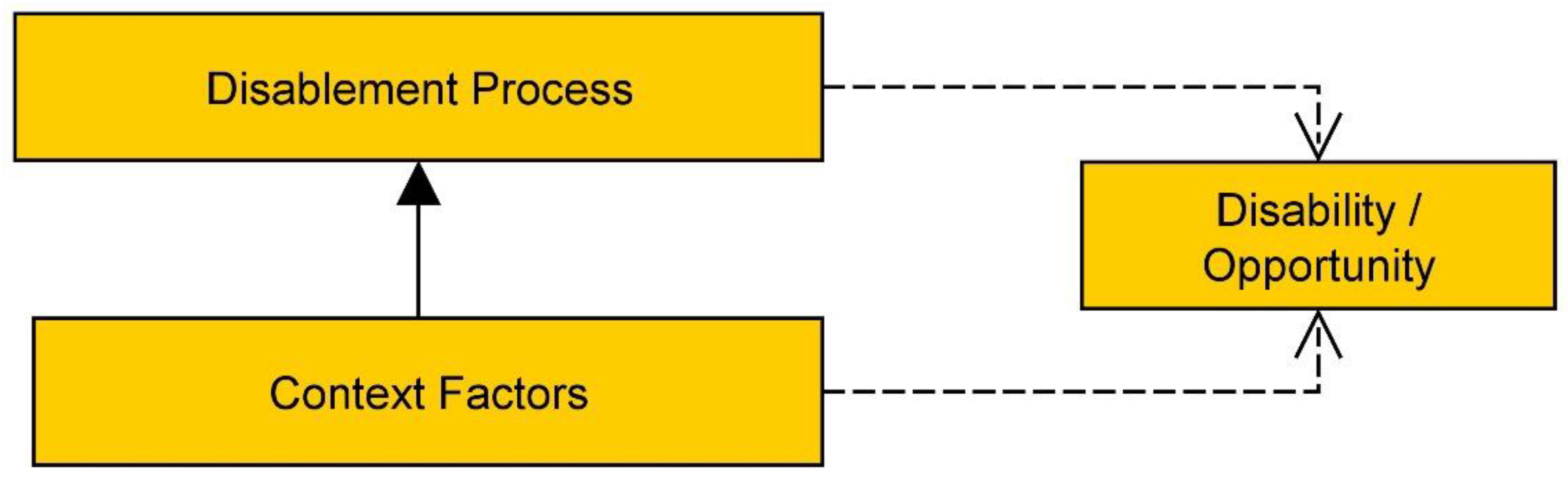
4.1.1. The Disablement Process
4.1.2. Context Factors
4.1.3. Quality of Life
4.1.4. Evaluation
- Definitions
- Application Context and Value Assumptions
- Content Validity
- Disease
- Illness
- Sickness
4.2. Second Generation (1996–1997; 2006)
4.2.1. Disability Relation and Context Factors
4.2.2. Evaluation
- Definitions
- Application Context and Value Assumptions
- Content Validity
- Disease
- Illness
- Sickness
4.3. Third Generation (1999–2019)
4.3.1. Main Components
4.3.2. Context Factors
4.3.3. Evaluation
- Definition
- Application Context and Value Assumptions
- Content Validity
- Disease
- Illness
- Sickness
5. Discussion
6. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Shakespeare, T.; Bickenbach, J.E.; Pfeiffer, D.; Watson, N. Models. In Encyclopedia of Disability; Albrecht, G.L., Ed.; Sage Publications: Thousand Oaks, CA, USA, 2006; pp. 1101–1107. ISBN 9780761925651. [Google Scholar]
- Waddington, L.; Priestley, M. A human rights approach to disability assessment. J. Int. Comp. Soc. Policy 2021, 37, 1–15. [Google Scholar] [CrossRef]
- World Health Organization; The World Bank. Chapter 1—Understanding Disability. In World Report on Disability; World Bank, Ed.; WHO: Geneva, Switzerland, 2011; pp. 3–17. [Google Scholar]
- Egen, C. Was Ist Behinderung? Abwertung und Ausgrenzung von Menschen mit Funktionseinschränkungen vom Mittelalter bis zur Postmoderne [What Is Disability? Devaluation and Exclusion of People with Functional Limitations from the Middle Ages to Postmodernity]; Transcript: Bielefeld, Germany, 2020; ISBN 9783837653335. [Google Scholar]
- Union of the Physically Impaired Against Segregation. Fundamental Principle of Disability. 1975. Available online: https://disability-studies.leeds.ac.uk/wp-content/uploads/sites/40/library/UPIAS-fundamental-principles.pdf (accessed on 26 May 2022).
- Hurst, R. The International Disability Rights Movement and the ICF. Disabil. Rehabil. 2003, 25, 572–576. [Google Scholar] [CrossRef] [PubMed]
- Fougeyrollas, P.; Beaureard, L. Disability: An Interactive Person-Environment Social Creation. In Handbook of Disability Studies; Albrecht, G.L., Seelman, K.D., Bury, M., Eds.; Sage Publications: Thousand Oaks, CA, USA, 2001; pp. 171–194. ISBN 9780761916529. [Google Scholar]
- Biermann, J.; Pfahl, L. A Global Monitoring Practice in the Making: Disability Measurement for UN Sustainable Development Goal 4 on Inclusive Education. Osterr. Z. Geschichtswissenschaften 2020, 31, 192–213. [Google Scholar] [CrossRef]
- Petretto, D.; Vinci, S.; Todde, I.; Piras, P.; Pistis, I.; Masala, C. Conceptual Models of Disability and Their Role in the Daily Routine of Clinical Rehabilitation. Rehabil. Sci. 2017, 4, 75–81. [Google Scholar]
- Altman, B.M. Definitions, Models, Classifications, Schemes, and Applications. In Handbook of Disability Studies; Albrecht, G.L., Seelman, K.D., Bury, M., Eds.; Sage Publications: Thousand Oaks, CA, USA, 2001; pp. 97–122. ISBN 9780761916529. [Google Scholar]
- Ralston, D.C. The Concept of Disability: A Philosophical Analysis. Ph.D. Thesis, Rice University, Houston, TX, USA, 2012. [Google Scholar]
- Snyder, A.R.; Parsons, J.T.; Valovich McLeod, T.C.; Curtis Bay, R.; Michener, L.A.; Sauers, E.L. Using disablement models and clinical outcomes assessment to enable evidence-based athletic training practice, Part I: Disablement models. J. Athl. Train. 2008, 43, 428–436. [Google Scholar] [CrossRef]
- Bickenbach, J.E.; Chatterji, S.; Badley, E.M.; Üstün, T.B. Models of disablement, universalism and the international classification of impairments, disabilities and handicaps. Soc. Sci. Med. 1999, 48, 1173–1187. [Google Scholar] [CrossRef]
- Bickenbach, J.E. The International Classifcation of Functioning, Disability and Health and its Relationship to Disability Studies. In Routledge Handbook of Disability Studies; Watson, N., Roulstone, A., Thomas, C., Eds.; First issued in, paperback; Routledge: London, UK; New York, NY, USA, 2014; pp. 51–66. ISBN 9780415574006. [Google Scholar]
- Nagi, S.Z. A Disability concepts revisited: Implication for prevention. In Disability in America; Institute of Medicine, Ed.; National Academies Press: Washington, DC, USA, 1991; ISBN 978-0-309-04378-6. [Google Scholar]
- Manhart, K. KI-Modelle in Den Sozialwissenschaften: Logische Struktur und Wissensbasierte Systeme von Balancetheorien [AI-Models in Social Sciences: Logical and Knowledge-Based Systems of Balance Theories]; Walter de Gruyter GmbH: Berlin, Germany; Boston, MA, USA, 2015; ISBN 3-486-56105-7. [Google Scholar]
- Saam, N.J.; Gautschi, T. Modellbildung in den Sozialwissenschaften (Modelling in the Social Sciences). In Handbuch Modellbildung und Simulation in den Sozialwissenschaften [Handbook Modelling and Simulation in Social Sciences]; Braun, N., Saam, N.J., Eds.; Springer: Berlin/Heidelberg, Germany, 2015; pp. 15–60. ISBN 978-3-658-01163-5. [Google Scholar]
- McLaren, N. A critical review of the biopsychosocial model. Aust. N. Z. J. Psychiatry 1998, 32, 86–92. [Google Scholar] [CrossRef]
- Lave, C.A.; March, J.G. An Introduction to Models in the Social Sciences; University Press of America: Lanham, MD, USA, 1993; ISBN 0819183814. [Google Scholar]
- Stachowiak, H. Allgemeine Modelltheorie [General Model Theory]; Springer: Wien, Austria, 1973; ISBN 3-211-81106-0. [Google Scholar]
- Koperski, J. Models. In The Internet Encyclopedia of Philosophy; Fieser, J., Dowden, B., Eds.; Stanford University: Stanford, CA, USA, 2019; Available online: https://iep.utm.edu/models/ (accessed on 30 August 2022).
- Wasserman, D.; Aas, S. Disability: Definitions and Models. In The Stanford Encyclopedia of Philosophy; Zalta, E.N., Ed.; Metaphysics Research Lab, Stanford University: Stanford, CA, USA, 2022; Available online: https://plato.stanford.edu/archives/sum2022/entries/disability/ (accessed on 27 August 2022).
- DeVidi, D.; Klausen, C. No Mere Difference. Dialogue 2017, 56, 357–379. [Google Scholar] [CrossRef]
- Fougeyrollas, P.; Grenier, Y. Monitoring Disability Policies and Legislation towards Effective Exercise of Rights to Equality and Inclusive Access for Persons with Disabilities: The Case of the Quebec Model. Societies 2018, 8, 41. [Google Scholar] [CrossRef]
- Rice, D.P.; Wunderlich, G.S.; Amado, N.L. The Dynamics of Disability: Measuring and Monitoring Disability for Social Security Programs; National Academy Press: Washington, DC, USA, 2002; ISBN 9780309084192. [Google Scholar]
- Verbrugge, L.M.; Jette, A.M. The disablement process. Soc. Sci. Med. 1994, 38, 1–14. [Google Scholar] [CrossRef]
- McKenzie, F.D. Systems Modeling: Analysis and Operations Research. In Modeling and Simulation Fundamentals: Theoretical Underpinnings and Practical Domains; Sokolowski, J.A., Banks, C.M., Eds.; Wiley: Hoboken, NJ, USA, 2010; pp. 147–180. ISBN 9780470590621. [Google Scholar]
- Masala, C.; Petretto, D.R. From disablement to enablement: Conceptual models of disability in the 20th century. Disabil. Rehabil. 2008, 30, 1233–1244. [Google Scholar] [CrossRef] [PubMed]
- Drum, C.E.; Krahn, G.; Culley, C.; Hammond, L. Recognizing and Responding to the Health Disparities of People with Disabilities. Calif. J. Health Promot. 2005, 3, 29–42. [Google Scholar] [CrossRef]
- Suddaby, R. Editor’s Comments: Construct Clarity in Theories of Management and Organization. Acad. Manag. Rev. 2010, 35, 346–357. [Google Scholar]
- Jette, A.M. Physical disablement concepts for physical therapy research and practice. Phys. Ther. 1994, 74, 380–386. [Google Scholar] [CrossRef]
- Institute of Medicine. Disability in America; National Academies Press: Washington, DC, USA, 1991; pp. 1–288. ISBN 978-0-309-04378-6. [Google Scholar]
- Forstner, M. Biophänomenosoziales Modell von Behinderung [Biophenomenosocial model of Disability]. Z. Disabil. Stud. 2022, 1–16. [Google Scholar] [CrossRef]
- Hofmann, B. Disease, Illness, and Sickness. The Routledge Companion to Philosophy of Medicine; Routledge: London, UK, 2016. [Google Scholar]
- World Health Organization. ICF—International Classification of Functioning, Disability and Health Functioning, Disability and Health; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Hahn, H.D.; Belt, T.L. Disability Identity and Attitudes Toward Cure in a Sample of Disabled Activists. J. Health Soc. Behav. 2004, 45, 453–464. [Google Scholar] [CrossRef]
- Oliver, M. Understanding Disability; Macmillan Education UK: London, UK, 1996; ISBN 978-0-333-59916-7. [Google Scholar]
- Oliver, M. Understanding Disability: From Theory to Practice, 2nd ed.; Palgrave Macmillan: Basingstoke, UK, 2009; ISBN 9780230220287. [Google Scholar]
- Thomas, C. Sociologies of Disability and Illness: Contested Ideas in Disability Studies and Medical Sociology; Palgrave Macmillan: Basingstoke, UK, 2007; ISBN 9781403936370. [Google Scholar]
- Bê, A. Ableism and disablism in higher education: The case of two students living with chronic illnesses. Alter 2019, 13, 179–191. [Google Scholar] [CrossRef]
- Terry, P.M. Preparing Educational Leaders to Eradicate the “Isms”. In Proceedings of the Annual Meeting of the International Congress on Challenges to Education, Palm Beach, Aruba, 10–12 July 1996. [Google Scholar]
- Badley, E.M. ICF and other conceptual models: Rethinking the role of context and implications for assesing health. In Perceived Health and Adaptation in Chronic Disease; Guillemin, F., Leplège, A., Briançon, S., Spitz, E., Coste, J., Eds.; Routledge: London, UK; Taylor & Francis Group: Abingdon, UK, 2018; pp. 32–43. ISBN 978-1-4987-7898-5. [Google Scholar]
- Whiteneck, G. Conceptual Models of Disability, Past Present and Future. In Workshop on Disability in America; Institute of Medicine, Ed.; National Academies Press: Washington, DC, USA, 2006; pp. 50–66. ISBN 978-0-309-10090-8. [Google Scholar]
- Nagi, S.Z. Some Conceptual Issues in Disability and Rehabilitation. In Sociology and Rehabilitation; Sussman, M.B., Ed.; American Sociological Association: Washington, DC, USA, 1965; pp. 100–113. [Google Scholar]
- Suchman, E.A. A Model for Research and Evaluation on Rehabilitation. In Sociology and Rehabilitation; Sussman, M.B., Ed.; American Sociological Association: Washington, DC, USA, 1965; pp. 52–70. [Google Scholar]
- Jette, A.M.; Badley, E.M. Conceptual Issues in the Measurement of Work Disability. In Survey Measurement of Work Disability: Summary of a Workshop; Mathiowetz, N., Wunderlich, G.S., Eds.; National Academies Press: Washington, DC, USA, 2000; pp. 4–27. ISBN 0309068991. [Google Scholar]
- Jette, A.M.; Keysor, J.J. Disability models: Implications for arthritis exercise and physical activity interventions. Arthritis Rheum. 2003, 49, 114–120. [Google Scholar] [CrossRef] [PubMed]
- de Leon, C.F.M.; Freedman, V.A. Measuring disability, physical functions and cognitive abilities of adults: Survey enhancements and options for a new panel study. J. Econ. Soc. Meas. 2015, 40, 371–399. [Google Scholar]
- World Health Organization. International Classification of Impairments, Disabilities, and Handicaps: A Manual of Classification Relating to the Consequences of Disease; WHO: Geneva, Switzerland, 1980. [Google Scholar]
- Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD); NIH; HHS. Research Plan for the National Center for Medical Rehabilitation Research. 1993. Available online: https://www.nichd.nih.gov/publications/product/109 (accessed on 28 August 2022).
- Eunice Kennedy Shriver National Institute of Child Health and Human Development; NIH; DHHS. National Center for Medical Rehabilitation Research (NCMRR), NICHD, Report to the NACHHD Council. 2006. Available online: https://www.nichd.nih.gov/publications/product/13 (accessed on 29 August 2022).
- Institute of Medicine. Enabling America: Assessing the Role of Rehabilitation Science and Engineering; National Academy Press: Washington, DC, USA, 1997; ISBN 9780309063746. [Google Scholar]
- Barnes, E.B. The Minority Body: A Theory of Disability, 1st ed.; Oxford University Press: Oxford, UK, 2016; ISBN 9780198822417. [Google Scholar]
- Swain, J.; French, S. Towards an Affirmation Model of Disability. Disabil. Soc. 2000, 15, 569–582. [Google Scholar] [CrossRef]
- Waldschmdit, A. Disability Goes Cultural. In Culture—Theory—Disability; Waldschmidt, A., Berressem, H., Ingwersen, M.F., Eds.; Transcript: Bielefeld, Germany, 2017; pp. 19–28. ISBN 9783839425336. [Google Scholar]
- Johnson, R.J.; Wolinsky, F.D. The Structure of Health Status Among Older Adults: Disease, Disability, Functional Limitation, and Perceived Health. J. Health Soc. Behav. 1993, 34, 105. [Google Scholar] [CrossRef] [PubMed]
- Verbrugge, L.M. Disability Experience and Measurement. J. Aging Health 2016, 28, 1124–1158. [Google Scholar] [CrossRef] [PubMed]
- Shakespeare, T.; Watson, N. The social model of disability: An outdated ideology? In Exploring Theories and Expanding Methodologies: Where We are and Where We Need to Go; Barnartt, S.N., Ed.; Emerald Group Publishing Limited: Bingley, UK, 2001; pp. 9–28. ISBN 0-7623-0773-0. [Google Scholar]
- Verbrugge, L. The iceberg of disability. In The Legacy of Logevity: Health and Health Care in Later Life; Stahl, S.M., Ed.; Sage Publications: Newbury Park, CA, USA, 1990; pp. 55–75. [Google Scholar]
- Hurst, R. To Revise or Not to Revise? Disabil. Soc. 2000, 15, 1083–1087. [Google Scholar] [CrossRef]
- Patrick, D.L. Rethinking prevention for people with disabilities. Part I: A conceptual model for promoting health. Am. J. Health Promot. 1997, 11, 257–260. [Google Scholar] [CrossRef]
- Degener, T. A human rights model of disability. In Routledge Handbook of Disability Law and Human Rights; Routledge: London, UK, 2014. [Google Scholar]
- Sparrow, R. Defending Deaf Culture: The Case of Cochlear Implants. J. Polit. Philos. 2005, 13, 135–152. [Google Scholar] [CrossRef]
- Bajan, B.; Parish, E. Deaf Culture. In Encyclopedia of Disability; Albrecht, G.L., Ed.; Sage Publications: Thousand Oaks, CA, USA, 2006; pp. 349–352. ISBN 9780761925651. [Google Scholar]
- Kostanjsek, N. Use of The International Classification of Functioning, Disability and Health (ICF) as a conceptual framework and common language for disability statistics and health information systems. BMC Public Health 2011, 11 (Suppl. 4), S3. [Google Scholar] [CrossRef]
- Mitra, S. The Capability Approach and Disability. J. Disabil. Policy Stud. 2006, 16, 236–247. [Google Scholar] [CrossRef]
- Fougeyrollas, P.; Boucher, N.; Edwards, G.; Grenier, Y.; Noreau, L. The Disability Creation Process Model: A Comprehensive Explanation of Disabling Situations as a Guide to Developing Policy and Service Programs. Scand. J. Disabil. Res. 2019, 21, 25–37. [Google Scholar] [CrossRef]
- Fougeyrollas, P.E.A. The Disability Creation Process: Analysis of the Consultation and New Proposal; QCICIDH: Quebéc City, QC, Canada, 1991. [Google Scholar]
- Hirschberg, M. Behinderung im Internationalen Diskurs: Die Flexible Klassifizierung der Weltgesundheitsorganisation [Disability in Interational Discourse]; Campus Verlag: Frankfurt, Germany; New York, NY, USA, 2009. [Google Scholar]
- Schuntermann, M.F. Einführung in die Internationale Klassifikation der Funktionsfähigkeit, Behinderung und Gesundheit (ICF) der Weltgesundheitsorganisation (WHO): Ein Grundkurs [Introduction to the International Classification of Functioning, Disability and Health (ICF) of the World Health Organization (WHO): A Basic Course]; Unter Besonderer Berücksichtigung der Sozialmedizinischen Begutachtung und Rehabilitation; Verband Deutscher Rentenversicherugnsträger: Frankfurt, Germany, 2004. [Google Scholar]
- World Health Organization. ICF—Internationale Klassifikation der Funktionsfähigkeit, Behinderung und Gesundheit [ICF—International Classification of Functioning, Disability and Health]; Deutsches Institut für Medizinische Dokumentation und Information (DIMDI): Cologne, Germany, 2005. [Google Scholar]
- Fougeyrollas, P.; Noreau, L.; Boschen, K. Interaction of Environment with Individual Characteristics and Social Participation: Theoretical Perspectives and Applications in Persons with Spinal Cord Injury. Top. Spinal Cord Inj. Rehabil. 2002, 7, 1–16. [Google Scholar] [CrossRef]
- Levasseur, M.; Desrosiers, J.; St-Cyr, T.D. Comparing the Disability Creation Process and International Classification of Functioning, Disability and Health models. Can. J. Occup. Ther. 2007, 74, 233–242. [Google Scholar] [CrossRef]
- Post, M.W.; de Witte, L.P.; Schrijvers, A.J. Quality of life and the ICIDH: Towards an integrated conceptual model for rehabilitation outcomes research. Clin. Rehabil. 1999, 13, 5–15. [Google Scholar] [CrossRef]
- Tomey, K.M.; Sowers, M.R. Assessment of physical functioning: A conceptual model encompassing environmental factors and individual compensation strategies. Phys. Ther. 2009, 89, 705–714. [Google Scholar] [CrossRef] [PubMed]
- Grampp, G. Die ICF Verstehen und Nutzen [Understanding and Using the ICF], 3rd ed.; BALANCE Buch + Medien Verlag: Cologne, Germany, 2019; ISBN 3867391874. [Google Scholar]
- Dijkers, M.P. Issues in the conceptualization and measurement of participation: An overview. Arch. Phys. Med. Rehabil. 2010, 91, S5–S16. [Google Scholar] [CrossRef] [PubMed]
- Hirschberg, M. Klassifizierung von Behinderung [Classification of Disability]. IMEW Konkret. 2009. Available online: https://www.imew.de/de/imew-publikationen/imew-konkret/klassifizierung-von-behinderung (accessed on 26 May 2022).
- Tengland, P.-A. Health promotion or disease prevention: A real difference for public health practice? Health Care Anal. 2010, 18, 203–221. [Google Scholar] [CrossRef]
- Antonovsky, A. The salutogenic model as a theory to guide health promotion. Health Promot. Int. 1996, 11, 11–18. [Google Scholar] [CrossRef]
- Martiny, K.M. How to develop a phenomenological model of disability. Med. Health Care Philos. 2015, 18, 553–565. [Google Scholar] [CrossRef] [PubMed]
- Chapireau, F. The Environment in the International Classification of Functioning, Disability and Health. J. Appl. Res. Intellect. Disabil. 2005, 18, 305–311. [Google Scholar] [CrossRef]
- Weigl, M.; Schwarzkopf, S.R.; Stucki, G. Anwendung der ICF in der rheumatologischen Rehabilitation (Using the ICF in rheumatological rehabilitation). Z. Rheumatol. 2008, 67, 565–574. [Google Scholar] [CrossRef]
- Fougeyrollas, P.; Noreau, L.; Dorweiler, A.; Felden-Özcoban, Ü.; Schlicht, M.; Dahmen, T. Assessment der Lebensgewohnheiten: Kurzversion (3.1) [Assesment of Life Habits—Short Version 3.1. German]; Réseau International sur le Processus de Production du Handicap: Québec City, QC, Canada, 2010; Available online: https://ripph.qc.ca/wp-content/uploads/2018/06/Assessment-der-Lebensgewohnheiten-Kurzversion-3.1-german.pdf (accessed on 26 May 2022).
- Shuttleworth, R.P.; Kasnitz, D. Cultural Context of Disability. In Encyclopedia of Disability; Albrecht, G.L., Ed.; Sage Publications: Thousand Oaks, CA, USA, 2006; pp. 330–337. ISBN 9780761925651. [Google Scholar]
- Pfeiffer, D. The conceptualization of disability. In Exploring Theories and Expanding Methodologies: Where We Are and Where We Need to Go; Barnartt, S.N., Ed.; Emerald Group Publishing Limited: Bingley, UK, 2001; pp. 29–52. ISBN 0-7623-0773-0. [Google Scholar]
- Vehmas, S.; Mäkelä, P. A realist account of the ontology of impairment. J. Med. Ethics 2008, 34, 93–95. [Google Scholar] [CrossRef] [PubMed]
- Wilson, I.B. Linking clinical variables with health-related quality of life. A conceptual model of patient outcomes. JAMA 1995, 273, 59–65. [Google Scholar] [CrossRef]
- Ferrans, C.E.; Zerwic, J.J.; Wilbur, J.E.; Larson, J.L. Conceptual model of health-related quality of life. J. Nurs. Scholarsh. 2005, 37, 336–342. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name (Abbreviation) | Year(s) of Publication |
|---|---|
| Nagi Model | 1965, 1991 |
| International Classification of Impairments, Disabilities, and Handicaps (ICIDH) | 1980 |
| 1st Model of the Institute of Medicine (IOM1) | 1991 |
| 1st Model of the National Center for Medical Rehabilitation Research (NCMRR1) | 1993 |
| Disablement Process | 1994 |
| Name (Abbreviation) | Year(s) of Publication |
|---|---|
| 2nd Model of the Institute of Medicine (IOM2) | 1997 |
| Conceptual Model for Promoting Health (CMPH) | 1997 |
| 2nd Model of the National Center for Medical Rehabilitation Research (NCMRR2) | 2006 |
| Name (Abbreviation) | Year(s) of Publication |
|---|---|
| Integrated Conceptual Model of Rehabilitation Output Research (ICMROR) | 1999 |
| International Classification of Functioning, Disability, and Health (ICF) | 2001 |
| Physical Functioning Assessment in Your Environment (PF-E) | 2009 |
| Disability Creation Process (DCP) | -, 2019 |
| Models/Dimensions | Disease (Biomedical Body) | Illness (Subjective Individual) | Sickness (Society) |
|---|---|---|---|
| Nagi (1965, 1991) [15,44] | active pathology (mc), impairment (mc), functional limitations (mc) | disability (oc) | |
| ICIDH (1980) [49] | disease or disorder (mc), impairment (mc), disability (mc) | handicap (oc) | |
| IOM1 (1991) [32] | pathology (mc), impairment (mc), biological context factors (cf), functional limitation (mc), biomedical context factors (cf) | behavioral and lifestyle-related context factors (cf), quality of life (mc) | disability (oc), physical and social environmental context factors (cf) |
| NCMRR 1 (1993) [50] | pathophysiology (mc), impairment (mc), functional limitation (mc), personal background: organic factors (cf) | personal background: psychosocial factors (cf) | disability (oc), societal limitations (mc), personal background: environmental factors (cf), quality of life (mc) |
| Disablement Process (1994) [26] | pathology (mc), impairment (mc), functional limitations (mc), biological risk factors (cf) | psychological risk factors (cf), intra-individual buffers and exacerbators (cf) | disability (oc), quality of life (oc), environmental risk factors (cf), extra-individual buffers and exacerbators (cf) |
| IOM2 (1997) [52] | pathology (mc), impairment (mc) biological context factors (cf), functional limitation (mc) = body with an impairment, biomedical context factors (cf) | behavioral and lifestyle-related context factors (cf), quality of life (mc) | disability (oc), environment (oc, cf) |
| CMPH (1997) [61] | disablement process: disease or injury, impairment, functional limitation (mc), total environment: biology, life stage (cf, mc) | total environment: lifestyle and behavior (mc, cf), quality of life (oc) | disablement process: activity restriction (mc), opportunity (oc), total environment: physical and social environment (mc, cf) |
| NCMRR2 (2006) [51] | pathophysiology (mc), organ dysfunction (mc), task performance (mc), roles (mc), biomedical influences (cf) | individual influences (cf) | roles (oc), environmental influences (cf) |
| ICMROR (1999) [74] | impairment (mc), disability (mc) | somatic sensation (mc), perceived health (mc), life satisfaction (mc), happiness (oc) | handicap (mc) |
| ICF (2001) [65] | health condition (mc), body functions and structures (mc) | activity (mc), personal context factors (cf) | participation (oc), environmental context factors (cf) |
| PF-E (1999) [75] | capacity (mc) | coping- and compensation strategies (mc) | environmental barriers and facilitators (mc), functioning performance (oc) |
| DCP (-, 2019) [67] | organ systems (mc), capability (mc), biological risk factors (cf) | identity factors (mc), life habits: daily activities (oc), behavioral risk factors (cf) | life habits: social roles (oc), macro-, meso- and microenvironment (mc), environmental risk factors (social and physical) (cf) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forstner, M. Conceptual Models of Disability: The Development of the Consideration of Non-Biomedical Aspects. Disabilities 2022, 2, 540-563. https://doi.org/10.3390/disabilities2030039
Forstner M. Conceptual Models of Disability: The Development of the Consideration of Non-Biomedical Aspects. Disabilities. 2022; 2(3):540-563. https://doi.org/10.3390/disabilities2030039
Chicago/Turabian StyleForstner, Matthias. 2022. "Conceptual Models of Disability: The Development of the Consideration of Non-Biomedical Aspects" Disabilities 2, no. 3: 540-563. https://doi.org/10.3390/disabilities2030039
APA StyleForstner, M. (2022). Conceptual Models of Disability: The Development of the Consideration of Non-Biomedical Aspects. Disabilities, 2(3), 540-563. https://doi.org/10.3390/disabilities2030039