
‘One Step at a Time, One Day at a Time’: Life Profiles of Individuals with Disabilities across the First Year of the COVID-19 Pandemic
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participant Recruitment
2.3. Data Collection
2.4. Data Analysis
3. Results
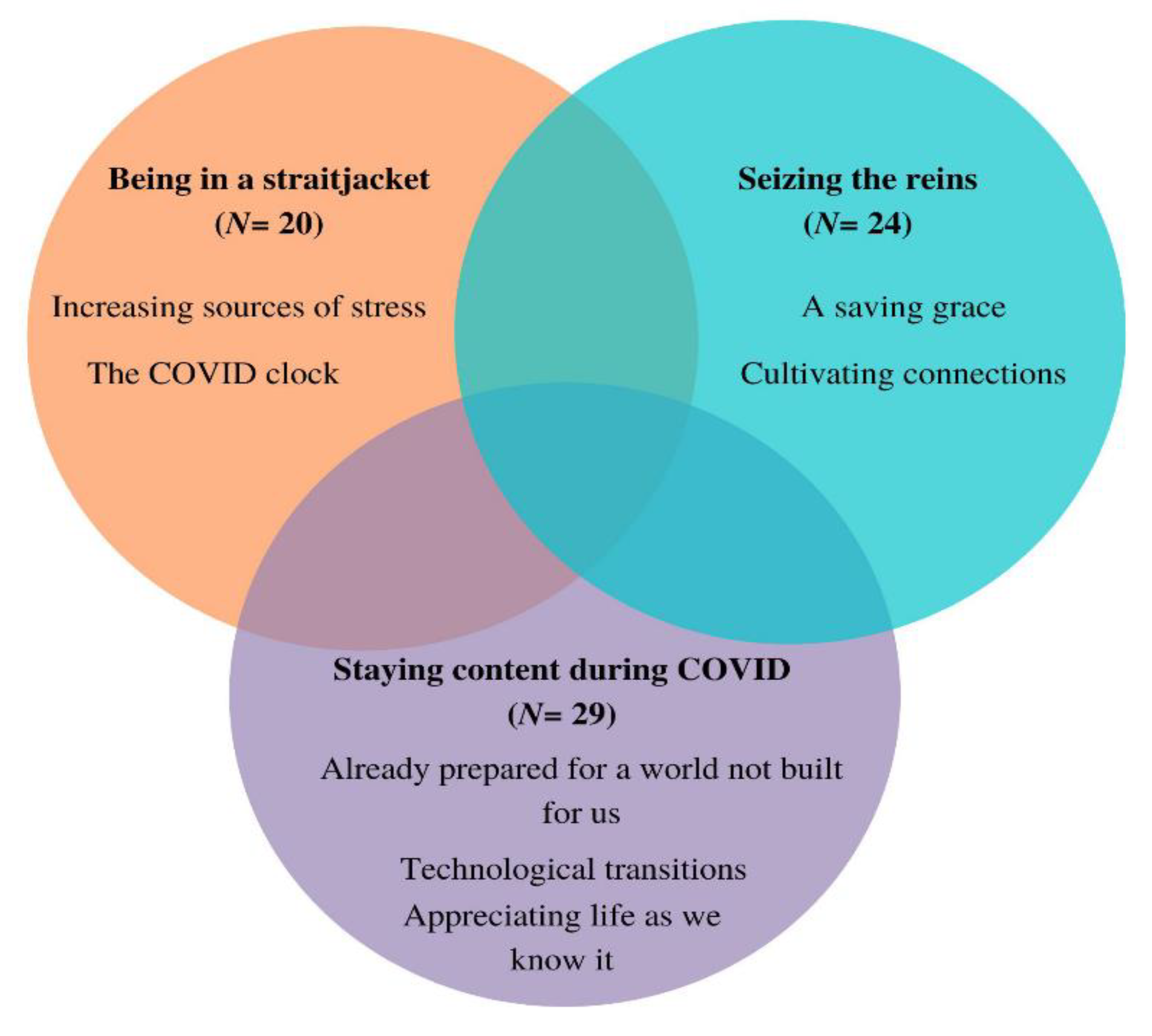
3.1. Being in a Straitjacket
3.1.1. Increasing Sources of Stress
“I kind of already work from home, so I do spend all my week at home anyways and now that the kids are home, I mean, that’s the only thing that’s really changed. So, when I was working at home, that was like my escape. Everybody left the house. I was home alone. And now nobody leaves. So, I’m kind of stuck and I don’t have an escape anymore. Kind of the biggest thing for me.”
“Not only do we touch our wheels, which have touched the ground, but we’re at a lower stature so that somebody who talks to us or sneezes above us, all those droplets will fall on us... I can imagine for those that have caregivers, that would be very challenging to make sure the caregiver is masked up and doing proper sanitation and things like that. There’s a lot of worry, I think as a disabled person.”
3.1.2. The COVID Clock
“… I’m at home everyday, I wake up, I see the [inaudible chatter] Do I want to go today? No. [Laughs]. Yeah, if I were just in school right now, I’d be like, I don’t even want to do school. That’s pretty much it. It’s hard to work from home.“
3.2. Seizing the Reins
3.2.1. A Saving Grace
“It represents sort of immersion, you know, being able to be out of the world as it is…if I let myself get involved in the music and do the work I’m supposed to be doing…all of a sudden it’s time to make supper. You lose track of time… it’s a way of being absorbed in doing something and not just sitting back on the sidelines going, yeah, it’s another day.“
3.2.2. Cultivating Connections
“Maybe it’s my own fault that I don’t have the community that I’d like to have because we’ve all been in lock down. Maybe we’re all feeling this way. Maybe I need to get out there and just ask and instigate, rather than sitting here and not doing anything. Yeah, be the instigator instead of the follower.“
3.3. Staying Content during COVID
3.3.1. Appreciating Life as We Know It
“I’m spending a lot of time with my wife now… we’re both very busy people…[it’s] actually a good thing, where I feel like I have my wife back again. [Laughs.] We’re doing things together... before, we were too busy. But now, suddenly we have time, so it’s been a good change that way.“
3.3.2. Technological Transitions
“... even exhausted as I was, and I was by the end of term, it wasn’t as exhausted by it as I would be if I had been in the past just even TA-ing courses. So, it’s been a really good experience, actually working remotely. And I hope that it continues to be an option.“
3.3.3. Already Prepared for a World Not Built for Us
“I think that overall, with my family, my immediate family, people have taken how I’ve adapted to things and maintained a more or less positive attitude as a good example of how to adapt to this COVID-19 thing, it is what it is, when there’s nothing you can do, you’ve got to just take it in stride.“
“[I have been] rehearsing for such a change in my environment through dealing with my stroke…And I’ve been practicing doing that, so when COVID-19 came along, it’s just using skills that I’ve been learning in the last few years since my strokes. I actually have an advantage over many people who have not had my experience with recovering from a stroke.“
“Some people are at the bottom of the ship and have no access to the lifeboats and some people have a huge cabin and all the luxuries and so, we may be in the same year together but we’re certainly not experiencing it at the [same level], even myself, like I’m on disability but I’ve got family support and I have a lifestyle where I can make it work on the money that I have.“
3.4. Interlinking Life Profiles
4. Discussion
4.1. Being in a Straitjacket
4.2. Seizing the Reins
4.3. Staying Content during COVID
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haug, N.; Geyrhofer, L.; Londei, A.; Dervic, E.; Desvars-Larrive, A.; Loreto, V.; Pinior, B.; Thurner, S.; Klimek, P. Ranking the effectiveness of worldwide COVID-19 government interventions. Nat. Hum. Behav. 2020, 4, 1303–1312. [Google Scholar] [CrossRef] [PubMed]
- Bezyak, J.L.; Sabella, S.; Hammel, J.; McDonald, K.; Jones, R.A.; Barton, D. Community participation and public transportation barriers experienced by people with disabilities. Disabil. Rehabil. 2020, 42, 3275–3283. [Google Scholar] [CrossRef] [PubMed]
- Cochran, A.L. Impacts of COVID-19 on access to transportation for people with disabilities. Transp. Res. Interdiscip. Perspect. 2020, 8, 100263. [Google Scholar] [CrossRef]
- Emerson, E.; Fortune, N.; Llewellyn, G.; Stancliffe, R. Loneliness, social support, social isolation and wellbeing among working age adults with and without disability: Cross-sectional study. Disabil. Health J. 2021, 14, 100965. [Google Scholar] [CrossRef] [PubMed]
- Pettinicchio, D.; Maroto, M.; Chai, L.; Lukk, M. Findings from an online survey on the mental health effects of COVID-19 on Canadians with disabilities and chronic health conditions. Disabil. Health J. 2021, 14, 101085. [Google Scholar] [CrossRef]
- Banks, L.M.; Kuper, H.; Polack, S. Correction: Poverty and disability in low- and middle-income countries: A systematic review. PLoS ONE 2018, 13, e0204881. [Google Scholar] [CrossRef]
- Vu, B.; Khanam, R.; Rahman, M.; Nghiem, S. The costs of disability in Australia: A hybrid panel-data examination. Health Econ. Rev. 2020, 10, 6. [Google Scholar] [CrossRef]
- Lund, E.M.; Forber-Pratt, A.J.; Wilson, C.; Mona, L.R. The COVID-19 pandemic, stress, and trauma in the disability community: A call to action. Rehabil. Psychol. 2020, 65, 313–322. [Google Scholar] [CrossRef]
- Okyere, C.; Fisher, M.H.; Park, J.; Sung, C.; Kammes, R.R. The Impacts and Experiences of COVID-19 on Employment for Individuals with Disabilities. J. Rehabil. 2021, 87, 25–32. [Google Scholar]
- Lee, J.J.; Tsang, W.N.; Yang, S.C.; Kwok, J.Y.Y.; Lou, V.W.; Lau, K.K. Qualitative Study of Chinese Stroke Caregivers’ Caregiving Experience During the COVID-19 Pandemic. Stroke 2021, 52, 1407–1414. [Google Scholar] [CrossRef]
- Czeisler, M.É.; Marynak, K.; Clarke, K.E.N.; Salah, Z.; Shakya, I.; Thierry, J.M.; Ali, N.; McMillan, H.; Wiley, J.F.; Weaver, M.D. Delay or Avoidance of Medical Care Because of COVID-19–Related Concerns—United States, June 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1250–1257. [Google Scholar] [CrossRef]
- Jesus, T.S.; Landry, M.D.; Jacobs, K. A ‘New Normal’ Following COVID-19 and the Economic Crisis: Using Systems Thinking to Identify Challenges and Opportunities in Disability, Telework, and Rehabilitation. Work 2020, 67, 37–46. [Google Scholar] [CrossRef]
- Friedman, C.; VanPuymbrouck, L. Telehealth Use By Persons with Disabilities During the COVID-19 Pandemic. Int. J. Telerehabilitation 2021, 13, e6402. [Google Scholar] [CrossRef]
- Valdez, R.S.; Rogers, C.C.; Claypool, H.; Trieshmann, L.; Frye, O.; Wellbeloved-Stone, C.; Kushalnagar, P. Ensuring full participation of people with disabilities in an era of telehealth. J. Am. Med. Inform. Assoc. 2021, 28, 389–392. [Google Scholar] [CrossRef]
- Elder, G.H.; Johnson, M.K.; Crosnoe, R. The Emergence and Development of Life Course Theory. In Handbook of the Life Course; Motimer, J., Schanahan, M., Eds.; Kluwer/Plenum: New York, NY, USA, 2003; pp. 3–19. [Google Scholar]
- Jones, N.L.; Gilman, S.E.; Cheng, T.L.; Drury, S.S.; Hill, C.V.; Geronimus, A.T. Life Course Approaches to the Causes of Health Disparities. Am. J. Public Health 2019, 109, S48–S55. [Google Scholar] [CrossRef]
- Umucu, E.; Lee, B. Examining the impact of COVID-19 on stress and coping strategies in individuals with disabilities and chronic conditions. Rehabil. Psychol. 2020, 65, 193–198. [Google Scholar] [CrossRef]
- Theis, N.; Campbell, N.; De Leeuw, J.; Owen, M.; Schenke, K.C. The effects of COVID-19 restrictions on physical activity and mental health of children and young adults with physical and/or intellectual disabilities. Disabil. Health J. 2021, 14, 101064. [Google Scholar] [CrossRef]
- Hearn, J.H.; Rohn, E.J.; Monden, K.R. Isolated and anxious: A qualitative exploration of the impact of the COVID-19 pandemic on individuals living with spinal cord injury in the UK. J. Spinal Cord Med. 2021, 45, 691–699. [Google Scholar] [CrossRef]
- Embregts, P.J.C.M.; Bogaard, K.J.H.M.V.D.; Frielink, N.; Voermans, M.A.C.; Thalen, M.; Jahoda, A. A thematic analysis into the experiences of people with a mild intellectual disability during the COVID-19 lockdown period. Int. J. Dev. Disabil. 2022, 68, 578–582. [Google Scholar] [CrossRef]
- Reid, H.; Miller, W.C.; Esfandiari, E.; Mohammadi, S.; Rash, I.; Tao, G.; Simpson, E.; Leong, K.; Matharu, P.; Sakakibara, B. The Impact of COVID-19–Related Restrictions on Social and Daily Activities of Parents, People With Disabilities, and Older Adults: Protocol for a Longitudinal, Mixed Methods Study. JMIR Res. Protoc. 2021, 10, e28337. [Google Scholar] [CrossRef]
- Morrow, S.L. Quality and trustworthiness in qualitative research in counseling psychology. J. Couns. Psychol. 2005, 52, 250–260. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, S.; Mikocka-Walus, A.; Klas, A.; Olive, L.; Sciberras, E.; Karantzas, G.; Westrupp, E.M. From ‘It Has Stopped Our Lives’ to ‘Spending More Time Together Has Strengthened Bonds’’: The Varied Experiences of Australian Families during COVID-19’. Front. Psychol. 2020, 11, 588667. [Google Scholar] [CrossRef] [PubMed]
- Stillman, M.D.; Capron, M.; Alexander, M.; Di Giusto, M.L.; Scivoletto, G. COVID-19 and spinal cord injury and disease: Results of an international survey. Spinal Cord Ser. Cases 2020, 6, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zitek, E.M.; Schlund, R.J. Psychological entitlement predicts noncompliance with the health guidelines of the COVID-19 pandemic. Pers. Individ. Differ. 2021, 171, 110491. [Google Scholar] [CrossRef] [PubMed]
- Droit-Volet, S.; Gil, S.; Martinelli, N.; Andant, N.; Clinchamps, M.; Parreira, L.; Rouffiac, K.; Dambrun, M.; Huguet, P.; Dubuis, B.; et al. Time and Covid-19 stress in the lockdown situation: Time free, «Dying» of boredom and sadness. PLoS ONE 2020, 15, e0236465. [Google Scholar] [CrossRef]
- Droit-Volet, S.; Dambrun, M. Awareness of the Passage of Time and Self-consciousness: What Do Meditators Report? Psych. J. 2019, 8, 51–65. [Google Scholar] [CrossRef] [Green Version]
- Rolland, J.S. COVID-19 Pandemic: Applying a Multisystemic Lens. Fam. Process. 2020, 59, 922–936. [Google Scholar] [CrossRef]
- Kim, J.; Kim, J.; Kim, Y.; Han, A.; Nguyen, M.C. The contribution of physical and social activity participation to social support and happiness among people with physical disabilities. Disabil. Health J. 2021, 14, 100974. [Google Scholar] [CrossRef]
- Nalder, E.; Hartman, L.; Hunt, A.; King, G. Traumatic brain injury resiliency model: A conceptual model to guide rehabilitation research and practice. Disabil. Rehabil. 2019, 41, 2708–2717. [Google Scholar] [CrossRef]
- Runswick-Cole, K.; Goodley, D. Resilience: A Disability Studies and Community Psychology Approach. Soc. Pers. Psychol. Compass 2013, 7, 67–78. [Google Scholar] [CrossRef]
- Oliver, M. Defining Impairment and Disability: Issues at Stake. In Disability and Equality Law; Routledge: London, UK, 2017; pp. 3–18. [Google Scholar]
- Navarro-Carrillo, G.; Alonso-Ferres, M.; Moya, M.; Valor-Segura, I. Socioeconomic Status and Psychological Well-Being: Revisiting the Role of Subjective Socioeconomic Status. Front. Psychol. 2020, 11, 1303. [Google Scholar] [CrossRef]
- Taylor, S.E. Tend and Befriend: Biobehavioral Bases of Affiliation under Stress. Curr. Dir. Psychol. Sci. 2006, 15, 273–277. [Google Scholar] [CrossRef]
- Navas, P.; Amor, A.M.; Crespo, M.; Wolowiec, Z.; Verdugo, M. Supports for people with intellectual and developmental disabilities during the COVID-19 pandemic from their own perspective. Res. Dev. Disabil. 2021, 108, 103813. [Google Scholar] [CrossRef]
- Manzoor, M.; Vimarlund, V. Digital technologies for social inclusion of individuals with disabilities. Health Technol. 2018, 8, 377–390. [Google Scholar] [CrossRef] [Green Version]
- Duplaga, M. Digital divide among people with disabilities: Analysis of data from a nationwide study for determinants of Internet use and activities performed online. PLoS ONE 2017, 12, e0179825. [Google Scholar] [CrossRef] [Green Version]
- Cho, M.; Kim, K.M. Effect of digital divide on people with disabilities during the COVID-19 pandemic. Disabil. Health J. 2022, 15, 101214. [Google Scholar] [CrossRef]
- Buono, V.L.; Corallo, F.; Bramanti, P.; Marino, S. Coping strategies and health-related quality of life after stroke. J. Health Psychol. 2017, 22, 16–28. [Google Scholar] [CrossRef]
- Barclay, L.; Lentin, P.; Bourke-Taylor, H.; McDonald, R. The Experiences of Social and Community Participation of People with Non-traumatic Spinal Cord Injury. Aust. Occup. Ther. J. 2019, 66, 61–67. [Google Scholar] [CrossRef]
- Holm, M.E.; Sainio, P.; Parikka, S.; Koskinen, S. The effects of the COVID-19 pandemic on the psychosocial well-being of people with disabilities. Disabil. Health J. 2021, 15, 101224. [Google Scholar] [CrossRef]


{kind=link}
| Spinal Cord Injury (n = 22) m ± SD/n (%) | Stroke (n = 26) m ± SD/n (%) | Other Disabilities (n = 13) m ± SD/n (%) | |
|---|---|---|---|
| Age | 53.77 ± 11.06 | 65.54 ± 12.68 | 55.76 ± 16.72 |
| Sex: Female | 9 (40.9) | 7 (26.9) | 8 (61.5) |
| Disability Duration: | |||
| Since birth | 2 (9.1) | 0 | 8 (61.5) |
| Since childhood | 1 (4.5) | 0 | 1 (7.7) |
| Since adolescence | 4 (18.1) | 0 | 1 (7.7) |
| Since adulthood | 6 (27.3) | 2 (7.7) | 1 (7.7) |
| Later in life | 9 (40.9) | 12 (46.2) | 2 (15.4) |
| Employment: | |||
| Full-time | 3 (13.6) | 1 (3.8) | 1 (7.7) |
| Part-time | 3 (13.6) | 2 (7.7) | 1 (7.7) |
| Unemployed | 1 (4.5) | 2 (7.7) | 0 (0) |
| Student | 0 (0) | 1 (3.8) | 1 (7.7) |
| Retired | 5 (22.7) | 15 (57.7) | 4 (30.8) |
| Disability assistance | 7 (31.8) | 2 (7.7) | 4 (30.8) |
| Homemaker | 0 (0) | 1 (3.8) | 0 (0) |
| Other | 3 (13.6) | 2 (7.7) | 2 (15.4) |
| Living environment: | |||
| Alone/Independent | 7 (31.8) | 7 (26.9) | 9 (69.2) |
| Assisted living | 1 (4.5) | 1 (3.8) | 0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mamman, R.; Mohammadi, S.; Rash, I.; Esfandiari, E.; Miller, W.C.; Mortenson, W.B.; Schmidt, J. ‘One Step at a Time, One Day at a Time’: Life Profiles of Individuals with Disabilities across the First Year of the COVID-19 Pandemic. Disabilities 2022, 2, 736-749. https://doi.org/10.3390/disabilities2040051
Mamman R, Mohammadi S, Rash I, Esfandiari E, Miller WC, Mortenson WB, Schmidt J. ‘One Step at a Time, One Day at a Time’: Life Profiles of Individuals with Disabilities across the First Year of the COVID-19 Pandemic. Disabilities. 2022; 2(4):736-749. https://doi.org/10.3390/disabilities2040051
Chicago/Turabian StyleMamman, Rinni, Somayyeh Mohammadi, Isabelle Rash, Elham Esfandiari, William C. Miller, William Ben Mortenson, and Julia Schmidt. 2022. "‘One Step at a Time, One Day at a Time’: Life Profiles of Individuals with Disabilities across the First Year of the COVID-19 Pandemic" Disabilities 2, no. 4: 736-749. https://doi.org/10.3390/disabilities2040051