

Co-Occurrence of Filifactor alocis with Red Complex Bacteria in Type 2 Diabetes Mellitus Subjects with and without Chronic Periodontitis: A Pilot Study

 , ,
, , 
Abstract
:1. Introduction
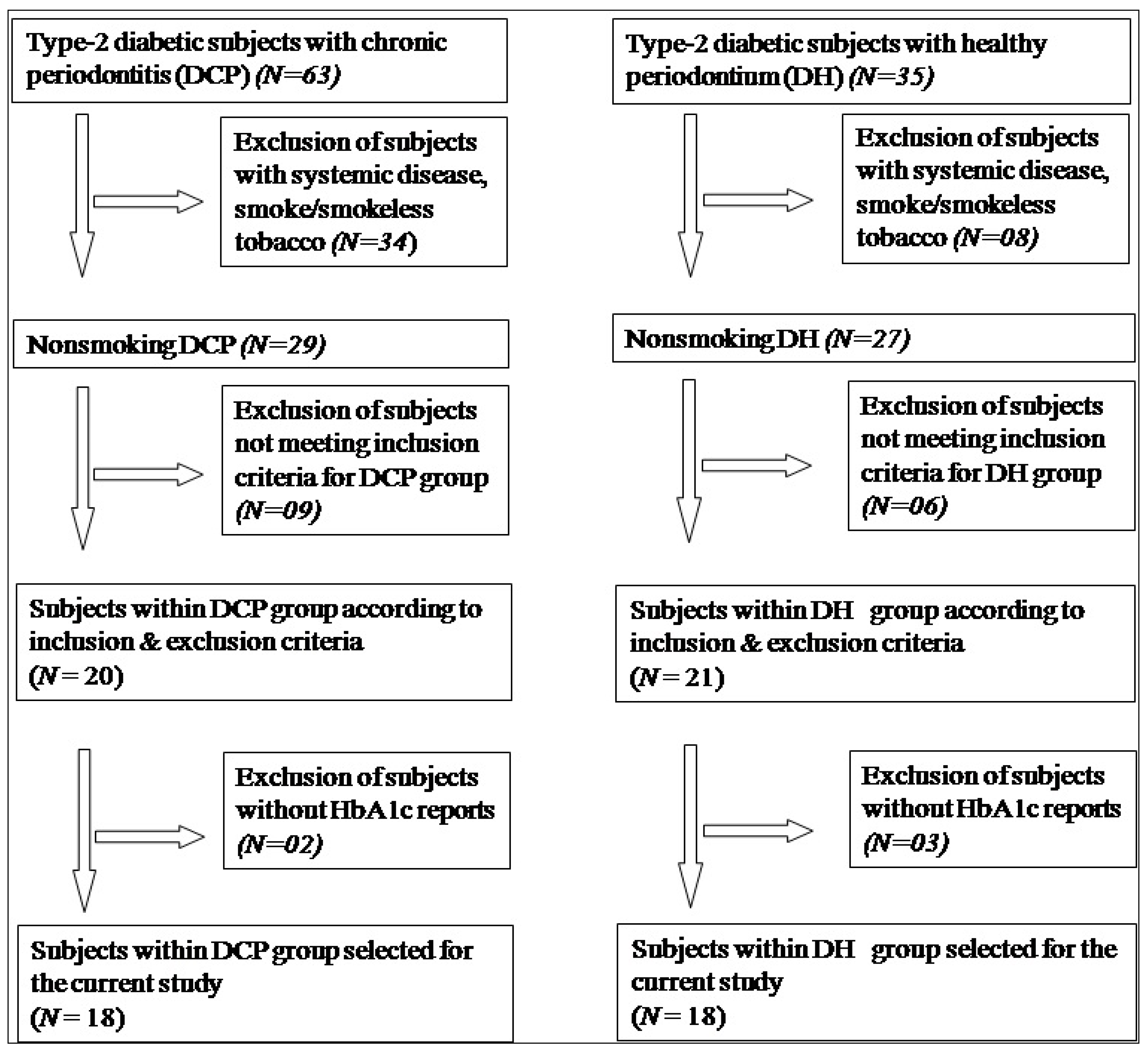
2. Materials and Methods
2.1. Clinical Periodontal Examination
2.2. Subgingival Sample Collection
2.3. DNA Isolation
2.4. Identification of F. alocis and Red Complex Bacteria—PCR Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Socransky, S.S.; Haffajee, A.D.; Cugini, M.A.; Smith, C.; Kent, R.L. Microbial Complexes in Subgingival Plaque. J. Clin. Periodontol. 1998, 25, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Slots, J.; Bragd, L.; Wikstrom, M.; Dahlen, G. The Occurrence of Actinobacillus Actinomycetemcomitans, Bacteroides Gingivalis and Bacteroides Intermedius in Destructive Periodontal Disease in Adults. J. Clin. Periodontol. 1986, 13, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Aruni, A.W.; Roy, F.; Fletcher, H.M. Filifactor Alocis Has Virulence Attributes That Can Enhance Its Persistence under Oxidative Stress Conditions and Mediate Invasion of Epithelial Cells by Porphyromonas Gingivalis. Infect. Immun. 2011, 79, 3872–3886. [Google Scholar] [CrossRef] [PubMed]
- Sonnenschein, S.K.; Meyle, J. Local Inflammatory Reactions in Patients with Diabetes and Periodontitis. Periodontology 2000 2015, 69, 221–254. [Google Scholar] [CrossRef] [PubMed]
- Firatli, E. The Relationship between Clinical Periodontal Status and Insulin-Dependent Diabetes Mellitus. Results after 5 Years. J. Periodontol. 1997, 68, 136–140. [Google Scholar] [CrossRef]
- Tervonen, T.; Karjalainen, K.; Knuuttila, M.; Huumonen, S. Alveolar Bone Loss in Type 1 Diabetic Subjects. J. Clin. Periodontol. 2000, 27, 567–571. [Google Scholar] [CrossRef]
- Tervonen, T.; Karjalainen, K. Periodontal disease related to diabetic status. A pilot study of the response to periodontal therapy in Type 1 diabetes. J. Clin. Periodontol. 1997, 24, 505–510. [Google Scholar] [CrossRef]
- Mealey, B.L.; Ocampo, G.L. Diabetes Mellitus and Periodontal Disease. Periodontology 2000 2007, 44, 127–153. [Google Scholar] [CrossRef]
- Ganesan, S.M.; Joshi, V.; Fellows, M.; Dabdoub, S.M.; Nagaraja, H.N.; O’Donnell, B.; Deshpande, N.R.; Kumar, P.S. A Tale of Two Risks: Smoking, Diabetes and the Subgingival Microbiome. ISME J. 2017, 11, 2075–2089. [Google Scholar] [CrossRef]
- Schlafer, S.; Riep, B.; Griffen, A.L.; Petrich, A.; Hübner, J.; Berning, M.; Friedmann, A.; Göbel, U.B.; Moter, A. Filifactor Alocis-Involvement in Periodontal Biofilms. BMC Microbiol. 2010, 10, 66. [Google Scholar] [CrossRef] [Green Version]
- Gomes, B.P.F.A.; Jacinto, R.C.; Pinheiro, E.T.; Sousa, E.L.R.; Zaia, A.A.; Ferraz, C.C.R.; Souza-Filho, F.J. Molecular Analysis of Filifactor Alocis, Tannerella Forsythia, and Treponema Denticola Associated with Primary Endodontic Infections and Failed Endodontic Treatment. J. Endod. 2006, 32, 937–940. [Google Scholar] [CrossRef]
- Armitage, G.C. Development of a Classification System for Periodontal Diseases and Conditions. Ann. Periodontol. 1999, 4, 1–6. [Google Scholar] [CrossRef]
- Löe, H. The Gingival Index, the Plaque Index and the Retention Index Systems. J. Periodontol. 1967, 38, 610–616. [Google Scholar] [CrossRef]
- Carter, H.G.; Barnes, G.P. The Gingival Bleeding Index. J. Periodontol. 1974, 45, 801–805. [Google Scholar] [CrossRef]
- Mahmood, K.; Aamir, A.H. Glycemic Control Status in Patients with Type-2 Diabetes. J. Coll. Physicians Surg. Pak. JCPSP 2005, 15, 323–325. [Google Scholar]
- Kugaji, M.S.; Bhat, K.G.; Joshi, V.M.; Pujar, M.; Mavani, P.T. Simplified Method of Detection of Dialister Invisus and Olsenella Uli in Oral Cavity Samples by Polymerase Chain Reaction. J. Adv. Oral Res. 2017, 8, 47–52. [Google Scholar] [CrossRef]
- Siqueira, J.F.; Rôças, I.N. Simultaneous Detection of Dialister Pneumosintes and Filifactor Alocis in Endodontic Infections by 16S RDNA-Directed Multiplex PCR. J. Endod. 2004, 30, 851–854. [Google Scholar] [CrossRef]
- D’Ercole, S.; Piccolomini, R.; Capaldo, G.; Catamo, G.; Perinetti, G.; Guida, L. Effectiveness of Ultrasonic Instruments in the Therapy of Severe Periodontitis: A Comparative Clinical-Microbiological Assessment with Curettes. New Microbiol. 2006, 29, 101–110. [Google Scholar]
- Pérez-Chaparro, P.J.; Gonçalves, C.; Figueiredo, L.C.; Faveri, M.; Lobão, E.; Tamashiro, N.; Duarte, P.; Feres, M. Newly Identified Pathogens Associated with Periodontitis. J. Dent. Res. 2014, 93, 846–858. [Google Scholar] [CrossRef]
- Dewhirst, F.E.; Chen, T.; Izard, J.; Paster, B.J.; Tanner, A.C.R.; Yu, W.-H.; Lakshmanan, A.; Wade, W.G. The Human Oral Microbiome. J. Bacteriol. 2010, 192, 5002–5017. [Google Scholar] [CrossRef]
- Kumar, P.S.; Griffen, A.L.; Barton, J.A.; Paster, B.J.; Moeschberger, M.L.; Leys, E.J. New Bacterial Species Associated with Chronic Periodontitis. J. Dent. Res. 2003, 82, 338–344. [Google Scholar] [CrossRef]
- Jalava, J.; Eerola, E. Phylogenetic Analysis of Fusobacterium alocis and Fusobacterium sulci Based on 16S RRNA Gene Sequences: Proposal of Filifactor alocis (Cato, Moore and Moore) Comb. Nov. and Eubacterium Sulci (Cato, Moore and Moore) Comb. Nov. Int. J. Syst. Bacteriol. 1999, 49, 1375–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cato, E.P.; Moore, L.V.H.; Moore, W.E.C. Fusobacterium alocis Sp. Nov. and Fusobacterium sulci Sp. Nov. from the Human Gingival Sulcus. Int. J. Syst. Bacteriol. 1985, 35, 475–477. [Google Scholar] [CrossRef]
- Kumar, P.S.; Leys, E.J.; Bryk, J.M.; Martinez, F.J.; Moeschberger, M.L.; Griffen, A.L. Changes in Periodontal Health Status Are Associated with Bacterial Community Shifts as Assessed by Quantitative 16S Cloning and Sequencing. J. Clin. Microbiol. 2006, 44, 3665–3673. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.S.; Griffen, A.L.; Moeschberger, M.L.; Leys, E.J. Identification of Candidate Periodontal Pathogens and Beneficial Species by Quantitative 16S Clonal Analysis. J. Clin. Microbiol. 2005, 43, 3944–3955. [Google Scholar] [CrossRef]
- Dahlén, G.; Leonhardt, Å. A New Checkerboard Panel for Testing Bacterial Markers in Periodontal Disease. Oral Microbiol. Immunol. 2006, 21, 6–11. [Google Scholar] [CrossRef]
- Colombo, A.P.V.; Boches, S.K.; Cotton, S.L.; Goodson, J.M.; Kent, R.; Haffajee, A.D.; Socransky, S.S.; Hasturk, H.; Van Dyke, T.E.; Dewhirst, F.; et al. Comparisons of Subgingival Microbial Profiles of Refractory Periodontitis, Severe Periodontitis, and Periodontal Health Using the Human Oral Microbe Identification Microarray. J. Periodontol. 2009, 80, 1421–1432. [Google Scholar] [CrossRef]
- Aruni, A.W.; Mishra, A.; Dou, Y.; Chioma, O.; Hamilton, B.N.; Fletcher, H.M. Filifactor Alocis—A New Emerging Periodontal Pathogen. Microbes Infect. 2015, 17, 517–530. [Google Scholar] [CrossRef]
- Giugliano, D.; Ceriello, A.; Paolisso, G. Diabetes Mellitus, Hypertension, and Cardiovascular Disease: Which Role for Oxidative Stress? Metabolism 1995, 44, 363–368. [Google Scholar] [CrossRef]
- Schara, R.; Skaleric, E.; Seme, K.; Skaleric, U. Prevalence of Periodontal Pathogens and Metabolic Control of Type 1 Diabetes Patients. J. Int. Acad. Periodontol. 2013, 15, 29–34. [Google Scholar]
- Miranda, T.S.; Feres, M.; Retamal-Valdes, B.; Perez-Chaparro, P.J.; Maciel, S.S.; Duarte, P.M. Influence of Glycemic Control on the Levels of Subgingival Periodontal Pathogens in Patients with Generalized Chronic Periodontitis and Type 2 Diabetes. J. Appl. Oral Sci. 2017, 25, 82–89. [Google Scholar] [CrossRef]
- Chen, H.; Liu, Y.; Zhang, M.; Wang, G.; Qi, Z.; Bridgewater, L.; Zhao, L.; Tang, Z.; Pang, X. A Filifactor Alocis-Centered Co-Occurrence Group Associates with Periodontitis across Different Oral Habitats. Sci. Rep. 2015, 5, 9053. [Google Scholar] [CrossRef]
- Haffajee, A.D.; Socransky, S.S. Relation of Body Mass Index, Periodontitis and Tannerella Forsythia. J. Clin. Periodontol. 2009, 36, 89–99. [Google Scholar] [CrossRef]
- Brennan, R.M.; Genco, R.J.; Wilding, G.E.; Hovey, K.M.; Trevisan, M.; Wactawski-Wende, J. Bacterial Species in Subgingival Plaque and Oral Bone Loss in Postmenopausal Women. J. Periodontol. 2007, 78, 1051–1061. [Google Scholar] [CrossRef]
- Smyth, S.; Heron, A. Diabetes and Obesity: The Twin Epidemics. Nat. Med. 2006, 12, 75–80. [Google Scholar] [CrossRef]
- Ardila Medina, C.M.; Ariza Garcés, A.A.; Guzmán Zuluaga, I.C. Coexistence of Porphyromonas Gingivalis, Tannerella Forsythia and Treponema Denticola in the Red Bacterial Complex in Chronic Periodontitis Subjects. Int. J. Odontostomatol. 2014, 8, 359–364. [Google Scholar] [CrossRef]
- Gonçalves, C.; Soares, G.M.S.; Faveri, M.; Pérez-Chaparro, P.J.; Lobão, E.; Figueiredo, L.C.; Baccelli, G.T.; Feres, M. Association of Three Putative Periodontal Pathogens with Chronic Periodontitis in Brazilian Subjects. J. Appl. Oral Sci. 2016, 24, 181–185. [Google Scholar] [CrossRef]
- Oliveira, R.R.D.S.; Fermiano, D.; Feres, M.; Figueiredo, L.C.; Teles, F.R.F.; Soares, G.M.S.; Faveri, M. Levels of Candidate Periodontal Pathogens in Subgingival Biofilm. J. Dent. Res. 2016, 95, 711–718. [Google Scholar] [CrossRef]
- Joshi, V.; Bhat, K.; Kugaji, M.; Ingalgi, P. Occurrence of Aggregatibacter Actinomycetemcomitans in Indian Chronic Periodontitis Patients and Periodontally Healthy Adults. J. Indian Soc. Periodontol. 2016, 20, 141–144. [Google Scholar] [CrossRef]
- Zambon, J.J.; Reynolds, H.; Fisher, J.G.; Shlossman, M.; Dunford, R.; Genco, R.J. Microbiological and Immunological Studies of Adult Periodontitis in Patients with Noninsulin-Dependent Diabetes Mellitus. J. Periodontol. 1988, 59, 23–31. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Organisms | Primer Sequence 5′-3′ | Product Size (Base Pairs) |
|---|---|---|
| F. alocis | 594 | |
| Forward | CAGGTGGTTTAACAAGTTAGTGG | |
| Reverse | CTAAGTTGTCCTTAGCTGTCTCG | |
| P. gingivalis | 404 | |
| Forward | AGGCAGCTTGCCATACTGCG | |
| Reverse | ACTGTTAGCAACTACCGATGT | |
| T. denticola | 316 | |
| Forward | TAATACCGAATGTGCTCATTTACAT | |
| Reverse | TCAAAGAAGCATTCCCTCTTCTTCTTA | |
| T. forsythia | 641 | |
| Forward | GCGTATGTAACCTGCCCGCA | |
| Reverse | TGCTTCAGTGTCAGTTATACCT |
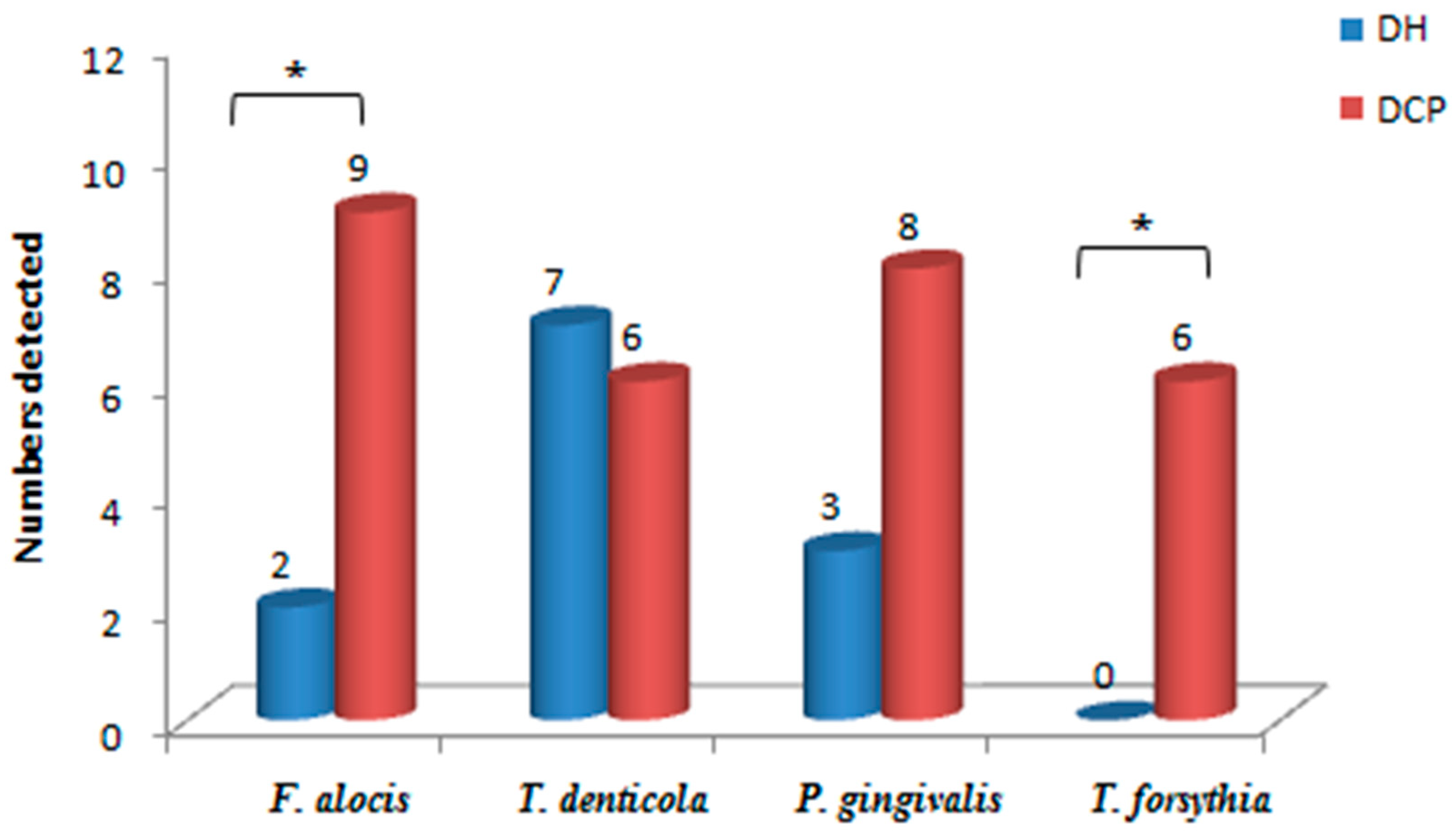
| Organism | DH (%) | DCP (%) | Odds Ratio | 95% Confidence Interval | p Value |
|---|---|---|---|---|---|
| F. alocis | 2 (11.11) | 9 (50%) | 0.12 | 0.02 to 0.70 | 0.02 * |
| T. denticola | 7 (38.88%) | 6 (33.33%) | 1.27 | 0.32 to 4.97 | 1.0 |
| P. gingivalis | 3 (16.66%) | 8 (44.44%) | 0.25 | 0.05 to 1.17 | 0.1 |
| T. forsythia | 0 (0%) | 6 (33.33%) | 0.051 | 0.002 to 1.00 | 0.01 * |
| Red Complex Bacteria | F. alocis | p-Value | ||
|---|---|---|---|---|
| Negative | Positive | |||
| T. denticola | Positive | 9 (36%) | 4 (36.36%) | 1.0 |
| Negative | 16 (64%) | 7 (63.64) | ||
| Total | 25 (100%) | 11 (100%) | ||
| P. gingivalis | Positive | 7 (28%) | 4 (36.36%) | 0.70 |
| Negative | 18 (72%) | 7 (63.64%) | ||
| Total | 25 (100%) | 11 (100%) | ||
| T. forsythia | Positive | 1 (4%) | 5 (45.45%) | 0.006 * |
| Negative | 24 (96%) | 6 (54.55%) | ||
| Total | 25 (100%) | 11 (100%) | ||
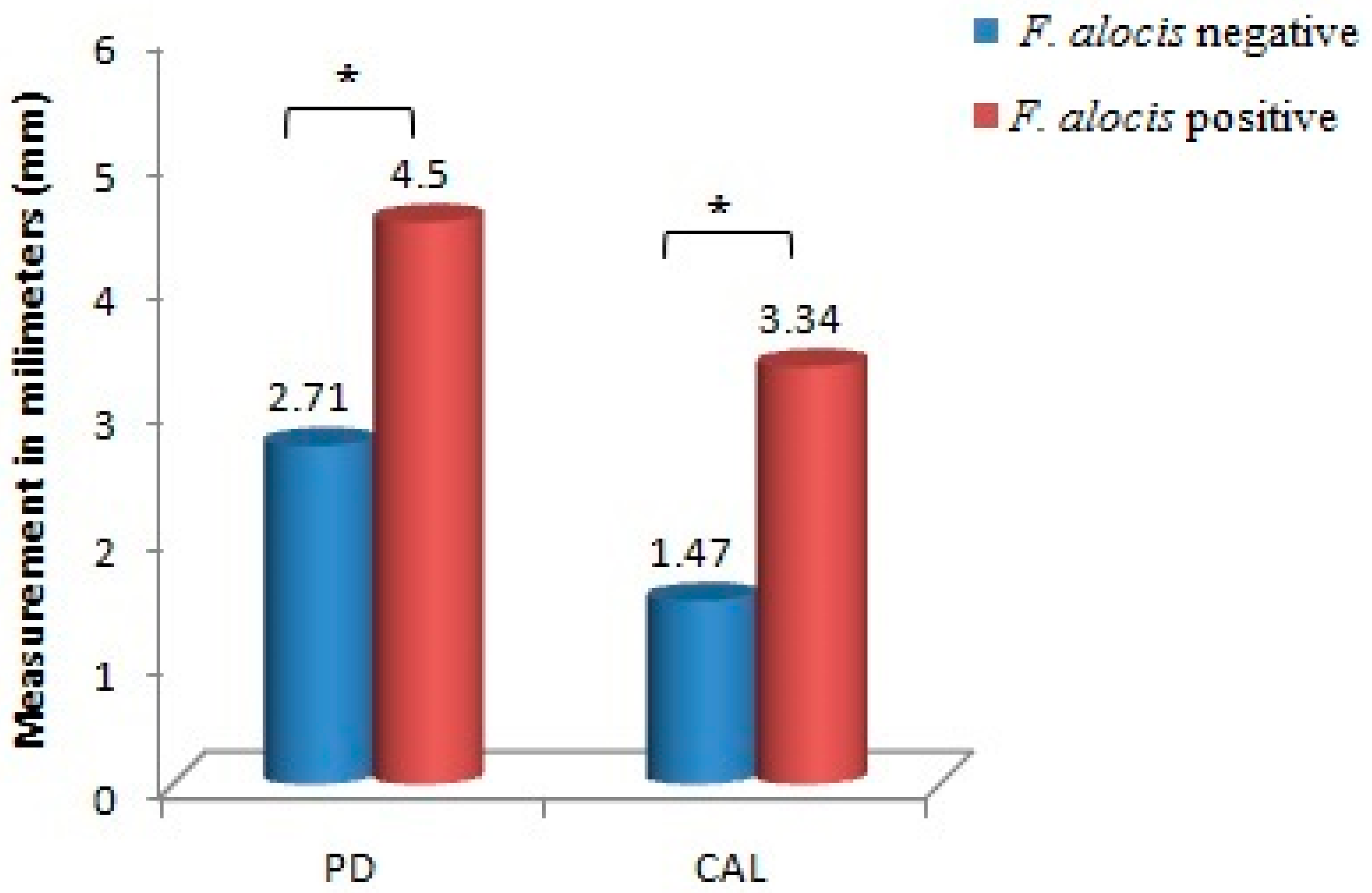
| Clinical Parameters | F. alocis | N | Mean | Standard Deviation | p-Value |
|---|---|---|---|---|---|
| GI | Negative | 25 | 0.76 | 0.90 | 0.15 |
| Positive | 11 | 1.57 | 0.75 | ||
| PI | Negative | 25 | 0.78 | 0.92 | 0.08 |
| Positive | 11 | 1.61 | 0.77 | ||
| BI (%) | Negative | 25 | 35.9 | 41.56 | 0.08 |
| Positive | 11 | 72.55 | 34.69 | ||
| PD | Negative | 25 | 2.71 | 1.90 | 0.01 * |
| Positive | 11 | 4.50 | 1.61 | ||
| CAL | Negative | 25 | 1.45 | 2.01 | 0.03 * |
| Positive | 11 | 3.35 | 1.75 |
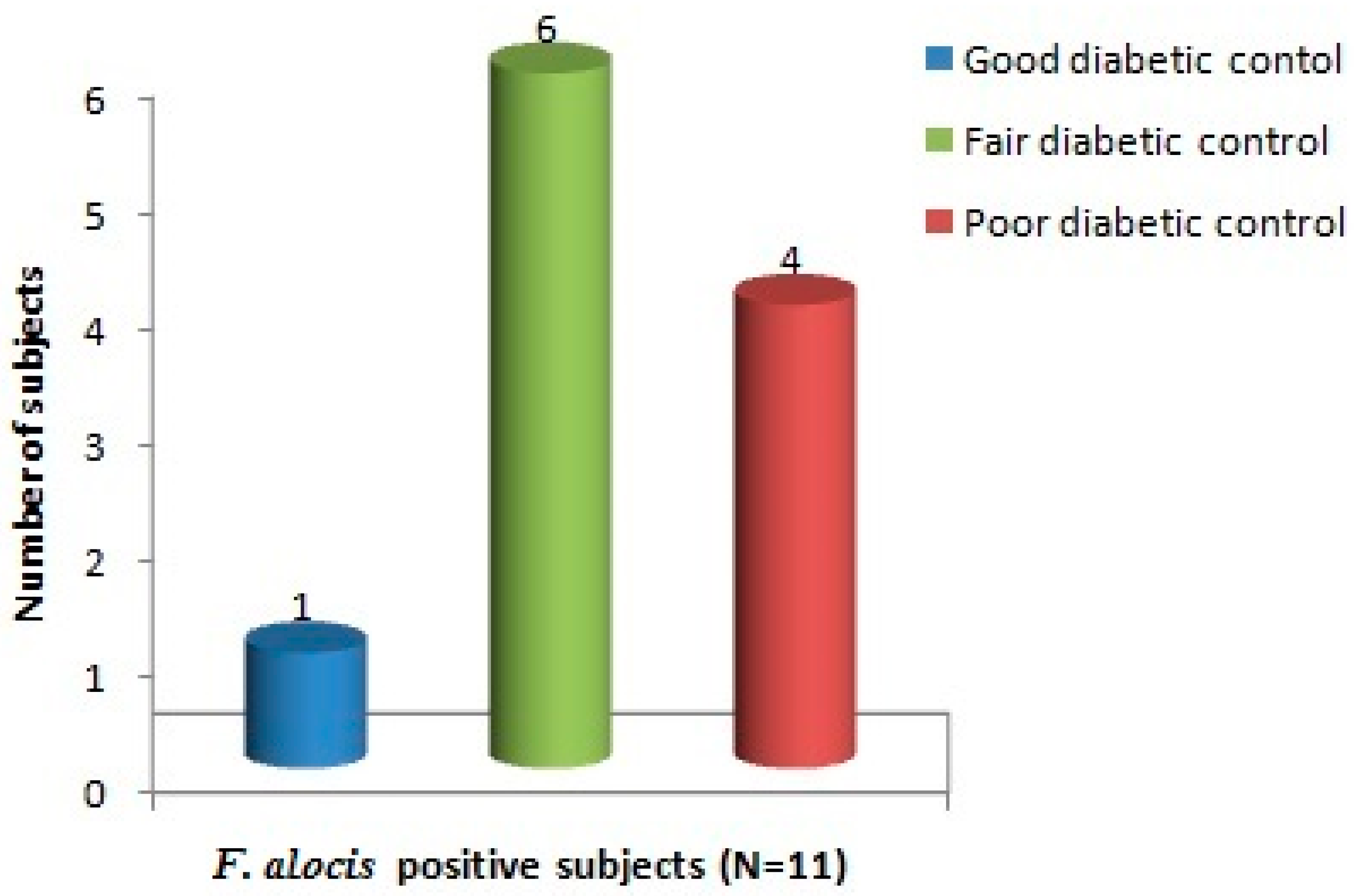
| HbA1C | F. alocis | p Value | |
|---|---|---|---|
| Negative | Positive | ||
| Good diabetic control (6–7%) | 0 | 1 | 0.21 |
| 0% | 100% | ||
| Fair diabetic control (7.1–8.2%) | 11 | 6 | |
| 64.7% | 35.3% | ||
| Poor diabetic control (>8.2%) | 14 | 4 | |
| 77.8% | 22.2% | ||
| Total | 25 | 11 | |
| 69.4% | 30.6% | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shaikh, H.F.M.; Oswal, P.U.; Kugaji, M.S.; Katti, S.S.; Bhat, K.G.; Joshi, V.M. Co-Occurrence of Filifactor alocis with Red Complex Bacteria in Type 2 Diabetes Mellitus Subjects with and without Chronic Periodontitis: A Pilot Study. Int. J. Transl. Med. 2023, 3, 97-107. https://doi.org/10.3390/ijtm3010009
Shaikh HFM, Oswal PU, Kugaji MS, Katti SS, Bhat KG, Joshi VM. Co-Occurrence of Filifactor alocis with Red Complex Bacteria in Type 2 Diabetes Mellitus Subjects with and without Chronic Periodontitis: A Pilot Study. International Journal of Translational Medicine. 2023; 3(1):97-107. https://doi.org/10.3390/ijtm3010009
Chicago/Turabian StyleShaikh, Hawaabi F. M., Pratima U. Oswal, Manohar S. Kugaji, Sandeep S. Katti, Kishore G. Bhat, and Vinayak M. Joshi. 2023. "Co-Occurrence of Filifactor alocis with Red Complex Bacteria in Type 2 Diabetes Mellitus Subjects with and without Chronic Periodontitis: A Pilot Study" International Journal of Translational Medicine 3, no. 1: 97-107. https://doi.org/10.3390/ijtm3010009
APA StyleShaikh, H. F. M., Oswal, P. U., Kugaji, M. S., Katti, S. S., Bhat, K. G., & Joshi, V. M. (2023). Co-Occurrence of Filifactor alocis with Red Complex Bacteria in Type 2 Diabetes Mellitus Subjects with and without Chronic Periodontitis: A Pilot Study. International Journal of Translational Medicine, 3(1), 97-107. https://doi.org/10.3390/ijtm3010009