Effects of Artificial Texture Insoles and Foot Arches on Improving Arch Collapse in Flat Feet


Abstract
:1. Introduction
2. Subjects, Materials and Methods
2.1. Subjects
2.2. Materials
2.2.1. MP-5 Footprint Device
2.2.2. MP-1 Plantar Pressure Test Strip
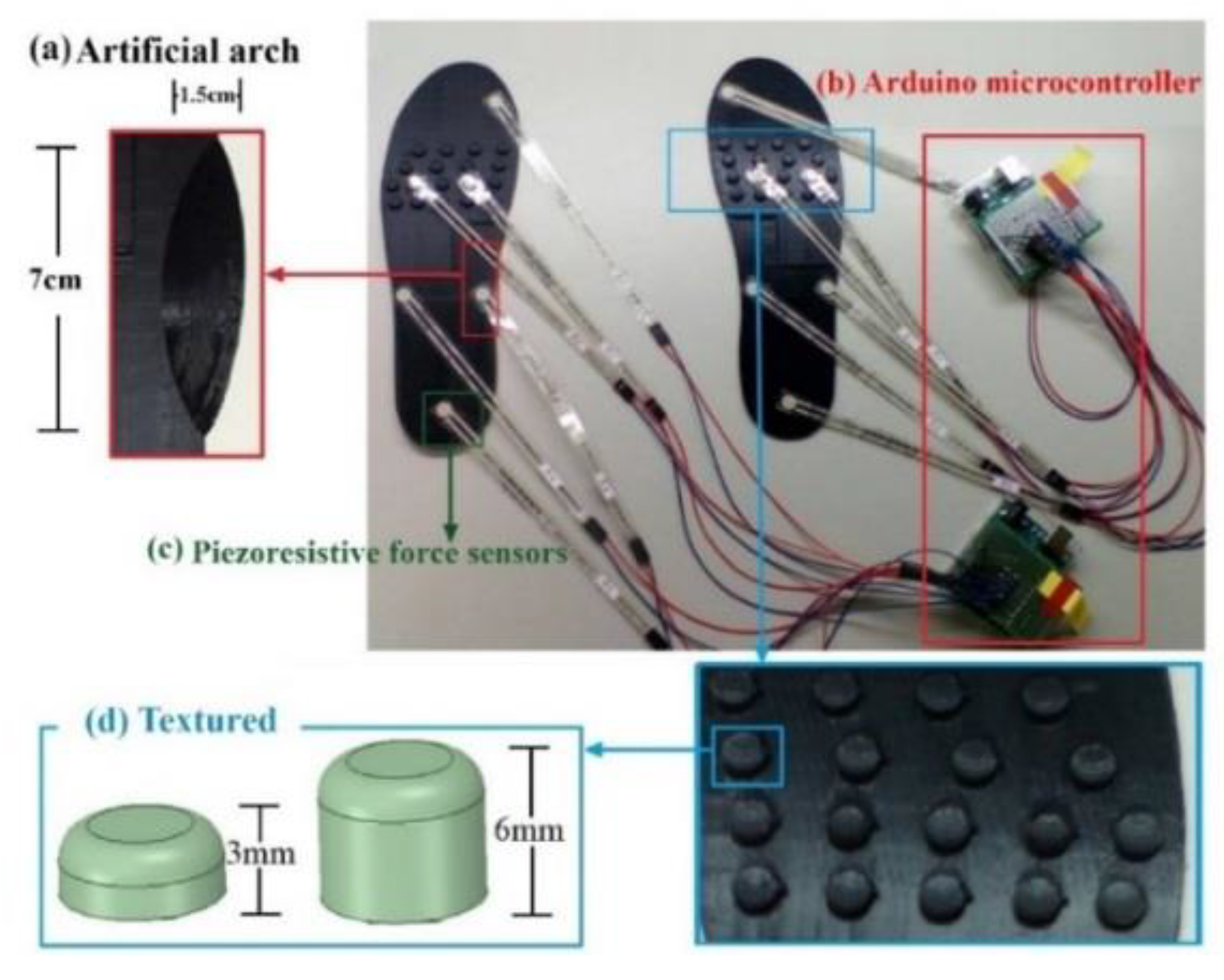
2.2.3. Homemade Foot Pressure Sensing Insoles
2.3. Methods
3. Results
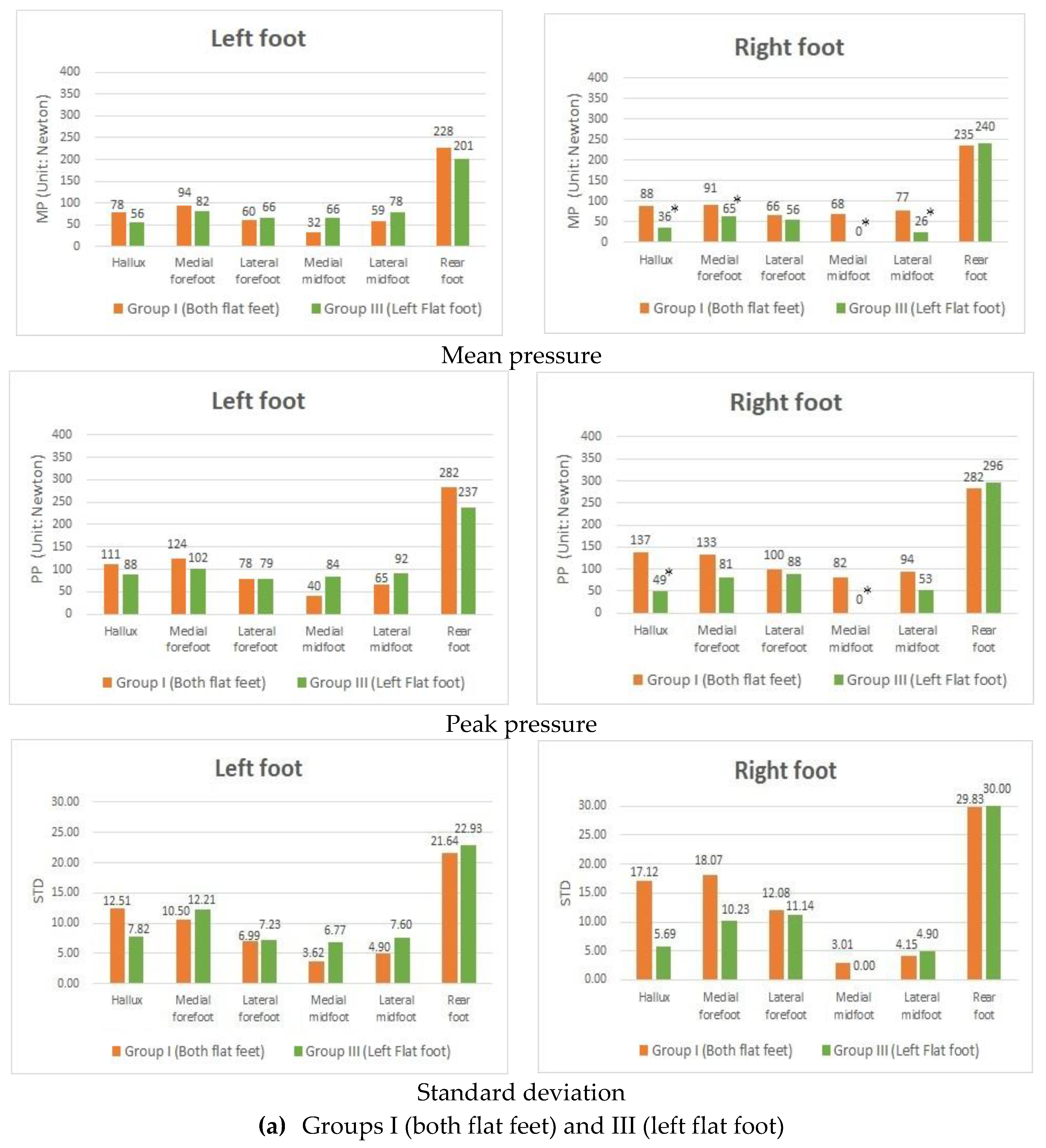
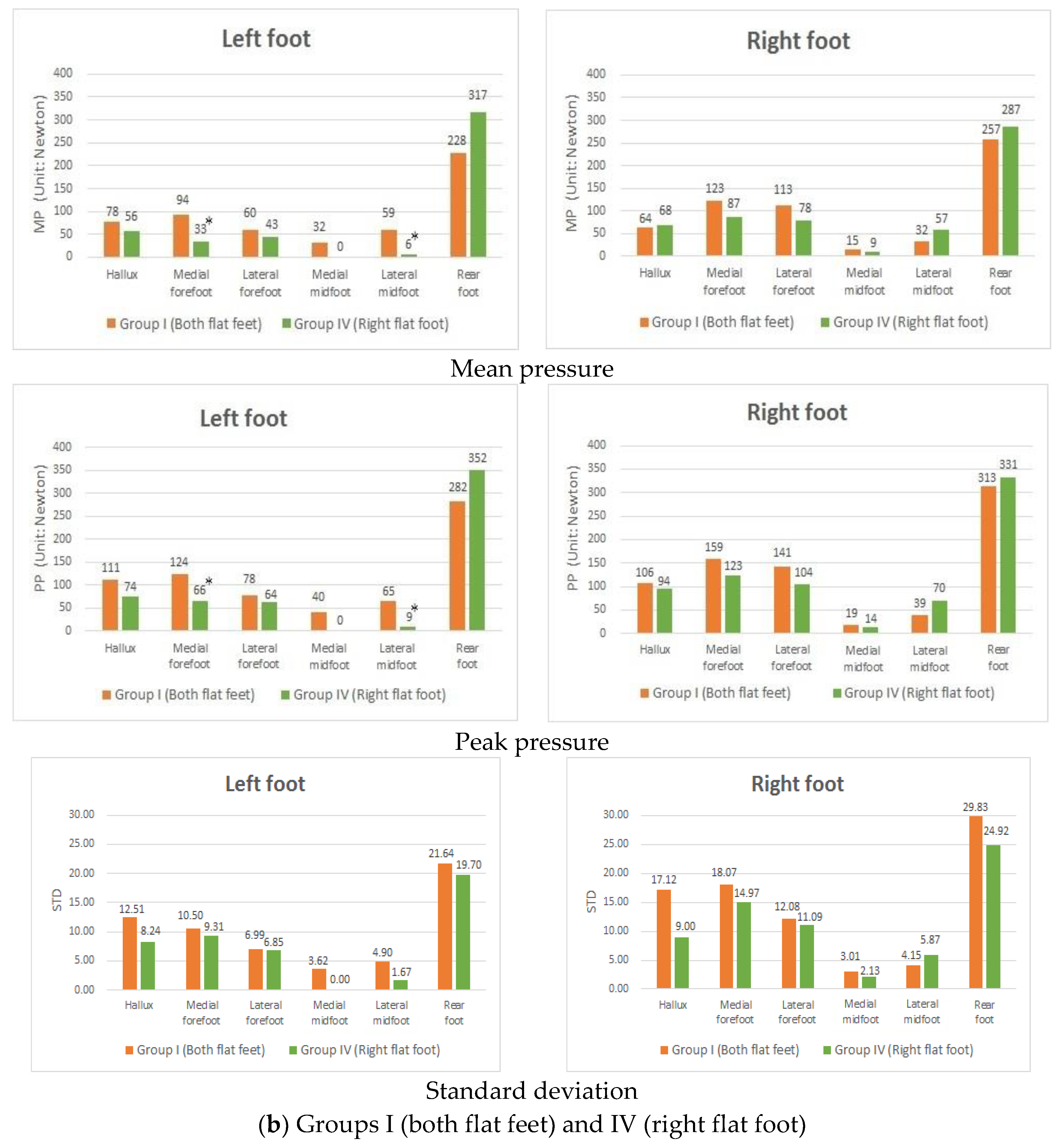
3.1. Difference in Plantar Pressure between Subjects with Fallen Arches in Both Feet and Those Only with One Flat Foot
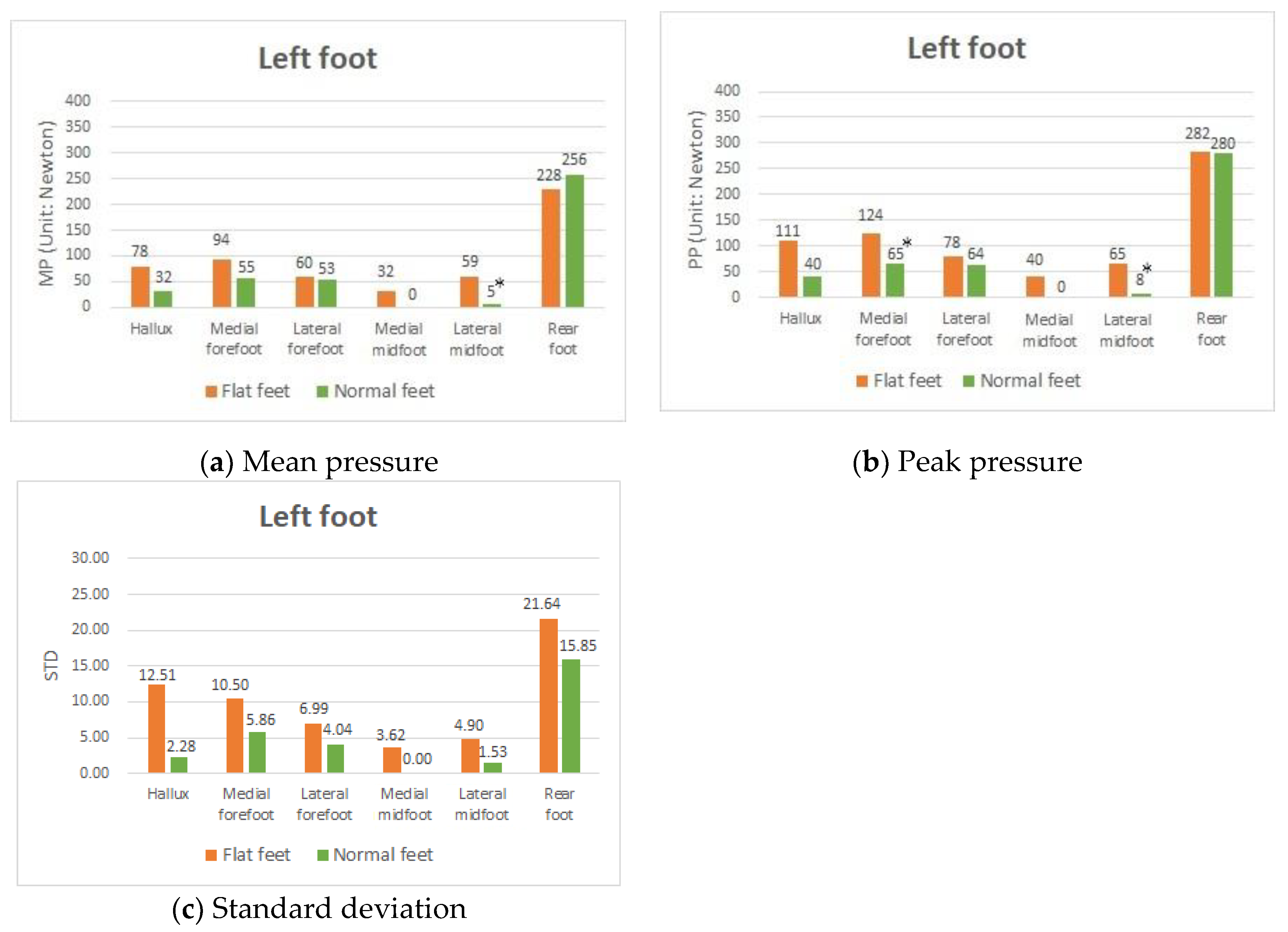
3.2. Difference in Plantar Pressure between Participants with Both Flat Feet and with Both Normal Feet
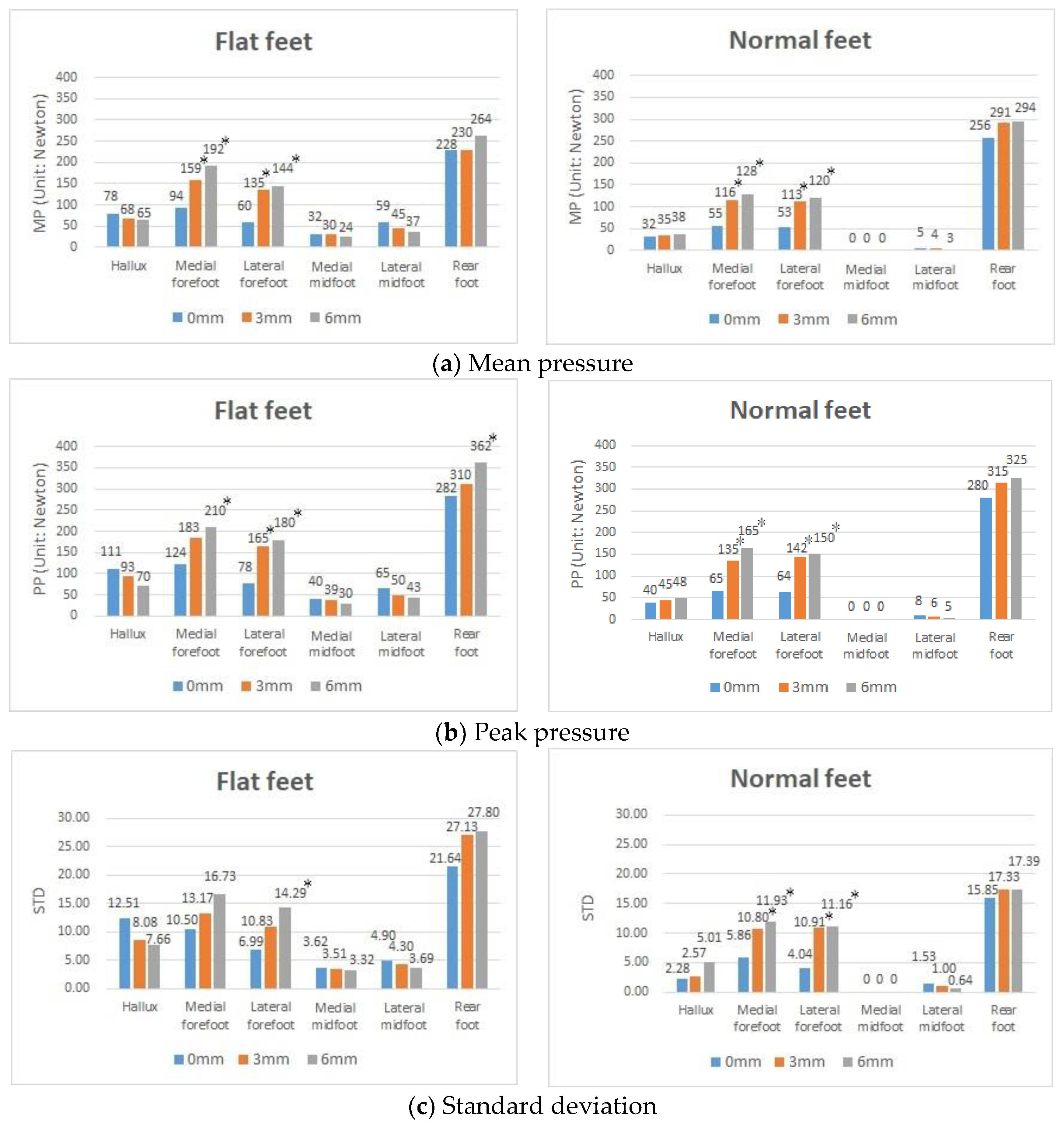
3.3. Effects of Using the Textured Insoles with Different Heights on Plantar Pressure in Both Flat Feet and Both Normal Feet
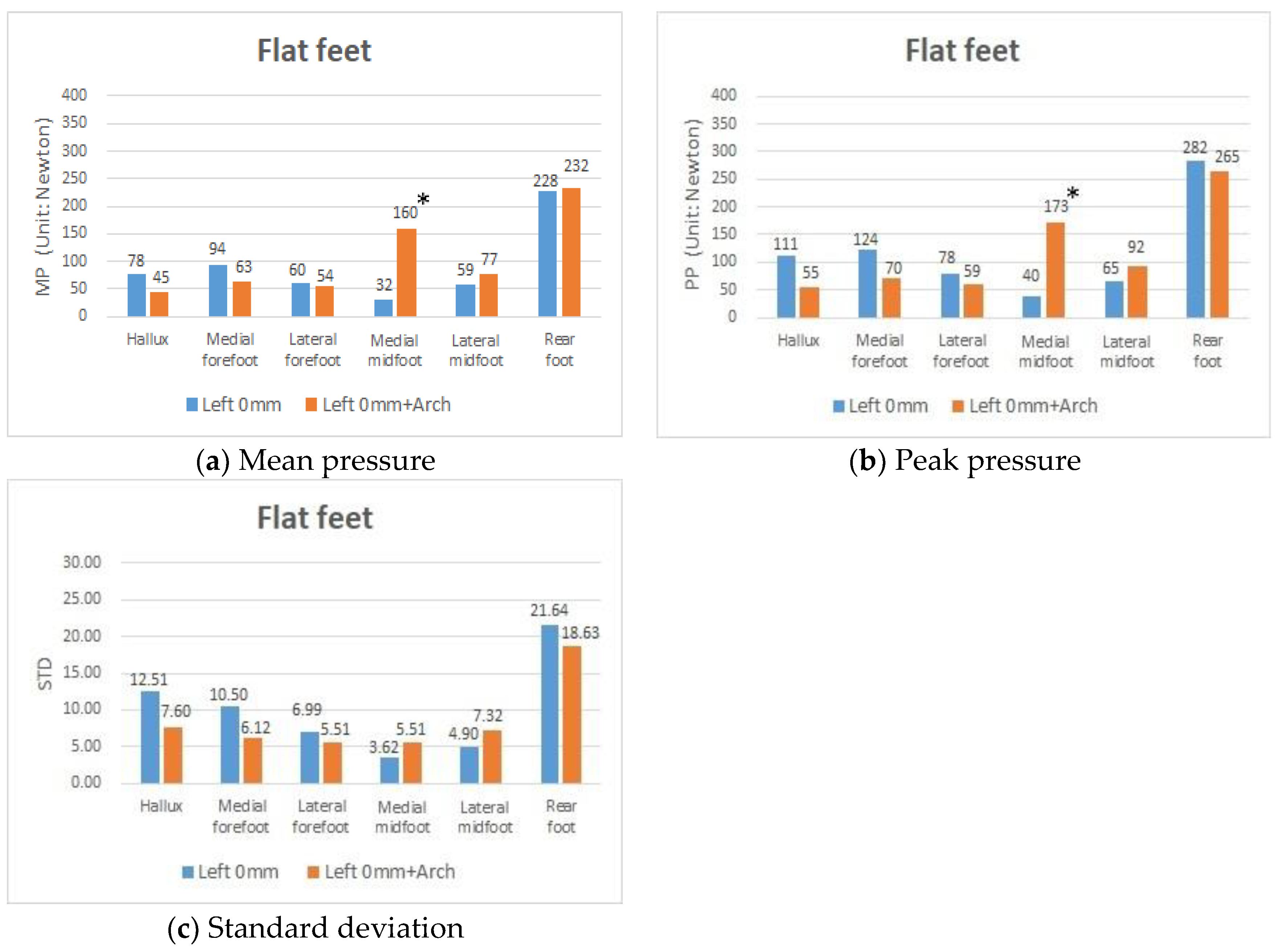
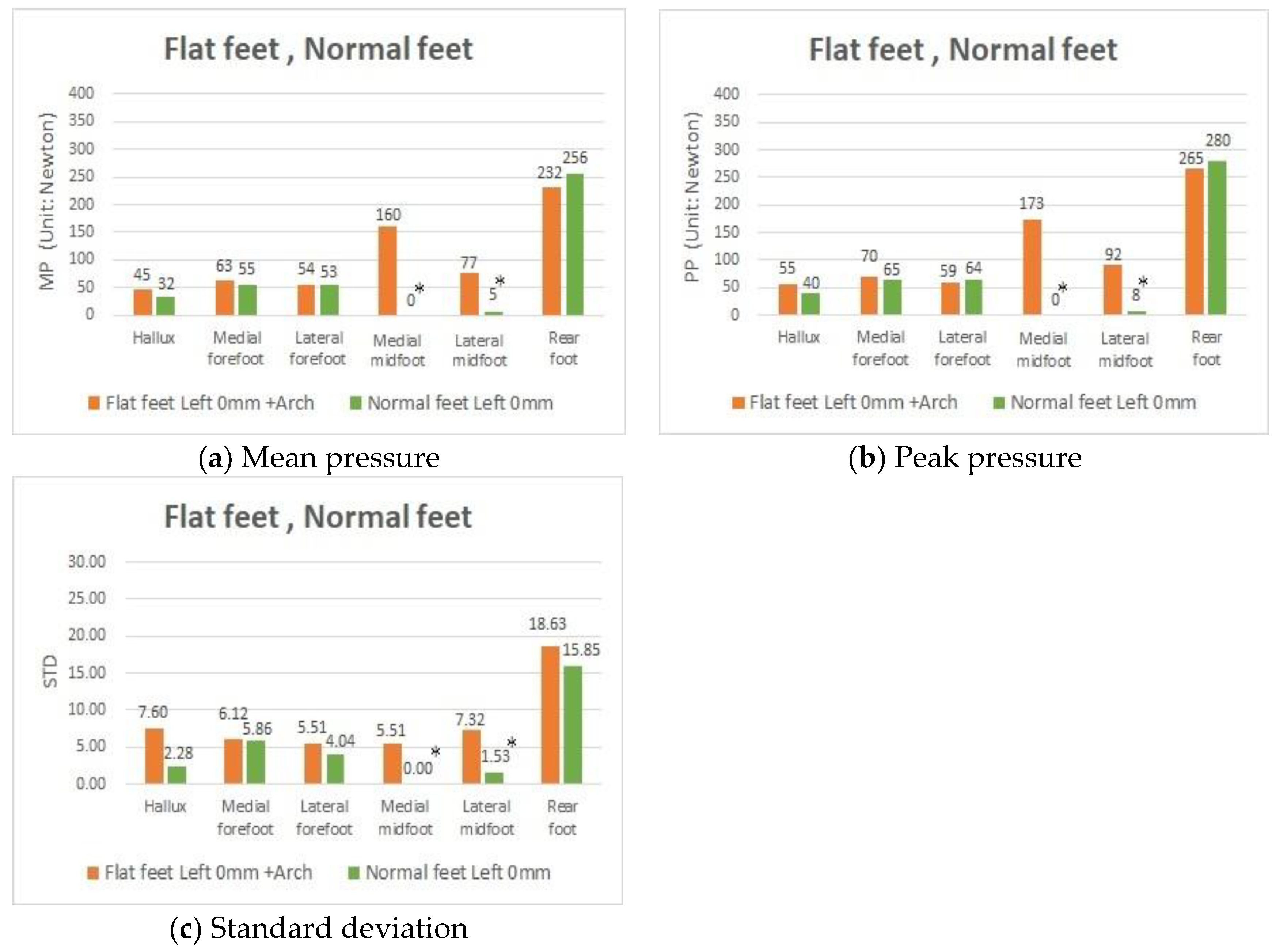
3.4. Effects of Using the Foot Arched Insoles on Plantar Pressure in People with Both Flat Feet
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AI | arch index |
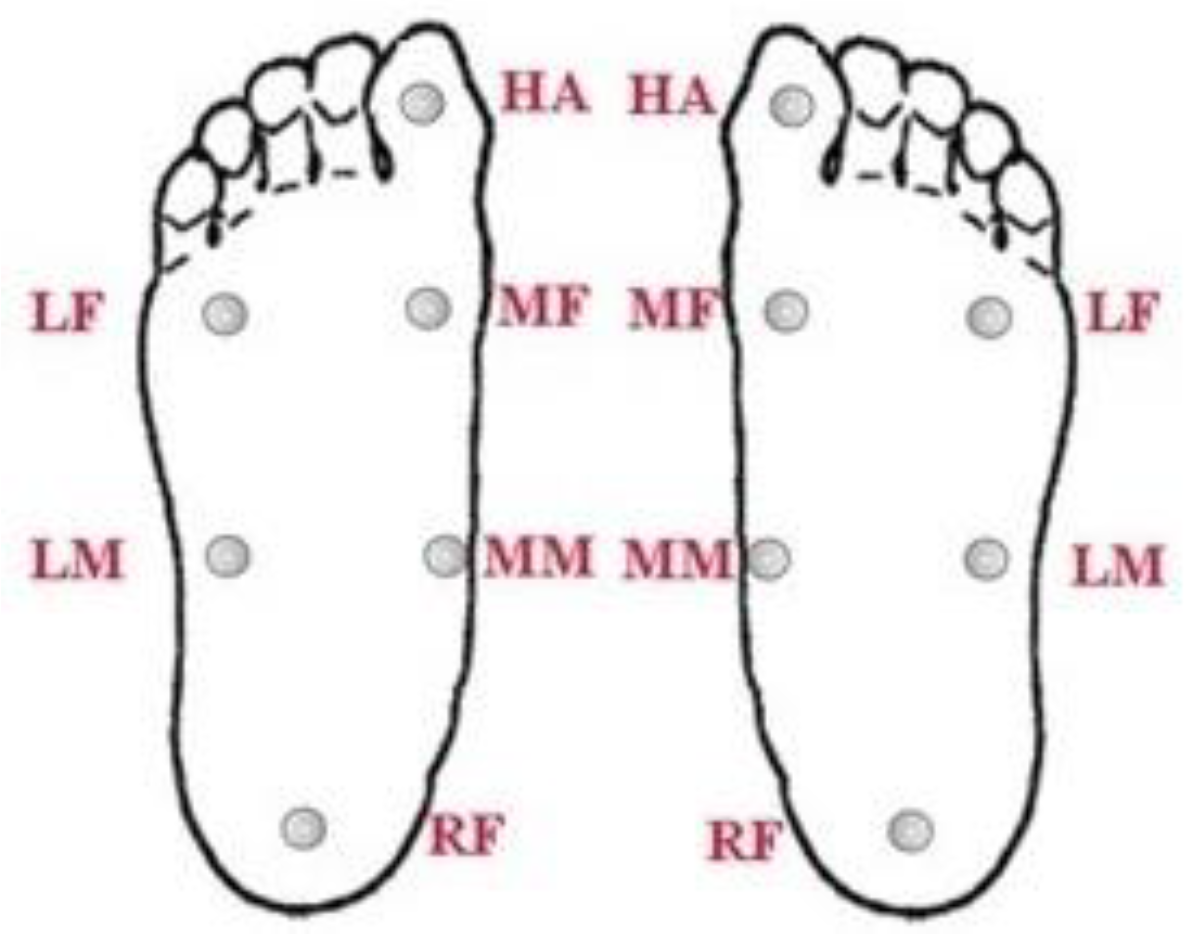
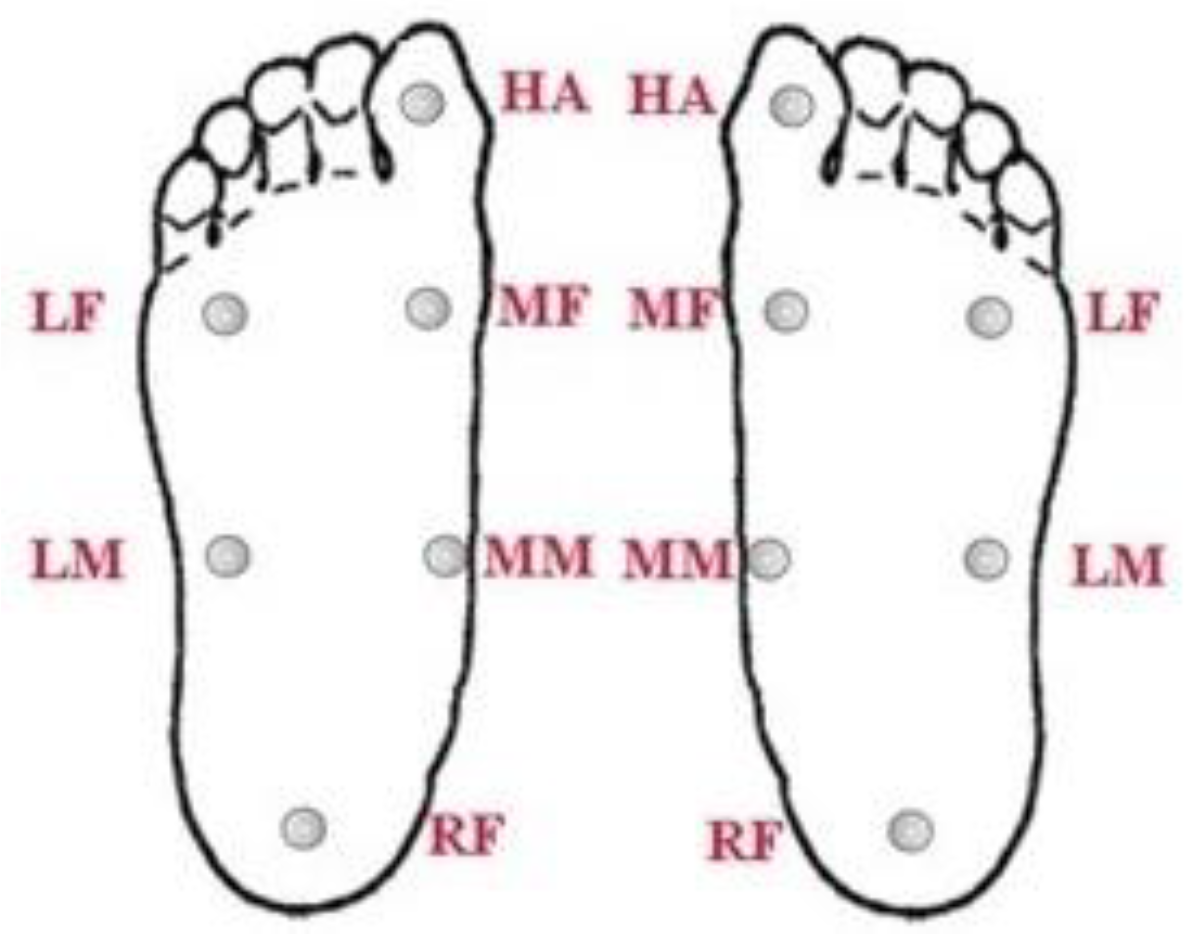
| HA | hallux |
| LF | lateral forefoot |
| LM | lateral midfoot |
| MF | medial forefoot |
| MM | medial midfoot |
| MP | mean pressure |
| PP | peak pressure |
| RF | rearfoot |
| STD | standard deviation |
References
- Rome, K.; Mch, S.D. A study of the Properties of Materials Used in Podiatry. J. Am. Podiatr. Med. Assoc. 1991, 81, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Kaye, R.A.; Jahss, M.H. Tibialis posterior: A review of anatomy and biomechanics in relation to support of the medial longitudinal arch. Foot Ankle Int. 1991, 11, 244–247. [Google Scholar] [CrossRef]
- Jin, T.H.; Hyun, M.K.; Jae, M.J.; Yeun, J.K.; Jung, H.L. Differences in Plantar Foot Pressure and COP between Flat and Normal Feet During Walking. J. Phys. Ther. Sci. 2011, 23, 683–685. [Google Scholar]
- Deland, J.T. The adult acquired flatfoot and spring ligament complex: Pathology and implications for treatment. Foot Ankle Clin. 2001, 6, 129–135. [Google Scholar] [CrossRef]
- Khodadadeh, S.; Welton, E.A. Gait studies of patients with flat feet. Foot 1993, 3, 189–193. [Google Scholar] [CrossRef]
- Memeo, A.; Verdoni, F.; Rossi, L.; Ferrari, E.; Panuccio, E.; Pedretti, L. Flexible Juvenile Flat Foot Surgical Correction: A Comparison between Two Techniques after Ten Years’ Experience. J. Foot Ankle Surg. 2019, 58, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Bertani, A.; Cappello, A.; Benedetti, M.G.; Simoncini, L.; Catani, F. Flat foot functional evaluation using pattern recognition of ground reaction data. Clin. Biomech. 1999, 14, 484–493. [Google Scholar] [CrossRef]
- Macwilliams, B.A.; Cowley, M.; Nicholson, D.E. Foot kinematics and kinetics during adolescent gait. Gait Posture 2003, 17, 214–224. [Google Scholar] [CrossRef]
- Keijsers, N.L.W.; Stolwijk, N.M.; Louwerens, J.W.K.; Duysens, J. Classification of forefoot pain based on plantar pressure measurements. Clin. Biomech. 2013, 28, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Orlin, M.N.; Mcpoil, T.G. Plantar pressure assessment. Phys. Ther. 2000, 80, 399–409. [Google Scholar] [CrossRef] [Green Version]
- Kavros, S.J.; Van Straaten, M.G.; Coleman Wood, K.A.; Kaufman, K.R. Forefoot plantar pressure reduction of off-the-shelf rocker bottom provisional footwear. Clin. Biomech. 2011, 26, 778–782. [Google Scholar] [CrossRef]
- Roy, K.J. Force, pressure and motion measurements in the foot: Current concepts [Review]. Clin. Podiatr. Med. Surg. 1988, 5, 491–508. [Google Scholar] [PubMed]
- Birtane, M.; Tuna, H. The evaluation of plantar pressure distribution in obese and non-obese adults. Clin. Biomech. 2004, 19, 1055–1059. [Google Scholar] [CrossRef] [PubMed]
- Sneyers, C.J.; Lysens, R.; Feys, H.; Andries, R. Influence of malaligment of foot on the plantar pressure pattern in running. Foot Ankle Int. 1995, 16, 624–632. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Su, F.C.; Huang, C.Y. Effects of the shoes and insoles on gait patterns in the flatfoot. J. Biomech. 2007, 40, S472. [Google Scholar] [CrossRef]
- Chen, H.; Nigg, B.M.; Hulliger, M.; Koning, J.D. Influence of sensory input on plantar pressure distribution. Clin. Biomech. 1995, 10, 271–274. [Google Scholar] [CrossRef]
- Kelleher, K.J.; Spence, W.D.; Solomonidis, S.; Apatsidis, D. The effect of textured insoles on gait patterns of people with multiple sclerosis. Gait Posture 2010, 32, 67–71. [Google Scholar] [CrossRef]
- Nurse, M.A.; Hulliger, M.; Wakeling, J.M.; Nigg, B.M.; Stefanyshyn, D.J. Changing the texture of footwear can alter gait patterns. J. Electromyogr. Kinesiol. 2005, 15, 496–506. [Google Scholar] [CrossRef]
- Hatton, A.L.; Dixon, J.; Rome, K.; Newton, J.L.; Martin, D.J. Altering gait by way of stimulation of the plantar surface of the foot: The immediate effect of wearing textured insoles in older fallers. J. Foot Ankle Res. 2012, 5, 5–11. [Google Scholar] [CrossRef] [Green Version]
- Charlie, C.M.; Lee, Y.J.; Chen, B.; Alexander, S.A. Immediate and short-term effects of wearing a single textured insole on symmetry of stance and gait in healthy adults. Gait Posture 2016, 49, 190–195. [Google Scholar]
- Milner, S. Common disorders of the foot and ankle. Surgery (Oxford) 2010, 28, 514–517. [Google Scholar] [CrossRef]
- Chen, Y.C.; Lou, S.Z.; Huang, C.Y.; Su, F.C. Effects of foot orthoses on gait patterns of flat feet patients. Clin. Biomech. 2010, 25, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, K.; Kakihana, W.; Nakagawa, T.; Mitomi, H.; Hikita, A.; Suzuki, R.; Akai, M.; Iwaya, T.; Nakamura, K.; Fukui, N. Addition of an arch support improves the biomechanical effect of a laterally wedged insole. Gait Posture 2009, 29, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Cavanagh, P.R.; Rodgers, M.M. The arch index: A useful measure from footprints. J. Biomech. 1987, 20, 547–551. [Google Scholar] [CrossRef]
- Zuil-Escobar, J.C.; Martínez-Cepa, C.B.; Martín-Urrialde, J.A.; Gómez-Conesa, A. Reliability and Accuracy of Static Parameters Obtained from Ink and Pressure Platform Footprints. J. Manip. Physiol. Ther. 2016, 39, 510–517. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subjects | Classification | AI of the Left Foot | AI of the Right Foot | |
|---|---|---|---|---|
| Group I | A | Both Flat Feet | 0.353 | 0.293 |
| B | 0.291 | 0.308 | ||
| C | 0.354 | 0.261 | ||
| D | 0.374 | 0.267 | ||
| E | 0.261 | 0.275 | ||
| F | 0.356 | 0.336 | ||
| G | 0.276 | 0.306 | ||
| H | 0.293 | 0.266 | ||
| I | 0.265 | 0.263 | ||
| Group II | J | Both Normal Feet | 0.229 | 0.228 |
| K | 0.259 | 0.251 | ||
| L | 0.254 | 0.254 | ||
| M | 0.250 | 0.256 | ||
| N | 0.244 | 0.238 | ||
| O | 0.242 | 0.255 | ||
| P | 0.216 | 0.259 | ||
| Q | 0.238 | 0.236 | ||
| R | 0.257 | 0.259 |
| Subjects | Classification | AI of the Left Foot | AI of the Right Foot | |
|---|---|---|---|---|
| Group III | S | Left Flat Foot | 0.353 | 0.256 |
| T | 0.303 | 0.247 | ||
| U | 0.293 | 0.251 | ||
| Group IV | V | Right Flat Foot | 0.235 | 0.263 |
| W | 0.249 | 0.300 | ||
| X | 0.241 | 0.289 | ||
| Y | 0.217 | 0.267 | ||
| Z | 0.239 | 0.265 |
| Research Findings | Author | Data Collection | Literature Review |
|---|---|---|---|
| The results showed that, when compared with people with normal feet, those with flat feet had a comparatively higher MP, PP, and STD in the HA and forefoot (MF and LF). The MP of people with flat feet was comparatively lower than that of people with normal feet in the RF. | Jin, T. H.; Hyun, M.K.; Jae, M. J.; Yeun, J.K.; Jung, H.L. (2011) [3] | Matscan system | In the heel region, the peak plantar pressure of the flat feet group was lower than in the normal feet group and the difference was statistically significant (p < 0.05). In the big toe area and the small toe area, peak plantar pressure of the flat feet group was higher than in the normal feet group, but without significant difference. |
| The results showed the MP and PP in the areas of the HA (hallux) and midfoot (MM and LM) decreased when the heights of the textured insoles were on the increase. | Chen, H.; Nigg, B. M.; Hulliger, M.; Koning, J. D. (1995) [16] | Flexible pressure measuring insole | The pressure increased in the midfoot area and decreased in the toe area with increasing sensory inputs. |
| The results showed the use of an artificial arch effectively improved the excessive peak in pressure, poor body stability, and alleviate the problem of plantar collapse for patients with flat feet, especially in the inner part of their hallux and forefoot. | Chen, Y. C.; Lou, S.Z.; Huang, C.Y.; Su, F.C. (2010) [22] | Kistler force plates | The results suggested that the foot insoles and shoes developed in this study might benefit the ankle joint in patients with flat feet. |
| The results showed the use of an artificial arch effectively improved the excessive peak in pressure, poor body stability, and alleviate the problem of plantar collapse for patients with flat feet, especially in the inner part of their hallux and forefoot. | Nakajima, K.; Kakihana, W.; Nakagawa, T.; Mitomi, H.; Hikita, A.; Suzuki, R.; Akai, M.; Iwaya, T.; Nakamura, K.; Fukui N. (2009) [23] | Kistler force plates | Addition of an arch support to the laterally wedged insole reduced knee adduction moment more efficiently, possibly through the elimination of potential negative effects of the laterally wedged insole. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.-T.; Chen, J.-C.; Lin, Y.-S. Effects of Artificial Texture Insoles and Foot Arches on Improving Arch Collapse in Flat Feet. Sensors 2020, 20, 3667. https://doi.org/10.3390/s20133667
Wang Y-T, Chen J-C, Lin Y-S. Effects of Artificial Texture Insoles and Foot Arches on Improving Arch Collapse in Flat Feet. Sensors. 2020; 20(13):3667. https://doi.org/10.3390/s20133667
Chicago/Turabian StyleWang, Yao-Te, Jong-Chen Chen, and Ying-Sheng Lin. 2020. "Effects of Artificial Texture Insoles and Foot Arches on Improving Arch Collapse in Flat Feet" Sensors 20, no. 13: 3667. https://doi.org/10.3390/s20133667
APA StyleWang, Y.-T., Chen, J.-C., & Lin, Y.-S. (2020). Effects of Artificial Texture Insoles and Foot Arches on Improving Arch Collapse in Flat Feet. Sensors, 20(13), 3667. https://doi.org/10.3390/s20133667