
Autologous Graft in the Anterior Maxilla—A Case Report †


{kind=link}
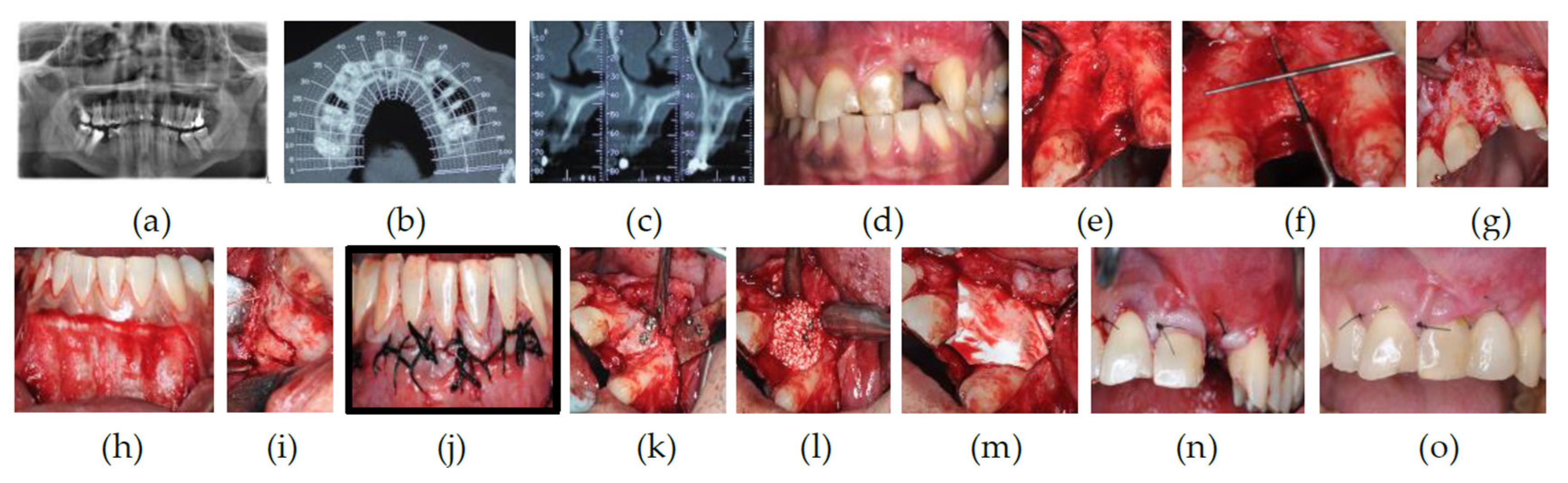
Abstract
:1. Introduction
2. Materials and Methods
3. Results and Discussion
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Danesh-Sani, S.; Engebretson, S.; Janal, M. Histomorphometric results of different grafting materials and effect of healing time on bone maturation after sinus floor augmentation: A systematic review and meta-analysis. J. Periodont Res. 2016, 52, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Khoury, F.; Hanser, T. Mandibular Bone Block Harvesting from the Retromolar Region: A 10-Year Prospective Clinical Study. Int. J. Oral Maxillofac. Implants 2015, 30, 688–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reininger, D.; Cobo-Vazquez, C.; Monteserin-Matesanz, M.; Lopez-Quiles, J. Complications in the use of the mandibular body, ramus and symphysis as donor sites in bone graft surgery. A systematic review. Medicina Oral Patologia Oral y Cirugia Bucal. 2016, 21, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Pourabbas, R.; Nezafati, S. Clinical results of localized alveolar ridge augmentation with bone grafts harvested from symphysis in comparison with ramus. J. Dent. Res. Dent. Clin. Dent. Prospect. 2007, 1, 7–12. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaz, R.; Gameiro, P.; Sottomayor, P.; Saldanha, B.; Rodrigues, P. Autologous Graft in the Anterior Maxilla—A Case Report. Med. Sci. Forum 2021, 5, 36. https://doi.org/10.3390/msf2021005036
Vaz R, Gameiro P, Sottomayor P, Saldanha B, Rodrigues P. Autologous Graft in the Anterior Maxilla—A Case Report. Medical Sciences Forum. 2021; 5(1):36. https://doi.org/10.3390/msf2021005036
Chicago/Turabian StyleVaz, Rodolfo, Pedro Gameiro, Pedro Sottomayor, Bernardo Saldanha, and Pedro Rodrigues. 2021. "Autologous Graft in the Anterior Maxilla—A Case Report" Medical Sciences Forum 5, no. 1: 36. https://doi.org/10.3390/msf2021005036
APA StyleVaz, R., Gameiro, P., Sottomayor, P., Saldanha, B., & Rodrigues, P. (2021). Autologous Graft in the Anterior Maxilla—A Case Report. Medical Sciences Forum, 5(1), 36. https://doi.org/10.3390/msf2021005036