


Effects of Saddle Position on Cycling: An Umbrella Review

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Results
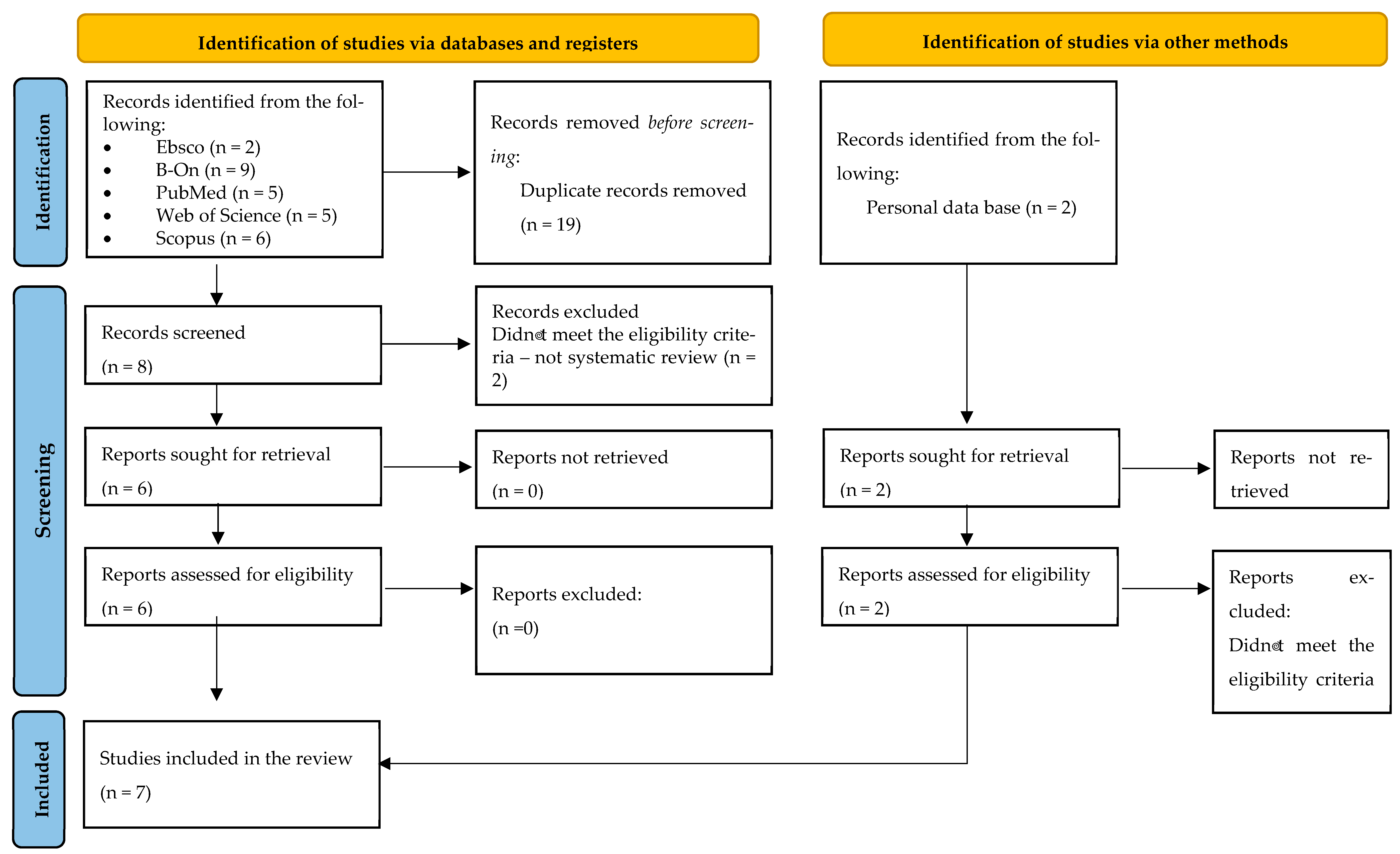
2.1. Included Systematic Reviews
2.2. Methodological Quality Assessment
3. Methods
3.1. Search Strategy
3.2. Study Selection and Eligibility Criteria
- (a)
- Examined the effects of saddle position on cycling,
- (b)
- Analyzed the data using systematic reviews,
- (c)
- Were published in English,
- (d)
- Full texts available.
- (a)
- Non-systematic reviews, including books, randomized controlled trials, case reports, expert opinions, mixed-methods, conference papers, academic thesis, literature reviews, or narrative reviews;
- (b)
- Those that assessed traumatic (acute) injuries in cycling;
- (c)
- Those composed by experimental or control groups that included animals, cadaveric, in vitro, or in silico samples.
3.3. Data Collection Process
- (1)
- List of authors and year of publication,
- (2)
- Objectives of the studies,
- (3)
- Number and type of studies included in the review,
- (4)
- Number and characteristics of participants,
- (5)
- Outcomes,
- (6)
- Main findings and conclusions of the studies.
3.4. Outcomes
- Low back pain,
- Knee injury/pain,
- Lumbar kyphosis,
- Impact on perineum.
- Muscle activation,
- Oxygen uptake,
- Load and intensity,
- Efficiency,
- Comfort.
3.5. Methodological Quality Evaluation
3.6. Prisma Statement
4. Discussion
4.1. Health
4.1.1. Low Back Pain
4.1.2. Knee Injury or Pain
4.1.3. Lumbar Kyphosis
4.1.4. Impact on Perineum
4.2. Performance
4.2.1. Muscular Activation
4.2.2. Oxygen Uptake
4.2.3. Load and Intensity
4.2.4. Efficiency
4.2.5. Comfort
5. Study Limitations
6. Conclusions
7. Implications of the Results for Practice, Policy, and Future Research
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Priego Quesada, J.I.; Kerr, Z.Y.; Bertucci, W.M.; Carpes, F.P.; Barbosa, T.M. A retrospective international study on factors associated with injury, discomfort and pain perception among cyclists. PLoS ONE 2019, 14, e0211197. [Google Scholar] [CrossRef] [PubMed]
- Hopker, J. Identifying and developing talent in cycle sport. Sports Med. J. 2016, 5, 416–422. [Google Scholar]
- Faria, E.W.; Parker, D.L.; Faria, I.E. The science of cycling. Factors affecting performance—Part 2. Sports Med. 2005, 35, 313–337. [Google Scholar] [CrossRef]
- Faria, E.W.; Parker, D.L.; Faria, I.E. The science of cycling. Physiology and training—Part 1. Sports Med. 2005, 35, 285–312. [Google Scholar] [CrossRef] [PubMed]
- Cook, O.; Dobbin, N. The association between sport nutrition knowledge, nutritional intake, energy availability, and training characteristics with the risk of an eating disorder amongst highly trained competitive road cyclists. Sport Sci. Health 2022, 18, 1243–1251. [Google Scholar] [CrossRef]
- Spindler, D.J.; Allen, M.S.; Vella, S.A.; Swann, C. The psychology of elite cycling: A systematic review. J. Sports Sci. 2018, 36, 1943–1954. [Google Scholar] [CrossRef]
- García-López, J.; Rodríguez-Marroyo, J.A.; Juneau, C.-E.; Peleteiro, J.; Martínez, A.C.; Villa, J.G. Reference values and improvementof aerodynamic drag in professional cyclists. J. Sports Sci. 2008, 26, 277–286. [Google Scholar] [CrossRef]
- Peveler, W.W.; Green, J.M. Effects of saddle height on economy and anaerobic power in well-trained cyclists. J. Strength Cond. Res. 2011, 25, 629–633. [Google Scholar] [CrossRef]
- Christiaans, H.H.C.M.; Bremner, A. Comfort on bicycles and the validity of a commercial bicycle fitting system. Appl. Ergon. 1998, 29, 201–211. [Google Scholar] [CrossRef]
- Rodríguez-Marroyo, J.A.; García-López, J.; Chamari, K.; Córdova, A.; Hue, O.; Villa, J.G. The rotor pedaling system improves anaerobic but not aerobic cycling performance in professional cyclists. Eur. J. Appl. Physiol. 2009, 106, 87–94. [Google Scholar] [CrossRef]
- Bini, R.R.; Hume, P.A.; Croft, J. Cyclists and triathletes have different body positions on the bicycle. Eur. J. Sport Sci. 2014, 14 (Suppl. S1), S109–S115. [Google Scholar] [CrossRef] [PubMed]
- Bini, R.R.; Carpes, F.P. (Eds.) Biomechanics of Cycling; Springer: Basel, Switzerland, 2014; pp. 13–21. [Google Scholar]
- Swart, J.; Holliday, W. Cycling biomechanics optimization—The (R) evolution of bicycle fitting. Curr. Sports Med. Rep. 2019, 18, 490–496. [Google Scholar] [CrossRef] [PubMed]
- García-López, J.; del Blanco, P.A. Kinematic analysis of bicycle pedalling using 2d and 3d motion capture systems. ISBS Proceed. Arch. 2017, 35, 125. [Google Scholar]
- Rankin, J.W.; Neptune, R.R. The influence of seat configuration on maximal average crank power during pedaling: A simulation study. J. Appl. Biomech. 2010, 26, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Ferrer-Roca, V.; Roig, A.; Galilea, P.; García-López, J. Influence of saddle height on lower limb kinematics in well-trained cyclists: Static vs. dynamic evaluation in bike fitting. J. Strength Cond. Res. 2012, 26, 3025–3029. [Google Scholar] [CrossRef]
- Burt, P. Bike Fit 2nd Edition: Optimise Your Bike Position for High Performance and Injury Avoidance; Bloomsbury Publishing: London, UK, 2022. [Google Scholar]
- Bini, R.; Priego-Quesada, J. Methods to determine saddle height in cycling and implications of changes in saddle height in performance and injury risk: A systematic review. J. Sports Sci. 2022, 40, 386–400. [Google Scholar] [CrossRef]
- Garside, I.; Doran, D.A. Effects of bicycle frame ergonomics on triathlon 10-km running performance. J. Sports Sci. 2000, 18, 825–833. [Google Scholar] [CrossRef]
- Ricard, M.D.; Hills-Meyer, P.; Miller, M.G.; Michael, T.J. The effects of bicycle frame geometry on muscle activation and power during a Wingate anaerobic test. J. Sports Sci. Med. 2006, 5, 25. [Google Scholar]
- Fonda, B.; Panjan, A.; Markovic, G.; Sarabon, N. Adjusted saddle position counteracts the modified muscle activation patterns during uphill cycling. J. Electrom. Kinesiol. 2011, 21, 854–860. [Google Scholar] [CrossRef]
- Holliday, W.; Swart, J. Anthropometrics, flexibility, and training history as determinants for bicycle configuration. Sports Med. Health Sci. 2021, 3, 93–100. [Google Scholar] [CrossRef]
- Bini, R.R.; Hume, P.A.; Lanferdini, F.J.; Vaz, M.A. Effects of moving forward or backward on the saddle on knee joint forces during cycling. Phys. Ther. Sport 2013, 14, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, M.J. Lower body problems and injury in cycling. J. Bodywork Mov. Ther. 2005, 9, 226–236. [Google Scholar] [CrossRef]
- Heron, N.; Sarriegui, I.; Jones, N.; Nolan, R. International consensus statement on injury and illness reporting in professional road cycling. Phys. Sports Med. 2021, 49, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Rooney, D.; Sarriegui, I.; Heron, N. ‘As easy as riding a bike’: A systematic review of injuries and illness in road cycling. BMJ Open Sport Exerc. Med. 2020, 6, e000840. [Google Scholar] [CrossRef]
- Sabeti-Aschraf, M.; Serek, M.; Geisler, M.; Schmidt, M.I.; Pachtner, T.; Ochsner, A.; Funovics, P.; Graf, A. Overuse Injuries Correlated to the Mountain Bikes Adjustment: A Prospective Field Study. Open Sports Sci. J. 2010, 3, 5–6. [Google Scholar] [CrossRef]
- Silberman, M.R. Bicycling injuries. Curr. Sports Med. Rep. 2013, 12, 337–345. [Google Scholar] [CrossRef]
- Millour, G.; Bertucci, W. Comparison of Genzling method vs. Hamley method allowing a postural adjustment in cycling: Preliminary study. Comp. Meth. Biomech. Biomed. Eng. 2017, 20 (Suppl. S1), S135–S136. [Google Scholar] [CrossRef]
- Antequera-Vique, J.A.; Oliva-Lozano, J.M.; Muyor, J.M. Effects of cycling on the morphology and spinal posture in professional and recreational cyclists: A systematic review. Sports Biomech. 2023, 22, 567–596. [Google Scholar] [CrossRef]
- Bini, R.R.; Flores Bini, A. Potential factors associated with knee pain in cyclists: A systematic review. Open A. J. Sports Med. 2018, 99–106. [Google Scholar] [CrossRef]
- Johnston, T.E.; Baskins, T.A.; Koppel, R.V.; Oliver, S.A.; Stieber, D.J.; Hoglund, L.T. The influence of extrinsic factors on knee biomechanics during cycling: A systematic review of the literature. Int. J. Sports Phys. Ther. 2017, 12, 1023. [Google Scholar] [CrossRef]
- Litwinowicz, K.; Choroszy, M.; Wróbel, A. Strategies for Reducing the Impact of Cycling on the Perineum in Healthy Males: Systematic Review and Meta-analysis. Sports Med. 2021, 51, 275–287. [Google Scholar] [CrossRef] [PubMed]
- Streisfeld, G.M.; Bartoszek, C.; Creran, E.; Inge, B.; McShane, M.D.; Johnston, T. Relationship between body positioning, muscle activity, and spinal kinematics in cyclists with and without low back pain: A systematic review. Sports Health 2017, 9, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Visentini, P.J.; McDowell, A.H.; Pizzari, T. Factors associated with overuse injury in cyclists: A systematic review. J. Sci. Med. Sport 2022, 25, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Baran, C.; Mitchell, G.C.; Hellstrom, W.J. Cycling-related sexual dysfunction in men and women: A review. Sex. Med. Rev. 2014, 2, 93–101. [Google Scholar] [CrossRef]
- Sommer, F.; Goldstein, I.; Korda, J.B. Bicycle riding and erectile dysfunction: A review. J. Sex. Med. 2010, 7, 2346–2358. [Google Scholar] [CrossRef]
- Bury, K.; Leavy, J.E.; Lan, C.; O’Connor, A.; Jancey, J. A saddle sores among female competitive cyclists: A systematic scoping review. J. Sci. Med. Sport 2021, 24, 357–367. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Fusar-Poli, P.; Radua, J. Ten simple rules for conducting umbrella reviews. BMJ Ment. Health 2018, 21, 95–100. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358. [Google Scholar] [CrossRef]
- Bini, R.R.; Hume, P.A. Effects of saddle height on knee forces of recreational cyclists with and without knee pain. Int. Sports Med. J. 2014, 15, 188–199. [Google Scholar]
- Dettori, N.J.; Norvell, D.C. Non-traumatic bicycle injuries: A review of the literature. Sports Med. 2006, 36, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Decock, M.; De Wilde, L.; Vanden Bossche, L.; Steyaert, A.; Van Tongel, A. Incidence and aetiology of acute injuries during competitive road cycling. Br. J. Sports Med. 2016, 50, 669. [Google Scholar] [CrossRef]
- Silberman, M.R.; Webner, D.; Collina, S.; Shiple, B.J. Road bicycle fit. Clin. J. Sport Med. 2005, 15, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Clarsen, B.; Krosshaug, T.; Bahr, R. Overuse injuries in professional road cyclists. Am. J. Sports Med. 2010, 38, 2494–2501. [Google Scholar] [CrossRef] [PubMed]
- du Toit, F.; Schwellnus, M.; Wood, P.; Swanevelder, S.; Killops, J.; Jordaan, E. Epidemiology, clinical characteristics, and severity of gradual onset injuries in recreational road cyclists: A cross-sectional study in 21,824 cyclists—SAFER XIII. Phys. Ther. Sport 2020, 46, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Barrios, C.; Bernardo, N.; Vera, P.; Laíz, C.; Hadala, M. Changes in sports injuries incidence over time in world-class road cyclists. Int. J. Sports Med. 2015, 36, 241–248. [Google Scholar] [CrossRef]
- Deakon, R.T. Chronic musculoskeletal conditions associated with the cycling segment of the triathlon: Prevention and treatment with an emphasis on proper bicycle fitting. Sports Med. Arthr. Rev. 2012, 20, 200–205. [Google Scholar] [CrossRef]
- Lebec, M.T.; Cook, K.; Baumgartel, D. Overuse injuries associated with mountain biking: Is single-speed riding a predisposing factor? Sports 2014, 2, 1–13. [Google Scholar] [CrossRef]
- Salai, M.; Brosh, T.; Blankstein, A.; Oran, A.; Chechik, A. Effect of changing the saddle angle on the incidence of low back pain in recreational bicyclists. Br. J. Sports Med. 1999, 33, 398–400. [Google Scholar] [CrossRef]
- Usabiaga, J.; Crespo, R.; Iza, I.; Aramendi, J.; Terrados, N.; Poza, J.J. Adaptation of the lumbar spine to different positions in bicycle racing. Spine 1997, 22, 1965–1969. [Google Scholar] [CrossRef]
- Marsden, M.; Schwellnus, M. Lower back pain in cyclists: A review of epidemiology, pathomechanics and risk factors. Int. Sport Med. J. 2010, 11, 216–225. [Google Scholar]
- Balasubramanian, V.; Jagannath, M.; Adalarasu, K. Muscle fatigue-based evaluation of bicycle design. Appl. Ergon. 2014, 45, 339–345. [Google Scholar] [CrossRef]
- Abt, J.P.; Smoliga, J.M.; Brick, M.J.; Jolly, J.T.; Lephart, S.M.; Fu, F.H. Relationship between cycling mechanics and core stability. J. Strength Cond. Res. 2007, 21, 1300–1304. [Google Scholar]
- Burnett, A.F.; Cornelius, M.W.; Dankaerts, W.; O’Sullivan, P.B. Spinal kinematics and trunk muscle activity in cyclists: A comparison between healthy controls and non-specific chronic low back pain subjects—A pilot investigation. Man. Ther. 2004, 9, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Muyor, J.M.; Alacid, F.; López-Miñarro, P.Á. Influence of hamstring muscles extensibility on spinal curvatures and pelvic tilt in highly trained cyclists. J. Hum. Kin. 2011, 29, 15–23. [Google Scholar] [CrossRef]
- Bressel, E.; Larson, B.J. Bicycle seat designs and their effect on pelvic angle, trunk angle, and comfort. Med. Sci. Sports Exerc. 2003, 35, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Wanich, T.; Hodgkins, C.; Columbier, J.A.; Muraski, E.; Kennedy, J.G. Cycling injuries of the lower extremity. JAAOS-J. Am. Acad. Orthopaedic. Surg. 2007, 15, 748–756. [Google Scholar] [CrossRef]
- Kotler, D.H.; Babu, A.N.; Robidoux, G. Prevention, evaluation, and rehabilitation of cycling-related injury. Curr. Sports Med. Rep. 2016, 15, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Salsich, G.B.; Ward, S.R.; Terk, M.R.; Powers, C.M. In vivo assessment of patellofemoral joint contact area in individuals who are pain free. Clin. Orthopaetics. Rel. Res. 2003, 417, 277–284. [Google Scholar] [CrossRef]
- Bailey, M.; Maillarder, F.; Messenger, N. Kinematics of cycling in relation to anterior knee pain and patellar tendinitis. J. Sports Sci. 2003, 21, 649–657. [Google Scholar] [CrossRef]
- Dieter, B.P.; McGowan, C.P.; Stoll, S.K.; Vella, C.A. Muscle activation patterns and patellofemoral pain in cyclists. Med. Sci. Sports Exerc. 2014, 46, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Tamborindeguy, A.C.; Bini, R.R. Does saddle height affect patellofemoral and tibiofemoral forces during bicycling for rehabilitation? J. Bodywork Mov. Ther. 2011, 15, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Fonda, B.; Babič, J.; Šarabon, N. The Medial-Lateral Pedal Force Component Correlates with Q-Angle during Steady-State Cycling at Different Workloads and Cadences. Appl. Sci. 2021, 11, 1004. [Google Scholar] [CrossRef]
- Farrell, K.C.; Reisinger, K.D.; Tillman, M.D. Force and repetition in cycling: Possible implications for iliotibial band friction syndrome. Knee 2003, 10, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Taunton, J.E.; Ryan, M.B.; Clement, D.B.; McKenzie, D.C.; Lloyd-Smith, D.R. A retrospective case-control analysis of 2002 injuries in competitive cyclists. Clin. J. Sport Med. 2002, 36, 95–101. [Google Scholar]
- Ménard, M.; Lacouture, P.; Domalain, M. Iliotibial Band Syndrome in Cycling: A combined experimental simulation approach assessing the effect of saddle setback. Int. J. Sports Phys. Ther. 2020, 15, 958–966. [Google Scholar] [CrossRef]
- Geisler, P.R. Current clinical concepts: Synthesizing the available evidence for improved clinical outcomes in iliotibial band impingement syndrome. J. Athl. Train. 2021, 56, 805–815. [Google Scholar] [CrossRef]
- Aderem, J.; Louw, Q.A. Biomechanical risk factors associated with iliotibial band syndrome in runners: A systematic review. BMC Musculoskelet. Dis. 2015, 16, 1–16. [Google Scholar] [CrossRef]
- Noehren, B.; Davis, I.; Hamill, J. ASB Clinical Biomechanics Award Winner 2006: Prospective study of the biomechanical factors associated with iliotibial band syndrome. Clin. Biomech. 2007, 22, 951–956. [Google Scholar] [CrossRef]
- Borgers, A.; Claes, S.; Vanbeek, N.; Claes, T. Etiology of knee pain in elite cyclists: A 14-month consecutive case series. Acta Orthop. Bel. 2020, 86, 262–271. [Google Scholar]
- Sanner, W.H.; O’Halloran, W.D. The biomechanics, etiology, and treatment of cycling injuries. J. Am. Podiatric Med. Assoc. 2000, 90, 354–376. [Google Scholar] [CrossRef] [PubMed]
- De Bernardo, N.; Barrios, C.; Vera, P.; Laíz, C.; Hadala, M. Incidence and risk for traumatic and overuse injuries in top-level road cyclists. J. Sports sci. 2012, 30, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Brand, A.; Sepp, T.; Klöpfer-Krämer, I.; Müßig, J.A.; Kröger, I.; Wackerle, H.; Augat, P. Upper body posture and muscle activation in recreational cyclists: Immediate effects of variable cycling setups. Res. Q. Exer. Sport 2019, 91, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Holliday, W.; Theo, R.; Fisher, J.; Swart, J. Cycling: Joint kinematics and muscle activity during differing intensities. Sports Biomech. 2019, 1–15. [Google Scholar] [CrossRef]
- Muyor, J.M.; Zabala, M. Road cycling and mountain biking produces adaptations on the spine and hamstring extensibility. Int. J. Sports Med. 2016, 37, 43–49. [Google Scholar] [CrossRef]
- Skovereng, K.; Aasvold, L.O.; Ettema, G.; Mourot, L. On the effect of changing handgrip position on joint specific power and cycling kinematics in recreational and professional cyclists. PLoS ONE 2020, 15, e0237768. [Google Scholar] [CrossRef]
- Caldwell, J.S.; McNair, P.J.; Williams, M. The effects of repetitive motion on lumbar flexion and erector spinae muscle activity in rowers. Clin. Biomech. 2003, 18, 704–711. [Google Scholar] [CrossRef]
- Olson, M.W.; Li, L.; Solomonow, M. Flexion-relaxation response to cyclic lumbar flexion. Clin. Biomech. 2004, 19, 769–776. [Google Scholar] [CrossRef]
- Muyor, J.M. The influence of handlebar-hands position on spinal posture in professional cyclists. J. Back Musc. Rehab. 2015, 28, 167–172. [Google Scholar] [CrossRef]
- Awad, M.A.; Gaither, T.W.; Murphy, G.P.; Chumnarnsongkhroh, T.; Metzler, I.; Sanford, T.; Sutcliffe, S.; Eisenberg, M.L.; Carroll, P.R.; Osterberg, E.C.; et al. Cycling, and male sexual and urinary function: Results from a large, multinational, cross-sectional study. J. Urol. 2018, 199, 798–804. [Google Scholar] [CrossRef]
- Balasubramanian, A.; Yu, J.; Breyer, B.N.; Minkow, R.; Eisenberg, M.L. The association between pelvic discomfort and erectile dysfunction in adult male bicyclists. J. Sex. Med. 2020, 17, 919–929. [Google Scholar] [CrossRef] [PubMed]
- Naňka, O.; Šedý, J.; Jarolim, L. Sulcus nervi dorsalis penis: Site of origin of Alcock’s syndrome in bicycle riders? Med. Hypotheses 2007, 69, 1040–1045. [Google Scholar] [CrossRef] [PubMed]
- Šedý, J.; Naňka, O.; Belišová, M.; Walro, J.M.; Jarolím, L. Sulcus nervi dorsalis penis/clitoridis: Anatomic structure and clinical significance. Eur. Urol. 2006, 50, 1079–1085. [Google Scholar] [CrossRef] [PubMed]
- Bini, R.; Hume, P.A.; Croft, J.L. Effects of bicycle saddle height on knee injury risk and cycling performance. Sports Med. 2011, 41, 463–476. [Google Scholar] [CrossRef]
- Bae, J.H.; Choi, J.S.; Kang, D.W.; Shin, Y.H.; Lee, J.H.; Tack, G.R. A study on lower limb joint angles and muscle activities during maximal and sub-maximal pedaling by saddle heights. In Proceedings of the 15th International Conference on Biomedical Engineering: ICBME 2013, Singapore, 4–7 December 2013; Springer International Publishing: Cham, Switzerland, 2014; pp. 748–751. [Google Scholar]
- de Moura, B.M.; Moro, V.L.; Rossato, M.; De Lucas, R.D.; Diefenthaeler, F. Effects of saddle height on performance and muscular activity during the Wingate test. J. Phys. Educ. (Maringa) 2017, 28, 1. [Google Scholar] [CrossRef]
- Verma, R.; Hansen, E.A.; De Zee, M.; Madeleine, P. Effect of seat positions on discomfort, muscle activation, pressure distribution and pedal force during cycling. J. Int. Soc. Electrophysiol. Kinesiol. 2016, 27, 78–86. [Google Scholar] [CrossRef]
- Diefenthaeler, F.; Bini, R.R.; Karolczak, A.P.B.; Carpes, F.P. Muscle activation during pedaling in different saddle position. Rev. Bras. Cinean. Des. Hum. 2008, 10, 161–169. [Google Scholar]
- Bassett, D.R.; Howley, E.T. Limiting factors for maximum oxygen uptake and determinants of endurance performance. Med. Sci. Sports Exerc. 2000, 32, 70–84. [Google Scholar] [CrossRef]
- Impellizzeri, F.M.; Marcora, S.M. The physiology of mountain biking. Sports Med. 2007, 37, 59–71. [Google Scholar] [CrossRef]
- Rankovic, G.; Mutavdzic, V.; Toskic, D.; Preljevic, A.; Kocic, M.; Nedin Rankovic, G.; Damjanovic, N. Aerobic capacity as an indicator in different kinds of sports. Bosn. J. Bas. Med. Sci. 2010, 10, 44–48. [Google Scholar] [CrossRef]
- Vandewalle, H. Oxygen uptake and maximal oxygen uptake: Interests and limits of their measurements. Ann. Réadaptation Méd. Phys. 2004, 47, 243–257. [Google Scholar] [CrossRef] [PubMed]
- Burnley, M.; Jones, A.M. Oxygen uptake kinetics as a determinant of sports performance. Eur. J. Sport Sci. 2007, 7, 63–79. [Google Scholar] [CrossRef]
- Joyner, M.J.; Coyle, E.F. Endurance exercise performance: The physiology of champions. J. Physiol. 2008, 586, 35–44. [Google Scholar] [CrossRef]
- Arriel, R.A.; Souza, H.L.; Sasaki, J.E.; Marocolo, M. Current perspectives of cross-country mountain biking: Physiological and mechanical aspects, evolution of bikes, accidents and injuries. Int. J. Environ. Res. Public Health 2022, 19, 12552. [Google Scholar] [CrossRef] [PubMed]
- Connick, M.J.; Li, F.X. The impact of altered task mechanics on timing and duration of eccentric bi-articular muscle contractions during cycling. J. Electrom. Kinesiol. 2013, 23, 223–229. [Google Scholar] [CrossRef]
- Ferrer-Roca, V.; Bescos, R.; Roig, A.; Galilea, P.; Valero, O.; Garcia-Lopez, J. Acute effects of small changes in bicycle saddle height on gross efficiency and lower limb kinematics. J. Strength Cond. Res. 2014, 28, 784–791. [Google Scholar] [CrossRef]
- Vrints, J.; Koninckx, E.; Van Leemputte, M.; Jonkers, I. The effect of saddle position on maximal power output and moment generating capacity of lower limb muscles during isokinetic cycling. J. Appl. Biomech. 2011, 27, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Galindo-Martínez, A.; López-Valenciano, A.; Vallés-González, J.M.; Elvira, J.L.L. Influencia del core en la producción de potencia en ciclistas. [Core influence on the power production in cyclists]. RICYDE. Rev. Int. Cienc. Dep. 2022, 18, 164–179. [Google Scholar] [CrossRef]
- Kruschewsky, A.B.; Dellagrana, R.A.; Rossato, M.; Ribeiro, L.F.P.; Lazzari, C.D.; Diefenthaeler, F. Saddle height and cadence effects on the physiological, perceptual, and affective responses of recreational cyclists. Perc. Motor Skills 2018, 125, 923–938. [Google Scholar] [CrossRef]
- Priego Quesada, J.I.; Perez-Soriano, P.; Lucas-Cuevas, A.G.; Salvador Palmer, R.; Cibrian Ortiz de Anda, R.M. Effect of bike-fit in the perception of comfort, fatigue and pain. J. Sports Sci. 2017, 35, 1459–1465. [Google Scholar] [CrossRef]
- Baino, F. Evaluation of the relationship between the body positioning and the postural comfort of non-professional cyclists: A new approach. J. Sports Med. Phys. Fit. 2011, 51, 59–65. [Google Scholar]
- Bini, R.R. Acute effects from changes in saddle height in perceived comfort during cycling. Int. J. Sports Sci. Coach. 2020, 15, 390–397. [Google Scholar] [CrossRef]

{kind=link}
| Amstar Items | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author(s) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | Score | Assessment Quality |
| Antequera-Vique et al. [30] | Yes | Yes * | No | Yes * | Yes | No | No | Yes | No | No | Not applicable | Not applicable | No | Yes | Not applicable | Yes | 44% (Moderate) | Critically Low |
| Bini and Bini. [31] | Yes | Yes * | Yes | Yes * | No | No | No | Yes * | Yes | No | Not applicable | Not applicable | No | Yes | Not applicable | No | 44% (Moderate) | Critically Low |
| Bini and Priego-Quesada [18] | Yes | Yes * | No | Yes * | Yes | No | No | Yes | Yes | No | Not applicable | Not applicable | Yes | Yes | Not applicable | Yes | 56% (Moderate) | Low quality |
| Johnston et al. [32] | Yes | Yes * | No | Yes * | No | Yes | No | Yes * | Yes | No | Not applicable | Not applicable | No | No | Not applicable | No | 38% (Low) | Critically Low |
| Litwinowicz et al. [33] | Yes | Yes * | No | Yes * | No | Yes | No | Yes* | Yes | No | Yes | No | No | No | No | Yes | 50% (Moderate) | Critically Low |
| Streisfeld et al. [34] | Yes | Yes * | No | Yes * | No | Yes | No | Yes * | Yes | No | Not applicable | Not applicable | No | No | Not applicable | No | 38% (Low) | Critically Low |
| Visentini et al. [35] | Yes | Yes * | Yes | Yes | Yes | Yes | No | Yes * | Yes | No | Not applicable | Not applicable | Yes | Yes | Not applicable | Yes | 69% (Moderate) | Low quality |
| Author(s) | Objectives | Type of Studies | No. of Studies | Participants Total/Range | Participants Characteristics | Evaluated Outcomes | Main Results and Conclusions |
|---|---|---|---|---|---|---|---|
| Antequera-Vique et al. [30] | To assess whether cycling affects spinal morphology in postures of the bicycle, such as adapting the spinal curvatures on the bicycle depending on the handlebar type and position on the handlebars. | Cross-sectional or longitudinal (experimental or cohorts) | 31 | 1518/3 to 128 | Competitive, recreational, master, and elite cyclists; Both genders; Road, mountain bike and triathlon; Non-cyclists and sedentary; Age 18–57 years. |
| Cycling posture influences spinal morphology and biomechanics:
|
| Bini & Bini [31] | To assess the main factors related to overuse knee-related pain and/or injuries in cyclists. | Cross-sectional; case studies; randomized controlled trials | 10 | 271/1 to 104 | Professional, competitive and recreational cyclists; Non-cyclists. |
| Cyclists with knee pain display distinct biomechanical and muscular activation patterns. Key observations include the following:
|
| Bini & Priego Quesada [18] | To assess the methods to determine bicycle saddle height and the effects of saddle height on cycling performance and injury risk outcomes. | Cross-sectional observational designs; cross-sectional randomized controlled trials; case study | 41 | n.a./1 to 142 | Both genders; Professional, competitive, recreational cyclists; Triathletes and non-cyclists. |
| The influence of saddle height on cycling performance and biomechanics is not yet fully understood. Key points include the following:
|
| Johnston et al. [32] | To determine the association between biomechanical factors and knee injury risk in cyclists. | Cross-sectional or longitudinal (experimental or cohorts) | 14 | 239/9 to 24 | Both genders; Age 19 to 50 years; Trained, competitive, amateur, experienced and recreational cyclists; Triathlon and non-cyclists; With or without knee pain or injury; |
| Several biomechanical factors influence knee pain and biomechanics in cyclists. Key findings include the following:
|
| Litwinowicz et al. [33] | To assess the effectiveness of strategies for reducing the impact of cycling on the perineum in healthy males. | Randomized controlled trials; crossover; before and after. | 22 | 601/9 to 100 | Only healthy males; |
| Different saddle designs and positions impact the cyclist’s perineum. Key findings include:
|
| Streisfeld et al. [34] | To determine whether relationships exist between body positioning, spinal kinematics, and muscle activity in active cyclists with nontraumatic low back pain. | Comparison studies; cross-sectional studies; case-based studies | 8 | 255/1 to 120 | Only men, aged 18 to 57 years; Weight: 54.43 to 72.57 kg; Height: 1.6 to 1.85 m; Elite, masters, professional competitive and unspecified cyclists. Professional off-road cyclists. With or without cycling experience. With or without low back pain. |
| Low back pain in cyclists is influenced by prolonged postures, muscle imbalances, and spinal mechanics. Key points include:
|
| Visentini et al. [35] | To identify risk factors associated with overuse injuries in cyclists. | Prospective cohort pretest–posttest design; epidemiological cohort studies; cross-sectional cohort study | 18 | 3881/n.a. | Recreational or elite cyclists on road, track, mountain, city/commuter, and time-trial bikes; Above 12 years old; With overuse pain and injury. |
| The relationship between cycling parameters and overuse injuries is not fully understood. Key findings include:
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vigário, P.C.; Ferreira, R.M.; Sampaio, A.R.; Martins, P.N. Effects of Saddle Position on Cycling: An Umbrella Review. Physiologia 2024, 4, 465-485. https://doi.org/10.3390/physiologia4040032
Vigário PC, Ferreira RM, Sampaio AR, Martins PN. Effects of Saddle Position on Cycling: An Umbrella Review. Physiologia. 2024; 4(4):465-485. https://doi.org/10.3390/physiologia4040032
Chicago/Turabian StyleVigário, Pedro Castro, Ricardo Maia Ferreira, António Rodrigues Sampaio, and Pedro Nunes Martins. 2024. "Effects of Saddle Position on Cycling: An Umbrella Review" Physiologia 4, no. 4: 465-485. https://doi.org/10.3390/physiologia4040032
APA StyleVigário, P. C., Ferreira, R. M., Sampaio, A. R., & Martins, P. N. (2024). Effects of Saddle Position on Cycling: An Umbrella Review. Physiologia, 4(4), 465-485. https://doi.org/10.3390/physiologia4040032