Relative Safety Assessment for Positioning Children in Vehicles with Varying Levels of Advanced Safety Technologies

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
- Children (0 if the person involved in the crash was older than 12 years, 1 otherwise);
- Restrained (0 if the person involved in the crash was not restrained, 1 otherwise);
- Latest vehicles (0 if the vehicle involved in the crash was older than model year (MY) 2000, 1 otherwise).
3. Results
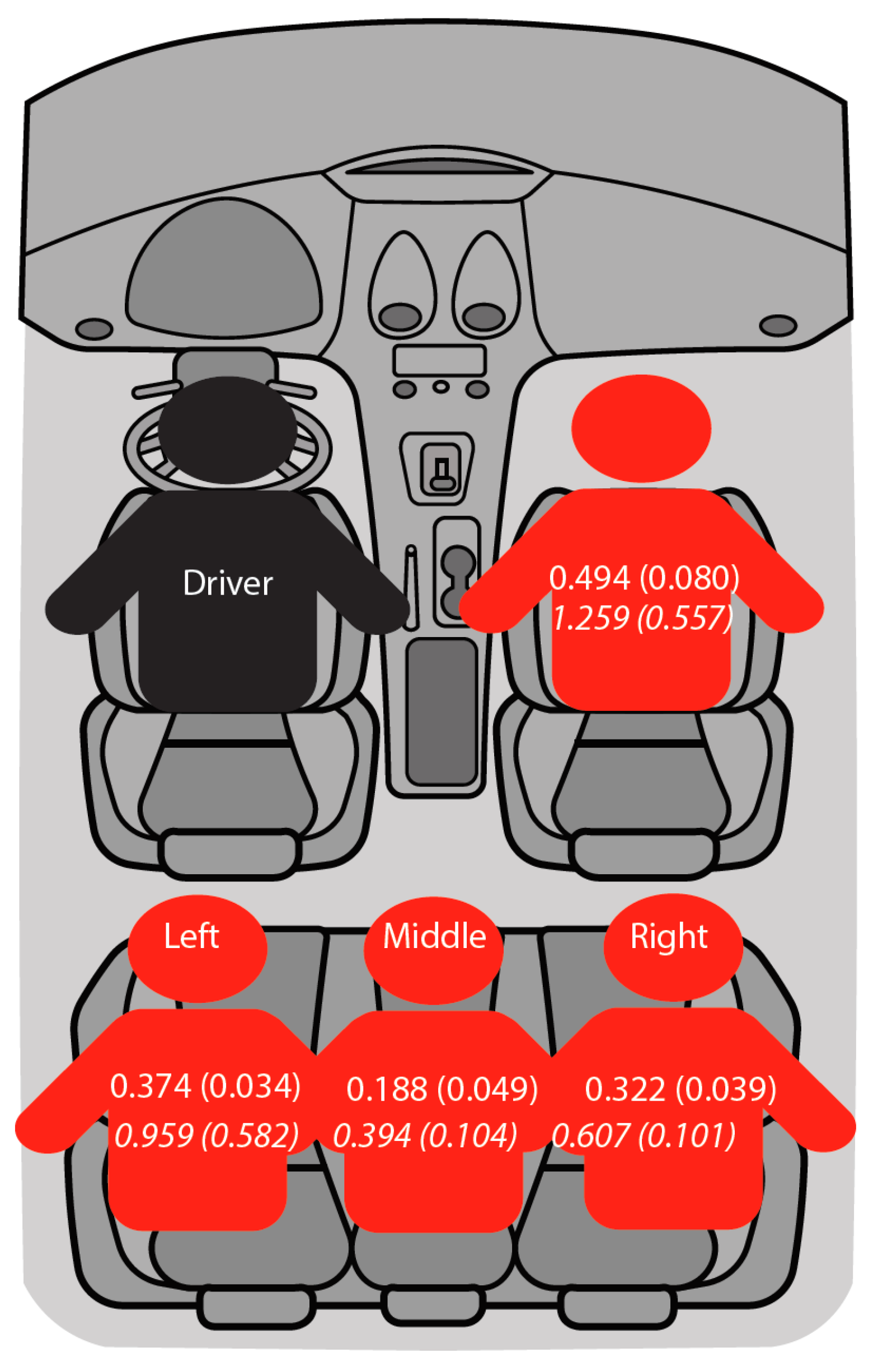
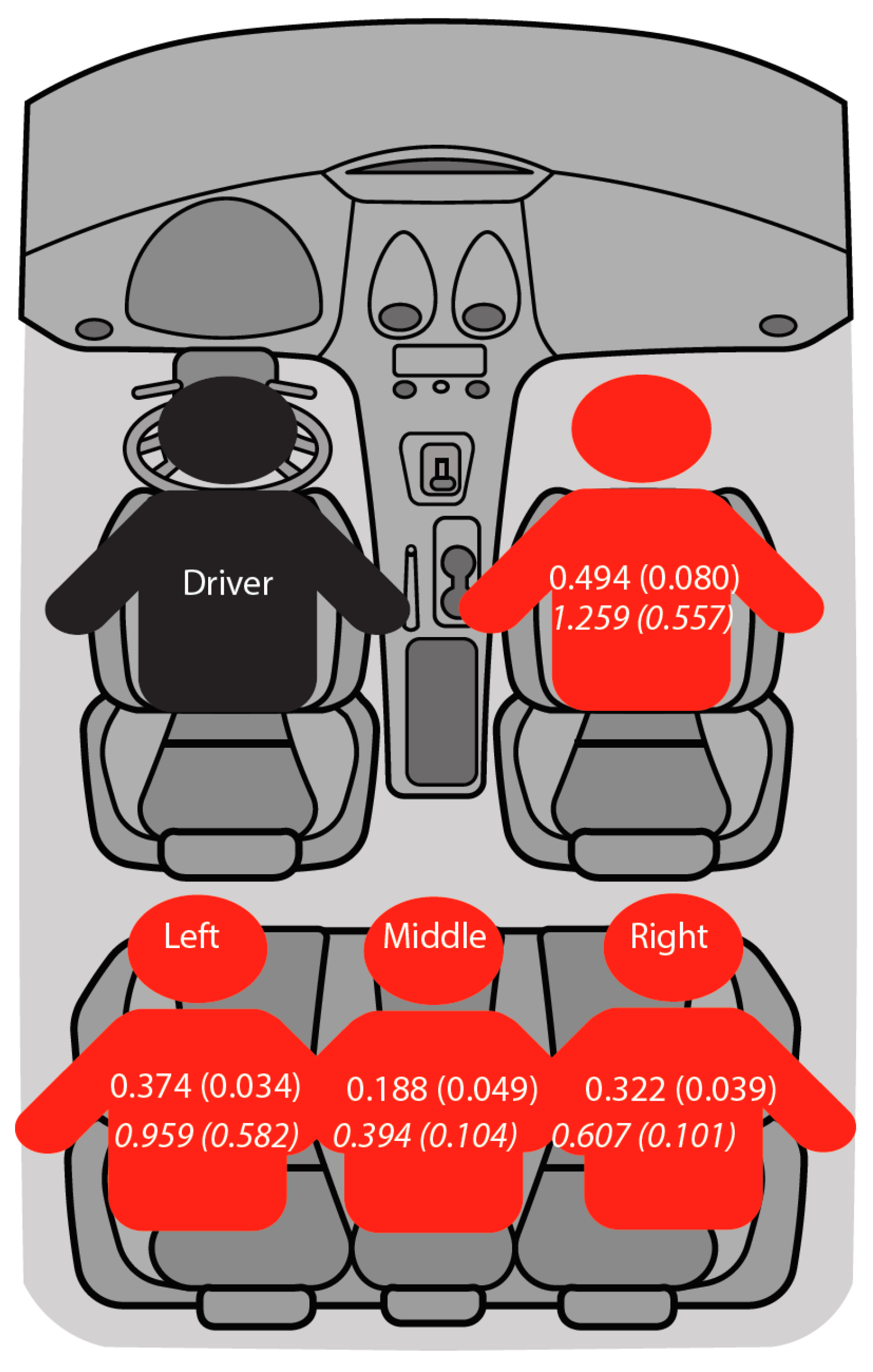
3.1. Safest Seat for Children in the Current Vehicle Fleet
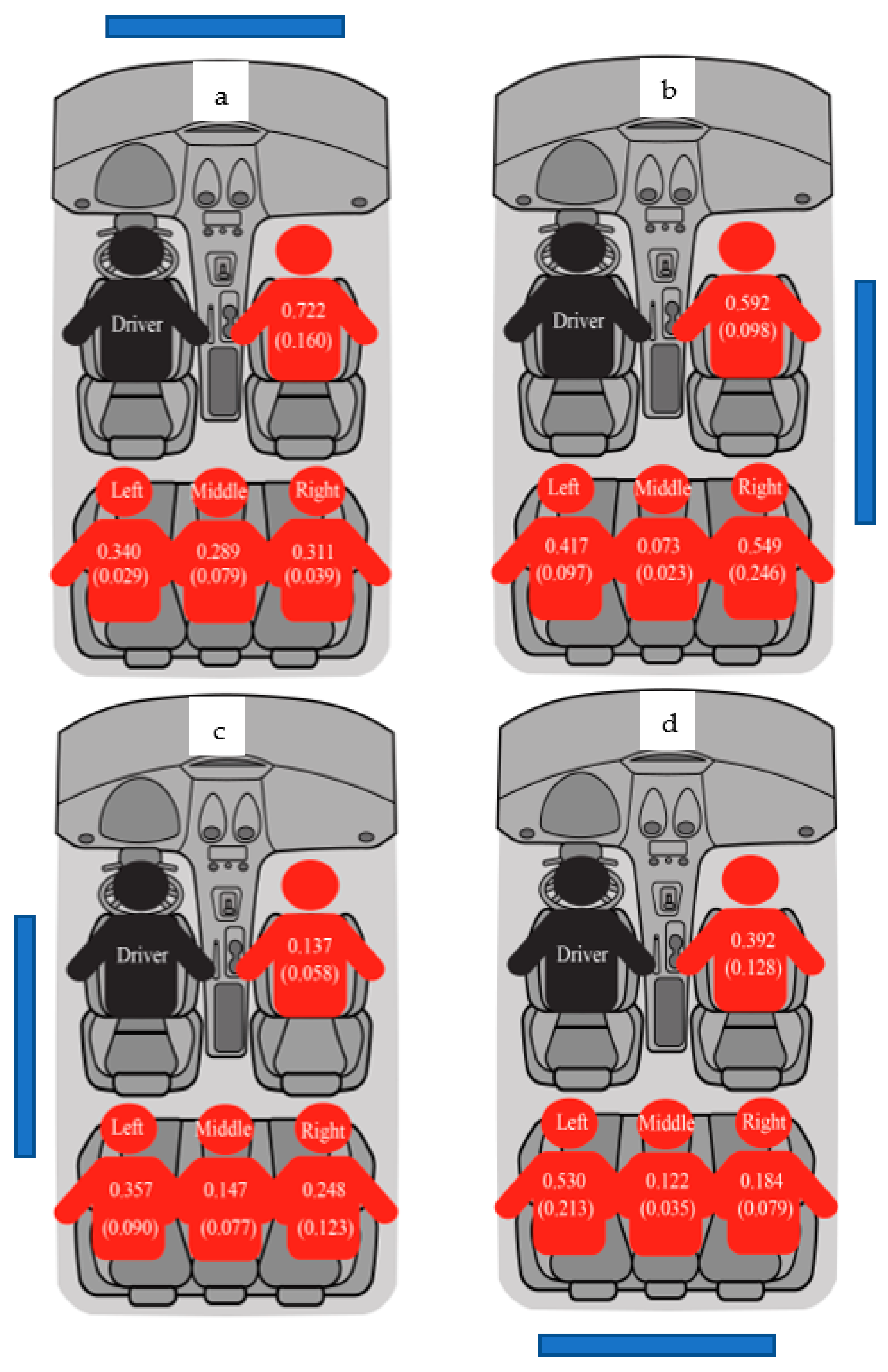
3.2. Safest Seat for Children in Tomorrow’s Cars
4. Discussion
- as advanced vehicle technologies have recently seen wider adoption, relatively fewer vehicles on roads are equipped with these technologies;
- as the crash rate is lower for vehicles equipped with advanced vehicle technologies, they will not appear in the crash data as frequently as traditional vehicles;
- publicly available crash data do not have information on the presence and activation of these systems in vehicles involved in crashes.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Child Passenger Safety: Get the Facts. Available online: https://www.cdc.gov/transportationsafety/child_passenger_safety/cps-factsheet.html (accessed on 28 February 2023).
- Durbin, D.R. Child passenger safety. Pediatrics 2011, 127, 1050–1066. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Frick, M.C. Seating position in cars and fatality risk. Am. J. Public Health 1988, 78, 1456–1458. [Google Scholar] [CrossRef] [PubMed]
- Agran, P.; Castillo, D.; Winn, D. Comparison of motor vehicle occupant injuries in restrained and unrestrained 4–14 year olds. Accid. Anal. Prev. 1992, 24, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Huelke, D.F.; Compton, C.P. The effects of seat belts on injury severity of front and rear-seat occupants in the same frontal crash. Accid. Anal. Prev. 1995, 27, 835–838. [Google Scholar] [CrossRef] [PubMed]
- Braver, E.R.; Whitfield, R.; Ferguson, S.A. Seating positions and children’s risk of dying in motor vehicle crashes. Inj. Prev. 1998, 4, 181–187. [Google Scholar] [CrossRef]
- Durbin, D.R.; Chen, I.; Smith, R.; Elliott, M.R.; Winston, F.K. Effects of Seating Position and Appropriate Restraint Use on the Risk of Injury to Children in Motor Vehicle Crashes. Pediatrics 2005, 115, e305–e309. [Google Scholar] [CrossRef]
- Glass, R.J.; Segui-Gomez, M.; Graham, J.D. Child passenger safety: Decisions about seating location, airbag exposure, and restraint use. Risk Anal. 2000, 20, 521–528. [Google Scholar] [CrossRef]
- Smith, K.M.; Cummings, P. Passenger seating position and the risk of passenger death or injury in traffic crashes. Accid. Anal. Prev. 2004, 36, 257–260. [Google Scholar] [CrossRef]
- Lennon, A.; Siskind, V.; Haworth, N. Rear seat safer: Seating position, restraint use and injuries in children in traffic crashes in Victoria, Australia. Accid. Anal. Prev. 2008, 40, 829–834. [Google Scholar] [CrossRef]
- Durbin, D.R.; Jermakian, J.S.; Kallan, M.J.; McCartt, A.T.; Arbogast, K.B.; Zonfrillo, M.R.; Myers, R.K. Rear seat safety: Variation in protection by occupant, crash and vehicle characteristics. Accid. Anal. Prev. 2015, 80, 185–192. [Google Scholar] [CrossRef]
- Mayrose, J.; Priya, A. The safest seat: Effect of seating position on occupant mortality. J. Saf. Res. 2008, 39, 433–436. [Google Scholar] [CrossRef] [PubMed]
- Kallan, M.J.; Durbin, D.R.; Arbogast, K.B. Seating patterns and corresponding risk of injury among 0- to 3-year-old children in child safety seats. Pediatrics 2008, 121, 1342–1347. [Google Scholar] [CrossRef] [PubMed]
- Bliston, L.E.; Du, W.; Brown, J. A matched-cohort analysis of belted front and rear-seat occupants in newer and older model vehicles shows that gains in front occupant safety have outpaced gains for rear-seat occupants. Accid. Anal. Prev. 2010, 42, 1974–1977. [Google Scholar] [CrossRef] [PubMed]
- Esfahani, E.S.; Digges, K. Trend of rear occupant protection in frontal crashes over model years of vehicles. SAE Tech. Pap. 2009, 1–8. [Google Scholar] [CrossRef]
- Sahraei, E.; Digges, K.; Marzougui, D. Reduced protection for belted occupants in rear-seats relative to front-seats of new model year vehicles. Ann. Adv. Automot. Med. 2010, 54, 149. [Google Scholar]
- Sahraei, E.; Soudbakhsh, D.; Digges, K. Protection of rear-seat occupants in frontal crashes, controlling for occupant and crash characteristics. SAE Tech. Pap. 2009, 53, 75–91. [Google Scholar]
- Tatem, W.M.; Gabler, H.C. Differential fatality risk between rear and front-seat passenger vehicle occupants in frontal crashes. In Proceedings of the 2019 International IRCOBI Conference on the Biomechanics of Injury, Florence, Italy, 11–13 September 2019. [Google Scholar]
- Atkinson, T.; Gawarecki, L.; Tavakoli, M. Paired vehicle occupant analysis indicates age and crash severity moderate likelihood of higher severity injury in second row seated adults in frontal crashes. Accid. Anal. Prev. 2016, 89, 88–94. [Google Scholar] [CrossRef]
- Mitchell, R.J.; Bambach, M.R.; Toson, B. Injury risk for matched front and rear-seat car passengers by injury severity and crash type: An exploratory study. Accid. Anal. Prev. 2015, 82, 171–179. [Google Scholar] [CrossRef]
- NHTSA Announces Update to Historic AEB Commitment by 20 Automakers. Available online: https://www.nhtsa.gov/press-releases/nhtsa-announces-update-historic-aeb-commitment-20-automakers (accessed on 28 February 2023).
- Driver Assistance Technologies. Available online: https://www.nhtsa.gov/equipment/driver-assistance-technologies#61996 (accessed on 28 February 2023).
- National Automotive Sampling System. Available online: https://www.nhtsa.gov/crash-data-systems/national-automotive-sampling-system (accessed on 28 February 2023).
- SAS Institute Inc. SAS/STAT® 14.2 User’s Guide: The SURVEYMEANS Procedure; SAS: Cary, NC, USA, 2016. [Google Scholar]
- Injury Severity Score. Available online: https://aci.health.nsw.gov.au/get-involved/institute-of-trauma-and-injury-management/data/injury-scoring/abbreviated_injury_scale (accessed on 28 February 2023).
- Advanced Driver Assistance Technology Names. Available online: https://www.aaa.com/AAA/common/AAR/files/ADAS-Technology-Names-Research-Report.pdf (accessed on 28 February 2023).
- Cicchino, J.B. Effectiveness of forward collision warning and autonomous emergency braking systems in reducing front-to-rear crash rates. Accid. Anal. Prev. 2017, 99, 142–152. [Google Scholar] [CrossRef]
- Cicchino, J.B. Effects of blind spot monitoring systems on police-reported lane-change crashes. Traffic Inj. Prev. 2018, 19, 615–622. [Google Scholar] [CrossRef]
- Sternlund, S.; Strandroth, J.; Rizzi, M.; Lie, A.; Tingvall, C. The effectiveness of lane departure warning systems—A reduction in real-world passenger car injury crashes. Traffic Inj. Prev. 2017, 18, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Cicchino, J.B. Effects of lane departure warning on police-reported crash rates. J. Saf. Res. 2018, 66, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Teoh, E.R. Effectiveness of Front Crash Prevention Systems in Reducing Large Truck Crash Rates. Traffic Inj. Prev. 2021, 22, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Quinones-Hinojosa, A.; Jun, P.; Manley, G.T.; Knudson, M.M.; Gupta, N. Airbag deployment and improperly restrained children: A lethal combination. J. Trauma Acute Care Surg. 2005, 59, 729–733. [Google Scholar]
- Braver, E.R.; Ferguson, S.A.; Greene, M.A.; Lund, A.K. Reductions in deaths in frontal crashes among right front passengers in vehicles equipped with passenger air bags. JAMA 1997, 278, 1437–1439. [Google Scholar] [CrossRef]
- Haboucha, C.J.; Ishaq, R.; Shiftan, Y. User preferences regarding autonomous vehicles. Transp. Res. Part C Emerg. Technol. 2017, 78, 37–49. [Google Scholar] [CrossRef]
- Lee, Y.C.; Mirman, J.H. Parents’ perspectives on using autonomous vehicles to enhance children’s mobility. Transp. Res. Part C Emerg. Technol. 2018, 96, 415–431. [Google Scholar] [CrossRef]
- Tremoulet, P.D.; Seacrist, T.; Ward McIntosh, C.; Loeb, H.; DiPietro, A.; Tushak, S. Transporting children in autonomous vehicles: An exploratory study. Hum. Factors 2020, 62, 278–287. [Google Scholar] [CrossRef]
- Greenwell, N.K. Results of the National Child Restraint Use Special Study. No. DOT HS 812 142. 2015. Available online: https://trid.trb.org/view/1361381 (accessed on 7 May 2023).
- Traffic Safety Facts, 2017 Data. Available online: https://crashstats.nhtsa.dot.gov/Api/Public/ViewPublication/812719 (accessed on 28 February 2023).
- Tessier, K. Effectiveness of hands-on education for correct child restraint use by parents. Accid. Anal. Prev. 2010, 42, 1041–1047. [Google Scholar] [CrossRef]
- Penmetsa, P.; Wang, T.; Nambisan, S. An Assessment of Child Restraint System Misuse in the United States. In Proceedings of the Transportation Research Board 97th Annual Meeting, Washington, DC, USA, 7–11 January 2018. [Google Scholar]
- Zhai, G.; Yang, H.; Liu, J. Is the front passenger seat always the “death seat”? An application of a hierarchical ordered probit model for occupant injury severity. Int. J. Inj. Control Saf. Promot. 2020, 27, 438–446. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | Weighted Frequency (%) | Unweighted Frequency (%) |
|---|---|---|
| Child | ||
| No | 82,190 (92.72) | 35,156,169 (93.02) |
| Yes | 6449 (7.28) | 2,636,136 (6.98) |
| Restraint use for children | ||
| No | 2881 (44.67) | 1,171,736 (44.45) |
| Yes | 3568 (55.33) | 1,464,400 (55.55) |
| Seat position of children | ||
| Front right | 698 (10.82) | 296,054 (11.23) |
| Second-row left seat | 1646 (25.52) | 656,056 (24.89) |
| Second-row middle seat | 835 (12.95) | 332,107 (12.60) |
| Second-row right seat | 1929 (29.91) | 858,261 (32.56) |
| Third-row left seat | 146 (2.26) | 73,288 (2.78) |
| Third-row middle seat | 67 (1.04) | 24,389 (0.93) |
| Third-row right seat | 151 (2.34) | 61,659 (2.34) |
| Greatest area of damage for vehicle with children | ||
| Back | 444 (6.88) | 205,895 (7.81) |
| Front | 2821 (43.74) | 1,148,710 (43.58) |
| Left | 825 (12.79 | 317,571 (12.05) |
| Right | 674 (10.45) | 258,809 (9.82) |
| Top | 306 (4.74) | 54,233 (2.06) |
| Under | 13 (0.20) | 7695 (0.29) |
| Maximum Abbreviated Injury Scale (MAIS) for children | ||
| Not injured | 2855 (44.27) | 1,418,301 (53.80) |
| Minor | 1389 (21.54) | 379,431 (14.39) |
| Moderate | 179 (2.78) | 24,526 (0.93) |
| Serious | 97 (1.50) | 10,240 (0.39) |
| Severe | 46 (0.71) | 3873 (0.15) |
| Critical | 31 (0.48) | 3729 (0.14) |
| Maximum (untreatable) | 16 (0.25) | 905 (0.03) |
| Seat Position | Mean ISS | Std. Error | Difference in Mean ISS | p-Value |
|---|---|---|---|---|
| Front right | ||||
| Older (2000 and before) | 1.233 | 0.376 | 0.74 | 0.047 * |
| Newer (2000 and after) | 0.494 | 0.08 | ||
| Second-row left seat | ||||
| Older | 0.447 | 0.125 | 0.074 | 0.582 |
| Newer | 0.374 | 0.034 | ||
| Second-row middle seat | ||||
| Older | 0.824 | 0.432 | 0.636 | 0.19 |
| Newer | 0.188 | 0.05 | ||
| Second-row right seat | ||||
| Older | 0.403 | 0.122 | 0.082 | 0.587 |
| Newer | 0.322 | 0.039 | ||
| Collision Alert | Collision Mitigation |
|---|---|
| Forward collision warning (FCW) | Forward automatic emergency braking (FAEB) |
| Lane departure warning (LDW) | Reverse automatic emergency braking (RAEB) |
| Blind spot warning (BSW) | Automatic emergency braking (AEB) |
| Rear cross-traffic warning (RCTW) | |
| Parking obstruction warning (POW) | |
| Pedestrian detection |
| Point of Impact | Frequency | Probabilities |
|---|---|---|
| Front | 5,655,758 | 0.50 |
| Back | 2,978,093 | 0.26 |
| Left | 1,091,709 | 0.09 |
| Right | 389,597 | 0.10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Penmetsa, P.; Adanu, E.K.; Lidbe, A.; Li, X.; Nambisan, S.; Jones, S.L. Relative Safety Assessment for Positioning Children in Vehicles with Varying Levels of Advanced Safety Technologies. Future Transp. 2023, 3, 615-625. https://doi.org/10.3390/futuretransp3020036
Penmetsa P, Adanu EK, Lidbe A, Li X, Nambisan S, Jones SL. Relative Safety Assessment for Positioning Children in Vehicles with Varying Levels of Advanced Safety Technologies. Future Transportation. 2023; 3(2):615-625. https://doi.org/10.3390/futuretransp3020036
Chicago/Turabian StylePenmetsa, Praveena, Emmanuel K. Adanu, Abhay Lidbe, Xiaobing Li, Shashi Nambisan, and Steven L. Jones. 2023. "Relative Safety Assessment for Positioning Children in Vehicles with Varying Levels of Advanced Safety Technologies" Future Transportation 3, no. 2: 615-625. https://doi.org/10.3390/futuretransp3020036
APA StylePenmetsa, P., Adanu, E. K., Lidbe, A., Li, X., Nambisan, S., & Jones, S. L. (2023). Relative Safety Assessment for Positioning Children in Vehicles with Varying Levels of Advanced Safety Technologies. Future Transportation, 3(2), 615-625. https://doi.org/10.3390/futuretransp3020036