
A Review of Behavioral and Pharmacological Treatments for Adult Trichotillomania

Abstract
:1. Background
Epidemiology
2. Proposed Causes
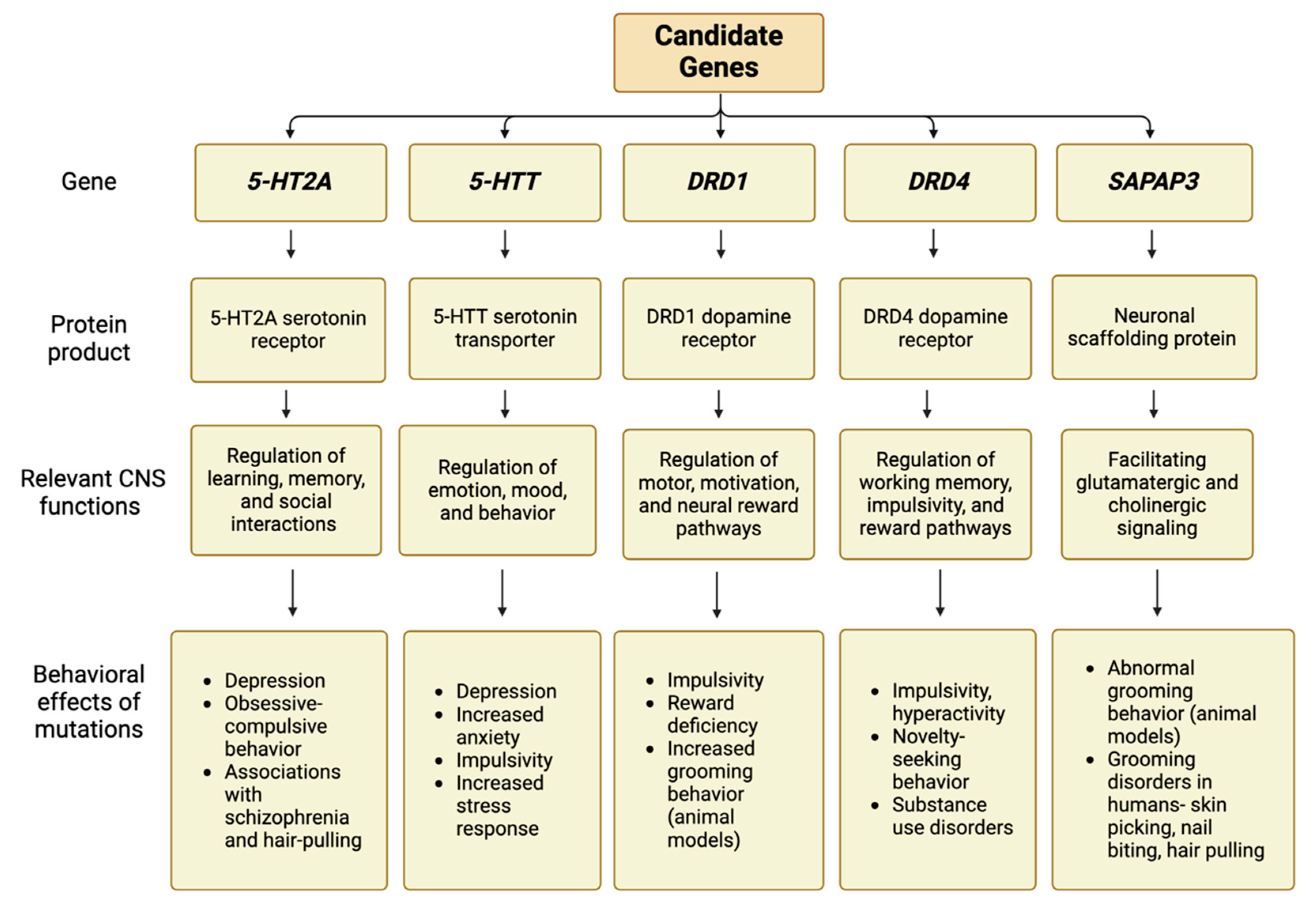
2.1. Genetic
2.2. Neurobiological
2.3. Environmental
3. Review Methodology
4. Treatment Approaches
4.1. Cognitive Behavioral Therapy (CBT)
4.2. Habit Reversal Training (HRT)
4.3. Acceptance and Commitment Therapy (ACT)
4.4. Decoupling Therapy (DC)
4.5. Dialectical Behavior Therapy (DBT)
4.6. Antipsychotics
4.7. Tricyclic Antidepressants (TCAs)
4.8. Selective Serotonin Reuptake Inhibitors (SSRIs)
4.9. N-Acetylcysteine (NAC)
4.10. Inositol
4.11. Naltrexone
4.12. Dronabinol
5. Discussion
6. Limitations
7. Conclusions and Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Clinical Scale | Description |
|---|---|
| Massachusetts General Hospital Hair-Pulling Scale (MGH-HPS) | The MGH-HPS is a 7-question, patient-rated assessment that utilizes a Likert scale to assess pulling severity and resistance/control abilities. Each question is scored from 0 to 4, with total scores ranging from 0 to 28. Higher scores reflect greater severity. This scale is particularly useful in documenting symptom change throughout treatment [81]. |
| NIMH-Trichotillomania Severity Scale (NIMH-TSS) and NIMH- Trichotillomania-Impairment Scale (NIMH-TIS) | The TSS is a 5-question, clinician-rated assessment asking about time spent pulling within the past week and day, ability to resist urges to pull, functional impairment, and level of associated distress. Total scores ranging from 0 to 25. Higher scores reflect greater symptom severity. The TIS is a 1-item, clinician-rated assessment, meant to provide a “snapshot” of the patient’s clinical presentation and severity. Scores range from 0 to 10, with higher scores reflecting greater severity [64]. |
| NIMH-Trichotillomania Physician Rating Scale (PRS) | The PRS is used to assess the severity of a patient’s trichotillomania symptoms. The baseline score is 10, with follow-up scores ranging from 0 to 20, with 0 indicating the absence of symptoms and 20 indicating “total incapacitation”, where virtually all waking hours are spent pulling [65]. |
| Clinical Global Impressions Severity and Improvement Scale (CGI) | The CGI is a clinician-rated assessment meant to gauge a patient’s global functioning prior to and after treatment administration, especially drug treatments. These scales measure current symptom severity and the level of improvement since the last assessment, with scores ranging from 1 (very much improved) to 7 (very much worse). The CGI is not specific for trichotillomania, as it has been used for a wide array of psychiatric disorders [81]. |
| Generic Body-Focused Repetitive Behavior Scale (GBS) | The GBS is an 8-item, patient-rated diagnostic scale devised in 2021. It was adapted from the Skin-Picking Scale-Revised (SPS-R) and Yale-Brown Obsessive–Compulsive Scale (Y-BOCS) in order to evaluate any body-focused repetitive behavior. Questions pertain to symptom severity and life impairment over the past week [92]. |
| Yale-Brown Obsessive–Compulsive Scale- Trichotillomania (Y-BOCS-TM) | Derived and adapted from the 67-question Yale-Brown Obsessive–Compulsive Scale (Y-BOCS), the Y-BOCS-TM is a 10-question, clinician-rated assessment measuring hair-pulling severity, specifically, intrusive thoughts and actual pulling behavior. Each question is scored from 0 to 5, with total scores ranging from 0 to 50. Higher scores indicate greater severity [64]. |
| The Psychiatric Institute Trichotillomania Scale (PITS) | The PITS rates trichotillomania severity and can be used for baseline and progress assessment over time. The PITS scores six items related to TTM: number of body sites, severity of hair loss, time spent pulling, resistance to pulling urges, severity of feelings regarding pulling, and interference with daily functioning. Total scores range from 0 to 42 [93]. |
| Severity Urge Resistance Frequency Scale (SURF) | The SURF is a collection of four, one-item questions that assess TTM symptom severity by quantifying hair-pulling urge and ability to resist the urge [35]. |
References
- Grant, J.E.; Chamberlain, S.R. Trichotillomania. Am. J. Psychiatry 2016, 173, 868–874. [Google Scholar] [CrossRef]
- França, K.; Kumar, A.; Castillo, D.; Jafferany, M.; Hyczy da Costa Neto, M.; Damevska, K.; Lotti, T. Trichotillomania (hair pulling disorder): Clinical characteristics, psychosocial aspects, treatment approaches, and ethical considerations. Dermatol. Ther. 2018, 32, e12622. [Google Scholar] [CrossRef]
- Mayo Clinic. Trichotillomania (Hair-Pulling Disorder)—Symptoms and Causes. Available online: https://www.mayoclinic.org/diseases-conditions/trichotillomania/symptoms-causes/syc-20355188 (accessed on 5 April 2022).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Grant, J.E.; Dougherty, D.D.; Chamberlain, S.R. Prevalence, gender correlates, and co-morbidity or trichotillomania. Psychiatry Res. 2020, 288, 112948. [Google Scholar] [CrossRef]
- Christenson, G.A.; Mackenzie, T.B.; Mitchell, J.E. Characteristics of 60 adult chronic hair pullers. Am. J. Psychiatry 1991, 148, 365–370. [Google Scholar] [CrossRef]
- Grant, J.E.; Redden, S.A.; Medeiros, G.C.; Tavares, H.; Odlaug, B.L.; Curley, E.E.; Keuthen, N.J. Trichotillomania and its clinical relationship to depression and anxiety. Int. J. Psychiatry Clin. Pract. 2017, 21, 302–306. [Google Scholar] [CrossRef]
- Gershuny, B.S.; Keuthen, N.J.; Gentes, E.L.; Russo, A.R.; Emmott, E.C.; Jameson, M.; Dougherty, D.D.; Loh, R.; Jenike, M.A. Current posttraumatic stress disorder and history of trauma in trichotillomania. J. Clin. Psychol. 2006, 62, 1521–1529. [Google Scholar] [CrossRef]
- Chesivoir, E.K.; Valle, S.; Grant, J.E. Comorbid trichotillomania and attention-deficit hyperactivity disorder in adults. Compr. Psychiatry 2022, 116, 152317. [Google Scholar] [CrossRef]
- Keuthen, N.J.; Curley, E.E.; Scharf, J.M.; Woods, D.W.; Lochner, C.; Stein, D.J.; Tung, E.S.; Greenberg, E.; Stewart, S.E.; Redden, S.A.; et al. Predictors of comorbid obsessive-compulsive disorder and skin-picking disorder in trichotillomania. Ann. Clin. Psychiatry 2016, 28, 280–288. [Google Scholar]
- Mamidi, P.; Gupta, K. Trichotillomania—An ayurvedic perspective. AYUHOM 2022, 9, 61–66. [Google Scholar] [CrossRef]
- Hemmings, S.; Kinnear, C.; Lochner, C.; Seedat, S.; Corfield, V.; Moolman-Smook, J.; Stein, D. Genetic correlates in trichotillomania—A case-control association study in the south african caucasian population. Isr. J. Psychiatry Relat. Sci. 2006, 43, 93–101. Available online: https://doctorsonly.co.il/wp-content/uploads/2011/12/2006_2_5.pdf (accessed on 12 April 2022).
- Zhang, G.; Stackman, R.W., Jr. The role of serotonin 5-HT2A receptors in memory and cognition. Front. Pharmacol. 2015, 6, 255. [Google Scholar] [CrossRef]
- De Deurwaerdere, P.; Chagraoui, A.; Di Giovanni, G. (Eds.) Multiple facets of serotonin modulation. In 5-HT Interaction with Other Neurotransmitters: Experimental Evidence and Therapeutic Relevance—Part B; Elsevier Inc.: Amsterdam, The Netherlands, 2021; pp. 3–39. ISBN 978-0-444-64258-5. [Google Scholar]
- Yokoyama, J.S.; Bonham, L.W.; Sturm, V.E.; Adhimoolam, B.; Karydas, A.; Coppola, G.; Miller, B.L.; Rankin, K.P. The 5-HTTLPR variant in the serotonin transporter gene modifies degeneration of brain regions important for emotion in behavioral variant frontotemporal dementia. NeuroImage Clin. 2015, 9, 283–290. [Google Scholar] [CrossRef]
- Bocchio, M.; Fucsina, G.; Oikonomidis, L.; McHugh, S.B.; Bannerman, D.M.; Sharp, T.; Capogna, M. Increased serotonin transporter expression reduces fear and recruitment of parvalbumin interneurons of the amygdala. Neuropsychopharmacology 2015, 40, 3015–3026. [Google Scholar] [CrossRef]
- Molloy, A.G.; Waddington, J.L. Assessment of grooming and other behavioural responses to the D1 dopamine receptor agonist SK & F 38393 and its R- and S-enantiomers in the intact adult rat. Psychopharmacology 1987, 92, 164–168. [Google Scholar] [CrossRef]
- Wachtel, S.R.; Brooderson, R.J.; White, F.J. Parametric and pharmacological analyses of the enhanced grooming response elicited by the D1 dopamine receptor agonist SKF 38393 in the rat. Psychopharmacology 1992, 109, 41–48. [Google Scholar] [CrossRef]
- Bienvenu, O.J.; Wang, Y.; Shugart, Y.Y.; Welch, J.M.; Grados, M.A.; Fyer, A.J.; Rauch, S.L.; McCracken, J.T.; Rasmussen, S.A.; Murphy, D.L.; et al. Sapap3 and pathological grooming in humans: Results from the OCD collaborative genetics study. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2009, 150B, 710–720. [Google Scholar] [CrossRef]
- O’Sullivan, R.L.; Rauch, S.L.; Breiter, H.C.; Grachev, I.D.; Baer, L.; Kennedy, D.N.; Keuthen, N.J.; Savage, C.R.; Manzo, P.A.; Caviness, V.S.; et al. Reduced basal ganglia volumes in trichotillomania measured via morphometric magnetic resonance imaging. Biol. Psychiatry 1997, 42, 39–45. [Google Scholar] [CrossRef]
- Ghandili, M.; Munakomi, S. Neuroanatomy, Putamen. In StatPearls; StatPearls: Tampa, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK542170/#:~:text=The%20putamen%20is%20involved%20in,%2C%20cognitive%20functioning%2C%20and%20addiction (accessed on 3 February 2023).
- Knierim, J. Neuroscience Online: An Electronic Textbook for the Neurosciences. Department of Neurobiology and Anatomy; The University of Texas Medical School at Houston: Houston, TX, USA, 2020; Chapter 5, Section 3: Cerebellum. [Google Scholar]
- Keuthen, N.J.; Makris, N.; Schlerf, J.E.; Martis, B.; Savage, C.R.; McMullin, K.; Seidman, L.J.; Schmahmann, J.D.; Kennedy, D.N.; Hodge, S.M.; et al. Evidence for reduced cerebellar volumes in trichotillomania. Biol. Psychiatry 2007, 61, 374–381. [Google Scholar] [CrossRef]
- Stein, D.J. Functional brain imaging and pharmacotherapy in trichotillomania Single photon emission computed tomography before and after treatment with the selective serotonin reuptake inhibitor citalopram. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2002, 26, 885–890. [Google Scholar] [CrossRef]
- Chamberlain, S.R.; Hampshire, A.; Menzies, L.A.; Garyfallidis, E.; Grant, J.E.; Odlaug, B.L.; Craig, K.; Fineberg, N.; Sahakian, B.J. Reduced brain white matter integrity in trichotillomania. Arch. Gen. Psychiatry 2010, 67, 965. [Google Scholar] [CrossRef]
- Chamberlain, S.R.; Fineberg, N.A.; Blackwell, A.D.; Robbins, T.W.; Sahakian, B.J. Motor inhibition and cognitive flexibility in obsessive-compulsive disorder and trichotillomania. Am. J. Psychiatry 2006, 163, 1282–1284. [Google Scholar] [CrossRef]
- Flessner, C.A.; Francazio, S.; Murphy, Y.E.; Brennan, E. An examination of executive functioning in young adult exhibiting body-focused repetitive behaviors. J. Nerv. Men. Dis. 2015, 203, 555–558. [Google Scholar] [CrossRef]
- Christenson, G.A.; Mansueto, C.S. Trichotillomania: Descriptive Characteristics and Phenomenology; American Psychiatric Press, Inc.: Washington, DC, USA, 1999; pp. 1–41. ISBN 0-88048-759-3. [Google Scholar]
- Boughn, S.; Holdom, J.J. The relationship of violence and trichotillomania. J. Nurs. Scholarsh. 2003, 35, 165–170. [Google Scholar] [CrossRef]
- Keuthen, N.J.; Fama, J.; Altenburger, E.A.; Allen, A.; Raff, A.; Pauls, D. Family environment in adolescent trichotillomania. J. Obs.-Compuls. Relat. Dis. 2013, 2, 366–374. [Google Scholar] [CrossRef]
- American Psychological Association. What Is Cognitive Behavioral Therapy? Available online: https://www.apa.org/ptsd-guideline/patients-and-families/cognitive-behavioral (accessed on 12 February 2022).
- Ninan, P.T.; Rothbaum, B.O.; Marsteller, F.A.; Knight, B.T.; Eccard, M.B. A placebo-controlled trial of cognitive-behavioral therapy and clomipramine in trichotillomania. J. Clin. Psychiatry 2000, 61, 47–50. [Google Scholar] [CrossRef]
- van Minnen, A.; Hoogduin, K.A.L.; Keijsers, G.P.J.; Hellenbrand, I.; Hendriks, G.J. Treatment of trichotillomania with behavioral therapy or fluoxetine: A randomized, waiting-list control study. Arch. Gen. Psychiatry 2003, 60, 517. [Google Scholar] [CrossRef]
- Toledo, E.L.; Muniz, E.D.T.; Brito, A.M.C.; Abreu, C.N.; de Tavares, H. Group Treatment for trichotillomania: Cognitive-behavioral therapy versus supportive therapy. J. Clin. Psychiatry 2014, 76, 7881. [Google Scholar] [CrossRef]
- Keijsers, G.P.J.; Maas, J.; van Opdorp, A.; van Minnen, A. Addressing self-control cognitions in the treatment of trichotillomania: A randomized controlled trial comparing cognitive therapy to behaviour therapy. Cogn. Ther. Res. 2016, 40, 522–531. [Google Scholar] [CrossRef]
- Maas, J.; Keijsers, G.P.J.; Rinck, M.; Becker, E.S. Does cognitive bias modification prior to standard brief cognitive behavior therapy reduce relapse rates in hair pulling disorder? A double-blind randomized controlled trial. J. Soc. Clin. Psychol. 2018, 37, 453–479. [Google Scholar] [CrossRef]
- Slikboer, R.; Rehm, I.C.; Lam, S.; Maloney, A.; Nedeljkovic, M. A brief, residential peer-support retreat for trichotillomania: A mixed methods evaluation. Aust. Psychol. 2020, 55, 169–180. [Google Scholar] [CrossRef]
- Golomb, R.; Franklin, M.; Grant, J.; Keuthen, N.; Mansueto, C.; Mouton-Odum, S.; Woods, D. Expert Consensus Treatment Guidelines for Body-Focused Repetitive Behaviors. Available online: https://www.bfrb.org/resources/expert-consensus-treatment-guidelines-for-body-focused-repetitive-behaviors (accessed on 23 February 2022).
- Shareh, H. A preliminary investigation of metacognitive therapy and habit reversal as a treatment for trichotillomania. Behav. Cog. Psychother. 2017, 46, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Woods, D.W.; Wetterneck, C.T.; Flessner, C.A. A controlled evaluation of acceptance and commitment therapy plus habit reversal for trichotillomania. Behav. Res. Ther. 2006, 44, 639–656. [Google Scholar] [CrossRef] [PubMed]
- Rogers, K.; Banis, M.; Falkenstein, M.J.; Malloy, E.J.; McDonough, L.; Nelson, S.O.; Rusch, N.; Haaga, D.A.F. Stepped care in the treatment of trichotillomania. J. Consult. Clin. Psychol. 2014, 82, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, D.D.; Loh, R.; Jenike, M.A.; Keuthen, N.J. Single modality versus dual modality treatment for trichotillomania: Sertraline, behavioral therapy, or both? J. Clin. Psychiatry 2006, 67, 1086–1092. [Google Scholar] [CrossRef] [PubMed]
- Twohig, M.P.; Woods, D.W. A preliminary investigation of acceptance and commitment therapy and habit reversal as a treatment for trichotillomania. Behav. Ther. 2004, 35, 803–820. [Google Scholar] [CrossRef]
- Moritz, S.; Penney, D.; Ahmed, K.; Schmotz, S. A head-to-head comparison of three self-help techniques to reduce body-focused repetitive behaviors. Behav. Modif. 2021, 46, 014544552110107. [Google Scholar] [CrossRef] [PubMed]
- Association for Contextual Behavioral Science. Acceptance and Commitment Therapy. Available online: https://contextualscience.org/act (accessed on 3 March 2022).
- Lee, E.B.; Homan, K.J.; Morrison, K.L.; Ong, C.W.; Levin, M.E.; Twohig, M.P. Acceptance and commitment therapy for trichotillomania: A controlled trial of adults and adolescents. Behav. Modif. 2013, 44, 70–91. Available online: https://pubmed.ncbi.nlm.nih.gov/30117327/ (accessed on 14 May 2022). [CrossRef]
- Crosby, J.M.; Dehlin, J.P.; Mitchell, P.R.; Twohig, M.P. Acceptance and commitment therapy and habit reversal training for the treatment of trichotillomania. Cogn. Behav. Pract. 2012, 19, 595–605. [Google Scholar] [CrossRef]
- Moritz, S.; Rufer, M. Movement decoupling: A self-help intervention for the treatment of trichotillomania. J. Behav. Ther. Exper. Psychiatry 2011, 42, 74–80. [Google Scholar] [CrossRef]
- Weidt, S.; Klaghofer, R.; Kuenburg, A.; Bruehl, A.B.; Delsignore, A.; Moritz, S.; Rufer, M. Internet-based self-help for trichotillomania: A randomized controlled study comparing decoupling and progressive muscle relaxation. Psychother. Psychosom. 2015, 84, 359–367. [Google Scholar] [CrossRef]
- Lebow, J. Overview of Psychotherapies. Available online: https://www.uptodate.com/contents/overview-of-psychotherapies/print (accessed on 24 April 2022).
- Keuthen, N.J.; Rothbaum, B.O.; Welch, S.S.; Taylor, C.; Falkenstein, M.; Heekin, M.; Jordan, C.A.; Timpano, K.; Meunier, S.; Fama, J.; et al. Pilot trial of dialectical behavior therapy-enhanced habit reversal for trichotillomania. Depress. Anxiety 2010, 27, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Keuthen, N.J.; Rothbaum, B.O.; Falkenstein, M.J.; Meunier, S.; Timpano, K.R.; Jenike, M.A.; Welch, S.S. DBT-enhanced habit reversal treatment for trichotillomania: 3-and 6-month follow-up results. Depress. Anxiety 2010, 28, 310–313. [Google Scholar] [CrossRef] [PubMed]
- Keuthen, N.J.; Rothbaum, B.O.; Fama, J.; Altenburger, E.; Falkenstein, M.J.; Sprich, S.; Kearns, M.C.; Meunier, S.; Jenike, M.A.; Welch, S.S. DBT-enhanced cognitive-behavioral treatment for trichotillomania: A randomized controlled trial. J. Behav. Addict. 2012, 1, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Chokhawala, K.; Stevens, L. Antipsychotic medications. In StatPearls; StatPearls: Tampa, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK519503/ (accessed on 14 March 2023).
- Van Ameringen, M.; Mancini, C.; Oakman, J.M.; Farvolden, P. The potential role of haloperidol in the treatment of trichotillomania. J. Affect. Disord. 1999, 56, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Stein, D.J.; Hollander, E. Low-dose pimozide augmentation of serotonin reuptake blockers in the treatment of trichotillomania. J. Clin. Psychiatry 1992, 53, 123–126. Available online: https://pubmed.ncbi.nlm.nih.gov/1532960/ (accessed on 22 May 2022). [PubMed]
- Stewart, R.S.; Nejtek, V.A. An open-label, flexible-dose study of olanzapine in the treatment of trichotillomania. J. Clin. Psychiatry 2003, 64, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Van Ameringen, M.; Mancini, C.; Patterson, B.; Bennett, M.; Oakman, J. A randomized, double-blind, placebo-controlled trial of olanzapine in the treatment of trichotillomania. J. Clin. Psychiatry 2010, 71, 1336–1343. [Google Scholar] [CrossRef] [PubMed]
- Stein, D.J.; Bouwer, C.; Hawkridge, S.; Emsley, R.A. Risperidone augmentation of serotonin reuptake inhibitors in obsessive compulsive and related disorders. J. Clin. Psychiatry 1997, 58, 119–122. [Google Scholar] [CrossRef]
- Epperson, C.N.; Fasula, D.; Wasylink, S.; Pride, L.H.; McDougle, J. Risperidone addition in serotonin reuptake inhibitor-resistant trichotillomania: Three cases. J. Child Adolesc. Psychopharmacol. 1999, 9, 43–49. [Google Scholar] [CrossRef]
- Oravecz, R.; Štuhec, M. Trichotillomania successfully treated with risperidone and naltrexone: A geriatric case report. J. Am. Med. Dir. Assoc. 2014, 15, 301–302. [Google Scholar] [CrossRef]
- White, M.P.; Koran, L.M. Open-label trial of aripiprazole in the treatment of trichotillomania. J. Clin. Psychopharmacol. 2011, 31, 503–506. [Google Scholar] [CrossRef] [PubMed]
- Moraczewski, J.; Awosika, A.O.; Aedma, K.K. Tricyclic antidepressants. In StatPearls; StatPearls: Tampa, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK557791/#:~:text=TCAs%20have%20the%20potential%20to (accessed on 15 September 2023).
- Woods, D.W.; Houghton, D.C. Diagnosis, evaluation, and management of trichotillomania. Psychiatr. Clin. N. Am. 2014, 37, 301–317. [Google Scholar] [CrossRef] [PubMed]
- Swedo, S.E.; Leonard, H.L.; Rapoport, J.L.; Lenane, M.C.; Goldberger, E.L.; Cheslow, D.L. A double-blind comparison of clomipramine and desipramine in the treatment of trichotillomania (Hair Pulling). N. Eng. J. Med. 1989, 321, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Pollard, C.A.; Ibe, I.O.; Krojanker, D.N.; Kitchen, A.D.; Bronson, S.S.; Flynn, T.M. Clomipramine treatment of trichotillomania: A follow-up report on four cases. J. Clin. Psychiatry 1991, 52, 128–130. Available online: https://pubmed.ncbi.nlm.nih.gov/2005076/ (accessed on 24 May 2022). [PubMed]
- Christenson, G.A.; Mackenzie, T.B.; Mitchel, J.E.; Callies, A.L. A placebo-controlled, double-blind crossover study of fluoxetine in trichotillomania. Am. J. Psychiatry 1991, 148, 1566–1571. [Google Scholar] [CrossRef] [PubMed]
- Streichenwein, S.M.; Thornby, J.I. A long-term, double-blind, placebo-controlled crossover trial of the efficacy of fluoxetine for trichotillomania. Am. J. Psychiatry 1995, 152, 1192–1196. [Google Scholar] [CrossRef]
- Koran, L.M.; Ringold, A.; Hewlett, W. Fluoxetine for trichotillomania: An open clinical trial. Psychopharmacol. Bull. 1992, 28, 145–149. Available online: https://pubmed.ncbi.nlm.nih.gov/1513916/ (accessed on 25 May 2022). [PubMed]
- Winchel, R.M.; Jones, J.S.; Stanley, B.; Molcho, A.; Stanley, M. Clinical characteristics of trichotillomania and its response to fluoxetine. J. Clin. Psychiatry 1992, 53, 304–308. Available online: https://pubmed.ncbi.nlm.nih.gov/1517191/ (accessed on 25 May 2022). [PubMed]
- Iancu, I.; Weizman, A.; Kindler, S.; Sasson, Y.; Zohar, J. Serotonergic drugs in trichotillomania: Treatment results in 12 patients. J. Nerv. Men. Dis. 1996, 184, 641–644. [Google Scholar] [CrossRef]
- Christenson, G.A.; Crow, S.J.; Mitchell, J.E.; Mackenzie, T.B.; Crosby, R.D.; Falls, J. Fluvoxamine in the Treatment of Trichotillomania: An 8-Week, Open-Label Study. CNS Spectr. 1998, 3, 64–71. [Google Scholar] [CrossRef]
- Stanley, M.A.; Breckenridge, J.K.; Swann, A.C.; Freeman, E.B.; Reich, L. Fluvoxamine treatment of trichotillomania. J. Clin. Psychopharmacol. 1997, 17, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Stein, D.J.; Bouwer, C.; Maud, C.M. Use of the selective serotonin reuptake inhibitor citalopram in treatment of trichotillomania. Eur. Arch. Psychiatry Clin. Neurosci. 1997, 247, 234–236. [Google Scholar] [CrossRef]
- Gadde, K.M.; Wagner, H.R., II; Connor, K.M.; Foust, M.S. Escitalopram treatment of trichotillomania. Int. Clin. Psychopharmacol. 2007, 22, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Porton, B.; Greenberg, B.D.; Askland, K.; Serra, L.M.; Gesmonde, J.; Rudnick, G.; Kao, H.-T. Isoforms of the neuronal glutamate transporter gene, SLC1A1/EAAC1, negatively modulate glutamate uptake: Relevance to obsessive-compulsive disorder. Transl. Psychiatry 2013, 3, e259. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.E.; Odlaug, B.L.; Won Kim, S. N-Acetylcysteine, a glutamate modulator, in the treatment of trichotillomania. Arch. Gen. Psychiatry 2009, 66, 756. [Google Scholar] [CrossRef] [PubMed]
- Vieira, G.d.L.T.; Lossie, A.C.; Lay, D.C.; Radcliffe, J.S.; Garner, J.P. Preventing, treating, and predicting barbering: A fundamental role for biomarkers of oxidative stress in a mouse model of trichotillomania. PLoS ONE 2017, 12, e0175222. [Google Scholar] [CrossRef] [PubMed]
- Braun, T.L.; Patel, V.; DeBord, L.C.; Rosen, T. A review of n-acetylcysteine in the treatment of grooming disorders. Int. J. Dermatol. 2019, 58, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues-Barata, A.; Rodríguez-Pichardo, A.; Tosti, A.; Camacho-Martínez, F. N-acetylcysteine in the treatment of trichotillomania. Int. J. Trichology 2012, 4, 176. [Google Scholar] [CrossRef] [PubMed]
- Leppink, E.W.; Redden, S.A.; Grant, J.E. A double-blind, placebo-controlled study of inositol in trichotillomania. Int. Clin. Psychopharmacol. 2017, 32, 107–114. [Google Scholar] [CrossRef]
- Fux, M.; Levine, J.; Aviv, A.; Belmaker, R.H. Inositol treatment of obsessive-compulsive disorder. Am. J. Psychiatry 1996, 153, 1219–1221. [Google Scholar] [CrossRef]
- Seedat, S.; Stein, D.J.; Harvey, B.H. Inositol in the Treatment of Trichotillomania and Compulsive Skin Picking. J. Clin. Psychiatry 2001, 62, 60–61. [Google Scholar] [CrossRef] [PubMed]
- Cleveland Clinic. Opioid Antagonist. Available online: https://my.clevelandclinic.org/health/treatments/24878-opioid-antagonist (accessed on 4 January 2024).
- Grant, J.E.; Odlaug, B.L.; Schreiber, L.; Kim, S.W. The opiate antagonist, naltrexone, in the treatment of trichotillomania. Results of a double blind, placebo-controlled study. J. Clin. Psychopharmacol. 2014, 34, 134–138. [Google Scholar] [CrossRef]
- O’Donnell, B.; Meissner, H.; Gupta, V. Dronabinol. In StatPearls; StatPearls: Tampa, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK557531/ (accessed on 19 January 2024).
- Herkenham, M.; Lynn, A.B.; Little, M.D.; Johnson, M.R.; Melvin, L.S.; de Costa, B.R.; Rice, K.C. Cannabinoid receptor localization in the brain. Proc. Natl. Acad. Sci. USA 1990, 87, 1932–1936. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.E.; Odlaug, B.L.; Chamberlain, S.R.; Kim, S.W. Dronabinol, a cannabinoid agonist, reduces hair pulling in trichotillomania: A pilot study. Psychopharmacology 2011, 218, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.E.; Valle, S.; Chesivoir, E.; Ehsan, D. Tetrahydrocannabinol fails to reduce hair pulling and skin picking: Results of a double-blind, placebo-controlled study of dronabinol. Int. J. Clin. Psychopharmacol. 2022, 37, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos Tenório, M.C.; Graciliano, N.G.; Moura, F.A.; de Oliveira, A.C.M.; Goulart, M.O.F. N-Acetylcysteine (NAC): Impacts on human health. Antioxidants 2021, 10, 967. [Google Scholar] [CrossRef] [PubMed]
- Cleveland Clinic. What Is Inositol? Available online: https://my.clevelandclinic.org/health/drugs/25173-inositol (accessed on 30 October 2023).
- Moritz, S.; Gallinat, C.; Weidinger, S.; Bruhns, A.; Lion, D.; Snorrason, I.; Keuthen, N.; Schmotz, S.; Penney, D. The generic BFRB scale-8 (GBS-8): A transdiagnostic scale to measure the severity of body-focused repetitive behaviors. Behav. Cogn. Psychother. 2022, 50, 620–628. [Google Scholar] [CrossRef]
- Winchel, R.M.; Jones, J.S.; Molcho, A.; Parsons, B.; Stanley, B.; Stanley, M. The psychiatric institute trichotillomania scale (PITS). Psychopharmacol. Bull. 1992, 28, 463–476. Available online: https://pubmed.ncbi.nlm.nih.gov/1296224/ (accessed on 30 October 2023).

| First Author, Year | Intervention | Study Design | Treatment Group | Control or Placebo Group(s) | Study Duration | Follow-Up | Clinical Scales or Assessments Used | Intervention Outcomes |
|---|---|---|---|---|---|---|---|---|
| Ninan, 2000 [32] | CBT | RCT: parallel design | n = 6 | Clomipramine n = 5; placebo n = 6 | 9 weeks | None | NIMH-TSS, NIMH-TIS, CGI | CBT significantly more effective than Clomipramine and placebo groups. |
| van Minnen, 2003 [33] | CBT | RCT: parallel design | n = 14 | Fluoxetine n = 11; waitlist n = 15 | 12 weeks | None | MGH-HPS | CBT superior to Fluoxetine and waitlist groups. |
| Toledo, 2015 [34] | CBT | RCT: parallel design | n = 22 | Supportive therapy n = 22 | 22 weeks | None | MGH-HPS, CGI | Significant improvement with CBT compared to supportive therapy. |
| Keijsers, 2016 [35] | CBT | RCT: parallel design | n = 26 | Behavior therapy n = 22 | 12 weeks | 3, 12, 24 months | MGH-HPS, SURF | No significant difference in improvement between groups. |
| Mass, 2018 [36] | CBT | RCT: parallel design | n = 27 | Cognitive bias training and CBT n = 27 | 18 weeks | 1, 3, 12 months | MGH-HPS, SURF | No significant differences in improvement between groups. Significant relapse in both groups by 12 month follow-up. |
| Slikboer, 2020 [37] | CBT | Uncontrolled, longitudinal | n = 6 | None | 3 days | 6, 12 months | MGH-HPS | All subjects had varying levels of responsiveness and relapse rates. |
| Shareh, 2017 [39] | HRT | RCT: parallel design | n = 22 | Waitlist n = 17 | 8 weeks | 1, 6, 12 months | MGH-HPS, Y-BOCS-TM | Significant improvement with HRT compared to waitlist group. |
| Rogers, 2014 [41] | BT, then HRT | RCT: parallel design | n = 41 | BT alone n = 19; waitlist n = 30 | 18 weeks | 3 months | MGH-HPS, PITS | Significant improvement with BT and HRT compared to BT and waitlist groups. |
| Dougherty, 2006 [42] | HRT | RCT: parallel design | n = 6 | HRT and Sertraline n = 11 | 22 weeks | None | MGH-HPS, CGI | HRT and Sertraline superior to HRT alone. |
| Twohig, 2004 [43] | HRT | Case series | n = 6 | None | 7 weeks | 3 months | MGH-HPS | A total of 67% considered responders to treatment. Of responders, 75% maintained progress at follow-up. |
| Moritz, 2021 [44] | HRT | RCT: parallel design | n = 17 | DC therapy n = 27 | 4 weeks | None | GBS | Both groups with statistically significant improvements, but no significant difference between groups. |
| Woods, 2006 [40] | HRT + ACT | RCT: parallel design | n = 12 | Waitlist n = 13 | 12 weeks | 3 months | MGH-HPS, NIMH-TIS | Significant improvement with ACT and HRT compared to waitlist group. |
| Crosby, 2012 [47] | HRT + ACT | Open clinical trial | n = 5 | None | 8 weeks | 3 months | MGH-HPS, daily self-tracking | All responded to treatment; 40% maintained progress at follow-up. |
| Lee, 2018 [46] | ACT | RCT: parallel design | n = 12 | Waitlist n = 13 | 10 weeks | 3 months | MGH-HPS, daily self-tracking | Significant improvement with ACT compared to waitlist group. |
| Moritz, 2011 [48] | DC | RCT: parallel design | n = 20 | PMR n = 20 | 4 weeks | None | MGH-HPS | Significant improvement with DC compared to PMR. |
| Weidt, 2015 [49] | DC | RCT: parallel design | n = 55 | PMR n = 50 | 4 weeks | 6 months | MGH-HPS | No statistically significant difference between DC and PMR groups. |
| * Moritz, 2021 [44] | DC | RCT: parallel design | n = 27 | HRT n = 17 | 4 weeks | None | GBS | No statistically significant difference between DC and HRT groups. |
| Keuthen, 2010 [51,52] | DBT | Open clinical trial | n = 10 | None | 11 weeks | 3, 6 months | PITS, MGH-HPS, CGI, NIMH-TIS | A total of 82% considered either partial or full responders. |
| Keuthen, 2012 [53] | DBT | RCT: parallel design | n = 20 | MAC n = 18 | 11 weeks | 3, 6 months | PITS, MGH-HPS, NIMH-TSS and TIS, CGI | Significant improvement with DBT compared to MAC group. |
| * van Minnen, 2003 [33] | SSRI, Fluoxetine | RCT: parallel design | n = 11 | Behavior therapy n = 14; waitlist n = 15 | 12 weeks | None | MGH-HPS | No statistically significant difference between Fluoxetine and waitlist groups. Behavior therapy superior to both. |
| Christenson, 1991 [67] | SSRI, Fluoxetine | RCT: crossover | n = 15 | Placebo n = 15 | 6 weeks per treatment, 5 week washout | None | Various patient-reported measures | No significant difference between groups. |
| Streichenwein, 1995 [68] | SSRI, Fluoxetine | RCT: crossover | n = 16 | Placebo n = 16 | 12 weeks per treatment, 5 week washout | None | Physical exam, patient-reported severity and number of hairs pulled | No significant difference between groups. |
| Koran, 1992 [69] | SSRI, Fluoxetine | Open-label | n = 13 | None | 8–12 weeks | None | Y-BOCS-TM | A total of 53% considered responders. |
| Winchel, 1992 [70] | SSRI, Fluoxetine | Open-label | n = 12 | None | 16 weeks | None | MGH-HPS, PITS | A total of 67% considered responders. |
| Iancu, 1996 [71] | SSRI, Fluoxetine | Open-label | n = 6 | None | 6–20 weeks | None | Patient-reported quantity and frequency of hairs pulled | A total of 17% considered responders. |
| Stanley, 1997 [73] | SSRI, Fluvoxamine | Open-label | n = 13 | None | 12 weeks | None | Y-BOCS-TM | Significant improvements in some severity measures. Significant improvement in compulsion and resistance measures. |
| Christenson, 1998 [72] | SSRI, Fluvoxamine | Open-label | n = 14 | None | 8 weeks | 6 months | NIMH-TSS, NIMH-TIS, NIMH-PRS, patient-reported hair-pulling episodes | A total of 29% considered responders. Regression towards baseline scores at follow-up. |
| Stein, 1997 [74] | SSRI, Citalopram | Open-label | n = 13 | None | 12 weeks | None | Y-BOCS-TM, CGI, NIMH | A total of 39% considered responders. |
| Gadde, 2007 [75] | SSRI, Escitalopram | Open-label | n = 16 | None | 12 weeks | None | CGI, NIMH-TSS | A total of 50% considered responders. |
| Van Ameringen, 1999 [55] | Antipsychotic, Haloperidol alone or with an SSRI | Open-label | n = 9 | None | Not specified | None | Patient-reported hair-pulling episodes, pulling site depilation severity | A total of 89% considered responders. |
| Stein, 1992 [56] | Antipsychotic, Pimozide + SSRI | Open-label | n = 7 | None | Not specified | None | CGI | A total of 86% considered responders. |
| Stewart, 2003 [57] | Antipsychotic, Olanzapine | Open-label | n = 13 | None | 12 weeks | 1 month | MGH-HPS, CGI | All subjects responded; 33% had relapsed at follow-up. |
| Van Ameringen, 2010 [58] | Antipsychotic, Olanzapine | RCT: parallel design | n = 13 | Placebo n = 12 | 12 weeks | 12 months | Y-BOCS-TM, CGI | Significant improvement with Olanzapine compared to placebo group. |
| Epperson, 1999 [60] | Antipsychotic, Risperidone + SSRI or Perphenazine | Case series | n = 3 | None | 6–30 weeks | None-8 months | Y-BOCS-TM, PITS | All subjects responded, with varying levels of symptom improvement. |
| Stein, 1997 [59] | Antipsychotic, Risperidone + SSRI | Open-label | n = 5 | None | 4 weeks | None | Y-BOCS-TM, CGI | A total of 60% considered responders. |
| Oravecz, 2014 [61] | Risperidone + Naltrexone | Case study | n = 1 | None | 2 weeks | None | None | Subject responded after two weeks of treatment. |
| White, 2011 [62] | Antipsychotic, Aripiprazole | Open-label | n = 11 | None | 8 weeks | None | MGH-HPS, CGI | A total of 64% considered responders. |
| Swedo, 1989 [65] | TCA, Clomipramine and Desipramine | RCT: crossover | n = 13 | None | 10 weeks, no washout | 4, 6 months | NIMH-TIS, NIMH-TSS, NIMH-PRS | Clomipramine statistically superior to Desipramine. |
| * Ninan 2000 [32] | TCA, Clomipramine | RCT: parallel design | n = 5 | CBT n = 6; placebo n = 6 | 9 weeks | None | NIMH-TSS, NIMH-TIS, CGI-I | No statistically significant difference between Clomipramine and placebo groups. CBT significantly superior to both. |
| Pollard, 1991 [66] | TCA, Clomipramine | Case series | n = 4 | None | Not specified | 3 months | Unspecified | All subjects responded, but 75% relapsed at follow-up. |
| Grant, 2009 [77] | NAC | RCT: parallel design | n = 22 | Placebo n = 22 | 12 weeks | None | MGH-HPS, CGI, PITS | Significant improvement with NAC compared to placebo. |
| Rodrigues-Barata, 2012 [80] | NAC | Case series | n = 2 | None | 3 months | 6 months | Physician assessment of hair growth | Both subjects responded to treatment. |
| Leppink, 2017 [81] | Inositol | RCT: parallel design | n = 19 | Placebo n = 12 | 10 weeks | None | MGH-HPS, NIMH-TSS, CGI | No significant difference between groups |
| Seedat, 2001 [83] | Inositol | Case series | n = 2 | None | 8–12 weeks | None | CGI | Both subjects responded to treatment. |
| Grant, 2014 [85] | Naltrexone | RCT: parallel design | n = 20 | Placebo n = 24 | 8 weeks | None | MGH-HPS, NIMH-TSS | No significant difference between groups. |
| Grant, 2011 [88] | Dronabinol | Open-label | n = 12 | None | 12 weeks | None | MGH-HPS, CGI | A total of 67% considered responders. |
| Grant, 2022 [89] | Dronabinol | RCT: parallel design | n = 34 | Placebo n = 16 | 10 weeks | None | NIMH-TSS, CGI | No significant difference between groups. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bennett, L.P.; Ryznar, R. A Review of Behavioral and Pharmacological Treatments for Adult Trichotillomania. Psychol. Int. 2024, 6, 509-530. https://doi.org/10.3390/psycholint6020031
Bennett LP, Ryznar R. A Review of Behavioral and Pharmacological Treatments for Adult Trichotillomania. Psychology International. 2024; 6(2):509-530. https://doi.org/10.3390/psycholint6020031
Chicago/Turabian StyleBennett, Lauren Parris, and Rebecca Ryznar. 2024. "A Review of Behavioral and Pharmacological Treatments for Adult Trichotillomania" Psychology International 6, no. 2: 509-530. https://doi.org/10.3390/psycholint6020031
APA StyleBennett, L. P., & Ryznar, R. (2024). A Review of Behavioral and Pharmacological Treatments for Adult Trichotillomania. Psychology International, 6(2), 509-530. https://doi.org/10.3390/psycholint6020031