
A Multi-Level Analysis of Biological, Social, and Psychological Determinants of Substance Use Disorder and Co-Occurring Mental Health Outcomes



Abstract
:1. Introduction
1.1. Psychoactive Substances and Addiction
1.2. Gender Differences
1.3. Age Differences
1.4. Comorbidity with Psychiatric Symptoms
1.5. Aim of this Study
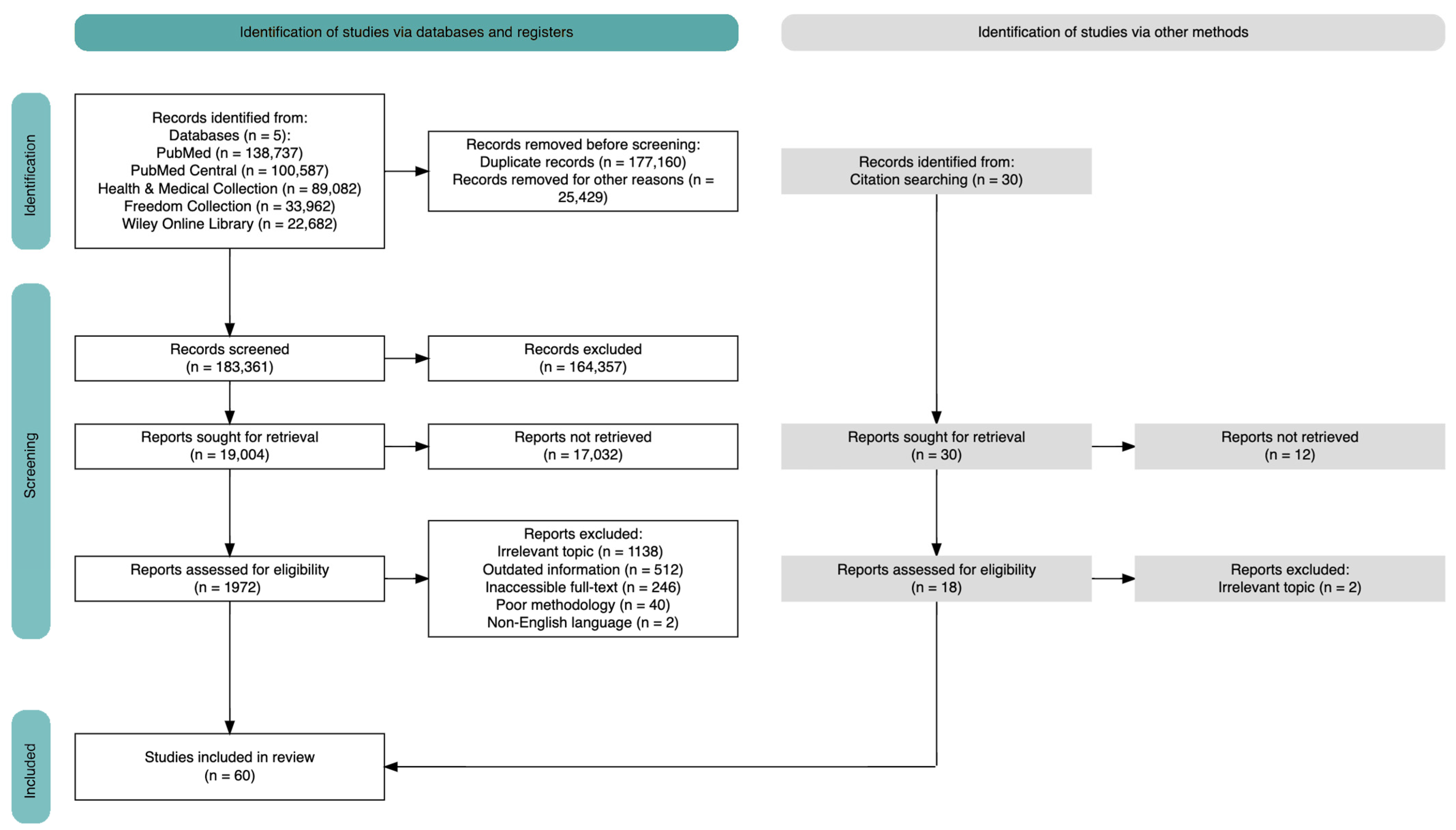
2. Materials and Methods
- (((substance use disorder) OR (addiction)) AND (psychiatric symptoms)) AND ((neurobiological factors) OR (genetic influences) OR (pharmacological factors));
- (((substance use disorder) OR (addiction)) AND (psychiatric symptoms)) AND ((mental health) OR (psychological factors) OR (cognitive processes));
- (((substance use disorder) OR (addiction)) AND (psychiatric symptoms)) AND ((family dynamics) OR (peer influence) Or (cultural norms));
- (((substance use disorder) OR (addiction)) AND (development) OR (progression patterns) OR (risk and protective factors)).
Eligibility Criteria
- All studies and reviews were published in indexed journals such as PubMed, PubMed Central, Health & Medical Collection, ScienceDirect Freedom Collection 2021, Wiley Online Library;
- Studies that included the keywords used and/or related to their topic;
- Studies that were published from the year 2022 on. The year 2022 was selected to provide sources as recent as possible that could include, but were not exclusively focused on, elements related to the COVID-19 pandemic lapse.
3. Results
Characteristics of Included Studies
4. Biological Factors
4.1. Cannabis Addiction
Genetic and Neurobiological Factors
4.2. Opioid Addiction
Genetic and Neurobiological Factors
4.3. Stimulant Addiction
Genetic and Neurobiological Factors
4.4. Hallucinogens Addiction
Genetic and Neurobiological Factors
4.5. Pharmacology and Treatment Insights on SUD
5. Psychological Factors
5.1. Complex Entanglement: Substance Use Disorder; Personality; and Psychopathology
5.2. Mental Health Conditions
5.2.1. Personality Factors and Addiction
5.2.2. Anxiety and Addiction
5.2.3. Mood Disorders and Addiction
5.2.4. ADHD and SUD
5.2.5. Traumatic Events, PTSD, and SUD
5.2.6. SUD and ASD
5.2.7. Self-Harm and Suicide Risk in People with SUD
6. Social Factors
6.1. Childhood
6.2. Adolescence
6.3. Adulthood
6.4. Social Background
7. Progression Patterns and Factors of Risk and Protection
7.1. Risk and Protection Factors
7.1.1. Impaired Illness Awareness
7.1.2. Transitional Age Youth (TAY)
7.1.3. Preexisting Mental Disorders
7.1.4. Socioeconomic Position
7.1.5. Physical Activity and Peer Interactions
7.1.6. Use Aimed at Increasing Sexual Performance
7.1.7. Media Representation of Drugs
7.1.8. Correlation between Risk and Protection Factors
8. Interactions between Psychological, Social, and Biological Factors
8.1. A Biopsychosocial Model for Understanding Addiction
8.2. Family History, Role Models, and Psychological Factors
8.3. Neurological Factors, Genetic Predispositions, and Personality Traits
8.4. Psychological Factors and Treatment Success Expectations
9. Discussion
9.1. Future Research
9.2. Limitations
10. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Drug Report 2023. Available online: www.unodc.org/unodc/en/data-and-analysis/world-drug-report-2023.html (accessed on 4 February 2024).
- Mefodeva, V.; Carlyle, M.; Walter, Z.; Chan, G.; Hides, L. Polysubstance Use in Young People Accessing Residential and Day-treatment Services for Substance Use: Substance Use Profiles, Psychiatric Comorbidity and Treatment Completion. Addiction 2022, 117, 3110–3120. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5-TR, 5th ed.; Text Revision; American Psychiatric Association Publishing: Washington, DC, USA, 2022; ISBN 978-0-89042-577-0. [Google Scholar]
- Nath, A.; Choudhari, S.G.; Dakhode, S.U.; Rannaware, A.; Gaidhane, A.M. Substance Abuse Amongst Adolescents: An Issue of Public Health Significance. Cureus 2022, 14, e31193. [Google Scholar] [CrossRef] [PubMed]
- National Institute on Drug Abuse. Psychedelic and Dissociative Drugs|National Institute on Drug Abuse (NIDA). Available online: https://nida.nih.gov/research-topics/psychedelic-dissociative-drugs (accessed on 8 February 2024).
- National Institute on Drug Abuse. Monitoring the Future|National Institute on Drug Abuse (NIDA). Available online: https://nida.nih.gov/research-topics/trends-statistics/monitoring-future (accessed on 8 February 2024).
- Epidemia dei Nuovi Tossicodipendenti Endovena: Ritorno al Passato? Available online: https://www.readfiles.it/pages/Archivio/Epidemia-dei-nuovi-tossicodipendenti-endovena-ritorno-al-passato-idA5 (accessed on 4 February 2024).
- National Institute on Drug Abuse. What Is Cocaine?|National Institute on Drug Abuse (NIDA). Available online: https://nida.nih.gov/publications/research-reports/cocaine/what-cocaine (accessed on 8 February 2024).
- United Nations Office on Drugs and Crime. Global Report on Cocaine 2023; United Nations Office on Drugs and Crime: Vienna, Austria, 2023. [Google Scholar]
- Iftikhar, M.; Riaz, D.S. Psycho-Social and Morbidity of Substance Use Disorder in Women. Int. J. Innov. Sci. Technol. 2022, 4, 82–87. [Google Scholar] [CrossRef]
- Efrati, Y.; Goldman, K.; Levin, K.; Rosca, P. Early-Life Trauma, Negative and Positive Life Events, Compulsive Sexual Behavior Disorder and Risky Sexual Action Tendencies among Young Women with Substance Use Disorder. Addict. Behav. 2022, 133, 107379. [Google Scholar] [CrossRef] [PubMed]
- Daigre, C.; Grau-López, L.; Palma-Alvarez, R.F.; Perea-Ortueta, M.; Sorribes-Puertas, M.; Serrano-Pérez, P.; Quesada, M.; Segura, L.; Coronado, M.; Ramos-Quiroga, J.A.; et al. A Multicenter Study on the Impact of Gender, Age, and Dual Diagnosis on Substance Consumption and Mental Health Status in Outpatients Treated for Substance Use Disorders During COVID-19 Lockdown. J. Dual Diagn. 2022, 18, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Chen, Y.; Li, H.; Zhang, X.; Xu, Y.; Ding, Z.-H.; Ma, Z.; Sun, Y. Association Between Psychiatric Symptoms and Craving in Drug Withdrawal. Int. J. Ment. Health Addict. 2023, 21, 3174–3184. [Google Scholar] [CrossRef]
- Chen, L.-Y.; Chen, C.-K.; Chen, C.-H.; Chang, H.-M.; Huang, M.-C.; Xu, K. Association of Craving and Depressive Symptoms in Ketamine-Dependent Patients Undergoing Withdrawal Treatment. Am. J. Addict. 2020, 29, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Haddaway, N.R.; Page, M.J.; Pritchard, C.C.; McGuinness, L.A. PRISMA2020: An R Package and Shiny App for Producing PRISMA 2020-compliant Flow Diagrams, with Interactivity for Optimised Digital Transparency and Open Synthesis. Campbell Syst. Rev. 2022, 18, e1230. [Google Scholar] [CrossRef]
- Navarrete, F.; García-Gutiérrez, M.; Gasparyan, A.; Navarro, D.; López-Picón, F.; Morcuende, Á.; Femenía, T.; Manzanares, J. Biomarkers of the Endocannabinoid System in Substance Use Disorders. Biomolecules 2022, 12, 396. [Google Scholar] [CrossRef]
- Schacht, J.P.; Hutchison, K.E.; Filbey, F.M. Associations between Cannabinoid Receptor-1 (CNR1) Variation and Hippocampus and Amygdala Volumes in Heavy Cannabis Users. Neuropsychopharmacology 2012, 37, 2368–2376. [Google Scholar] [CrossRef] [PubMed]
- Arias Horcajadas, F.; Dávila Píriz, J.R.; Parra González, A.; Sánchez Romero, S.; Sánchez-Morla, E.; Ampuero Sánchez, I.; Ramos Atance, J.A. Cannabinoid Receptor Type 2 Gene is Associated with Comorbidity of Schizophrenia and Cannabis Dependence and Fatty Acid Amide Hydrolase Gene is Associated with Cannabis Dependence in the Spanish Population.|Adicciones|EBSCOhost. Available online: https://openurl.ebsco.com/contentitem/gcd:161894901?sid=ebsco:plink:crawler&id=ebsco:gcd:161894901 (accessed on 20 February 2024).
- Manza, P.; Yuan, K.; Shokri-Kojori, E.; Tomasi, D.; Volkow, N.D. Brain Structural Changes in Cannabis Dependence: Association with MAGL. Mol. Psychiatry 2020, 25, 3256–3266. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, S.; Egerton, A.; Kim, E.; Rosso, L.; Riano Barros, D.; Hammers, A.; Brammer, M.; Turkheimer, F.E.; Howes, O.D.; McGuire, P. Acute Induction of Anxiety in Humans by Delta-9-Tetrahydrocannabinol Related to Amygdalar Cannabinoid-1 (CB1) Receptors. Sci. Rep. 2017, 7, 15025. [Google Scholar] [CrossRef] [PubMed]
- Viganò, D.; Grazia Cascio, M.; Rubino, T.; Fezza, F.; Vaccani, A.; Di Marzo, V.; Parolaro, D. Chronic Morphine Modulates the Contents of the Endocannabinoid, 2-Arachidonoyl Glycerol, in Rat Brain. Neuropsychopharmacology 2003, 28, 1160–1167. [Google Scholar] [CrossRef] [PubMed]
- Zuo, L.; Kranzler, H.R.; Luo, X.; Yang, B.; Weiss, R.; Brady, K.; Poling, J.; Farrer, L.; Gelernter, J. Interaction between Two Independent CNR1 Variants Increases Risk for Cocaine Dependence in European Americans: A Replication Study in Family-Based Sample and Population-Based Sample. Neuropsychopharmacology 2009, 34, 1504–1513. [Google Scholar] [CrossRef] [PubMed]
- Jordan, C.; Xi, Z. Identification of the Risk Genes Associated with Vulnerability to Addiction: Major Findings from Transgenic Animals. Front. Neurosci. 2022, 15, 811192. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Li, H.; Wang, L.; Zhang, J.; Liu, C.; Wan, X.; Liu, X.; Hu, Y.; Fang, Q.; Xiao, Y.; et al. Endocannabinoid Signaling Regulates the Reinforcing and Psychostimulant Effects of Ketamine in Mice. Nat. Commun. 2020, 11, 5962. [Google Scholar] [CrossRef]
- Vasiliu, O. Current Trends and Perspectives in the Immune Therapy for Substance Use Disorders. Front. Psychiatry 2022, 13, 882491. [Google Scholar] [CrossRef]
- Uhl, G.R.; Koob, G.F.; Cable, J. The Neurobiology of Addiction. Ann. N. Y. Acad. Sci. 2019, 1451, 5–28. [Google Scholar] [CrossRef]
- Bozkurt, M. Neuroscientific Basis of Treatment for Substance Use Disorders. Noro Psikiyatri Arsivi 2022, 59 (Suppl. 1), 75–80. [Google Scholar] [CrossRef]
- Volkow, N.D.; Boyle, M. Neuroscience of Addiction: Relevance to Prevention and Treatment. Am. J. Psychiatry 2018, 175, 729–740. [Google Scholar] [CrossRef] [PubMed]
- Poon, J.Y.K.; Hu, H.; Lam, M.; Lui, S.S.Y.; Chan, R.C.K. The Interplay between Addictive Behaviour and Psychopathology and Personality in Substance Use Disorder: A Network Analysis in Treatment-Seeking Patients with Alcohol and Drug Use. Int. J. Ment. Health Addict. 2022. [Google Scholar] [CrossRef]
- Santens, E.; Dom, G.; Dierckx, E.; Claes, L. Reactive and Regulative Temperament in Relation to Clinical Symptomatology and Personality Disorders in Patients with a Substance Use Disorder. J. Clin. Med. 2022, 11, 591. [Google Scholar] [CrossRef] [PubMed]
- Santens, E.; Dom, G.; Dierckx, E.; Claes, L. The Role of Effortful Control in Substance Use Disorders. Eur. Psychiatry 2022, 65, S51. [Google Scholar] [CrossRef]
- Buică, A.M.; Preda, D.M.; Andrei, L.E.; Stancu, M.; Gică, N.; Rad, F. Maladaptive Personality Traits in a Group of Patients with Substance Use Disorder and ADHD. Med. Kaunas Lith. 2022, 58, 962. [Google Scholar] [CrossRef]
- Basedow, L.A.; Wiedmann, M.F.; Roessner, V.; Golub, Y.; Kuitunen-Paul, S. Coping Motives Mediate the Relationship between PTSD and MDMA Use in Adolescents with Substance Use Disorders. Addict. Sci. Clin. Pract. 2022, 17, 46. [Google Scholar] [CrossRef] [PubMed]
- McKowen, J.; Woodward, D.; Yule, A.M.; DiSalvo, M.; Rao, V.; Greenbaum, J.; Joshi, G.; Wilens, T.E. Characterizing Autistic Traits in Treatment-seeking Young Adults with Substance Use Disorders. Am. J. Addict. 2022, 31, 108–114. [Google Scholar] [CrossRef] [PubMed]
- López-Toro, E.; Wolf, C.J.H.; González, R.A.; van den Brink, W.; Schellekens, A.; Vélez-Pastrana, M.C.; AFP Working Collaborative Group. Network Analysis of DSM Symptoms of Substance Use Disorders and Frequently Co-Occurring Mental Disorders in Patients with Substance Use Disorder Who Seek Treatment. J. Clin. Med. 2022, 11, 2883. [Google Scholar] [CrossRef] [PubMed]
- Er, S.; Buzlu, S. The Relationships between Self-transcendence and Depressive Symptoms, Self-esteem, and Locus of Control in Individuals Diagnosed with Substance Addiction. Perspect. Psychiatr. Care 2022, 58, 2137–2144. [Google Scholar] [CrossRef]
- Mustonen, A.; Rodriguez, A.; Scott, J.G.; Vuori, M.; Hurtig, T.; Halt, A.; Miettunen, J.; Alakokkare, A.; Niemelä, S. Attention Deficit Hyperactivity and Oppositional Defiant Disorder Symptoms in Adolescence and Risk of Substance Use Disorders—A General Population-based Birth Cohort Study. Acta Psychiatr. Scand. 2023, 148, 277–287. [Google Scholar] [CrossRef]
- Vekaria, V.; Patra, B.G.; Xi, W.; Murphy, S.M.; Avery, J.; Olfson, M.; Pathak, J. Association of Opioid or Other Substance Use Disorders with Health Care Use among Patients with Suicidal Symptoms. J. Subst. Use Addict. Treat. 2024, 156, 209177. [Google Scholar] [CrossRef] [PubMed]
- Andersson, H.W.; Mosti, M.P.; Nordfjærn, T. Suicidal Ideation among Inpatients with Substance Use Disorders: Prevalence, Correlates and Gender Differences. Psychiatry Res. 2022, 317, 114848. [Google Scholar] [CrossRef] [PubMed]
- Grinspoon, P. Poverty, Homelessness, and Social Stigma Make Addiction More Deadly. Available online: https://www.health.harvard.edu/blog/poverty-homelessness-and-social-stigma-make-addiction-more-deadly-202109282602 (accessed on 28 March 2024).
- Stewart, S.; Copeland, A.; Cherry, K. Risk Factors for Substance Use across the Lifespan. J. Genet. Psychol. 2022, 184, 145–162. [Google Scholar] [CrossRef] [PubMed]
- Mulhern, J.P. Consideration of Social Determinants Risks in Substance Use Disorder Assessment and Treatment Plan Formulation. J. Addict. Nurs. 2022, 33, 200–202. [Google Scholar] [CrossRef] [PubMed]
- Pomrenze, M.; Paliarin, F.; Maiya, R. Friend of the Devil: Negative Social Influences Driving Substance Use Disorders. Front. Behav. Neurosci. 2022, 16, 836996. [Google Scholar] [CrossRef] [PubMed]
- Stillman, M.A.; Daddis, S.T. Portrayal of Substance Use in Media and Its Effects on Substance Use Disorders among Youth. Addict. Subst. Abuse 2022, 1, 1–2. [Google Scholar] [CrossRef]
- Maxwell, A.M.; Harrison, K.; Rawls, E.; Zilverstand, A. Gender Differences in the Psychosocial Determinants Underlying the Onset and Maintenance of Alcohol Use Disorder. Front. Neurosci. 2022, 16, 808776. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, S.; Abdelmonem, R.; Hassan, S. Relationship between Self-Efficacy, Social Support and Treatment Motivation among Addict Patients. Minia Sci. Nurs. J. 2022, 012, 106–113. [Google Scholar] [CrossRef]
- Dalton, K. Matching Treatment to Development: Emerging Adults and Substance-Use Disorder; Memorial University of Newfoundland: St. John’s, NL, Canada, 2019. [Google Scholar]
- Kim, J.; Kambari, Y.; Taggar, A.; Quilty, L.C.; Selby, P.; Caravaggio, F.; Ueno, F.; Torres, E.; Song, J.; Pollock, B.G.; et al. A Measure of Subjective Substance Use Disorder Awareness—Substance Use Awareness and Insight Scale (SAS). Drug Alcohol Depend. 2022, 231, 109129. [Google Scholar] [CrossRef]
- Köck, P.; Meyer, M.; Elsner, J.; Dürsteler, K.M.; Vogel, M.; Walter, M. Co-Occurring Mental Disorders in Transitional Aged Youth With Substance Use Disorders—A Narrative Review. Front. Psychiatry 2022, 13, 827658. [Google Scholar] [CrossRef]
- Matson, P.A.; Ridenour, T.; Ialongo, N.; Spoth, R.; Prado, G.; Hammond, C.J.; Hawkins, J.D.; Adger, H. State of the Art in Substance Use Prevention and Early Intervention: Applications to Pediatric Primary Care Settings. Prev. Sci. 2022, 23, 204–211. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, L.; Elam, K.K.; Quinn, P.D.; Adams, S.; Chirica, M.G.; Klonsky, E.D.; Pettersson, E.; Lundström, S.; Larsson, H.; Lichtenstein, P.; et al. Examining Protective Factors for Substance Use Problems and Self-Harm Behavior during Adolescence: A Longitudinal Co-Twin Control Study. Dev. Psychopathol. 2022, 34, 1781–1802. [Google Scholar] [CrossRef]
- Abram, K.M.; Zwecker, N.A.; Welty, L.J.; Hershfield, J.A.; Dulcan, M.K.; Teplin, L.A. Comorbidity and Continuity of Psychiatric Disorders in Youth After Detention: A Prospective Longitudinal Study. JAMA Psychiatry 2015, 72, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Allebeck, P.; Burstöm, B.; Danielsson, A.-K.; Degenhardt, L.; Eikemo, T.A.; Ferrari, A.; Knudsen, A.K.; Lundin, A.; Manhica, H.; et al. Educational Level and the Risk of Mental Disorders, Substance Use Disorders and Self-Harm in Different Age-Groups: A Cohort Study Covering 1,6 Million Subjects in the Stockholm Region. Int. J. Methods Psychiatr. Res. 2023, 32, e1964. [Google Scholar] [CrossRef] [PubMed]
- Castelpietra, G.; Knudsen, A.K.S.; Agardh, E.E.; Armocida, B.; Beghi, M.; Iburg, K.M.; Logroscino, G.; Starace, F.; Steel, N.; Addolorato, G.; et al. The Burden of Mental Disorders, Substance Use Disorders and Self-Harm among Young People in Europe, 1990–2019: Findings from the Global Burden of Disease Study 2019. Lancet Reg. Health Eur. 2022, 16, 100341. [Google Scholar] [CrossRef]
- Solfrank, M.; Nikendei, C.; Zehetmair, C.; Friederich, H.-C.; Nagy, E. The Burden of Substance Use and (Mental) Distress among Asylum Seekers: A Cross Sectional Study. Front. Psychiatry 2023, 14, 1258140. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.P.; Tucker, J.S.; Dunbar, M.; Seelam, R.; D’Amico, E.J. Poly-Victimization and Opioid Use during Late Adolescence and Young Adulthood: Health Behavior Disparities and Protective Factors. Psychol. Addict. Behav. 2022, 36, 440–451. [Google Scholar] [CrossRef]
- Jepsen, D.; Luck, T.; Bernard, M.; Moor, I.; Watzke, S. Study Protocol: Hypersexual and Hyposexual Behavior among Adults Diagnosed with Alcohol- and Substance Use Disorders-Associations between Traumatic Experiences and Problematic Sexual Behavior. Front. Psychiatry 2023, 14, 1088747. [Google Scholar] [CrossRef]
- SAMHSA—Substance Abuse and Mental Health Services Administration. Risk and Protective Factors 2019; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2019. [Google Scholar]
- Montiel Ishino, F.A.; McNab, P.R.; Gilreath, T.; Salmeron, B.; Williams, F. A Comprehensive Multivariate Model of Biopsychosocial Factors Associated with Opioid Misuse and Use Disorder in a 2017–2018 United States National Survey. BMC Public Health 2020, 20, 1740. [Google Scholar] [CrossRef]
- Skewes, M.C.; Gonzalez, V.M. The Biopsychosocial Model of Addiction. In Principles of Addiction; Elsevier: Amsterdam, The Netherlands, 2013; pp. 61–70. ISBN 978-0-12-398336-7. [Google Scholar]
- Bukowski, W.M.; Laursen, B.; Rubin, K.H. (Eds.) Handbook of Peer Interactions, Relationships, and Groups, 2nd ed.; The Guilford Press: New York, NY, USA, 2018; ISBN 978-1-4625-2501-0. [Google Scholar]
- Furman, W.; Simon, V.A.; Shaffer, L.; Bouchey, H.A. Adolescents’ Working Models and Styles for Relationships with Parents, Friends, and Romantic Partners. Child Dev. 2002, 73, 241–255. [Google Scholar] [CrossRef]
- Jones, T.M.; Hill, K.G.; Epstein, M.; Lee, J.O.; Hawkins, J.D.; Catalano, R.F. Understanding the Interplay of Individual and Social–Developmental Factors in the Progression of Substance Use and Mental Health from Childhood to Adulthood. Dev. Psychopathol. 2016, 28, 721–741. [Google Scholar] [CrossRef] [PubMed]
- Renaud, F.; Jakubiec, L.; Swendsen, J.; Fatseas, M. The Impact of Co-Occurring Post-Traumatic Stress Disorder and Substance Use Disorders on Craving: A Systematic Review of the Literature. Front. Psychiatry 2021, 12, 786664. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Addiction Type | Biological Factors | Description |
|---|---|---|
| Cannabis | Genetic variants of elements of the endocannabinoid system [17] | Variants in genes related to the body’s endocannabinoid system. |
| CNR1 gene polymorphism (G allele) associated with increased withdrawal and craving [17] | Genetic variation linked to heightened withdrawal and cravings. | |
| Structural brain alterations associated with regional differences in MAGL expression [20] | Brain structure changes related to differences in endocannabinoid degradation. | |
| Opioids | Genetic variants and reduced CB1R binding in morphine-tolerant rats [17,22] | Genetic variations in CNR1 gene linked to opioid dependence and decreased cannabinoid receptor activity. |
| CNR1 gene C allele correlated with lower prevalence of lifelong major depression [17] | Specific gene variant associated with reduced likelihood of lifelong major depression. | |
| Stimulants | Endocannabinoid system involvement in brain responses to cocaine and methamphetamine [17] | Endocannabinoid system role in the brain’s reactions to stimulant drugs. |
| CNR1 gene polymorphisms associated with stimulant dependence [17] | Genetic variations in CNR1 gene linked to susceptibility to stimulant dependence. | |
| Genetic variants contributing to vulnerability to relapse in stimulant-dependent individuals [23] | Specific genetic variations increasing the risk of relapse in stimulant-dependent individuals. | |
| Importance of dopaminergic system in mediating actions and effects of stimulants [24] | Dopamine system significance in mediating stimulant drug effects. | |
| Hallucinogens | Subchronic administration of ketamine increases endocannabinoid concentrations in specific brain regions [25] | Prolonged ketamine use elevates endocannabinoid levels in specific brain regions. |
| Pharmacology and Treatment | No FDA- or EMA-approved drug treatment for most substance use disorders [26] | Lack of officially approved pharmaceutical treatments for most substance use disorders. |
| Studies on efficacy of antiepileptic drugs and combination therapies targeting GABAergic system dysfunction [27,28] | Research on antiepileptic drugs and combination therapies for GABA system dysfunction. | |
| Targeting endophenotypes associated with SUDs using cognitive enhancers [29] | Use of cognitive enhancers to address substance use disorder characteristics. | |
| Exploration of alternative therapies such as psychotherapy, mindfulness-based interventions, and virtual reality techniques [28] | Investigation into alternative treatments like therapy and mindfulness techniques. |
| Psychological Factors | Description | Reference(s) |
|---|---|---|
| Complex Entanglement | SUD intertwined with behavior, personality, and psychopathology; co-occurrence with psychiatric disorders and personality traits. | [30,31,32,33,34,35,36] |
| Personality Factors and Addiction | Temperament and personality traits (e.g., disinhibition, self-control) contributing to addiction development and persistence. | [31,32,37] |
| Anxiety and Addiction | Strong association between anxiety disorders and SUD; anxiety symptoms related to substance use and addiction severity. | [30,31,36] |
| Mood Disorders and Addiction | Common comorbidity between mood disorders and SUD; correlation between depression and craving intensity for specific substances. | [30,31,36] |
| ADHD and SUD | Attention deficit hyperactivity disorder (ADHD) as a risk factor for SUD development and a predictor of severe SUD course; bidirectional impact. | [33,36] |
| Traumatic Events, PTSD, and SUD | Co-occurrence of PTSD and SUD; traumatic events in adolescence promoting SUD development; substance use as coping strategy for PTSD symptoms. | [2,34] |
| SUD and ASD | Common dual diagnosis of SUD and Autism Spectrum Disorder (ASD); substance use to manage anxiety, stress, and social difficulties. | [35] |
| Self-Harm and Suicide Risk | Heightened suicide risk in individuals with chronic pain or mood disorders and SUD; opioids exhibit stronger correlation with suicidal ideation. | [39,40] |
| Social Factors | Description | Reference(s) |
|---|---|---|
| Childhood | Parenting styles (authoritarian, authoritative, neglectful, permissive) influence likelihood of substance use in children; childhood traumas (physical/emotional abuse, neglect) linked to increased cortisol levels and risk of substance use. | [42,43,44] |
| Adolescence | Adolescents susceptible to substance use due to curiosity, societal pressure, relationship issues, etc.; parental support as protective factor; peer support correlated with higher alcohol consumption; social isolation exacerbates substance use. | [44,45,46,47] |
| Adulthood | Family characteristics (cohesion, expressiveness, conflict) influence alcohol use in adults with AUD; loneliness associated with increased alcohol use; lack of social support, medical complications, bereavement contribute to onset of SUD or AUD. | [42,46] |
| Social Background | Social context influences addiction development; urban areas with drug accessibility and security issues associated with addiction; neighborhood disorder (graffiti, crime) and social cohesion impact alcohol use. | [46,47] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belfiore, C.I.; Galofaro, V.; Cotroneo, D.; Lopis, A.; Tringali, I.; Denaro, V.; Casu, M. A Multi-Level Analysis of Biological, Social, and Psychological Determinants of Substance Use Disorder and Co-Occurring Mental Health Outcomes. Psychoactives 2024, 3, 194-214. https://doi.org/10.3390/psychoactives3020013
Belfiore CI, Galofaro V, Cotroneo D, Lopis A, Tringali I, Denaro V, Casu M. A Multi-Level Analysis of Biological, Social, and Psychological Determinants of Substance Use Disorder and Co-Occurring Mental Health Outcomes. Psychoactives. 2024; 3(2):194-214. https://doi.org/10.3390/psychoactives3020013
Chicago/Turabian StyleBelfiore, Cecilia Ilaria, Valeria Galofaro, Deborah Cotroneo, Alessia Lopis, Isabella Tringali, Valeria Denaro, and Mirko Casu. 2024. "A Multi-Level Analysis of Biological, Social, and Psychological Determinants of Substance Use Disorder and Co-Occurring Mental Health Outcomes" Psychoactives 3, no. 2: 194-214. https://doi.org/10.3390/psychoactives3020013
APA StyleBelfiore, C. I., Galofaro, V., Cotroneo, D., Lopis, A., Tringali, I., Denaro, V., & Casu, M. (2024). A Multi-Level Analysis of Biological, Social, and Psychological Determinants of Substance Use Disorder and Co-Occurring Mental Health Outcomes. Psychoactives, 3(2), 194-214. https://doi.org/10.3390/psychoactives3020013