
Preimplantation Testing for Polygenic Disease (PGT-P): Brave New World or Mad Pursuit?



Abstract
:
{kind=link}
1. Background
2. Polygenic Risk Scores
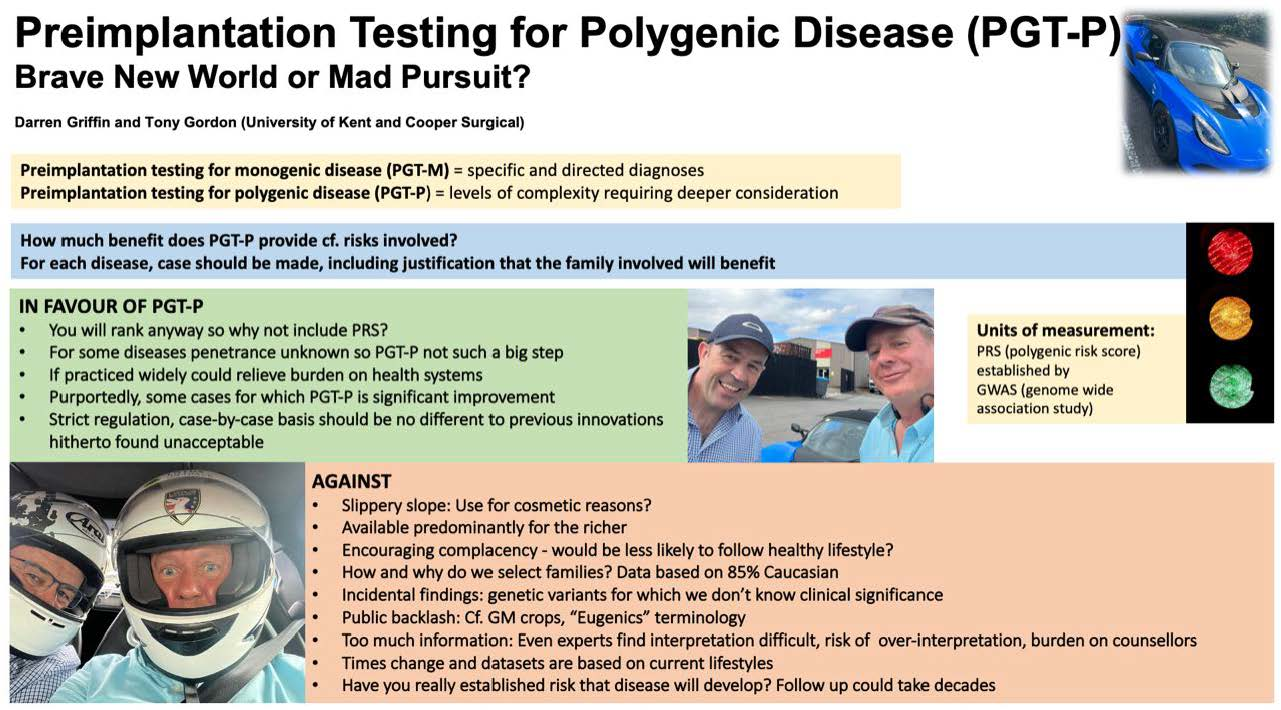
3. Positives in Favour of PGT-P
4. Risks of PGT-P
- Risk without benefit: This treatment could lead to putting patients at risk of the complications associated with IVF (particularly in young, good prognosis patients) with only minimal demonstrable benefits afforded by PGT-P.
- Available only for the rich: The thorny issue to all of this type of treatment is that it is not free at the point of delivery. Richer families are therefore inevitably more likely to benefit from it, and the process could lead to exploitation of families desperate to have children, exposing them to another “add-on” with no proven clinical benefit.
- Slippery slope: By introducing PGT-P, the opportunity for using it for more cosmetic reasons (e.g., height, IQ) less clearly associated with health becomes more likely. Moreover, could the licensing of PGT-P be seen as a prelude to the licensing of the more controversial gene editing or manipulation of embryos? Some say that this is inevitable.
- Encouraging complacency: If a person or parents are safe in the knowledge that they/their child are in a genetically lower risk group of cancer or heart disease, to take two examples, would they be less likely to follow a more healthy lifestyle, thereby negating the benefits of the PGT-P?
- How do we select the families? Which families should be selected for PGT-P, and why? This is not a straightforward question, and it could depend on a series of factors that are not necessarily related to clinical need. The data is based on the 100,000 genomes database, which is 85% Caucasian—other racial backgrounds (including admixtures) might not know whether they should be in a high-risk group.
- Incidental findings and pleiotropic effects: There are many genetic variants for which we do not know (or only partially know) the clinical significance. Many of these will be revealed (potentially) through PGT-P, without proper knowledge or evaluation. These traits do not occur in a vacuum; by selecting against the likelihood of a certain disease, we may be selecting against further traits. Moreover, PGT-P are selected for one polygenic phenotype but since we don’t fully understand the inter-relationships between polygenic trait genes we could accidentally be selecting for another undesirable phenotype?
- Effects of rare SNPs: Some SNPs that are under-represented in databases may have high impact on some PRS and thus skew the interpretation of results.
- Public backlash: We know through experience of GM crops, to take an example, that the public can react badly to certain technologies. Could PGT providers be damaged financially and reputationally as a result of offering PGT-P putting the whole field in jeopardy? People are acutely aware of the “eugenics” terminology and the press for PGT-P thus far has not been good.
- Too much information: Provided with incredible amounts of genomic information that even the experts find it difficult to interpret, there is a genuine risk of obsessive over-interpretation of the PRS on the part of the patients. This could place an unreasonable burden on genetic counsellors—relative risk is hard enough to establish, even at the best of times.
- Times change: The datasets are based on current people’s lifestyles. These will inevitably change by the time the disease develops (or not) in the current embryo. There may also be more effective treatments for these diseases by the time that they become an issue. This applies to all late onset diseases, whether they be monogenic or polygenic.
- Evidence-based medicine: Although it will be possible to ascertain that the foetus has the same genomic sequence as the original diagnosis in the embryo, it really will not be practicable to establish, for most polygenic disorders, whether PGT-P has significantly reduced the chances of the diseases developing. The follow-up of cases could take decades. Some children will also get the disease for which they were diagnosed with a low PRS. Families might not hear the message, “we only told you that your risk was lower”.
5. Cost-Benefit Ratio
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deciphering Developmental Disorders Study. Prevalence and architecture of de novo mutations in developmental disorders. Nature 2017, 542, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Nash, A. National Population Projections: 2018-Based, 2019. Office for National Statistics. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationprojections/bulletins/nationalpopulationprojections/2018based (accessed on 2 February 2023).
- Choi, S.W.; Mak, T.S.H.; O’Reilly, P.F. Tutorial: A guide to performing polygenic risk score analyses. Nat. Protoc. 2020, 15, 2759–2772. [Google Scholar] [CrossRef] [PubMed]
- Ao, A.; Wells, D.; Handyside, A.H.; Winston, R.M.; Delhanty, J.D. Preimplantation genetic diagnosis of inherited cancer: Familial adenomatous polyposis coli. J. Assist. Reprod. Genet. 1998, 15, 140–144. [Google Scholar] [CrossRef]
- Sagi, M.; Weinberg, N.; Eilat, A.; Aizenman, E.; Werner, M.; Girsh, E.; Siminovsky, Y.; Abeliovich, D.; Peretz, T.; Simon, A.; et al. Preimplantation genetic diagnosis for BRCA1/2—A novel clinical experience. Prenat. Diagn. Publ. Affil. Int. Soc. Prenat. Diagn. 2009, 29, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Treff, N.R.; Eccles, J.; Marin, D.; Messick, E.; Lello, L.; Gerber, J.; Xu, J.; Tellier, L.C. Preimplantation genetic testing for polygenic disease relative risk reduction: Evaluation of genomic index performance in 11,883 adult sibling pairs. Genes 2020, 11, 648. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Griffin, D.K.; Gordon, A.T. Preimplantation Testing for Polygenic Disease (PGT-P): Brave New World or Mad Pursuit? DNA 2023, 3, 104-108. https://doi.org/10.3390/dna3020008
Griffin DK, Gordon AT. Preimplantation Testing for Polygenic Disease (PGT-P): Brave New World or Mad Pursuit? DNA. 2023; 3(2):104-108. https://doi.org/10.3390/dna3020008
Chicago/Turabian StyleGriffin, Darren K., and Anthony T. Gordon. 2023. "Preimplantation Testing for Polygenic Disease (PGT-P): Brave New World or Mad Pursuit?" DNA 3, no. 2: 104-108. https://doi.org/10.3390/dna3020008
APA StyleGriffin, D. K., & Gordon, A. T. (2023). Preimplantation Testing for Polygenic Disease (PGT-P): Brave New World or Mad Pursuit? DNA, 3(2), 104-108. https://doi.org/10.3390/dna3020008