
The Role of Language Barriers on Hospital Outcomes in Culturally and Linguistically Diverse Patients following Trauma Admission


Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Literature Screening
2.4. Data Extraction and Synthesis
2.5. Quality and Risk of Bias Assessment
3. Results
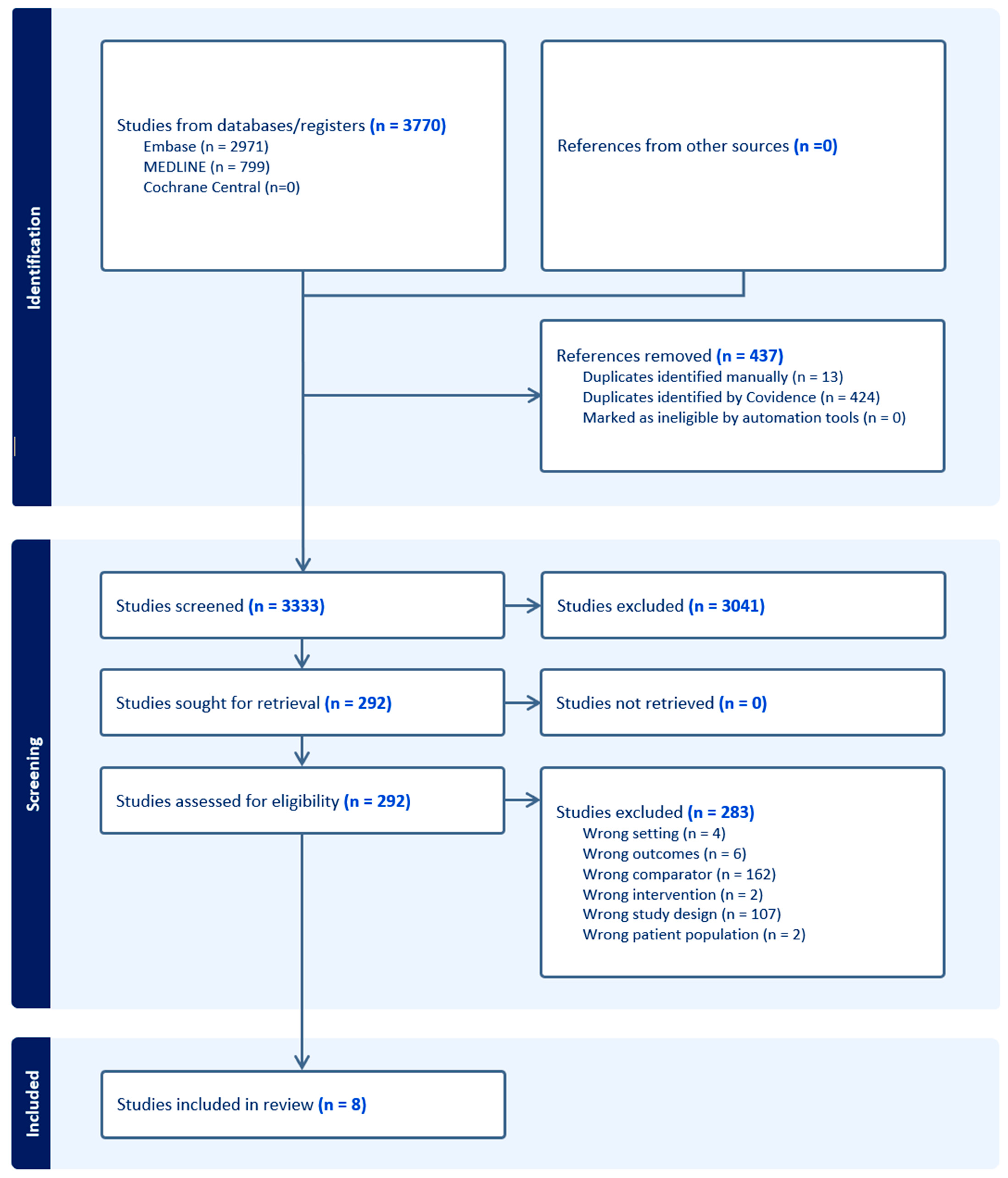
3.1. Literature Search Results
3.2. Overview of Studies
3.3. Comparison of Injury Severity
3.4. Discrepancy in Outcomes of Inpatient Care
3.5. Discrepancy in Functional Outcomes upon Follow-Up Evaluation
3.6. Communication Barriers
3.7. Risk of Bias
4. Discussion
4.1. Limitations
4.2. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Literature Search
- “Wounds and Injuries”/or accidental injuries/or exp amputation, traumatic/or exp multiple trauma/or BrainInjuries, Traumatic/or Brain Injuries/or exp Wounds, Nonpenetrating/or exp Wounds, Penetrating/or Trauma Centers/
- ((trauma* adj3 (injur* or admission* or surger*)) or trauma care or ((major or multiple or serious) adj trauma*)).tw,kf.
- 1 or 2
- Racial Groups/or Ethnicity/or Cross-Cultural Comparison/or Cultural Diversity/
- exp black people/or “black or african american”/or “native hawaiian or other pacific islander”/or “australianaboriginal and torres strait islander peoples”/
- ((cultur* or linguistic* or ethnic* or race or racial or socioethnic* or multicultural) adj2 (divers* or minorit*or group* or population* or background* or difference* or disparit* or variation*)).tw,kf.
- (((indigenous or aboriginal or first nation*) adj3 Australia*) or (Torres Strait Islander* or Maori)).tw.
- 4 or 5 or 6 or 7
- Disability Evaluation/or Outcome Assessment, Health Care/or Survival Rate/or Treatment Outcome/or Recovery ofFunction/or “Patient Discharge”/or exp postoperative complications/
- Stress Disorders, Post-Traumatic/or Depression/or Anxiety Disorders/or Anxiety/
- exp morbidity/or mortality/or hospital mortality/or survival rate/
- (outcome* or survival* or disabilit* or mortality or morbidity).ti,kf.
- (postoperative complication* or post-operative complication*).tw,kf.
- (((posttraumatic or post-traumatic) adj (stress or symptom*)) or anxiety or depression or mental health).ti,kf.
- 9 or 10 or 11 or 12 or 13 or 14)
- 3 and 8 and 15
- ((exp child/or adolescent/) not adult/) or (p?ediatric or child* or infan* or juvenile or adolescen* or teen*).ti.
- 16 not 17
References
- Lord, J.M.; Midwinter, M.J.; Chen, Y.-F.; Belli, A.; Brohi, K.; Kovacs, E.J.; Koenderman, L.; Kubes, P.; Lilford, R.J. The systemic immune response to trauma: An overview of pathophysiology and treatment. Lancet 2014, 384, 1455–1465. [Google Scholar] [CrossRef] [PubMed]
- Osuka, A.; Ogura, H.; Ueyama, M.; Shimazu, T.; Lederer, J.A. Immune response to traumatic injury: Harmony and discordance of immune system homeostasis. Acute Med. Surg. 2014, 1, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Gando, S.; Otomo, Y. Local hemostasis, immunothrombosis, and systemic disseminated intravascular coagulation in trauma and traumatic shock. Crit. Care 2015, 19, 72. [Google Scholar] [CrossRef] [PubMed]
- Arango-Lasprilla, J.C.; Rosenthal, M.; Deluca, J.; Komaroff, E.; Sherer, M.; Cifu, D.; Hanks, R. Traumatic brain injury and functional outcomes: Does minority status matter? Brain Inj. 2007, 21, 701–708. [Google Scholar] [CrossRef] [PubMed]
- Arango-Lasprilla, J.C.; Kreutzer, J.S. Racial and ethnic disparities in functional, psychosocial, and neurobehavioral outcomes after brain injury. J. Head Trauma Rehabil. 2010, 25, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Perrin, P.B.; Krch, D.; Sutter, M.; Snipes, D.J.; Arango-Lasprilla, J.C.; Kolakowsky-Hayner, S.A.; Wright, J.; Lequerica, A. Racial/ethnic disparities in mental health over the first 2 years after traumatic brain injury: A model systems study. Arch. Phys. Med. Rehabil. 2014, 95, 2288–2295. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Cultural Diversity in Australia, 2016; Australian Bureau of Statistics: Canberra, Australia, 2017.
- Clark, A.; Gilbert, A.; Rao, D.; Kerr, L. ‘Excuse me, do any of you ladies speak English?’ Perspectives of refugee women living in South Australia: Barriers to accessing primary health care and achieving the Quality Use of Medicines. Aust. J. Prim. Health 2014, 20, 92–97. [Google Scholar] [PubMed]
- Hadgkiss, E.J.; Renzaho, A.M. The physical health status, service utilisation and barriers to accessing care for asylum seekers residing in the community: A systematic review of the literature. Aust. Health Rev. 2014, 38, 142–159. [Google Scholar] [CrossRef] [PubMed]
- Hannah, C.T.; Le, Q. Factors affecting access to healthcare services by intermarried Filipino women in rural Tasmania: A qualitative study. Rural Remote Health 2012, 12, 1–9. [Google Scholar] [CrossRef]
- Taylor, J.; Haintz, G.L. Influence of the social determinants of health on access to healthcare services among refugees in Australia. Aust. J. Prim. Health 2018, 24, 14–28. [Google Scholar] [CrossRef]
- Mead, N.; Roland, M. Understanding why some ethnic minority patients evaluate medical care more negatively than white patients: A cross sectional analysis of a routine patient survey in English general practices. Bmj 2009, 339, b3450. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, L.M.; Jacquez, F.; Bakar, R.C. Cultural health attributions, beliefs, and practices: Effects on healthcare and medical education. Open Med. Educ. J. 2009, 2, 64–74. [Google Scholar]
- Ponsford, J.; Downing, M.; Pechlivanidis, H. The impact of cultural background on outcome following traumatic brain injury. Neuropsychol. Rehabil. 2020, 30, 85–100. [Google Scholar] [CrossRef] [PubMed]
- Saltapidas, H.; Ponsford, J. The influence of cultural background on motivation for and participation in rehabilitation and outcome following traumatic brain injury. J. Head Trauma Rehabil. 2007, 22, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Saltapidas, H.; Ponsford, J. The influence of cultural background on experiences and beliefs about traumatic brain injury and their association with outcome. Brain Impair. 2008, 9, 1–13. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2000. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 19 December 2023).
- Costello, R.S.; Downing, M.G.; Ponsford, J. The experience of traumatic brain injury in a culturally and linguistically diverse sample in Australia. Disabil. Rehabil. 2023, 1–10. [Google Scholar] [CrossRef]
- Garduño-Ortega, O.; Li, H.; Smith, M.; Yao, L.; Wilson, J.; Zarate, A.; Bushnik, T. Assessment of the individual and compounding effects of marginalization factors on injury severity, discharge location, recovery, and employment outcomes at 1 year after traumatic brain injury. Front. Neurol. 2022, 13, 942001. [Google Scholar] [CrossRef]
- Hines, A.L.; Andrews, R.M.; Moy, E.; Barrett, M.L.; Coffey, R.M. Disparities in rates of inpatient mortality and adverse events: Race/ethnicity and language as independent contributors. Int. J. Environ. Res. Public Health 2014, 11, 13017–13034. [Google Scholar] [CrossRef]
- de la Plata, C.M.; Hewlitt, M.; de Oliveira, A.; Hudak, A.; Harper, C.; Shafi, S.; Diaz-Arrastia, R. Ethnic differences in rehabilitation placement and outcome after TBI. J. Head Trauma Rehabil. 2007, 22, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.; Zeidan, A.; Beshara, G.; Cortes, J.; Tibbetts, C.; Tracy, B.M.; Muralidharan, V.J.; Sola Jr, R.; Irizarry, R.H.; Williams, K. Characterizing injury patterns and outcomes in hospitalized trauma patients with non-English Language Preferences. Am. J. Surg. 2023, 225, 948–952. [Google Scholar] [CrossRef] [PubMed]
- Sander, A.M.; Ketchum, J.M.; Lequerica, A.H.; Pappadis, M.R.; Bushnik, T.; Hammond, F.M.; Sevigny, M. Primary language and participation outcomes in hispanics with traumatic brain injury: A traumatic brain injury model systems study. J. Head Trauma Rehabil. 2021, 36, E218. [Google Scholar] [CrossRef] [PubMed]
- Kinney, A.R.; Bahrani, N.H.; Brenner, L.A.; Starosta, A.J.; Mata-Greve, F.; Humbert, A.; Zheng, Z.; Prado, M.G.; Au, M.A.; Mollis, B. Intersectionality of systemic disadvantage on mortality and care following TBI. J. Head Trauma Rehabil. 2023, 38, 137–146. [Google Scholar]
- Kellezi, B.; Earthy, S.; Sleney, J.; Beckett, K.; Barnes, J.; Christie, N.; Horsley, D.; Jones, T.; Kendrick, D. What can trauma patients’ experiences and perspectives tell us about the perceived quality of trauma care? A qualitative study set within the UK National Health Service. Injury 2020, 51, 1231–1237. [Google Scholar]
- Miner, A.S.; Shah, N.; Bullock, K.D.; Bailenson, J. Key considerations for incorporating conversational AI in psychotherapy. Front. Psychiatry 2019, 10, 441761. [Google Scholar] [CrossRef]


{kind=link}
| Author | Year | Country of Publication | Study Design | Age | Sex | Total Patients | Injury Severity Scale | English and Non-English Speakers | Percentage of Non-English Speakers | Languages |
|---|---|---|---|---|---|---|---|---|---|---|
| Costello et al. [20] | 2023 | Australia | Reflexive thematic analysis | English proficient: 41, CALD: 35.57 | 10M (4 English proficient; 6 CALD), 5F (4 English proficient, 1 CALD) | 15 | Qualitative (all severe, except 1 moderate—CALD) | English proficient (n = 8), CALD (n = 7) | 46.67% | Punjabi (6.67%), Hindi (6.67%), Italian (6.67%), Turkish (6.67%), Mandarin (6.67%), Urdu (6.67%), Nepali (6.67%) |
| Garduno-Ortega et al. [21] | 2022 | USA | Retrospective cohort study | Total: 42.11 (±14.01) English proficient: not stated CALD: 42.85 (±14.03) | English proficient: not stated CALD: M: 85 F: 11 | 249 | Odds (SD) 1.58 (1.32) (unadjusted) 1.75 (1.35) (adjusted) | English proficient: 153, CALD: 96 | 38.55% | Spanish (67.7%), Other (32.3%) |
| Hines et al. [22] | 2014 | USA | Retrospective cohort study | English proficient: 46 CALD: 38.41 | English proficient: M: 1,348,811 F: 1,862,645 CALD: M: 198,664 F: 347,098 | 3,757,218 | NR | English proficient: 3,211,939, CALD: 545,279 | 14.50% | Spanish (12.6%), API (1.9%) |
| De La Plata et al. [23] | 2007 | USA | Retrospective cohort study | English proficient: 37.69 CALD Hispanic: 34 | English proficient: M: 299 F: 44 CALD: M = 35, F: 7 | 476 | English proficient: 21 (9) English proficient Hispanic: 22 (11) CALD Hispanic: 22 (10) | English Proficient: 434 CALD: 42 | 8.82% | Spanish (8.82% |
| Meyer et al. [24] | 2023 | USA | Retrospective cohort study | English proficient: 44.26, CALD: 45.13 | Total: M: 7395, F: 3340 English proficient (M: 7202, F: 3276), CALD: (M: 193, F: 64) | 10735 | English proficient: 12.35, CALD: 10.43 | English proficient: 10478, CALD: 257 | 2.39% | Spanish: 80.9%, Vietnamese: 6%, American Sign Language: 3.7%, Other: 9.4% |
| Ponsford et al. [14] | 2020 | Australia | Retrospective cohort study | English proficient: 37.25 ± 16.29, CALD: 39.82 ± 17.18 | NR | 206 | NR | English proficient: 103, CALD: 103 | 50% | Asian: 44.66%, European: 37.86%, Africa and Middle East: 11.65%, Polynesian: 3.89%, Latin American: 1.94%, |
| Sander et al. [25] | 2023 | USA | Prospective, cross-sectional cohort study | English proficient: 33.7 ± 15.9, CALD: 40.8 ± 19 | Total: M: 768, F: 230 English proficient: (M: 359, F: 133), CALD: (M: 409, F: 97) | 998 | NR | English proficient: 492, CALD: 506 | 50.70% | Spanish: 100% |
| Kinney et al. [26] | 2023 | USA | Retrospective cohort study | <40: 3510, 40–64: 3951, ≥65: 3348 | M: 7449, F: 3360 | 10809 (3348 available for analysis) | 21.1 ± 12.2 | English proficient: 9920 (3087 available for analysis), CALD: 889 (261 available for analysis) | 8.22% (7.80% from analysable population) | NR |
| Study | Representative of the Exposed Cohort | Selection of External Control/Non-Exposed Cohort | Ascertainment of Exposure | Outcome of Interest not Present at Start of Study | Study Controls for Intervention | Study Control for External Confounders | Assessment of Outcomes/Ascertainment of Exposure | Sufficient Follow-Up/Same Method of Ascertainment for Cases and Controls | Adequacy of Follow-Up/Non-Response Rate | Total Score (/9) |
|---|---|---|---|---|---|---|---|---|---|---|
| Costello et al. [20] | - | - | + | + | - | - | + | + | + | 5 |
| Garduno-Ortega et al. [21] | - | + | + | + | + | - | + | + | - | 6 |
| Hines et al. [22] | - | + | + | + | + | + | + | + | - | 7 |
| De La Plata et al. [23] | + | + | + | + | + | + | + | - | - | 7 |
| Meyer et al. [24] | - | + | + | + | + | - | + | + | + | 7 |
| Ponsford et al. [14] | - | + | + | + | + | - | + | - | - | 5 |
| Sander et al. [25] | - | + | + | + | + | + | + | + | + | 8 |
| Starrosta et al. [26] | + | + | + | + | + | + | + | - | - | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le, K.D.R.; Le, K.; Shahzad, A.; Lee, S.J. The Role of Language Barriers on Hospital Outcomes in Culturally and Linguistically Diverse Patients following Trauma Admission. Trauma Care 2024, 4, 107-119. https://doi.org/10.3390/traumacare4020010
Le KDR, Le K, Shahzad A, Lee SJ. The Role of Language Barriers on Hospital Outcomes in Culturally and Linguistically Diverse Patients following Trauma Admission. Trauma Care. 2024; 4(2):107-119. https://doi.org/10.3390/traumacare4020010
Chicago/Turabian StyleLe, Khang Duy Ricky, Kelvin Le, Abdullah Shahzad, and Su Jin Lee. 2024. "The Role of Language Barriers on Hospital Outcomes in Culturally and Linguistically Diverse Patients following Trauma Admission" Trauma Care 4, no. 2: 107-119. https://doi.org/10.3390/traumacare4020010
APA StyleLe, K. D. R., Le, K., Shahzad, A., & Lee, S. J. (2024). The Role of Language Barriers on Hospital Outcomes in Culturally and Linguistically Diverse Patients following Trauma Admission. Trauma Care, 4(2), 107-119. https://doi.org/10.3390/traumacare4020010