
Deep-Learning-Based Smartphone Application for Self-Diagnosis of Scleral Jaundice in Patients with Hepatobiliary and Pancreatic Diseases

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
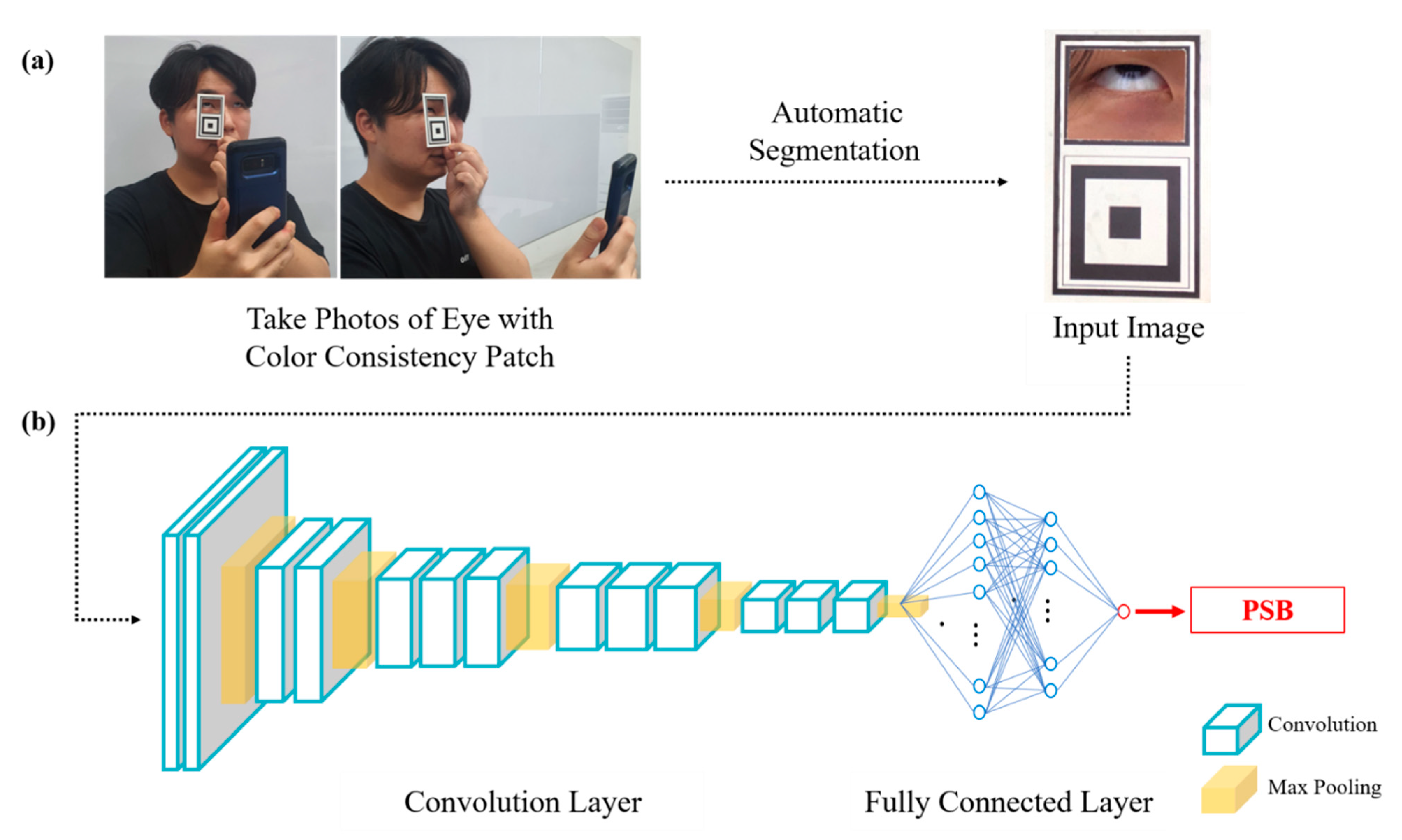
2.2. Data Collection
2.3. Architecture of Deep-Learning System (Figure 1b)
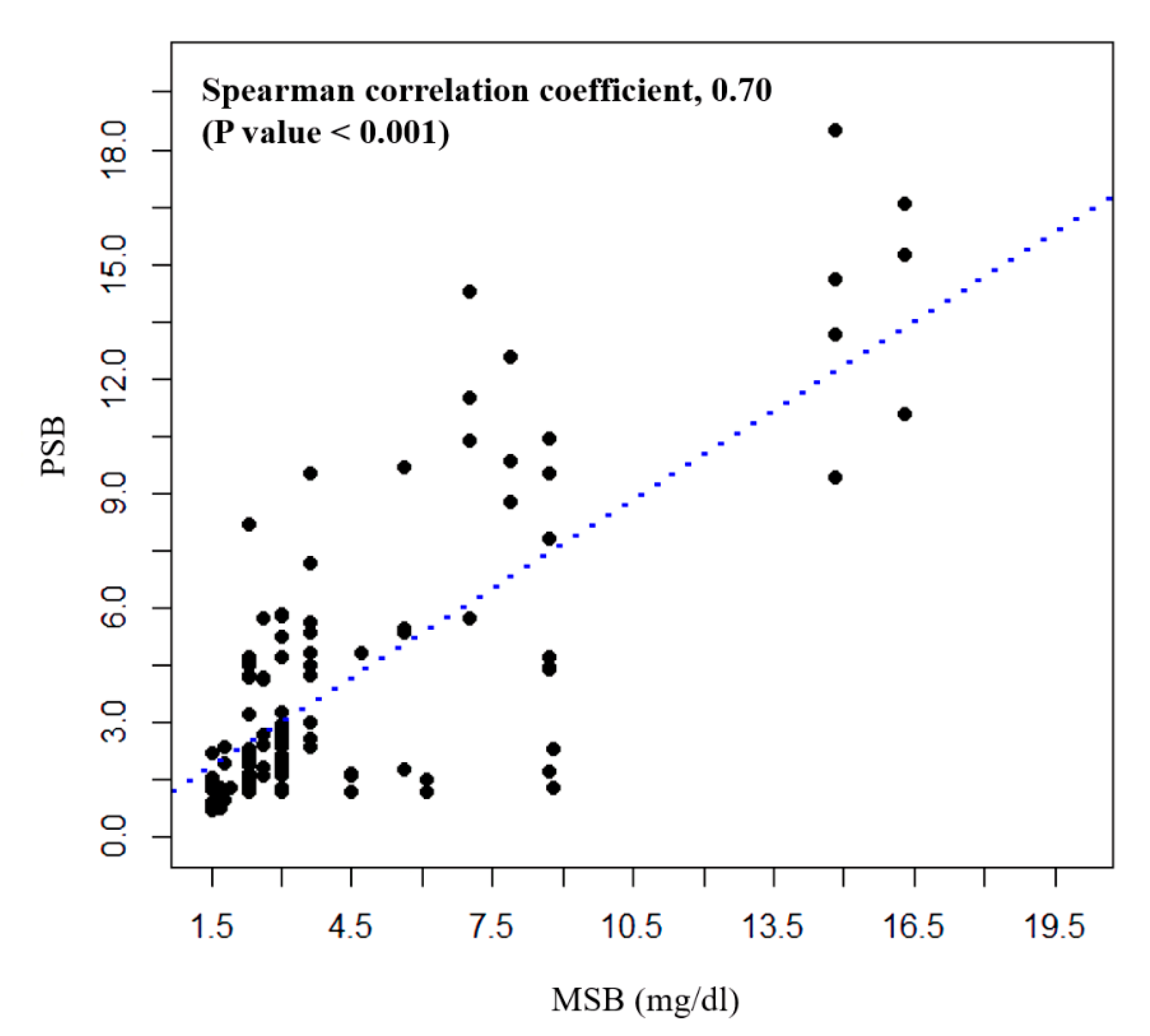
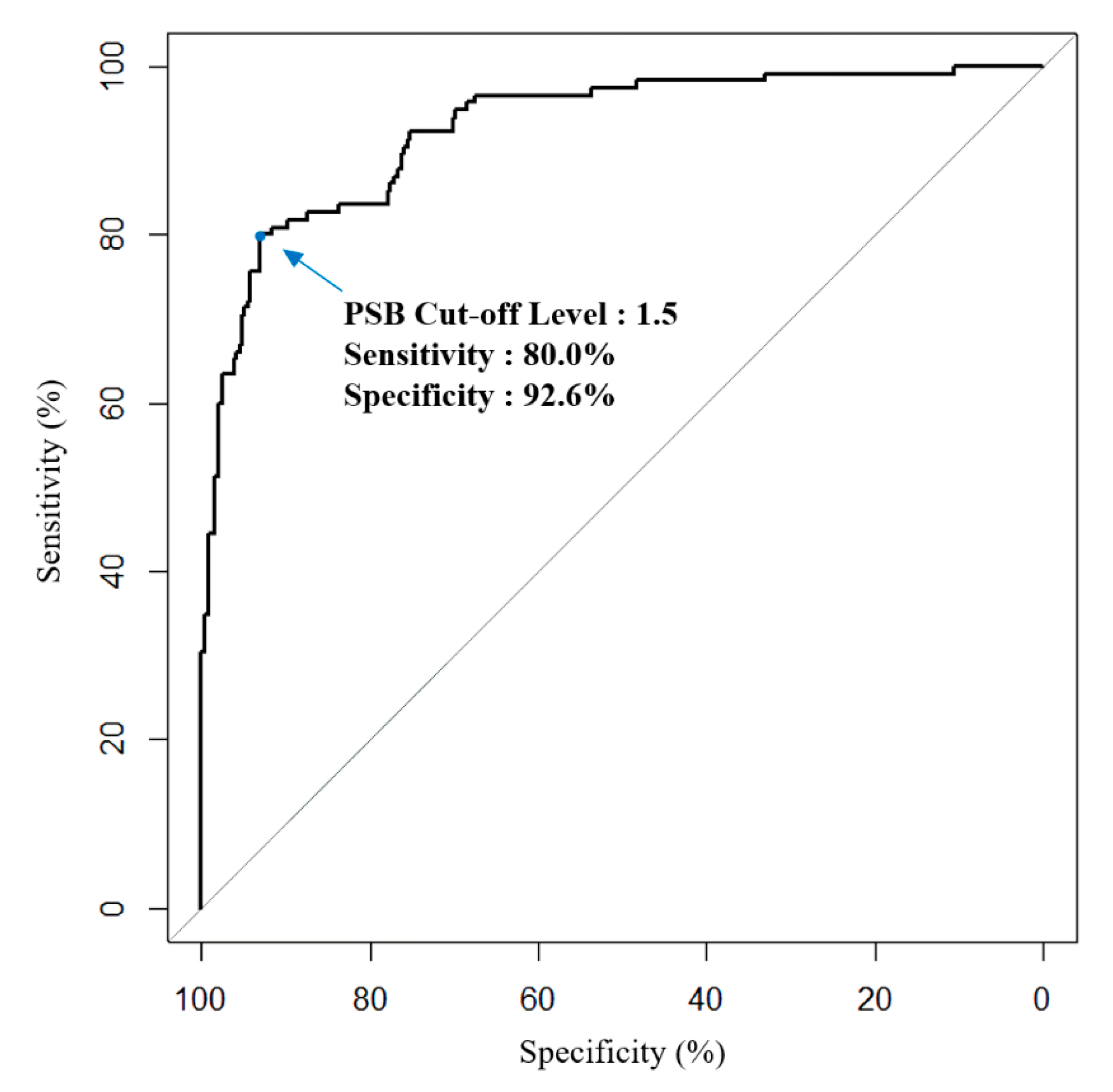
2.4. Outcome Measurements and Statistical Analyses
3. Results
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Hall, J.E.; Hall, M.E. Guyton and Hall Textbook of Medical Physiology E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Fujiwara, R.; Haag, M.; Schaeffeler, E.; Nies, A.T.; Zanger, U.M.; Schwab, M. Systemic Regulation of Bilirubin Homeostasis: Potential Benefits of Hyperbilirubinemia. Hepatology 2018, 67, 1609–1619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fargo, M.V.; Grogan, S.P.; Saguil, A. Evaluation of Jaundice in Adults. Am. Fam. Physician 2017, 95, 164–168. [Google Scholar] [PubMed]
- Roche, S.P.; Kobos, R. Jaundice in the Adult Patient. Am. Fam. Physician 2004, 69, 299–304. [Google Scholar] [PubMed]
- Shieh, Y.Y.; Tsai, F.Y.; Anavim, A.; Wang, M.D.; Lin, C.-M.C. Mobile Healthcare: Opportunities and Challenges. In Proceedings of the International Conference on the Management of Mobile Business (ICMB 2007), Toronto, ON, Canada, 9–11 July 2007; p. 50. [Google Scholar]
- Wac, K.; Bults, R.; Van Beijnum, B.; Widya, I.; Jones, V.; Konstantas, D.; Vollenbroek-Hutten, M.; Hermens, H. Mobile Patient Monitoring: The MobiHealth System. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 1238–1241. [Google Scholar]
- Esteva, A.; Robicquet, A.; Ramsundar, B.; Kuleshov, V.; DePristo, M.; Chou, K.; Cui, C.; Corrado, G.; Thrun, S.; Dean, J. A Guide to Deep Learning in Healthcare. Nat. Med. 2019, 25, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Alagappan, M.; Brown, J.R.G.; Mori, Y.; Berzin, T.M. Artificial Intelligence in Gastrointestinal Endoscopy: The Future Is Almost Here. World J. Gastrointest. Endosc. 2018, 10, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Byrne, M.F.; Chapados, N.; Soudan, F.; Oertel, C.; Pérez, M.L.; Kelly, R.; Iqbal, N.; Chandelier, F.; Rex, D.K. Real-time differentiation of adenomatous and hyperplastic diminutive colorectal polyps during analysis of unaltered videos of standard colonoscopy using a deep learning model. Gut 2019, 68, 94–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice; Prentice Hall: Pearson Upper Saddle River, NJ, USA, 2009; Volume 892. [Google Scholar]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef] [PubMed]
- De Greef, L.; Goel, M.; Seo, M.J.; Larson, E.C.; Stout, J.W.; Taylor, J.A.; Patel, S.N. Bilicam: Using Mobile Phones to Monitor Newborn Jaundice. In Proceedings of the 2014 A.C.M. International Joint Conference on Pervasive and Ubiquitous Computing, Seattle, WA, USA, 13–17 September 2014; pp. 331–342. [Google Scholar]
- Mariakakis, A.; Banks, M.A.; Phillipi, L.; Yu, L.; Taylor, J.; Patel, S.N. Biliscreen: Smartphone-Based Scleral Jaundice Monitoring for Liver and Pancreatic Disorders. In Proceedings of the ACM on Interactive, Mobile, Wearable and Ubiquitous Technologies; Association for Computing Machinery: New York, NY, USA, 2017; Volume 1, pp. 1–26. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | Training Set | Validation Set | p-Value |
|---|---|---|---|---|
| No. of patients | 130 | 90 | 40 | |
| No. of hospital visits | 298 | 211 | 87 | |
| Average visit per patient | 2.3 | 2.3 | 2.1 | 0.67 |
| No. of total photos | 1460 | 1034 | 426 | |
| Photos/cases | 4.9 | 4.9 | 4.9 | 0.95 |
| Age | 70.0 ± 4.8 | 68.9 ± 15.4 | 72.6 ± 13.1 | 0.05 |
| Male (%) | 173 (58.1) | 120 (56.9) | 53 (60.2) | 0.51 |
| Underlying disease | 0.17 | |||
| Hepatobiliary | 92 (70.8) | 67 (74.4) | 25 (62.5) | |
| Pancreatic disease | 38 (29.2) | 23 (25.6) | 15 (37.5) | |
| Total bilirubin | 0.8 (0.4–1.8) | 0.9 (0.5–1.9) | 0.7 (0.4–1.6) | 0.88 |
| AST | 31.0 (19.0–70.0) | 31.0 (19.0–70.0) | 31.5 (21.3–67.8) | 0.49 |
| ALT | 19.0 (9.0–50.0) | 20.0 (9.0–54.0) | 18.5 (9.0–41.5) | 0.21 |
| PSB Level | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|
| 1.3 mg/dL | 82.6% | 83.6% | 65.1% | 92.9% |
| 1.5 mg/dL | 80.0% | 92.6% | 80.0% | 92.6% |
| 2.0 mg/dL | 63.4% | 97.1% | 89.0% | 87.8% |
| 2.5 mg/dL | 52.2% | 98.1% | 90.9% | 84.7% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.H.; Yang, M.J.; Kim, J.S.; Park, B.; Kim, J.H.; Sunwoo, M.H. Deep-Learning-Based Smartphone Application for Self-Diagnosis of Scleral Jaundice in Patients with Hepatobiliary and Pancreatic Diseases. J. Pers. Med. 2021, 11, 928. https://doi.org/10.3390/jpm11090928
Park JH, Yang MJ, Kim JS, Park B, Kim JH, Sunwoo MH. Deep-Learning-Based Smartphone Application for Self-Diagnosis of Scleral Jaundice in Patients with Hepatobiliary and Pancreatic Diseases. Journal of Personalized Medicine. 2021; 11(9):928. https://doi.org/10.3390/jpm11090928
Chicago/Turabian StylePark, Joon Hyeon, Min Jae Yang, Ji Su Kim, Bumhee Park, Jin Hong Kim, and Myung Hoon Sunwoo. 2021. "Deep-Learning-Based Smartphone Application for Self-Diagnosis of Scleral Jaundice in Patients with Hepatobiliary and Pancreatic Diseases" Journal of Personalized Medicine 11, no. 9: 928. https://doi.org/10.3390/jpm11090928
APA StylePark, J. H., Yang, M. J., Kim, J. S., Park, B., Kim, J. H., & Sunwoo, M. H. (2021). Deep-Learning-Based Smartphone Application for Self-Diagnosis of Scleral Jaundice in Patients with Hepatobiliary and Pancreatic Diseases. Journal of Personalized Medicine, 11(9), 928. https://doi.org/10.3390/jpm11090928