
LGBTQ2S+ Youth Perspectives on Mental Healthcare Provider Bias, Standards of Care, and Accountability



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Aim and Design
2.2. Study Sample and Setting
2.3. Data Analysis
3. Results
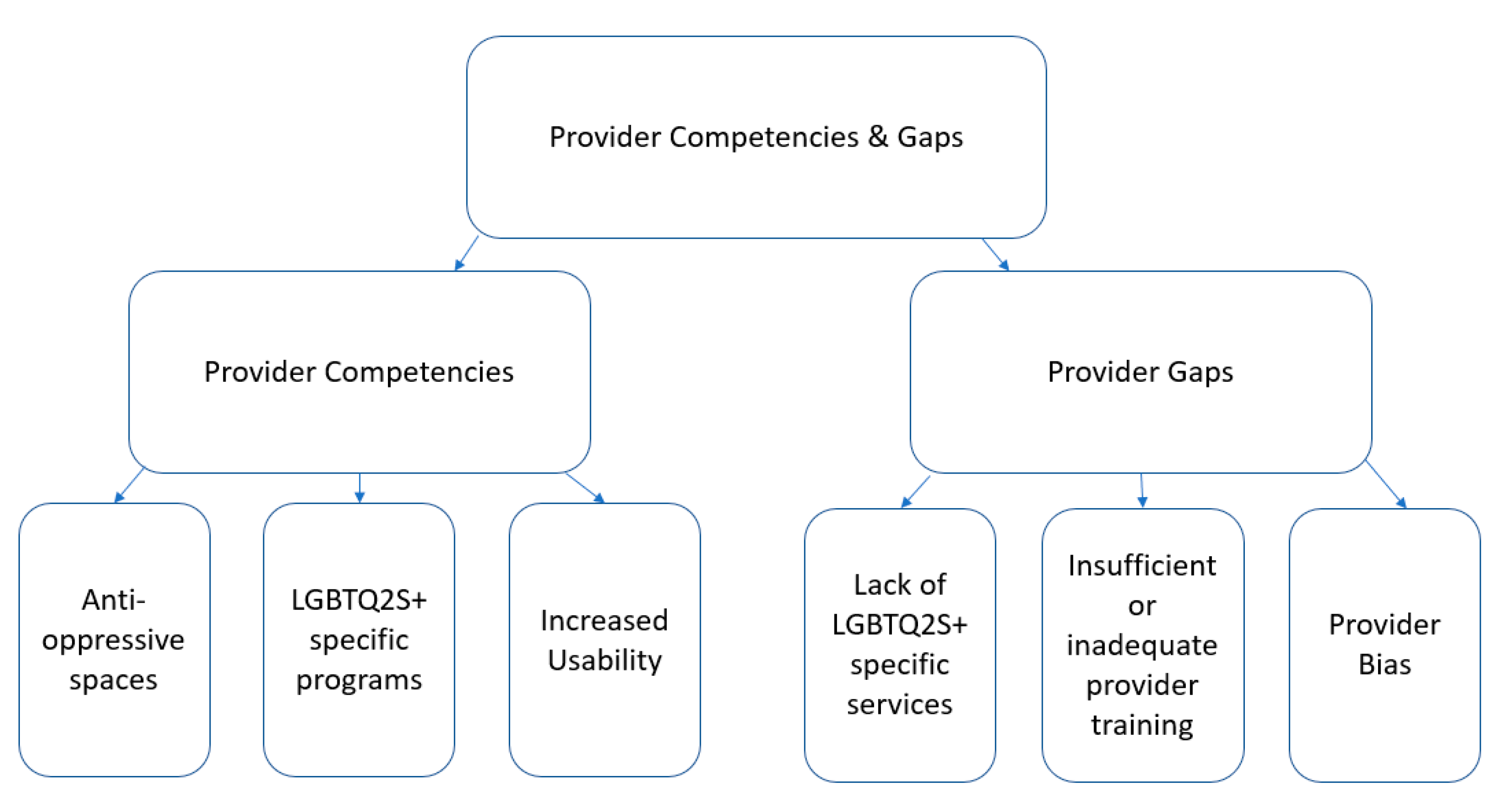
3.1. Provider Competencies and Gaps
3.1.1. Anti-Oppressive Spaces
3.1.2. LGBTQ2S+ Specific Programs
3.1.3. Virtual Usability
3.1.4. Lack of LGBTQ2S+ Specific Services
3.1.5. Insufficient and Inadequate Training
3.1.6. Provider Bias
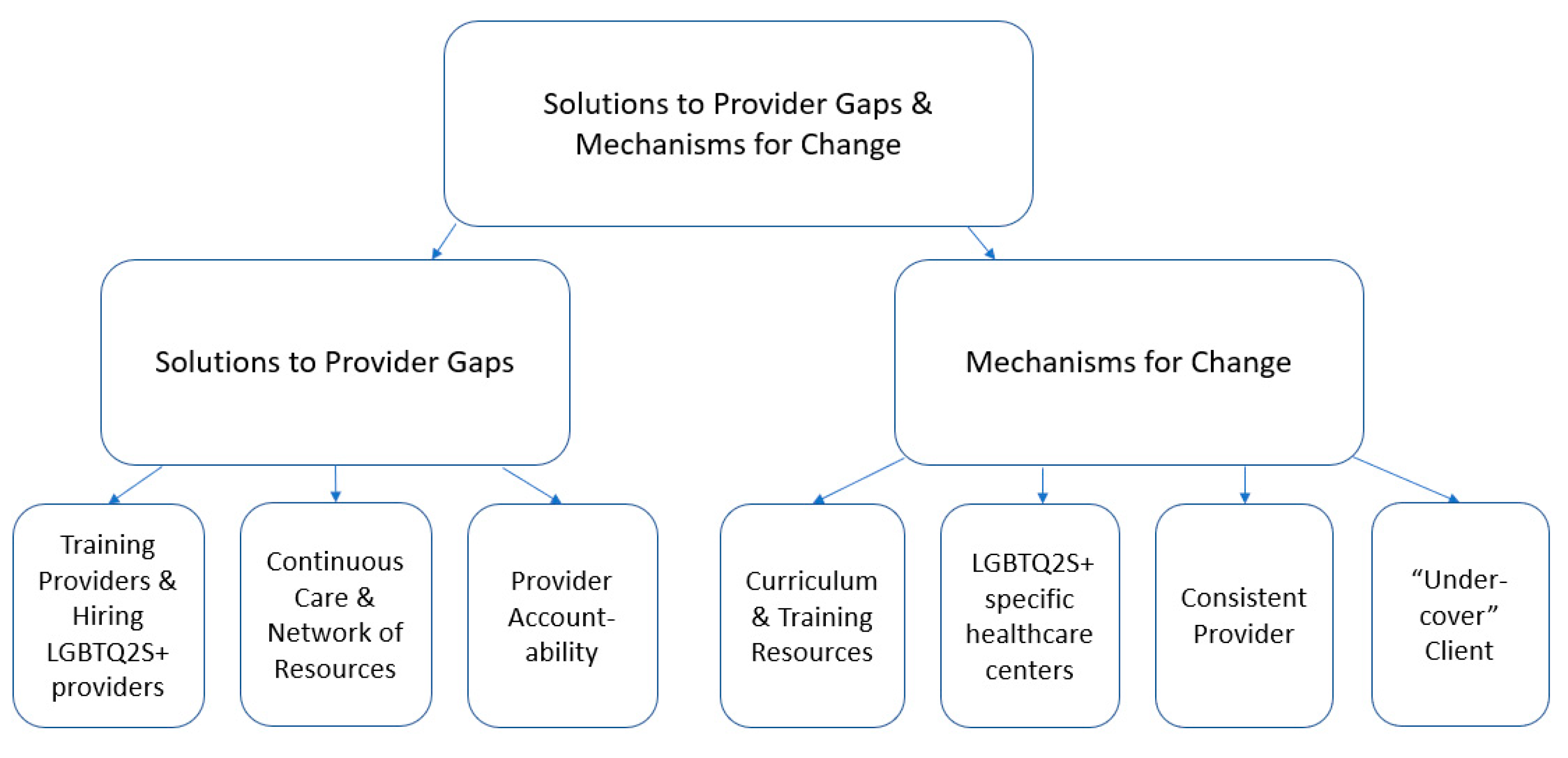
3.2. Solutions to Provider Gaps
3.2.1. Training Providers and Hiring LGBTQ2S+ Providers
3.2.2. Continuous Care and Network of Resources
3.2.3. Accountability
3.3. Mechanisms of Change
3.3.1. Updating Provider Training
3.3.2. LGBTQ2S+ Specific Healthcare Centre
3.3.3. Consistent Provider Model
3.3.4. Provider Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Structured Activities and Results in Sessions 2 and 3
Appendix A.1. Brainstorming
Appendix A.2. Idea Definition and Prototyping
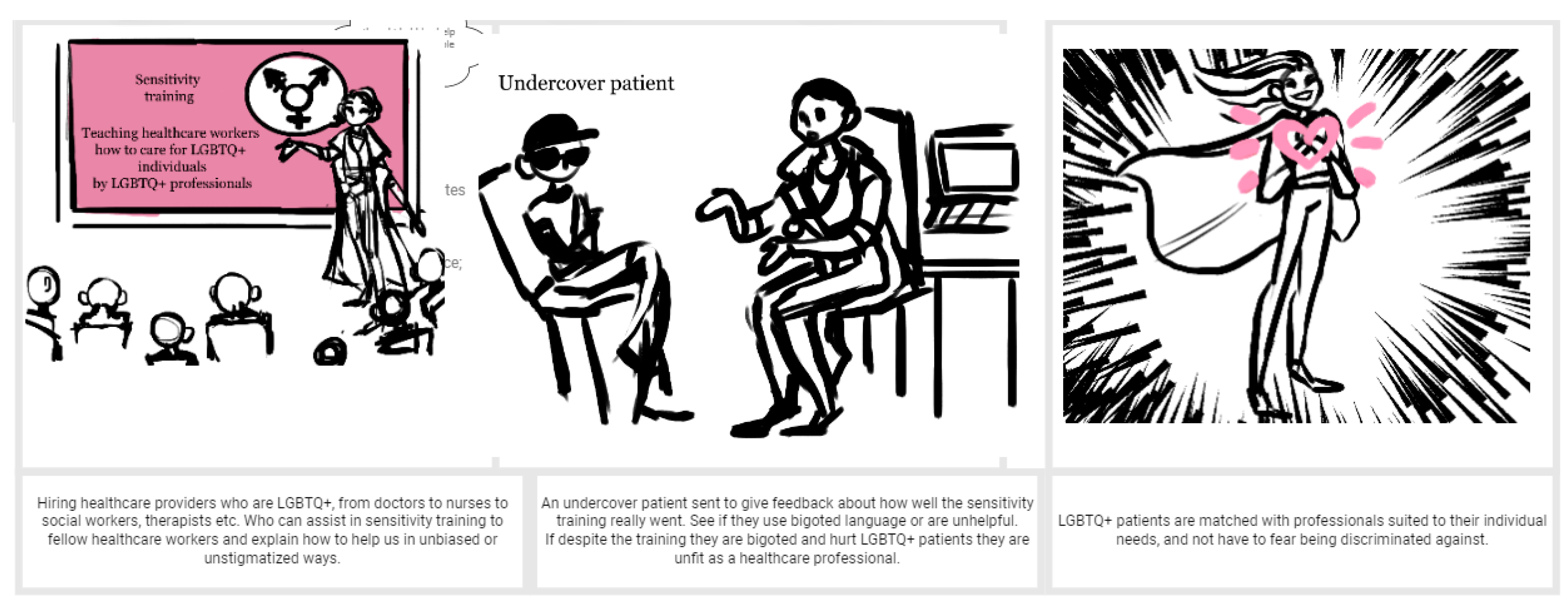
Appendix A.3. Concept Blueprint and Storyboard
Appendix A.3.1. Pre-Engagement
Appendix A.3.2. Engagement
Appendix A.3.3. Post-Engagement
References
- Almeida, J.; Johnson, R.M.; Corliss, H.L.; Molnar, B.E.; Azrael, D. Emotional Distress Among LGBT Youth: The Influence of Perceived Discrimination Based on Sexual Orientation. J. Youth Adolesc. 2009, 38, 1001–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, A. Scrambling for access: Availability, accessibility, acceptability and quality of healthcare for lesbian, gay, bisexual and transgender people in South Africa. BMC Int. Health Hum. Rights 2017, 17, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hillier, L.; Jones, T.; Monagle, M.; Overton, N.; Gahan, L.; Blackman, J.; Mitchell, A. Writing Themselves in 3: The Third National Study on the Sexual Health and Wellbeing of Same Sex Attracted and Gender Questioning Young People. 2010. Available online: https://apo.org.au/sites/default/files/resource-files/2010-11/apo-nid53195.pdf. (accessed on 21 December 2022).
- Smith, E.; Jones, T.; Ward, R.; Dixon, J.; Mitchell, A.; Hillier, L. From Blues to Rainbows: The Mental Health and Well-Being of Gender Diverse and Transgender Young People in Australia. 2014. Available online: https://www.latrobe.edu.au/__data/assets/pdf_file/0007/598804/from-blues-to-rainbows-report-sep2014.pdf (accessed on 21 December 2022).
- Kosciw, J.; Clark, C.; Truong, N.; Zongrone, A. GSLEN National School Climate Survey. 2019. Available online: https://files.eric.ed.gov/fulltext/ED608534.pdf (accessed on 21 December 2022).
- Jadva, V.; Guasp, A.; Bradlow, J.; Bower-Brown, S.; Foley, S. Predictors of Self-Harm and Suicide in LGBT Youth: The Role of Gender, Socio-Economic Status, Bullying and School Experience. J. Public Health 2021. [Google Scholar] [CrossRef] [PubMed]
- Adelson, S.; Miller, A.M.; Johnson, K.; Reid, G. What psychiatry can do to end LGBT conversion therapy. Lancet Psychiatry 2022, 9, e40. [Google Scholar] [CrossRef] [PubMed]
- Wallach, S.; Garner, A.; Howell, S.; Adamson, T.; Baral, S.; Beyrer, C. Address Exacerbated Health Disparities and Risks to LGBTQ+ Individuals during COVID-19. Health Hum. Rights 2020, 22, 313. [Google Scholar] [PubMed]
- Curtis, M.; Ryder, D. LGBT Teens, Social Media Use & Depressive Symptoms. Think. Matters Symp. Arch. 2019. Available online: https://digitalcommons.usm.maine.edu/thinking_matters/210 (accessed on 20 December 2022).
- Salerno, J.P.; Devadas, J.; Pease, M.; Nketia, B.; Fish, J.N. Sexual and Gender Minority Stress Amid the COVID-19 Pandemic: Implications for LGBTQ Young Persons’ Mental Health and Well-Being. Public Health Rep. 2020, 135, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Jones, T. Improving Services for Transgender and Gender Variant Youth: Research, Policy and Practice for Health and Social Care Professionals; Jessica Kingsley Publishers: Philadelphia, PA, USA, 2019. [Google Scholar]
- Jones, T. Policy and Gay, Lesbian, Bisexual, Transgender and Intersex Students; Springer International Publishing: Cham, Switzerland, 2015. [Google Scholar] [CrossRef]
- Toomey, R.B.; Ryan, C.; Diaz, R.M.; Russell, S.T. High School Gay–Straight Alliances (GSAs) and Young Adult Well-Being: An Examination of GSA Presence, Participation, and Perceived Effectiveness. Appl. Dev. Sci. 2011, 15, 175–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magritte, E.; Williams, J.; Amyot, E.; Usipuik, M.; Sanders, C. Listening to Individuals with Differences in Sex Development or Intersex and Their Families: “Not Doing Surgery Does Not Mean Doing Nothing. Horm. Res. Paediatr. 2022, 94, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jadwin-Cakmak, L.; Bauermeister, J.A.; Cutler, J.M.; Loveluck, J.; Sirdenis, T.K.; Fessler, K.B.; Popoff, E.E.; Benton, A.; Pomerantz, N.F.; Atkins, S.L.; et al. The Health Access Initiative: A Training and Technical Assistance Program to Improve Health Care for Sexual and Gender Minority Youth. J. Adolesc. Health 2020, 67, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Rees, S.N.; Crowe, M.; Harris, S. The lesbian, gay, bisexual and transgender communities’ mental health care needs and experiences of mental health services: An integrative review of qualitative studies. J. Psychiatr. Ment. Health Nurs. 2021, 28, 578–589. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | Percentage of Sample |
|---|---|
| Gender Identity | |
| Agender | 6% |
| Genderfluid | 9% |
| Genderqueer | 12% |
| Man | 6% |
| Non-binary | 24% |
| Trans man | 9% |
| Trans woman | 3% |
| Two-Spirit | 3% |
| Woman | 27% |
| Sexual Identity | |
| Asexual | 3% |
| Bisexual | 18% |
| Gay | 9% |
| Lesbian | 12% |
| Pansexual | 12% |
| Queer | 30% |
| Questioning | 3% |
| Straight/Heterosexual | 6% |
| Two-Spirit | 6% |
| Lived in Canada | |
| From birth | 82% |
| More than 10 years | 6% |
| 1–10 years | 12% |
| Highest level of education | |
| Some high school | 24% |
| High school diploma | 39% |
| More than high school | 33% |
| Employment Status | |
| Employee | 21% |
| Self-emp. | 6% |
| Working unpaid | 3% |
| Student | 36% |
| Long-term sick/disabled | 9% |
| Unemployed | 12% |
| Covid unemployed | 12% |
| Person Living with a Disability | |
| Yes | 55% |
| No | 45% |
| Race | |
| African Canadian/American | 3% |
| Black | 12% |
| Caribbean | 12% |
| East Asian | 3% |
| First Nations | 9% |
| Latin American | 3% |
| Métis | 6% |
| Middle Eastern | 6% |
| Multiracial/Mixed | 9% |
| South Asian | 12% |
| White | 24% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaiton, M.; Thorburn, R.; Sutton, M.; Feng, P. LGBTQ2S+ Youth Perspectives on Mental Healthcare Provider Bias, Standards of Care, and Accountability. Youth 2023, 3, 93-106. https://doi.org/10.3390/youth3010006
Chaiton M, Thorburn R, Sutton M, Feng P. LGBTQ2S+ Youth Perspectives on Mental Healthcare Provider Bias, Standards of Care, and Accountability. Youth. 2023; 3(1):93-106. https://doi.org/10.3390/youth3010006
Chicago/Turabian StyleChaiton, Michael, Rachel Thorburn, Megan Sutton, and Patrick Feng. 2023. "LGBTQ2S+ Youth Perspectives on Mental Healthcare Provider Bias, Standards of Care, and Accountability" Youth 3, no. 1: 93-106. https://doi.org/10.3390/youth3010006
APA StyleChaiton, M., Thorburn, R., Sutton, M., & Feng, P. (2023). LGBTQ2S+ Youth Perspectives on Mental Healthcare Provider Bias, Standards of Care, and Accountability. Youth, 3(1), 93-106. https://doi.org/10.3390/youth3010006