Abstract
This study aims to analyze the pressure on Italian public hospitals from the additional demand created by COVID-19. Starting from the analysis of regulatory interventions ordered by the central government in response to the emergency, this paper analyzes daily the trend of hospital beds and admissions in intensive care units from March to November 2020. The results revealed a critical situation in the system for meeting demand, with numerous regions operating beyond their capacity, especially in the first wave of the pandemic. The study presents two relevant messages. First, it is necessary to slow the spread of COVID-19 in the Italian population allowing more time for the reorganization of the supply and relieve the pressure on the health system: a third wave of the COVID-19 pandemic would cause the collapse of the national health system. Another suggestion regards the regionalized organization of health services: the design may be adequate in situations of routine demand but faces important challenges during pandemics.
1. Introduction
The new coronavirus (SARS-CoV-2 or COVID-19) outbreak appeared in Wuhan, China in December 2019 and rapidly was spread in Europe (EU) [1]. Italy was the first EU country to suffer severe effects of this virus diffusion, with a spiral of infections that placed this country at the top of the international rankings, overtaking China on 19 March 2020 [2,3].
The outbreak of COVID-19 in Italy officially started on 31 January 2020, after two Chinese visitors staying at a central hotel in Rome tested positive for the new coronavirus SARS-CoV-2 [4,5].
On 21 February, after a few days of increasing concern, a 38-year-old man was admitted to the hospital in Codogno, Lombardy, and was confirmed as the first Italian citizen with COVID-19 [4].
From there, in less than one week, the number of cases in Italy increased beyond expectations, putting the Italian health service under considerable strain; cases were found initially in several bordering regions and autonomous provinces of northern Italy and then gradually spread across all Italian regions [4].
One of the major consequences of the rapid spread of the virus has been the overload of hospitals, particularly in intensive care units (ICUs); the SARS-CoV-2 infection caused clusters of severe respiratory illness similar to severe acute respiratory syndrome coronavirus and was associated with ICU admission, mechanical ventilation and high mortality in older patients and those with medical comorbidities [6].
In this context, the central government has promoted new policies to contain the spread of the virus. The new decrees were initially intended for the “red zone” regions, then spread through the whole country (Table 1).

Table 1.
Measures adopted by the central government.
The measures introduced have not been enough to contain the further spread of the epidemic and the consequent overloading of hospital structures.
The need to face the epidemiological emergency from COVID-19 has forced the adoption of extraordinary and urgent measures aimed at strengthening the NHS, mainly introduced with the decree-laws of 9 March 2020 [7] and 17 March 2020 [8].
The decrees directly involve hospital structures. The main measures concerned:
- the strengthening of human resources. To address the urgent needs deriving from the diffusion of COVID-19, the entities of the National Health Service have been authorized to re-determine the plans of personnel needs and proceed with the consequent recruitment of health personnel. The increase in personnel concerned the hospital units most affected by the emergency (such as infectious and tropical diseases, emergency medicine, internal medicine, ICUs);
- the establishment of temporary health areas. Hospitals have activated temporary health areas both inside and outside of the structures, for the management of the COVID-19 emergency;
- the suspension of hospitalizations and non-urgent outpatient activities. For priority management of the coronavirus emergency, hospitals have been authorized to suspend or remodel non-urgent hospitalization and outpatient activities;
- the increase in beds. The emergency from COVID-19 required the immediate strengthening of the ICUs, especially in the most affected regions. The circular of 29 February 2020 n. 2619 of the Ministry of Health (whose recommendations were subsequently regulated by the decree-law of 9 March 2020) underlined the urgent need for the regions to prepare an emergency plan to guarantee suitable levels of treatment through an adequate number of intensive care beds. Subsequently, the circular of the Ministry of Health of 1 March 2020 n. 2627 (whose recommendations were subsequently regulated by decree-law n. 18 of 17 March 2020) required that, in the shortest possible time, an interregional cooperation model coordinated at the national level was activated, with the involvement of public and private accredited structures. At the regional level, the model envisaged an increase of 50 percent in the number of beds in ICUs and 100 percent in the pulmonary and infectious disease units.
This study aims to analyze the pressure on Italian public hospitals from the additional demand created by COVID-19. Specifically, the trend of hospital beds and admissions in ICUs from March to November 2020 was analyzed daily, highlighting the daily bed occupancy rate and the regions whose public hospitals have been subjected to increased pressure [9].
The paper is organized as follows:
2. Materials and Methods
This study analyzes the daily trend of ICU beds and admissions for COVID-19 in Italian public hospitals between 2 March and 30 November 2020 [9].
Data were obtained from the official website of the Italian Health Ministry (http://www.salute.gov.it/nuovocoronavirus, accessed on 15 December 2020) that reports information of COVID-19 infection in Italy, and from the website of the National Agency for Regional Health Services (Agenas—Agenzia Nazionale per i Servizi Sanitari Regionali) (https://www.agenas.gov.it/covid19/web/index.php, accessed on 15 December 2020) that contains information of hospital ICU bed trend in Italian regions.
3. Results
From March to November 2020, the number of beds in ICUs increased from 5213 to 7216 (Figure 1). The sudden emergency did not allow an immediate response from hospitals to the increase in cases. Until then, the organization of the Italian healthcare system was the result of a massive process of reform based on “managerialism” of healthcare. As a result, deep changes were made in the public healthcare offering, with a significant reduction in beds and health personnel. For this reason, the first months of the pandemic put public health facilities under great pressure. Starting from April, the national lockdown imposed in March allowed a reduction in cases, with a further decrease in the period between June and August. Starting from September 2020, the infections started to increase again. Public health structures, more prepared for a second wave of the epidemic, increased the number of beds in ICUs; between September and October, the number of beds went from 5889 to 7216. However, this has not prevented a new strong pressure on public health facilities.
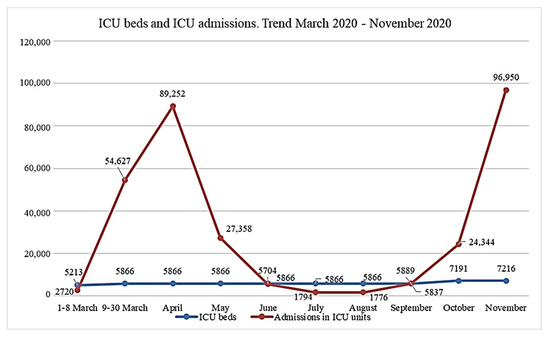
Figure 1.
Overall trend of beds and admissions.
The following table (Table 2) shows the pressure on public hospitals in the Italian regions. The hospital bed occupancy rates in ICUs were calculated daily; the table shows a summary of the results for each month (lowest bed occupancy rate, highest bed occupancy rate and the average value for each period/month). The month of March was divided into two subperiods: the period from 2 to 8 March, as in those days most regions did not report COVID-19 cases, and the period from 9 to 30 March, in which the sudden increase in cases led to an increase in the bed occupancy rate in all regions. In the analyzed period, the regions under the greatest pressure were Lombardy and the autonomous provinces of Trento and Bolzano, Marche, Piemonte, and Valle d’Aosta, especially in the first wave of the pandemic.
Table 2.
Hospital bed occupancy rates in ICUs.
In these regions, in the first months of the pandemic, the total daily number of ICU admissions exceeded the number of beds (Figure 2). However, in the same period, there was also a large number of discharges, but also deaths (for example, on 23 March 2020, Lombardy recorded a total of 1183 hospitalizations in intensive care, 983 beds. On the same day, the region reported 210 discharges and 320 deaths). In many cases, pressure on hospitals forced regions to take extraordinary measures. Regions responded to the lack of beds for patients with COVID-19 by sending patients who needed intensive care but were not infected with COVID-19 to hospitals outside of the region to contain the virus [2].
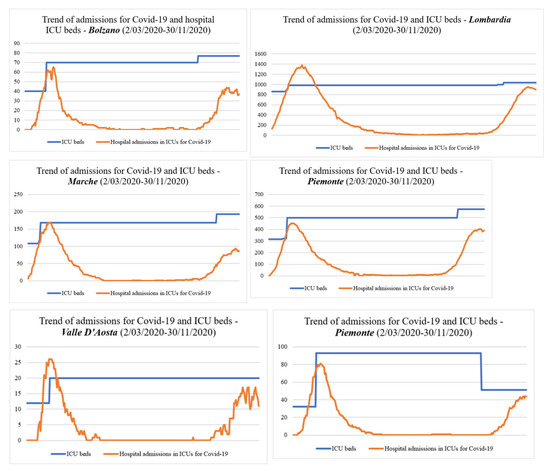
Figure 2.
Regions under pressure.
4. Discussion and Conclusions
This study analyzed the pressure on Italian public hospitals from the additional demand created by COVID-19, with a particular focus on public hospital ICUs. Starting from the analysis of regulatory interventions ordered by the central government in response to the emergency, this paper illustrated the daily trend of hospital beds and admissions in ICUs from 2 March to 30 November 2020. The results revealed a critical situation in the system for meeting demand, with numerous regions operating beyond their capacity. Especially in the first wave of the pandemic, the results have shown a strong increase in cases in regions where the supply of health services was not sufficiently prepared.
The study presents two relevant messages. First, it is necessary to slow the spread of COVID-19 in the Italian population allowing more time for the reorganization of the supply and relieve the pressure on the health system; a third wave of the COVID-19 pandemic would cause the collapse of the national health system. Another suggestion regards the regionalized organization of health services. Italy is used as a case study considering that (like in many other countries) a massive process of reform based on “managerialism” of healthcare is being carried out [10].
As a result:
- deep changes have been made in the public healthcare offering, with a significant reduction in beds and health personnel (this is one of the reasons why hospitals found themselves unprepared to face such an important health emergency [11]);
- responsibilities for healthcare have been decentralized to regions, though the central government still retains a key role in ensuring all citizens have uniform access to health services throughout the country [12]. During the COVID-19 emergency, the central government directly intervened by introducing specific measures with a direct impact on the healthcare system and hospital management.
The adopted measures have been aimed at increasing the production capacity of the INHS, showing that the regionalized organization of health services may be adequate in situations routine demand but faces important challenges during pandemics.
Supplementary Materials
The Supplementary Materials are available online at https://sciforum.net/event/ECERPH-3/keynote/ffa0b6660a369c0d7d50b35569e57da3/presentation_video/Paper%20presentation.mp4. Appendixes containing the data used for the analysis (daily admission in ICUs, public hospital ICU beds for each Italian region, discharges, deaths, hospital bed occupancy rates in ICUs, etc.) will be made available on request to the corresponding author at the following address: mgiancotti@unicz.it.
Funding
This research received no external funding.
Conflicts of Interest
The author declares no conflict of interest.
References
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and corona virus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed]
- Remuzzi, A.; Remuzzi, G. COVID-19 and Italy: What next? Lancet 2020, 395, 1225–1228. [Google Scholar] [CrossRef]
- Bontempi, E. The Europe second wave of COVID-19 infection and the Italy “strange” situation. Environ. Res. 2020, 193, 110476. [Google Scholar] [CrossRef] [PubMed]
- Carinci, F. Covid-19: Preparedness, decentralisation, and the hunt for patient zero. BMJ 2020, 368, 799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albarello, F.; Pianura, E.; Di Stefano, F.; Cristofaro, M.; Petrone, A.; Marchioni, L.; Campioni, P.; Eskild, P.; Zumla, A.; Ippolito, G.; et al. 2019-novel Coronavirus severe adult respiratory distress syndrome in two cases in Italy: An uncommon radiological presentation. Int. J. Infect. Dis. 2020, 93, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Möhlenkamp, S.; Thiele, H. Ventilation of COVID-19 patients in intensive care units. Herz 2020, 45, 329–331. [Google Scholar] [CrossRef] [PubMed]
- DECRETO-LEGGE 9 Marzo 2020, n. 14. Disposizioni Urgenti per il Potenziamento del Servizio Sanitario Nazionale in Relazione All’emergenza COVID-19. (20G00030) (GU Serie Generale n.62 del 09-03-2020). Available online: https://www.gazzettaufficiale.it/eli/id/2020/03/09/20G00030/sg (accessed on 1 November 2020).
- DECRETO-LEGGE 17 Marzo 2020, n. 18 Misure di Potenziamento del Servizio Sanitario Nazionale e di Sostegno Economico per Famiglie, Lavoratori e Imprese Connesse All’emergenza Epidemiologica da COVID-19. (20G00034) (GU Serie Generale n.70 del 17-03-2020). Available online: https://www.gazzettaufficiale.it/eli/id/2020/03/17/20G00034/sg (accessed on 1 November 2020).
- Mackay, M.; Lee, M. Choice of models for the analysis and forecasting of hospital beds. Health Care Manag. Sci. 2005, 8, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Anessi-Pessina, E.; Cantù, E. Whither managerialism in the Italian national health service? Int. J. Health Plan. Manag. 2006, 21, 327–355. [Google Scholar] [CrossRef] [PubMed]
- Mattiuzzi, C.; Lippi, G. Which lessons shall we learn from the 2019 novel coronavirus outbreak? Ann. Transl. Med. 2020, 8, 48. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, Regional Office for Europe. European Observatory on Health Systems and Policies. In Italy: Health System Review; Ferre, F., de Belvis, A.G., Valerio, L., Longhi, S., Lazzari, A., Fattore, G., Ricciardi, W., Maresso, A., Eds.; World Health Organization, Regional Office for Europe: Geneva, Switzerland, 2014. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).