Abstract
Arachnophobia is a specific phobia characterized by an intense and persistent fear of spiders, often leading to avoidance behaviors that can significantly impact daily life. Virtual Reality Exposure Therapy (VRET) offers a controlled, adaptable, and immersive therapeutic environment, allowing for greater personalization, flexibility, and the real-time modulation of exposure parameters. This pilot study employed a quasi-experimental design without a control group to evaluate the efficacy of a gamified VRET intervention for treating arachnophobia. A sample of 25 participants underwent the intervention, with outcomes assessed through a Behavioral Approach Test (BAT) and self-report measures, including the Fear of Spiders Questionnaire (FSQ) and the Spider Phobia Questionnaire (SPQ-15), administered pre-intervention, post-intervention, and at a two-week follow-up. Findings indicate that gamified VRET led to significant reductions in self-reported fear and avoidance behaviors, suggesting its potential as an effective therapeutic tool for arachnophobia. Although some results were not entirely conclusive, the overall improvements observed support further investigation in larger, controlled trials.
1. Introduction
Anxiety is an emotional response to uncertain situations that requires appropriate coping strategies. It affects psychophysiological components and can significantly alter an individual’s quality of life [1]. When anxiety is excessive or disproportionate to the stimulus, or when it does not correspond to the expected response in a given context, it is considered pathological and can impact all aspects of an individual’s daily functioning [1].
Anxiety disorders are among the most common mental health conditions worldwide, affecting approximately 3.6% of the global population, with a higher prevalence among women, who are 1.5 times more susceptible [2]. Specific phobias, as defined by the Diagnostic and Statistical Manual of Mental Disorders [DSM-V-TR], are the most prevalent anxiety disorders, characterized by extreme fear and anxiety in response to a particular stimulus. In the case of arachnophobia, this stimulus is spiders [3]. Studies suggest that individuals living in rural areas, where interaction with natural environments is more frequent, tend to exhibit fewer animal-related phobias. Conversely, individuals in urban settings, who have less exposure to natural environments, are more likely to develop a fear of spiders, as reduced contact with nature is a risk factor for arachnophobia [4]. Individuals with this condition actively avoid environments where spiders may be present, leading to impairment in daily activities and affecting between 3.5% and 6.1% of individuals diagnosed with anxiety disorders [3,5,6].
Exposure therapy, a core component of cognitive behavioral therapy (CBT), is recognized as the most effective treatment for specific phobias, including arachnophobia [7,8,9,10,11,12]. CBT aims to restructure maladaptive cognitions and behaviors by challenging dysfunctional thoughts and promoting gradual exposure to feared stimuli [9,10,11]. Traditional in vivo exposure therapy involves real-world confrontation with phobic stimuli while maintaining controlled anxiety levels [10,12,13,14,15]. However, this approach has limitations, including logistical difficulties and high dropout rates due to the distress caused by direct exposure [13,16].
Virtual Reality Exposure Therapy (VRET) has emerged as an innovative alternative, offering controlled and immersive three-dimensional environments that can systematically expose individuals to their phobic stimuli in a safe and personalized manner [17,18,19,20,21]. By leveraging VR technology, clinicians can precisely control environmental variables, adjust the level of exposure to match individual needs, and reduce the unpredictability associated with real-world exposure [17,18,19,20,21]. Furthermore, VRET enables the real-time assessment of behavioral, emotional, cognitive, and physiological responses, providing valuable insights into the individual’s progress [20,22]. This controlled setting facilitates systematic desensitization, thereby enhancing emotional self-regulation and cognitive restructuring [23,24].
Gamification, an increasingly used technique in various contexts, has shown promise in enhancing engagement and motivation, particularly in the realm of mental health treatment. Defined as the application of game design elements in non-game contexts, gamification has proven to be effective in increasing participation and motivation in activities that might otherwise be perceived as challenging or monotonous. When integrated into therapeutic interventions, especially those involving virtual reality, gamification can significantly improve the treatment experience, making it more engaging and less aversive.
In the context of VRET, gamification elements such as scoring systems, progressive challenges, instant feedback, and goal setting can enhance the effectiveness of exposure therapy. These elements help motivate the patient and maintain engagement, thus reducing resistance to treatment and improving adherence. For example, patients might receive rewards as they progress through increasingly difficult exposure levels, helping to build confidence and providing a sense of achievement. Additionally, gamified narratives and avatars could help contextualize challenges, making the process more enjoyable and relatable [25,26,27,28,29].
Despite the growing body of research supporting VRET for various anxiety disorders, studies focusing specifically on gamified VRET interventions for arachnophobia remain limited. The integration of gamification into VR exposure therapy has the potential to increase motivation, adherence, and treatment efficacy, as it taps into the patient’s intrinsic desire for progress and rewards. While current research highlights the effectiveness of VR-based exposure, further exploration into the role of gamification in optimizing therapeutic outcomes is crucial.
Based on these considerations, this study aims to evaluate the efficacy of a gamified virtual reality-based intervention in the treatment of arachnophobia. By integrating interactive and engaging elements into exposure therapy, we seek to enhance user experience, improve treatment adherence, and contribute to the growing field of VR-based interventions for anxiety disorders.
2. Materials and Methods
This is a quasi-experimental study without a control group. The main aim of this study was to assess the feasibility of the intervention and explore its initial effects, rather than to establish definitive causal relationships. Therefore, the absence of a control group was justified, considering that the focus was on testing applicability and obtaining preliminary data. All participants were assessed before, during, and at the end of the intervention. There was also a follow-up two weeks after the intervention session [30,31,32]. For this purpose, the hypotheses for this study were determined as follows:
- ○
- The virtual reality-based intervention reduces the avoidance of phobic situations in individuals who are afraid of spiders;
- ○
- The virtual reality-based intervention reduces the levels of fear, disgust, and anxiety in individuals who are afraid of spiders.
2.1. Participants
Participants were selected using a non-probabilistic convenience sampling method, obtained from the general population. This approach was adopted due to time and resource constraints, allowing an accessible sample to be obtained within the period available to carry out the study. Recruitment was carried out by publicizing a questionnaire on social media, in which those interested in taking part filled in an initial form. The questionnaire was publicized for approximately two weeks after approval by the Ethics Committee. However, only individuals who met the inclusion criteria were selected to take part in the study.
Inclusion criteria required participants to be of legal age and score above five on the Spider Phobia Questionnaire-15 (SPQ-15). Exclusion criteria included health conditions that could interfere with the virtual reality experience (e.g., epilepsy, labyrinthitis, sensorimotor disorders, and visual impairments), substance dependence (excluding nicotine), and concurrent therapeutic interventions that might influence study outcomes [33,34]. The existing literature does not establish a specific cut-off point for the SPQ-15; however, this cut-off score was chosen to ensure the inclusion of individuals with different levels of fear of spiders, while maintaining a threshold of symptoms sufficient for a meaningful evaluation of the intervention. Selecting a lower cut-off point made it possible to obtain a more heterogeneous sample, which is particularly relevant in pilot or exploratory studies.
2.2. Instruments
Sociodemographic questionnaire: Sociodemographic information was collected, including gender, age, academic level, place of residence, any conditions contraindicating exposure to virtual reality, and the impact of the phobia on their daily living activities.
Fear of Spiders Questionnaire (FSQ): This is a self-report questionnaire made up of 18 items, answered on a Likert scale from 1 to 7. The aim is to assess anxiety and fear of spiders, and higher scores correspond to greater fear. This study used a Portuguese-language version of the questionnaire [27,35,36,37].
Spider Phobia Questionnaire—15 (SPQ-15): This is a self-administered scale comprising 15 dichotomous questions. It aims to assess various aspects of arachnophobia’s cognitive and behavioral components. Higher scores correspond to higher levels of arachnophobia. Since the shortened version of the questionnaire does not have a validated version in Portuguese, the questions were selected from the long version available in Portuguese, based on the structure of the original shortened version [36,38,39,40].
Behavioral Avoidance Test (BAT): This was conducted in a virtual environment and divided into 8 stages. Higher scores indicate less adverse reactions to the presence of spiders. The BAT ends when all steps have been completed or if the participant does not proceed to the next step. The virtual environment used was adapted from the description presented in a previous study, ensuring its relevance and validity for this research [33,34].
Simulator Sickness Questionnaire (SSQ): This was applied to assess the presence of some discomfort during the simulation. It consists of 16 questions evaluated on a 4-point Likert scale from 0 to 3, and higher values indicate worse reactions to VR. This study used a Portuguese version of the questionnaire [41,42].
Presence Questionnaire (PQ): This was applied to evaluate the virtual reality experience and was evaluated on a 7-point Likert scale from 1 to 7. Higher scores indicate greater immersion. This study used a Portuguese version of the questionnaire [43,44,45].
2.3. Procedures
Subjects’ participation in the study was formalized through the completion of an informed consent form, in accordance with the Declaration of Helsinki [46,47]. This process ensured the privacy and confidentiality of the collected data, as well as the participants’ right to access all relevant information needed to make an informed decision about their voluntary participation [47]. The study received approval from the Ethics Committee.
All participants previously completed an online pre-test questionnaire on the Microsoft Forms platform, with the following sections: (1) Sociodemographic data; (2) FSQ; and (3) SPQ-15.
Recognizing the importance of ethical considerations when recruiting participants and to ensure ethical compliance, participants provided initial consent before completing the online questionnaire. Only those who met the inclusion criteria were subsequently contacted for the experimental phase, in which they provided written informed consent before taking part in the VR intervention.
Based on the answers obtained in the questionnaire, the participants who agreed to be contacted for the second phase of the study and who met the previously defined inclusion and exclusion criteria were selected. The intervention sessions were scheduled according to the availability of each participant, with a difference of approximately two weeks between the two.
To ensure the safety of participants during exposure to VR, risk monitoring and control measures were implemented. Before the intervention began, a risk assessment was carried out to identify potential adverse reactions, and action protocols were defined for any situations of significant discomfort or extreme anxiety.
During exposure, participants were continuously monitored, and the presence of a therapist ensured immediate intervention if necessary. In situations of discomfort, participants had the possibility of interrupting the session at any time. These measures ensured that the experiment was conducted in a safe and controlled manner, thereby minimizing possible risks associated with VR exposure in the context of phobia.
Intervention Protocol
Immersion and presence in the virtual environment were carried out using Meta Quest 2 virtual reality glasses and the corresponding controls, and with the help of a computer so that the researcher could follow what the person was seeing and provide support in the event of difficulties. Throughout the intervention, the participants navigated the virtual environment using joystick controls, adjusted their field of vision by moving their head, and interacted with objects using the control’s trigger button.
The exposure to stimuli in the virtual environment, except points 1, 6, 7, and 8 of the intervention, took place in a dark and nocturnal environment. This space was the same for the rest of the intervention, and may or may not have contained phobic stimuli, depending on the objective of the stage. The intervention consisted of a session lasting approximately 2 h, structured as follows:
- (1)
- Psychoeducation on relaxation and breathing techniques.
- This environment was separate from the room where the rest of the intervention would take place. At this stage, no control was necessary. This was a virtual environment where relaxation and breathing techniques were taught that could be used throughout the exhibition (Figure A1).
- (2)
- Participant preparation and warm-up—getting used to the virtual space (Figure A2).
- The virtual environment without phobic stimuli (spiders) was presented, just so that the person could adapt to the environment, the glasses, and the VR controls.
- The controls were explained, after which the participants had time to get used to the VR equipment and the controls. After getting used to the space and before starting the exhibition, all the participants were asked to rate, from 0 to 10, their degree of disgust, fear, and anxiety in anticipation of what was going to be done.
- (3)
- Initial BAT (Figure A3).
- The purpose and environment of the BAT were explained, and participants were informed that they could stop at any time. Before starting the BAT, participants rated their levels of fear, anxiety, and disgust on a scale of 0 to 10. If they chose not to enter the room, the BAT was rated 0. When they clicked on ‘BAT’, the test began with a spider in a terrarium. The minimum score was 1, but it could be higher depending on the number of steps completed. Interactions could only be started 10 s after the previous one, to avoid quick interactions via the trigger button to avoid the spider. At this step, the field of vision was limited to prevent participants from looking away from the terrarium. At the end of the BAT, participants again rated their levels of fear, anxiety, and disgust on a scale of 0 to 10 [33,34,48,49].
- (4)
- Psychoeducation on spiders and their role in ecosystems and on spider phobia and its treatment.
- A virtual environment where you can see 3 blocks with a few sentences each was presented. One of the blocks contained sentences about spiders and their importance. The central block contained sentences about spider phobia, such as its etiology and consequences. Finally, the last block contained sentences about the treatment of spider phobia. The sentences could be read by the person, or a button could be pressed on each sentence to turn the text into an auditory stimulus. In addition, in the center of the screen, between the 3 blocks, you can see a circle containing a kind of lever that you can move. When you move the lever, the circle becomes less opaque, which makes a spider visible. As well as the spider being visible, two other levers allow you to change the zoom and the perspective from which it is seen.
- (5)
- Progressive exposure to virtual environments for systematic desensitization (Resistance).
- Three activities were carried out at 6 different levels of difficulty. In all the levels of all the activities, 3 min was set as the completion time, with a score counter always visible (Table A1) (Figure A4). At the start of the three activities in the six levels, all the participants were asked to rate their degree of disgust, fear, and anxiety about what they were about to do from 0 to 10. At the end of each of the moments, they were asked to rate their degree of disgust, fear, and anxiety, from 0 to 10, about what had just been done.
- As the person progressed through the levels, the difficulty of the task and the realism of the spiders increased.
- If necessary, the participant had the option of using the pause function.
- Activity 1 consisted of looking at the spiders for as long as possible. The longer the person looked at the spider, the more points they earned. If the spider was in the center of the field of vision, even from a distance, the person earned points. The spiders moved around the room, appearing and disappearing, and the aim was to always keep at least one in the field of vision.
- In Activity 2, the aim was to protect a spider from falling spheres. The playing field was reduced to a small space in the environment. The number of falling spheres increased with the difficulty of the levels. The person increased their points every time they defended the spider and lost when the spider was hit.
- Finally, in Activity 3, the spider moved, and the objective was to always maintain a distance equal to or less than the idealized distance, which varied according to the level being played. The longer it kept the correct distance, the more points it earned. When not at the correct distance, participants did not earn any points (Figure A5) [25,26]. The level of realism of the spider also changed throughout the activity (Figure A6).
- (6)
- Final BAT (Figure A3).
- This works in the same way as the initial BAT, since the environment and rules are the same.
- (7)
- Relaxation and feedback.
- This featured the same atmosphere and format as the ‘Psychoeducation in relaxation and breathing techniques’ moment, where the relaxation and breathing techniques taught at the beginning of the session were recalled.
- The aim was to help the person return to their initial state after prolonged exposure to the phobia.
- In addition, each participant was asked how they felt after the relaxation and the whole intervention.
- The person was also given some feedback on the session and on strategies they could adopt in their day-to-day life.
- (8)
- Filling out the post-test questionnaire (Table A2).
- In addition to completing the post-test questionnaires, a follow-up session was scheduled.
Thus, this treatment strategy consists of a combination of therapeutic ingredients, including exposure to fear-triggering stimuli, therapeutic instructions, client progress monitoring, performance feedback, and contingent performance improvement. The integration of gamification throughout the intervention, namely the reward and scoring system, mechanics of progression through different levels of difficulty, and methods of interaction with the environment in real time (please see this explanatory video: Due to the limitations of static images, a full understanding of the gameplay may be challenging (check the following video for more information on the VR environment developed: https://www.youtube.com/watch?v=WfKW5lt9mTw&ab_channel=LabRP (accessed on 9 April 2025)).
At the end of the exposure, participants answered an online post-test questionnaire, again on the Microsoft Forms platform, with the following sections: (1) FSQ and (2) SPQ-15. In addition, a new BAT identical to the initial one was carried out.
At the 2-week mark, a follow-up session was conducted, consisting of a new BAT, identical to the other two. A new online post-test questionnaire, the same as the one completed at the end of the exposure, again on the Microsoft Forms platform, was also completed [50,51,52].
2.4. Statistical Analyses
To analyze the information collected, statistical tests were used in IBM SPSS Statistics 29 software. Descriptive statistics characterized sociodemographic data, calculating means and standard deviations, as well as absolute and relative frequencies for categorical variables such as gender. In the inferential analysis, the assumptions for applying the repeated measures Analysis of Variance (ANOVA), used to identify significant differences between the intervention phases, were checked. If the assumptions were not met, the Friedman test was used. The initial significance level (α) of 0.05 was adjusted to control the risk of type I error, making the analysis more robust [53,54,55,56].
3. Results
There were twenty-five participants in the sample, and, as shown in Table 1, most of this group was female (76%), single (84%), and had a degree (48%). In addition, 36% of the sample included students.

Table 1.
Sample sociodemographic characterization.
3.1. Virtual Reality Questionnaires
The ANOVA assumptions were tested for the SSQ and PQ variables, but in both cases, they could not be used due to the assumptions being violated. It was therefore decided to follow the non-parametric route. PQ was the only variable that showed a significant value at any point, with p < 0.001. In the Wilcoxon test, PQ was only significant when comparing the first and last moments (Table 2).
Table 2.
Summary statistical measures for the three moments in the Simulator Sickness Questionnaire and the Presence Questionnaire.
3.2. Subjective Evaluation of Emotions
The assumptions of ANOVA were tested for the evaluation of the three emotions: fear, disgust, and anxiety. However, only the fear and disgust variables met the assumptions necessary for the use of parametric tests. The analyses for these two emotions revealed significant differences, with p-values < 0.001 in either case. The emotion of anxiety, on the other hand, did not meet the assumptions for ANOVA, and was therefore assessed using non-parametric tests. In the Friedman test, anxiety also showed a p < 0.001, indicating a significant difference at some point (Table 3).
Table 3.
Summary statistical measures for all moments in subjective evaluation of fear, anxiety, and disgust.
3.3. Scores Obtained in the Different Games
The assumptions of ANOVA were tested for the variables of the three activities, but it could not be used for any of them due to violating the assumptions. We therefore opted to follow the non-parametric route. All showed a significant value at some point, with p < 0.001 in the Wilcoxon test. Table 4 shows the median scores for each activity at each level and the respective Interquartile Range. It also shows the scores for the same activities between the different levels.
Table 4.
Summary statistical measures for the scores of all activities at all levels.
3.4. Spider Fear Questionnaires
The ANOVA assumptions were assessed, and only the FSQ and SPQ data met the requirements. The ANOVA for the FSQ resulted in a p-value of 0.008 and for the SPQ, 0.013, indicating significant differences between the moments, which led to post hoc analyses being carried out to identify the origin of these differences. In the case of the BAT, as the ANOVA assumptions were not met, the Friedman test was used, which resulted in a p < 0.001. Based on this result, the Wilcoxon test was applied to investigate the differences between the specific moments (Table 5).
Table 5.
Summary statistical measures for the three moments in the Fear of Spiders Questionnaire, the Spider Phobia Questionnaire, and the Behavioral Avoidance Test.
4. Discussion
This study investigated the impact of a virtual reality-based intervention to treat spider phobia. The analysis included virtual reality questionnaires, subjective assessments of emotions, scores on different activities, and specific questionnaires on fear of spiders.
The results obtained through the Simulator Sickness Questionnaire indicated that adverse reactions to exposure to virtual reality gradually increased throughout the intervention session, though these changes were not statistically significant. Many participants reported similar reactions in the first and last assessments, as reflected in the score obtained in “Dif(m6-m1)”. Notably, the highest scores were related to generalized malaise, which could be linked to the fear of spiders rather than just the virtual environment exposure [41,42,57,58,59,60,61].
Several factors can explain the increase in the SSQ score. One of the main ones is sensory conflict, occurring when there is a discrepancy between what someone’s vision and body perceive, resulting in nausea and discomfort [16,62,63,64,65]. For instance, the likelihood of cybersickness increases when the user is virtually moving but physically stationary, as in the VR experience [66,67]. While higher-quality VR equipment tends to provide a smoother, more realistic immersive experience that can reduce cybersickness, it may paradoxically intensify adverse reactions due to increased presence and immersion. This can exacerbate sensory conflicts, leading to more acute symptoms [59,68]. Additionally, prolonged exposure, especially in fast-moving VR experiences, increases the risk of cybersickness [69,70]. Individual characteristics also matter; participants using VR for the first time may be more susceptible, as many were in this study. Those prone to motion sickness or in less favorable health conditions (e.g., fatigue or dehydration) are at a higher risk of experiencing these symptoms [71,72]. Environmental factors, such as bright lights, cramped spaces, or high temperatures, can further contribute to discomfort, thereby aggravating cybersickness [16,62,63,64].
The sense of presence increased throughout the study, significantly rising between the first and last moments. This could be due to the wide field of vision and the user’s ability to interact naturally and in real-time with the virtual environment, where their actions generated immediate and coherent responses. The involvement of multiple senses and the alignment of stimuli also likely reinforced the sense of presence [43,44,45,62,63].
Emotions were assessed to measure the intervention’s impact on the participants’ fear, disgust, and anxiety towards the phobic stimulus. The results showed a consistent decrease in fear and disgust from the beginning to the end of the intervention. Anxiety scores also decreased, with the most notable differences occurring between the first and last moments. The significant impact of these emotions suggests that repeated exposure to virtual spiders may have desensitized the participants, reducing their adverse emotional responses [25,27,33,34,48,49].
The participants’ performance in the three activities at six levels was also analyzed. Activity 1 showed score improvements at almost every time point, with significant changes at two points. In Activity 2, participants demonstrated consistent progress across levels, with significant differences at almost every point. The last activity showed a trend towards improvement, although only one comparison reached statistical significance after Bonferroni adjustment. These findings support the idea that repeated practice and gradual exposure helped participants improve their performance, likely reflecting reduced aversion or fear that initially hindered their performance [34,73,74,75,76,77].
Furthermore, the application of gamification in this framework amplifies the effectiveness of therapy. By integrating elements such as rewards, progressive challenges, and real-time feedback, gamification transforms the therapeutic process into an engaging and motivating experience. By incorporating game-like features, VR-based therapy becomes more interactive and less intimidating, which can significantly increase participant motivation and treatment adherence. The inclusion of gamification elements may have contributed to maintaining engagement and motivation, even with increased exposure. Through progressive challenges and immediate feedback, gamification probably made the exposure process less aversive and more engaging, encouraging persistence. This playful aspect may have facilitated gradual desensitization, promoting continuous performance improvement [78,79].
The results of the BAT also indicated a positive evolution concerning the fear of spiders reported by the participants, with a significant increase in the steps they could complete. The Wilcoxon test showed significant differences between the pre-test and post-test and between the pre-test and follow-up, suggesting that the intervention was effective and maintained its effectiveness over time. This adds to the evidence that this VRET protocol positively impacted reducing participants’ fear of spiders [3,33,34,80].
The results obtained in the specific spider fear questionnaires (FSQ and SPQ-15) showed significant changes only between the pre-test and follow-up, although the average score always decreased. This reduction suggests that the VRET protocol had a positive effect on reducing the participants’ level of anxiety in relation to exposure to spiders [3,80]. The significant difference between pre-test and follow-up in the FSQ aligns with the perception that the FSQ is effective in capturing subtle and progressive changes in fear levels. The SPQ-15 showed a significant difference only between pre-test and follow-up.
These results highlight the importance of using instruments that accurately and sensitively capture changes in fear levels over time. According to studies, while the SPQ-15 is useful, the FSQ seems more suitable for monitoring participants’ progress throughout an intervention like Virtual Reality Exposure Therapy, particularly in studies aiming to detect gradual and sustained changes in behavior and cognition [27,35,37,38,39].
Overall, the study’s findings suggest that the virtual reality intervention effectively reduced spider phobia, as evidenced by the significant reduction in negative emotional responses and improved performance in related activities. These results align with the literature that supports VRET as a positive treatment method for phobias [23,81,82,83,84,85].
Despite the growing body of research supporting VRET for various anxiety disorders, studies focusing specifically on gamified VRET interventions for arachnophobia remain limited. In this sense, this study contributes to adding to the existing literature by providing new knowledge on the effectiveness of gamified VRET for spider phobia. The results of this study suggest that the inclusion of gamification through progressive challenges, rewards, and real-time feedback not only increases immersion but also facilitates a more gradual and engaging desensitization process. Furthermore, this study expands on previous research by employing a multi-level task-based approach to measure behavioral improvements alongside emotional responses, providing a more comprehensive assessment of therapeutic outcomes. Significant reductions in fear and disgust, combined with improved task performance, reinforce the potential of gamified VRET as an effective and engaging alternative to traditional exposure therapies [83,85,86,87,88,89].
Finally, this study has some limitations. One of these limitations is the small size and variability of the sample, which may limit the robustness and statistical validity of the results, reducing the ability to detect significant effects. The fidelity of the virtual experience is another factor; if the spiders are not realistic enough, the participants’ responses may not reflect the same intensity as they would in a real-life scenario. Immersion is also crucial; technical issues or discomfort, such as motion sickness, can affect the validity of the experience. The subjective nature of fear measures poses another limitation, as self-reports are prone to bias. Complementing these with objective indicators, such as physiological responses, would be valuable. The lack of long-term follow-up also prevents a proper assessment of the durability of the therapeutic effects observed.
Individual factors, such as the participants’ personal history, fear intensity, and other psychological conditions, can influence responses to VR-based exposure therapy. Participants’ acceptance and familiarity with VR technology also affect their engagement and response to treatment. Given that many participants were new to VR, they might have been more focused on the VR experience than the stimuli presented. Future studies should consider improving technology, incorporating more natural interactions, and adding tactile feedback to enhance immersion. More advanced assessment methods, such as physiological measurements and conducting longitudinal studies, would help verify the maintenance of therapeutic effects over time. In addition, it is essential to investigate how demographic factors such as gender, age, education, and ethnicity can influence the effectiveness of VRET, ensuring that interventions are suitable for different populations. Comparative studies between VR exposure therapy and other treatment modalities, as well as exploring the combination of VR with other therapeutic approaches, would be beneficial to determine the most effective treatment strategies. Furthermore, future studies must include control groups to validate the changes observed and strengthen the conclusions about the effectiveness of the intervention, allowing for a more rigorous assessment of the causal effects of VRET.
In summary, this study highlights that VRET can be an effective treatment for spider phobia. The significant reduction in fear and improvement in activity scores suggest that VRET may be a promising alternative to traditional therapies. The findings provide valuable insights into the potential of VR in mental health interventions, although more research is needed to confirm and extend these results.
5. Conclusions
The results of this study demonstrate that exposure therapy using virtual reality shows positive results and is a promising approach in the treatment of individuals with spider phobia. Although some results were not entirely conclusive, it was possible to observe significant positive differences in reducing anxiety in anxiogenic contexts. These findings suggest that virtual reality can be an effective tool for addressing and mitigating the symptoms of specific phobias, providing a controlled and safe environment for therapeutic exposure.
However, to strengthen the evidence in this area, future studies must be carried out with larger and more diverse samples, as well as greater control of the variables under study. Further research should also explore the combination of virtual reality with other therapeutic modalities and include objective measures, such as physiological indicators, to obtain a more comprehensive assessment of the effectiveness of this approach.
Author Contributions
Conceptualization, I.L., R.S.d.A. and P.V.G.; data curation, I.L.; formal analysis, I.L.; investigation, I.L.; methodology, I.L., R.S.d.A. and P.V.G.; project administration, I.L. and R.S.d.A.; resources provision, A.M.; supervision, R.S.d.A. and A.M.; validation, R.S.d.A., A.M. and P.V.G.; visualization, I.L.; writing—original draft preparation, I.L.; writing—review and editing, R.S.d.A., P.V.G. and A.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of E2S, Polytechnic of Porto [CE0015E].
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data are available upon reasonable request from the authors.
Acknowledgments
The authors would like to thank Gonçalo Oliveira for his support in developing the virtual environment.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A

Figure A1.
Initial view of the virtual environment.
Figure A1.
Initial view of the virtual environment.


Figure A2.
Appearance of the main and initial environment.
Figure A2.
Appearance of the main and initial environment.


Figure A3.
BAT’s appearance.
Figure A3.
BAT’s appearance.
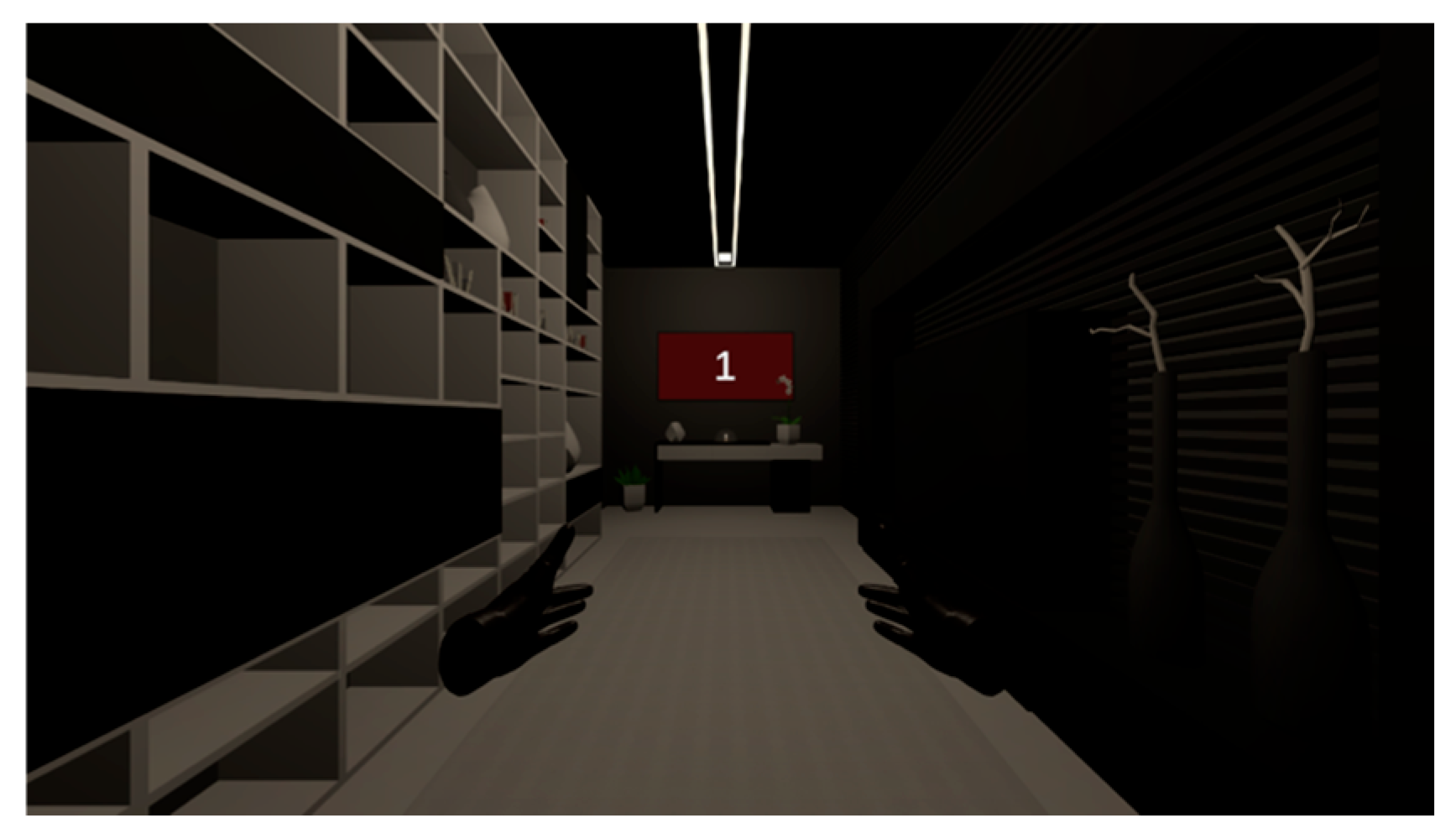

Figure A4.
Appearance of the activity difficulty selection menu and the activity time and score display.
Figure A4.
Appearance of the activity difficulty selection menu and the activity time and score display.
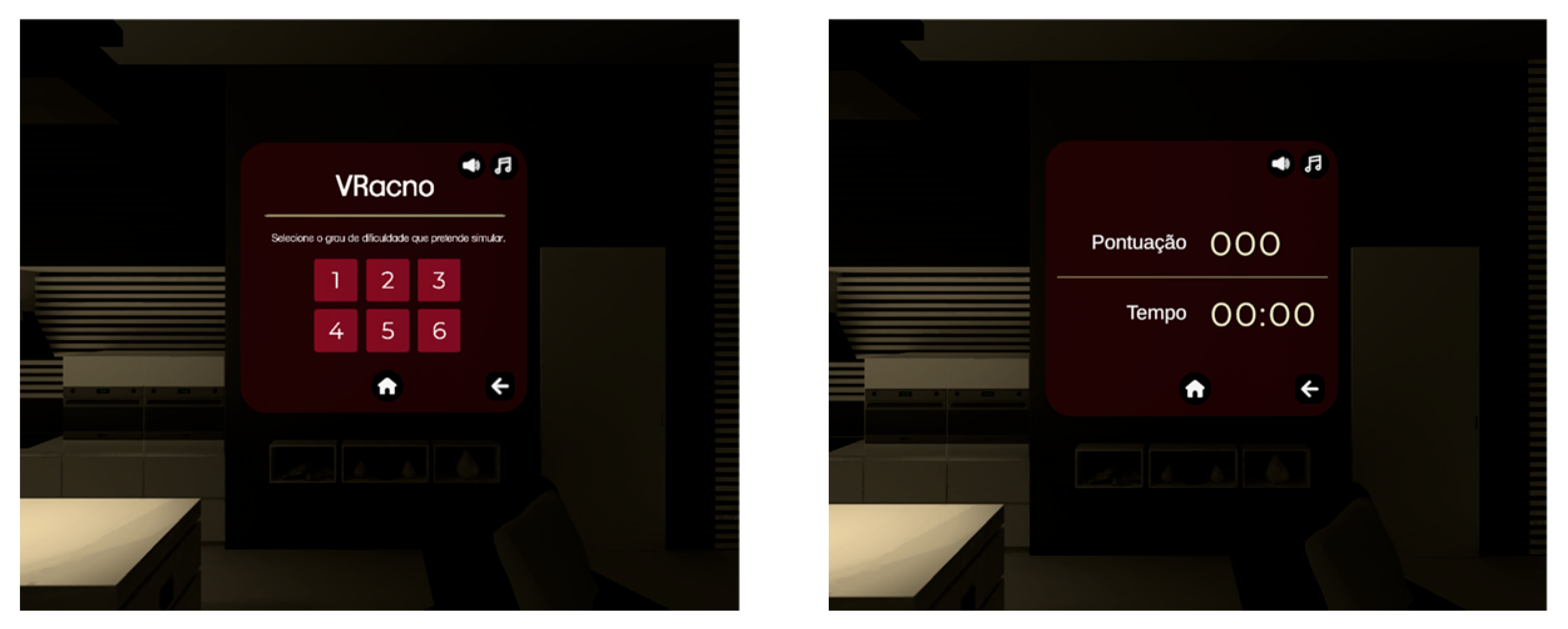
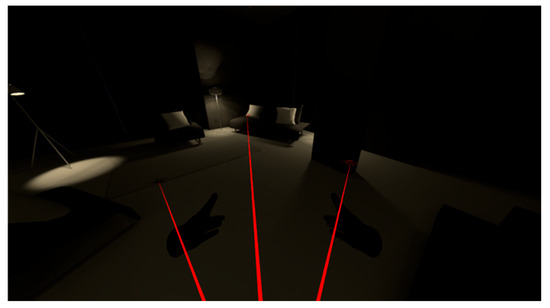
Figure A5.
Appearance of activity 3 when the correct distance to the spider is maintained.
Figure A5.
Appearance of activity 3 when the correct distance to the spider is maintained.
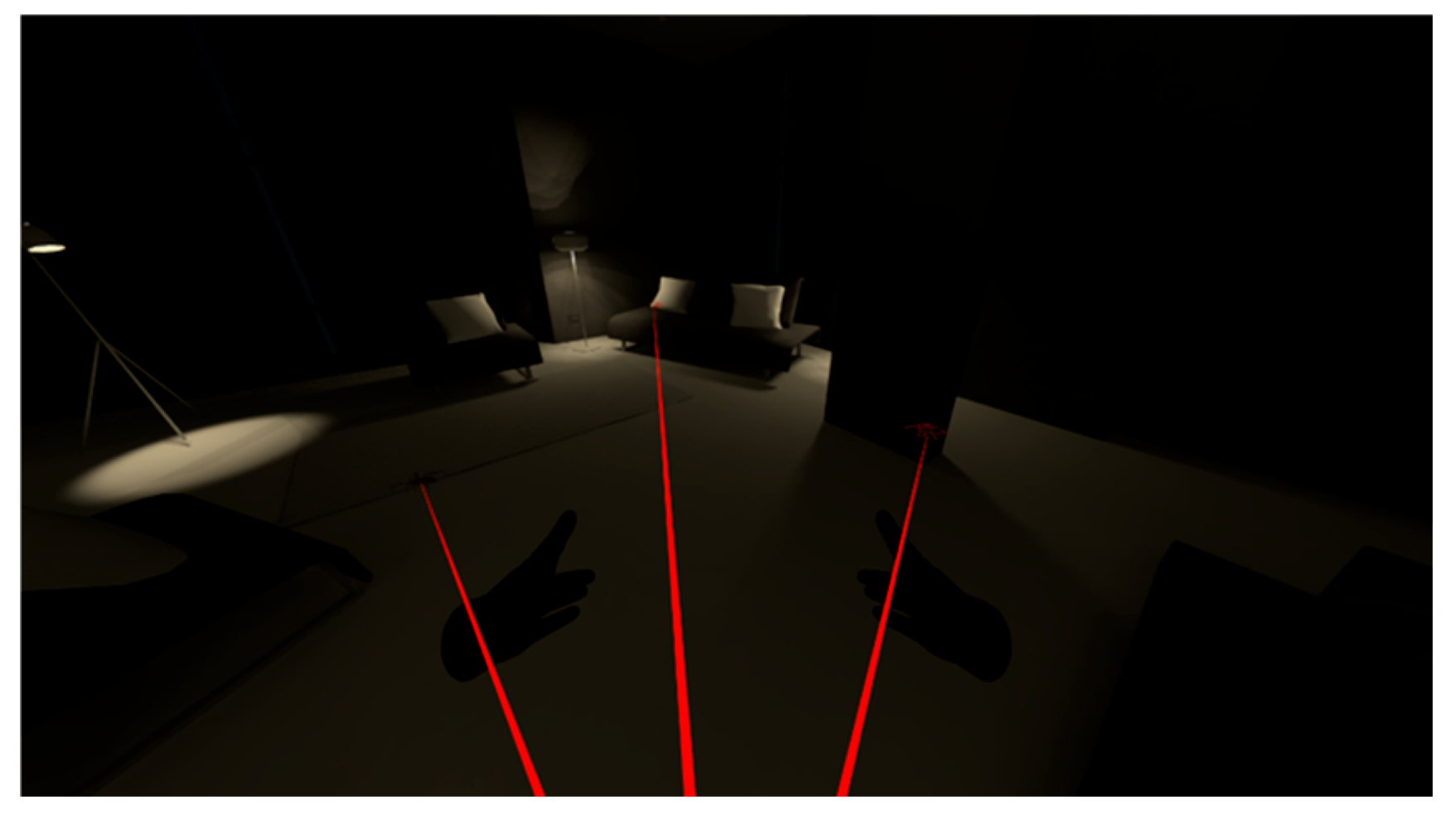
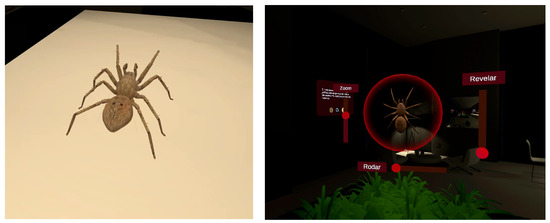
Figure A6.
Spider levels of realism.
Figure A6.
Spider levels of realism.
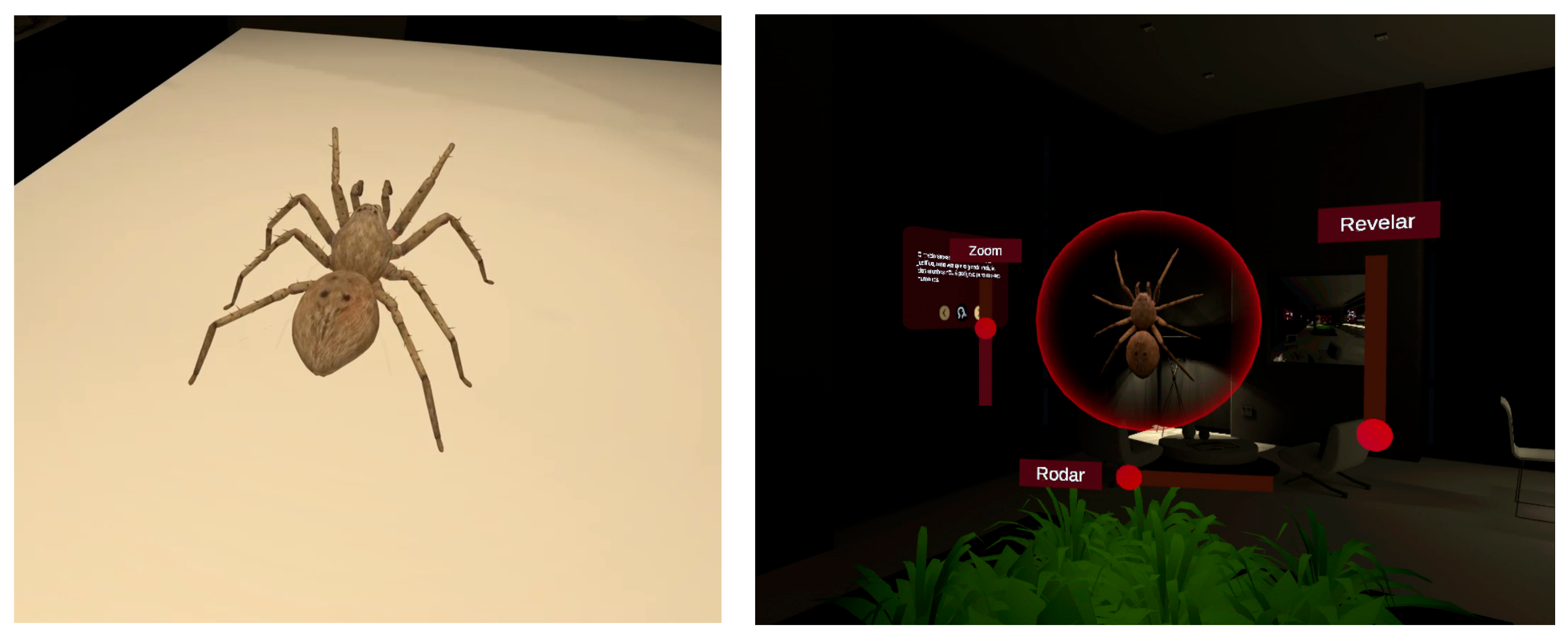
Table A1.
Organization of activities by level of difficulty.
Table A1.
Organization of activities by level of difficulty.
| Level 1: Activity 1: 1 spider, non-realistic, size 0.5. For 20 s each; Activity 2: 1 spider, non-realistic, size 0.5. Spheres appear every 6–8 s and wait 3 s before attacking; Activity 3: 1 spider, non-realistic, size 0.5. Desired distance: 2 m. | Level 2: Activity 1: 2 spiders, realistic, size 1. For 20 s each; Activity 2: 1 spider, realistic, size 1. Spheres appear every 5–7 s and wait 2.5 s before attacking; Activity 3: 1 spider, realistic, size 1. Desired distance: 2 m. | Level 3: Activity 1: 3 spiders, realistic, size 1.5. For 20 s each; Activity 2: 1 spider, realistic, size 1.5. Spheres appear every 4–6 s and wait 2 s before attacking; Activity 3: 2 spiders, realistic, size 1.5. Desired distance: 2 m. |
| Level 4: Activity 1: 4 spiders, realistic, size 1.5. For 10 s each; Activity 2: 1 spider, realistic, size 1.5. Spheres appear every 3–5 s and wait 1.5 s before attacking; Activity 3: 2 spiders, realistic, size 1.5. Desired distance: 1 m. | Level 5: Activity 1: 5 spiders, realistic, size 2. For 10 s each; Activity 2: 1 spider, realistic, size 2. Spheres appear every 2–4 s and wait 1 s before attacking; Activity 3: 3 spiders, realistic, size 1.5. Desired distance: 1 m. | Level 6: Activity 1: 6 spiders, realistic, size 2. For 10 s each; Activity 2: 1 spider, realistic, size 2.5. Spheres appear every 1–3 s and wait 0.5 s before attacking; Activity 3: 3 spiders, realistic, size 2. Desired distance: 1 m. |
Table A2.
Moments of evaluation in the intervention.
Table A2.
Moments of evaluation in the intervention.
| Time | Step | Evaluation |
|---|---|---|
| 5 | Pre-test questionnaire | Sociodemographic data, SPQ-15 e FSQ [PT] |
| 3 | Breathing techniques | Fear, anxiety, and disgust on a scale of 0 to 10 pre-intervention [M1] |
| 3 | Ambiance | |
| 3 | BAT | Fear, anxiety, and disgust on a scale of 0 to 10 [M2] |
| 3 | Information | |
| 9 | Level 1 | Fear, anxiety, and disgust on a scale of 0 to 10 [M3] |
| 3 | Pause | SSQ e PQ [m1] |
| 9 | Level 2 | Fear, anxiety, and disgust on a scale of 0 to 10 [M4] |
| 3 | Pause | SSQ e PQ [m2] |
| 9 | Level 3 | Fear, anxiety, and disgust on a scale of 0 to 10 [M5] |
| 3 | Pause | SSQ e PQ [m3] |
| 9 | Level 4 | Fear, anxiety, and disgust on a scale of 0 to 10 [M6] |
| 3 | Pause | SSQ e PQ [m4] |
| 9 | Level 5 | Fear, anxiety, and disgust on a scale of 0 to 10 [M7] |
| 3 | Pause | SSQ e PQ [m5] |
| 9 | Level 6 | Fear, anxiety, and disgust on a scale of 0 to 10 [M8] |
| 3 | Pause | SSQ e PQ [m6] |
| 3 | Post-test BAT | Fear, anxiety, and disgust on a scale of 0 to 10 [M9] |
| 3 | Breathing techniques | Fear, anxiety, and disgust on a scale of 0 to 10 post-intervention [M10] |
| 3 | Post-test questionnaire | SPQ-15 e FSQ [PsT] |
| 3 | Follow-up BAT | Fear, anxiety, and disgust on a scale of 0 to 10 [M11] |
| 3 | Follow-up questionnaire | SPQ-15 e FSQ [FU] |
References
- Romo-Barrientos, C.; Criado-Álvarez, J.J.; Gil-Ruiz, M.T.; González-González, J.; Rodríguez-Hernández, M.; Corregidor-Sánchez, A.I.; Ubeda-Bañon, I.; Flores-Cuadrado, A.; Mohedano-Moriano, A.; Polonio-López, B. Anatomical prosection practices in the Occupational Therapy degree. Student anxiety levels and academic effectiveness. Ann. Anat. 2019, 221, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Marco, P.L.; Valério, I.D.; Zanatti, C.L.d.M.; Gonçalves, H. Systematic review: Symptoms of parental depression and anxiety and offspring overweight. Rev. Saude Publica 2020, 54, 49. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association Publishing: Washington, DC, USA, 2022. [Google Scholar]
- Zsido, A.N.; Coelho, C.M.; Polák, J. Nature relatedness: A protective factor for snake and spider fears and phobias. People Nat. 2022, 4, 669–682. [Google Scholar] [CrossRef]
- Schmitt, W.J.; Müri, R.M. Neurobiologie der Spinnenphobie. Schweiz. Arch. Neurol. 2009, 160, 352–355. [Google Scholar]
- Vargas-Herrera, D.; Oropeza, L.A.; Cabrera, O.E.; Caldelas, I.; Brambila-Paz, F.; Montúfar-Chaveznava, R. Exploring virtual reality for neural rehabilitation and phobia treatment. Commun. Comput. Inf. Sci. 2019, 1002, 46–57. [Google Scholar]
- Morina, N.; Ijntema, H.; Meyerbröker, K.; Emmelkamp, P.M.G. Can virtual reality exposure therapy gains be generalized to real-life? A meta-analysis of studies applying behavioral assessments. Behav. Res. Ther. 2015, 74, 18–24. [Google Scholar] [CrossRef]
- Suso-Ribera, C.; Fernández-Álvarez, J.; García-Palacios, A.; Hoffman, H.G.; Bretón-López, J.; Baños, R.M.; Quero, S.; Botella, C. Virtual Reality, Augmented Reality, and In Vivo Exposure Therapy: A Preliminary Comparison of Treatment Efficacy in Small Animal Phobia. Cyberpsychol. Behav. Soc. Netw. 2019, 22, 31. [Google Scholar] [CrossRef]
- Axelsson, E.; Hedman-Lagerlöf, E. Cognitive behavior therapy for health anxiety: Systematic review and meta-analysis of clinical efficacy and health economic outcomes. Expert Rev. Pharmacoeconomics Outcomes Res. 2019, 19, 663–676. [Google Scholar] [CrossRef]
- Wechsler, T.F.; Mühlberger, A.; Kümpers, F. Inferiority or Even Superiority of Virtual Reality Exposure Therapy in Phobias?—A Systematic Review and Quantitative Meta-Analysis on Randomized Controlled Trials Specifically Comparing the Efficacy of Virtual Reality Exposure to Gold Standard in vivo Exposure in Agoraphobia, Specific Phobia, and Social Phobia. Front. Psychol. 2019, 10, 1758. [Google Scholar]
- Apolinário-Hagen, J.; Drüge, M.; Fritsche, L. Cognitive behavioral therapy, mindfulness-based cognitive therapy and acceptance commitment therapy for anxiety disorders: Integrating traditional with digital treatment approaches. Adv. Exp. Med. Biol. 2020, 1191, 291–329. [Google Scholar]
- Lindner, P.; Miloff, A.; Hamilton, W.; Reuterskiöld, L.; Andersson, G.; Powers, M.B.; Carlbring, P. Creating state of the art, next-generation Virtual Reality exposure therapies for anxiety disorders using consumer hardware platforms: Design considerations and future directions. Cogn. Behav. Ther. 2017, 46, 404–420. [Google Scholar] [CrossRef] [PubMed]
- Linke, J.O.; Jones, E.; Pagliaccio, D.; Swetlitz, C.; Lewis, K.M.; Silverman, W.K.; Bar-Haim, Y.; Pine, D.S.; Brotman, M.A. Efficacy and mechanisms underlying a gamified attention bias modification training in anxious youth: Protocol for a randomized controlled trial. BMC Psychiatry 2019, 19, 246. [Google Scholar] [CrossRef] [PubMed]
- Eaton, W.W.; Bienvenu, O.J.; Miloyan, B. Specific phobias. Lancet Psychiatry 2018, 5, 678–686. [Google Scholar] [CrossRef] [PubMed]
- Verkuyl, M.; Romaniuk, D.; Mastrilli, P. Virtual gaming simulation of a mental health assessment: A usability study. Nurse Educ. Pract. 2018, 31, 83–87. [Google Scholar] [CrossRef]
- Aldaba, C.N.; White, P.J.; Byagowi, A.; Moussavi, Z. Virtual reality body motion induced navigational controllers and their effects on simulator sickness and pathfinding. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Republic of Korea, 11–15 July 2017; pp. 4175–4178. [Google Scholar]
- Halldorsson, B.; Hill, C.; Waite, P.; Partridge, K.; Freeman, D.; Creswell, C. Annual Research Review: Immersive virtual reality and digital applied gaming interventions for the treatment of mental health problems in children and young people: The need for rigorous treatment development and clinical evaluation. J. Child Psychol. Psychiatry 2021, 62, 584–605. [Google Scholar] [CrossRef]
- Hatta, M.H.; Sidi, H.; Sharip, S.; Das, S.; Saini, S.M. The Role of Virtual Reality as a Psychological Intervention for Mental Health Disturbances during the COVID-19 Pandemic: A Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 2390. [Google Scholar] [CrossRef]
- Yeung, A.W.K.; Tosevska, A.; Klager, E.; Eibensteiner, F.; Laxar, D.; Stoyanov, J.; Glisic, M.; Zeiner, S.; Kulnik, S.T.; Crutzen, R.; et al. Virtual and augmented reality applications in medicine: Analysis of the scientific literature. J. Med. Internet Res. 2021, 23, e25499. [Google Scholar] [CrossRef]
- Emmelkamp, P.M.G.; Meyerbröker, K. Virtual Reality Therapy in Mental Health. Annu. Rev. Clin. Psychol. 2021, 17, 495–519. [Google Scholar] [CrossRef]
- Hanifah, H.; Ito, Y.; Yao, D.P.G.; Suyama, N.; Inoue, K. Promoting Sports Engagement during the COVID-19 Pandemic via Virtual Reality Games. Occup. Ther. Int. 2022, 2022, 4824152. [Google Scholar] [CrossRef]
- Freeman, D.; Reeve, S.; Robinson, A.; Ehlers, A.; Clark, D.; Spanlang, B.; Slater, M. Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol. Med. 2017, 47, 2393. [Google Scholar] [CrossRef]
- Botella, C.; Fernández-Álvarez, J.; Guillén, V.; García-Palacios, A.; Baños, R. Recent Progress in Virtual Reality Exposure Therapy for Phobias: A Systematic Review. Curr. Psychiatry Rep. 2017, 19, 42. [Google Scholar] [CrossRef] [PubMed]
- Schweizer, T.; Schmitz, J.; Plempe, L.; Sun, D.; Becker-Asano, C.; Leonhart, R.; Tuschen-Caffier, B. The impact of pre-existing anxiety on affective and cognitive processing of a Virtual Reality analogue trauma. PLoS ONE 2017, 12, e0190360. [Google Scholar] [CrossRef] [PubMed]
- Miloff, A.; Lindner, P.; Hamilton, W.; Reuterskiöld, L.; Andersson, G.; Carlbring, P. Single-session gamified virtual reality exposure therapy for spider phobia vs. traditional exposure therapy: Study protocol for a randomized controlled non-inferiority trial. Trials 2016, 17, 60. [Google Scholar] [CrossRef] [PubMed]
- Lindner, P.; Rozental, A.; Jurell, A.; Reuterskiöld, L.; Andersson, G.; Hamilton, W.; Miloff, A.; Carlbring, P. Experiences of gamified and automated virtual reality exposure therapy for spider phobia: Qualitative study. JMIR Serious Games 2020, 8, e17807. [Google Scholar] [CrossRef]
- Lindner, P.; Miloff, A.; Bergman, C.; Andersson, G.; Hamilton, W.; Carlbring, P. Gamified, Automated Virtual Reality Exposure Therapy for Fear of Spiders: A Single-Subject Trial Under Simulated Real-World Conditions. Front. Psychiatry 2020, 11, 116. [Google Scholar] [CrossRef]
- Khaleghi, A.; Narimani, A.; Aghaei, Z.; Banaraki, A.K.; Hassani-Abharian, P. A Smartphone-Gamified Virtual Reality Exposure Therapy Augmented With Biofeedback for Ailurophobia: Development and Evaluation Study. JMIR Serious Games 2024, 12, e34535. [Google Scholar] [CrossRef]
- Donker, T.; Van Esveld, S.; Fischer, N.; Van Straten, A. 0Phobia—Towards a virtual cure for acrophobia: Study protocol for a randomized controlled trial. Trials 2018, 19, 433. [Google Scholar] [CrossRef]
- De Oliveira, A.G. Bioestatística, Epidemiologia e Investigação; LIDEL—Edições Técnicas: Lisbon, Portugal, 2009; p. 255. [Google Scholar]
- Andrews, J.; Likis, F.E. Study Design Algorithm. J. Low. Genit. Tract Dis. 2015, 19, 364–368. [Google Scholar] [CrossRef]
- Ranganathan, P.; Aggarwal, R. Study designs: Part 1—An overview and classification. Perspect. Clin. Res. 2018, 9, 184. [Google Scholar] [CrossRef]
- Grill, M.; Haberkamp, A. Development and validation of an open-access online Behavioral Avoidance Test (BAT) for spider fear. Psychol. Assess. 2023, 36, 351. [Google Scholar] [CrossRef]
- Öst, L.G.; Salkovskis, P.M.; Hellström, K. One-session therapist-directed exposure vs. self-exposure in the treatment of spider phobia. Behav. Ther. 1991, 22, 407–422. [Google Scholar] [CrossRef]
- Szymanski, J.; O’Donohue, W. Fear of Spiders Questionnaire. J. Behav. Ther. Exp. Psychiatry 1995, 26, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Granado, L.C.; Peláez, F.J.R.; Garcia-Mijares, M. Estudo no contexto brasileiro de três questionários para avaliar aracnofobia. Aval. Psicol. 2005, 4, 125–139. [Google Scholar]
- Booth, R.W.; Peker, M.; Oztop, P. Turkish adaptation of the Fear of Spiders Questionnaire: Reliability and validity in non-clinical samples. Cogent Psychol. 2016, 3, 1144250. [Google Scholar] [CrossRef]
- Zsido, A.N. The spider and the snake—A psychometric study of two phobias and insights from the Hungarian validation. Psychiatry Res. 2017, 257, 61–66. [Google Scholar] [CrossRef]
- Cowdrey, F.A.; Walz, L. Exposure therapy for fear of spiders in an adult with learning disabilities: A case report. Br. J. Learn. Disabil. 2015, 43, 75–82. [Google Scholar] [CrossRef]
- Olatunji, B.O.; Woods, C.M.; de Jong, P.J.; Teachman, B.A.; Sawchuk, C.N.; David, B. Development and Initial Validation of an Abbreviated Spider Phobia Questionnaire Using Item Response Theory. Behav. Ther. 2009, 40, 114–130. [Google Scholar] [CrossRef]
- Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal, M.G. Simulator Sickness Questionnaire: An Enhanced Method for Quantifying Simulator Sickness. Int. J. Aviat. Psychol. 1993, 3, 203–220. [Google Scholar] [CrossRef]
- De Carvalho, M.R.; da Costa, R.T.; Nardi, A.E. Simulator Sickness Questionnaire: Tradução e adaptação transcultural. J. Bras. Psiquiatr. 2011, 60, 247–252. [Google Scholar] [CrossRef]
- Vasconcelos-Raposo, J.; Melo, M.; Barbosa, L.; Teixeira, C.; Cabral, L.; Bessa, M. Assessing presence in virtual environments: Adaptation of the psychometric properties of the Presence Questionnaire to the Portuguese populations. Behav. Inf. Technol. 2021, 40, 1417–1427. [Google Scholar] [CrossRef]
- Vasconcelos-Raposo, J.; Bessa, M.; Melo, M.; Barbosa, L.; Rodrigues, R.; Teixeira, C.M.; Cabral, L.; Sousa, A.A. Adaptation and Validation of the Igroup Presence Questionnaire (IPQ) in a Portuguese Sample. Presence Teleoperators Virtual Environ. 2016, 25, 191–203. [Google Scholar] [CrossRef]
- Witmer, B.G.; Singer, M.J. Measuring presence in virtual environments: A presence questionnaire. Presence Teleoperators Virtual Environ. 1998, 7, 225–240. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Braga, R. Ética na publicação de trabalhos científicos. Rev. Port. Med. Geral Fam. 2013, 29, 354–356. [Google Scholar] [CrossRef]
- Woronko, S.E.; Jessup, S.C.; Armstrong, T.; Anwyl-Irvine, A.L.; Dalmaijer, E.S.; Olatunji, B.O. A novel probe of attentional bias for threat in specific phobia: Application of the “MouseView.js” approach. J. Anxiety Disord. 2023, 96, 102700. [Google Scholar] [CrossRef]
- Tardif, N.; Therrien, C.É.; Bouchard, S. Re-Examining Psychological Mechanisms Underlying Virtual Reality-Based Exposure for Spider Phobia. Cyberpsychol. Behav. Soc. Netw. 2019, 22, 39–45. [Google Scholar] [CrossRef]
- Garcia-Palacios, A.; Hoffman, H.; Carlin, A.; Furness, T.A.; Botella, C. Virtual reality in the treatment of spider phobia: A controlled study. Behav. Res. Ther. 2002, 40, 983–993. [Google Scholar] [CrossRef]
- Sloan, T.; Telch, M.J. The effects of safety-seeking behavior and guided threat reappraisal on fear reduction during exposure: An experimental investigation. Behav. Res. Ther. 2002, 40, 235–251. [Google Scholar] [CrossRef]
- Kamphuis, J.H.; Telch, M.J. Effects of distraction and guided threat reappraisal on fear reduction during exposure-based treatments for specific fears. Behav. Res. Ther. 2000, 38, 1163–1181. [Google Scholar] [CrossRef]
- Marôco, J. Análise Estatística com o SPSS Statistics. 8a. ReportNumber, Lda. 2021. Available online: https://scholar.google.pt/citations?view_op=view_citation&hl=pt-PT&user=KNPseK8AAAAJ&citation_for_view=KNPseK8AAAAJ:K7YvBqpTqvwC (accessed on 9 April 2025).
- Lumley, T.; Diehr, P.; Emerson, S.; Chen, L. The importance of the normality assumption in large public health data sets. Annu. Rev. Public Health 2002, 23, 151–169. [Google Scholar] [CrossRef]
- Pereira, A.; Patrício, T. SPSS: Guia Prático de Utilização: Análise de Dados para Ciências Sociais e Psicologia, 8th ed.; Edições Silabo, Lda.: Lisboa, Spain, 2013; p. 256. [Google Scholar]
- Pestana, M.H.; Gageiro, J.N. Análise de Dados Para ciências Sociais: A Complementaridade do SPSS, 6th ed.; Robalo, M., Ed.; Edições Silabo, Lda.: Lisboa, Spain, 2014. [Google Scholar]
- Rzeźniczek, P.; Lipiak, A.; Bilski, B.; Laudańska-Krzemińska, I.; Cybulski, M.; Chawłowska, E. Exploring the Participant-Related Determinants of Simulator Sickness in a Physical Motion Car Rollover Simulation as Measured by the Simulator Sickness Questionnaire. Int. J. Environ. Res. Public Health 2020, 17, 7044. [Google Scholar] [CrossRef] [PubMed]
- Tovote, P.; Fadok, J.P.; Lüthi, A. Neuronal circuits for fear and anxiety. Nat. Rev. Neurosci. 2015, 16, 317–331. [Google Scholar] [CrossRef] [PubMed]
- Weech, S.; Kenny, S.; Barnett-Cowan, M. Presence and cybersickness in virtual reality are negatively related: A review. Front. Psychol. 2019, 10, 415654. [Google Scholar] [CrossRef] [PubMed]
- Albakri, G.; Bouaziz, R.; Alharthi, W.; Kammoun, S.; Al-Sarem, M.; Saeed, F.; Hadwan, M. Phobia Exposure Therapy Using Virtual and Augmented Reality: A Systematic Review. Appl. Sci. 2022, 12, 1672. [Google Scholar] [CrossRef]
- Distéfano, M.J.; Labandeira, L.P.; Tarnogol, F.M.; Mesurado, B. Presence, Cybersickness, Anxiety, and Heart Rate Variability in a Non-Clinical Population Using Virtual Reality Environments Designed For Specific Phobias’ Treatment. Psychol. Ment. Health Care 2020, 4, 2705–2732. [Google Scholar] [CrossRef]
- Park, S.H.; Lee, G.C. Full-immersion virtual reality: Adverse effects related to static balance. Neurosci. Lett. 2020, 733, 134974. [Google Scholar] [CrossRef]
- Rueda, J.; Lara, F. Virtual Reality and Empathy Enhancement: Ethical Aspects. Front. Robot. AI 2020, 7, 506984. [Google Scholar] [CrossRef]
- Kim, H.K.; Park, J.; Choi, Y.; Choe, M. Virtual reality sickness questionnaire (VRSQ): Motion sickness measurement index in a virtual reality environment. Appl. Ergon. 2018, 69, 66–73. [Google Scholar] [CrossRef]
- Benson, A.J.; Stott, J.R.R. Motion Sickness. In Ernsting’s Aviation and Space Medicine, 5th ed.; CRC Press: Boca Raton, FL, USA, 2023; pp. 781–796. [Google Scholar]
- LaViola, J.J. A discussion of cybersickness in virtual environments. ACM SIGCHI Bull. 2000, 32, 47–56. [Google Scholar] [CrossRef]
- Ramaseri Chandra, A.N.; El Jamiy, F.; Reza, H. A Systematic Survey on Cybersickness in Virtual Environments. Computers 2022, 11, 51. [Google Scholar] [CrossRef]
- Weech, S.; Kenny, S.; Lenizky, M.; Barnett-Cowan, M. Narrative and gaming experience interact to affect presence and cybersickness in virtual reality. Int. J. Hum. Comput. Stud. 2020, 138, 102398. [Google Scholar] [CrossRef]
- Alamirah, H.; Schweiker, M.; Azar, E. Immersive virtual environments for occupant comfort and adaptive behavior research—A comprehensive review of tools and applications. Build. Environ. 2022, 207, 108396. [Google Scholar] [CrossRef]
- Hale, K.S.; Stanney, K.M. Handbook of Virtual Environments: Design, Implementation, and Applications; CRC Press: Boca Raton, FL, USA, 2017; p. 1418. Available online: https://www.taylorfrancis.com/books/mono/10.1201/b17360/handbook-virtual-environments-kay-stanney-kelly-hale (accessed on 9 April 2025).
- Rebenitsch, L.; Owen, C. Review on cybersickness in applications and visual displays. Virtual Real. 2016, 20, 101–125. [Google Scholar] [CrossRef]
- Oh, H.; Son, W. Cybersickness and Its Severity Arising from Virtual Reality Content: A Comprehensive Study. Sensors 2022, 22, 1314. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Asnaani, A.; Vonk, I.J.J.; Sawyer, A.T.; Fang, A. The Efficacy of Cognitive Behavioral Therapy: A Review of Meta-analyses. Cogn. Ther. Res. 2012, 36, 427. [Google Scholar] [CrossRef]
- Eysenck, M.W. Anxiety: The Cognitive Perspective; Psychology Press: London, UK, 1992. [Google Scholar] [CrossRef]
- Craske, M.G.; Treanor, M.; Conway, C.C.; Zbozinek, T.; Vervliet, B. Maximizing Exposure Therapy: An Inhibitory Learning Approach. Behav. Res. Ther. 2014, 58, 10. [Google Scholar] [CrossRef]
- Sars, D.; van Minnen, A. On the use of exposure therapy in the treatment of anxiety disorders: A survey among cognitive behavioural therapists in the Netherlands. BMC Psychol. 2015, 3, 26. [Google Scholar] [CrossRef]
- Abramowitz, J.S.; Deacon, B.J.; Whiteside, S.P.H. Exposure Therapy for Anxiety: Principles and Practice; Guilford Publications: New York, NY, USA, 2019; p. 459. [Google Scholar]
- Tertuliano, M.L.; Lopes, I.F.; Coelho, T.; Fernandes, Â. Playing to Improve Memory: How Serious Games and Gamification Have Contributed to the Neurocognitive Rehabilitation of the Elderly; IGI Global Scientific Publishing: Hershey, PA, USA, 2023; pp. 187–207. [Google Scholar]
- Lumsden, J.; Edwards, E.A.; Lawrence, N.S.; Coyle, D.; Munafò, M.R. Gamification of cognitive assessment and cognitive training: A systematic review of applications and efficacy. JMIR Serious Games 2016, 4, e5888. [Google Scholar] [CrossRef]
- Dunsmoor, J.E.; Paz, R. Fear Generalization and Anxiety: Behavioral and Neural Mechanisms. Biol. Psychiatry 2015, 78, 336–343. [Google Scholar] [CrossRef]
- Parsons, T.D.; Rizzo, A.A. Affective outcomes of virtual reality exposure therapy for anxiety and specific phobias: A meta-analysis. J. Behav. Ther. Exp. Psychiatry 2008, 39, 250–261. [Google Scholar] [CrossRef]
- Opriş, D.; Pintea, S.; García-Palacios, A.; Botella, C.; Szamosközi, Ş.; David, D. Virtual reality exposure therapy in anxiety disorders: A quantitative meta-analysis. Depress. Anxiety 2012, 29, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Carl, E.; Stein, A.T.; Levihn-Coon, A.; Pogue, J.R.; Rothbaum, B.; Emmelkamp, P.; Asmundson, G.J.G.; Carlbring, P.; Powers, M.B. Virtual reality exposure therapy for anxiety and related disorders: A meta-analysis of randomized controlled trials. J. Anxiety Disord. 2019, 61, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Demir, M.; Köskün, T. Efficacy of Virtual Reality Exposure Therapy in the Treatment of Specific Phobias: A Systematic Review. Curr. Approaches Psychiatry 2023, 15, 562–576. [Google Scholar] [CrossRef]
- Freitas, J.R.; Velosa, V.H.; Abreu, L.T.; Jardim, R.L.; Santos, J.A.; Peres, B.; Campos, P.F. Virtual Reality Exposure Treatment in Phobias: A Systematic Review. Psychiatr. Q. 2021, 92, 1685–1710. [Google Scholar] [CrossRef]
- Meyerbröker, K.; Emmelkamp, P.M.G. Virtual Reality Exposure Therapy for Anxiety Disorders: The State of the Art. Stud. Comput. Intell. 2011, 337, 47–62. [Google Scholar]
- Rimer, E.; Husby, L.V.; Solem, S. Virtual Reality Exposure Therapy for Fear of Heights: Clinicians’ Attitudes Become More Positive After Trying VRET. Front. Psychol. 2021, 12, 671871. [Google Scholar] [CrossRef]
- Linares-Chamorro, M.; Domènech-Oller, N.; Jerez-Roig, J.; Piqué-Buisan, J. Immersive Therapy for Improving Anxiety in Health Professionals of a Regional Hospital during the COVID-19 Pandemic: A Quasi-Experimental Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 9793. [Google Scholar] [CrossRef]
- Freeman, D.; Haselton, P.; Freeman, J.; Spanlang, B.; Kishore, S.; Albery, E.; Denne, M.; Brown, P.; Slater, M.; Nickless, A. Automated psychological therapy using immersive virtual reality for treatment of fear of heights: A single-blind, parallel-group, randomised controlled trial. Lancet Psychiatry 2018, 5, 625. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).