
Self-Reported Digital Literacy of the Pharmacy Workforce in North East Scotland

Abstract
:1. Introduction
2. Experimental Section
2.1. Design
2.2. Setting
2.3. Sampling of Community and Hospital Pharmacies
- urban, remote and rural geographical settings;
- technology infrastructures;
- pharmacy management systems implemented; and
- hospital pharmacy (community, major) and community pharmacy (small independent through to small, medium or large chain multiples; in the NHS Grampian area there are 23 small independents (single pharmacy), 67 small (1–4 pharmacies) to medium (5–25 pharmacies) chain multiples, and 41 national chain multiples) [26].
2.4. Recruitment of Pharmacy Owners and Managers
2.5. Recruitment of Pharmacists, Pharmacy Technicians, Dispensing Assistants and Medicines Counter Assistants
2.6. Data Collection

{kind=link}
{kind=link}
{kind=link}
| Course title | Description | |
|---|---|---|
| ← Increasing level of difficulty | Computing for the Terrified | If you are new to computing then this is the course for you. This short course gives you the opportunity to explore the basics of using a computer in a friendly and relaxed environment. Overcome your fears of using a computer and learn a new subject. |
| Computing for the Quietly Confident | To provide students with a firm understanding of Microsoft Office applications. Learners should finish the course with a good grasp of word processing. | |
| Computing for the Courageous | Learners should finish the course with a more advanced grasp of word processing, basic spreadsheets, basic databases and basic presentations. | |
| European Computer Driving Licence (ECDL) | Attaining a European Computer Driving Licence is the best way to ensure you have all the necessary computing qualifications of any workplace. This course covers the first steps of using a computer—IT fundamentals, the internet, email and security. | |
| ECDL Advanced | Enables the learner to work more effectively with IT. This unit looks at using advanced tools to save time and effort when producing word processed documents, presentations and spread sheets. | |
| Computing Degree or Diploma | Course content includes: Computer Architecture, Computer Operating Systems 1; Computing: Planning; Computing: Graded Unit; Information Technology: Applications Software 1, Working within a Project Team. | |
2.7. Data Analysis
| Case | Setting | chain multiple Type | Rural/Urban | P | PT | DA | MCA | No. of Rx per month | High tech/ Low tech | Pharmacy Management system |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | community | large, independent, chain multiple | R | 1 | 1 | 0 | 4 | 8000 | L | Cegidem |
| 2 | community | small, independent, chain multiple | U | 1 | 0 | 1 | 3 | 5000 | L | ProScript |
| 3 | community | small, independent, chain multiple | U | 1 | 1 | 0 | 2 | 7000 | L | ProScript |
| 4 | community | small, independent, chain multiple | R | 1 | 1 | 0 | 1 | 4000 | L | ProScript |
| 5 | community | small, independent, chain multiple | R | 1 | 1 | 0 | 2 | 4500 | L | Cegidem |
| 6 | community | small, independent, chain multiple | R | 1 | 0 | 1 | 2 | 6500 | L | Cegidem |
| 7 | community | small, independent, chain multiple | R | 1 | 0 | 1 | 1 | 3000 | L | Cegidem |
| 8 | community | small, independent, chain multiple | R | 1 | 0 | 0 | 1 | 850 | L | Cegidem |
| 9 | community | small, independent, chain multiple | R | 0 | 0 | 0 | 1 | 1350 items | L | Cegidem |
| 10 | community | large, chain multiple | U | 1 | 0 | 0 | 1 | 11,000 | L | Nexphase |
| 11 | community | small, independent, chain multiple | U | 3 | 2 | 1 | 2 | Info withheld | H | Positive Solutions |
| 12 | community | small, independent, chain multiple | U | 1 | 1 | 0 | 1 | 2500 items | L | ProScript |
| 13 | community | large, independent, chain multiple | R | 1 | 1 | 0 | 2 | 3500 | L | Cegidem |
| 14 | community | large, chain multiple | R | 1 | 1 | 1 | 3 | 11,000 | L | ProScript |
| 15 | community | small, independent, chain multiple | U | 1 | 1 | 0 | 4 | Info withheld | H | Positive Solutions |
| 16 | community | small, independent, chain multiple | U | 3 | 0 | 2 | 2 | 8000 | L | Cegidem |
| 17 | community | small, independent, chain multiple | U | 2 | 2 | 2 | 2 | Info withheld | H | Positive Solutions |
| 18 | hospital | medium | U | 4 | 3 | 1 | 0 | not available | L | JAC |
| 19 | hospital | large | U | 1 | 4 | 5 | 0 | > 800 items per day | H | JAC |
3. Results and Discussion
3.1. Types of Pharmacy and Settings
3.2. Hardware and Software Implemented
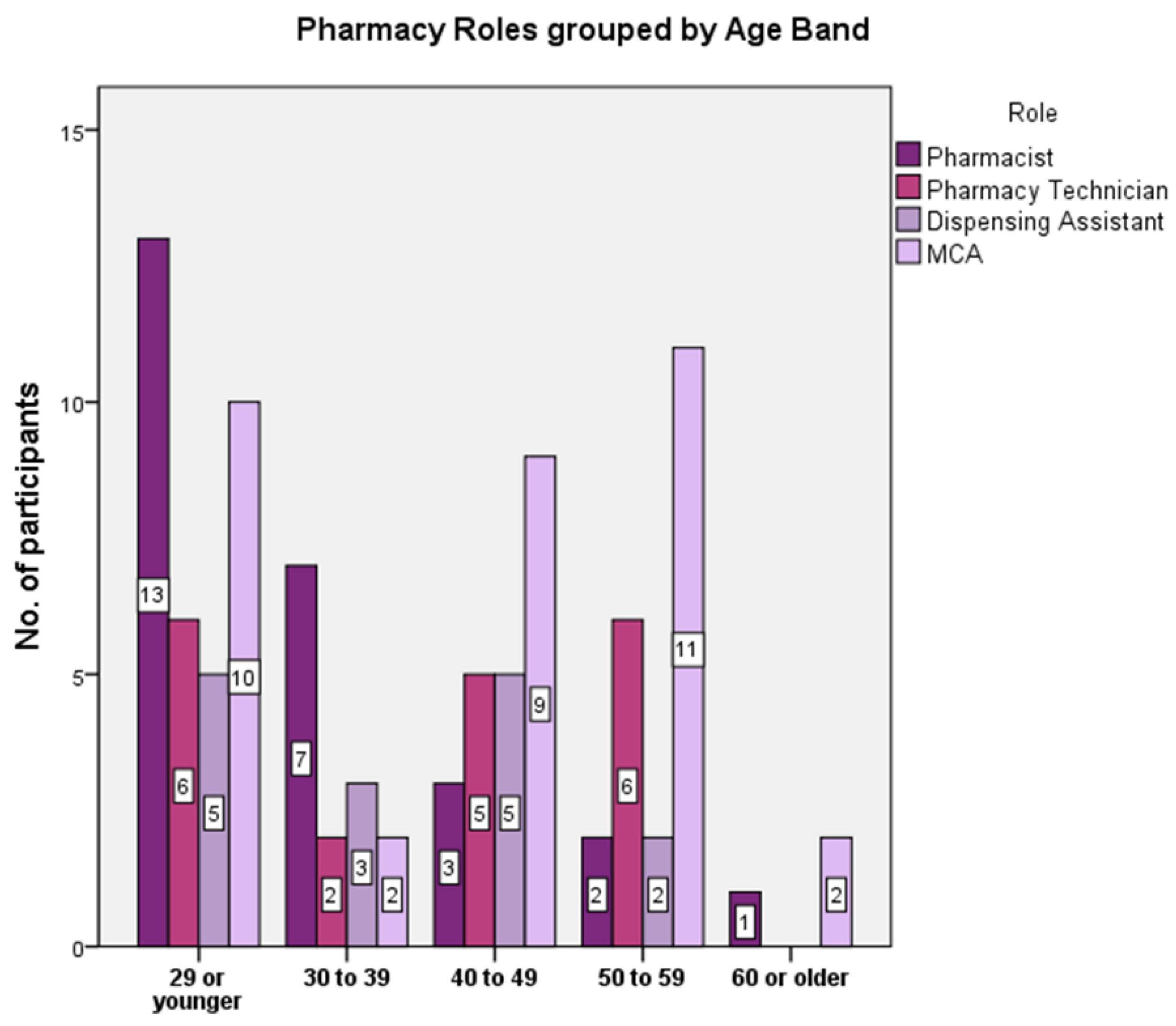
3.3. Participant Demographics
- 24 pharmacists, two of whom were locums;
- 2 pre-registration pharmacy graduates;
- 19 pharmacy technicians;
- 15 dispensing assistants; and
- 34 medicines counter assistants.



3.4. Key Findings
3.5. Strengths and Weaknesses
3.6. Interpretation in Context with Existing Literature
3.7. Driving Forces for Technology in Pharmacy
3.8. Restraining Forces for Technology in Pharmacy
3.9. Conditions for Change
3.10. Further Work
4. Conclusions
Key Messages
- With few exceptions, pharmacy staff in the NHS Grampian area work with minimum levels of technology and perceive their own digital literacy to be at a basic level.
- Role, age, gender and work experience were not clear determinants of digital literacy.
- Pharmacy staff need to be trained to harness pharmacy technologies effectively and efficiently in support of their role development.
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Darzi, A. High Quality Care for All: NHS Next Stage Review Final Report; Department of Health: London, UK, 2008. Available online: http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_085825 (accessed on 12 June 2009).
- Scottish Government. eHealth Strategy 2011–2017; Scottish Government: Edinburgh, Scotland, 2011. Available online: http://www.gov.scot/resource/doc/357616/0120849.pdf (accessed on 12 April 2012).
- Department of Health. A Report from the NHS Future Forum: Education and Training; Department of Health: London, England, 2011. Available online: https://www.gov.uk/government/uploads/system/.../dh_132025.pdf (accessed on 12 June 2012).
- Crown, J. Review of Prescribing, Supply & Administration of Medicines. Final Report; Department of Health: London, England, 1999. Available online: webarchive.nationalarchives.gov.uk/.../http:/.../dh_4077153.pdf (accessed on 1 June 2010).
- General Pharmaceutical Council. Future Pharmacists: Standards for Initial Education and Training of Pharmacists. 2011. Available online: www.pharmacyregulation.org (accessed on 4 February 2012).
- Beetham, H.; McGill, L.; Littlejohn, A. Thriving in the 21st Century: The Report of the LLiDA Project (Learning Literacies for the Digital Age): Provision in the UK. 2009. Available online: http://www.jisc.ac.uk/media/documents/projects/llidareportjune2009.pdf (accessed on 23 November 2012).
- British Computer Society. Digital Literacy for Life Programme. 2013. Available online: http://dlfl.bcs.org/ (accessed on 11 October 2013).
- American Library Association. Digital Literacy, Libraries, and Public Policy: Report of the Office for Information Technology Policy’s Digital Literacy Task Force. 2013. Available online: http://www.districtdispatch.org/wp-ontent/uploads/2013/01/2012_OITP_digilitreport_1_22_13.pdf (accessed on 1 October 2013).
- Lankshear, C.; Knobel, M. Digital Literacies: Concepts, Policies and Practices; Peter Lang: New York, NY, USA, 2008; Volume 30. [Google Scholar]
- UNESCO. Institute for Technologies in Education Policy Brief: Digital Literacy in Education. 2011. Available online: http://iite.unesco.org/publications/3214688/ (accessed on 19 November 2012).
- European Commission. Digital Agenda for Europe. 2012. Available online: http://ec.europa.eu/information_society/digital-agenda/index_en.htm (accessed on 29 February 2013).
- European Commission. eHealth Action Plan 2012–2020 Public Consultation. 2012. Available online: http://ec.europa.eu/information_society/activities/health/ehealth_ap_consultation/ index_en.htm (accessed on 1 May 2011).
- Innovation & Business Skills Australia. Scoping Study—Identifying Digital Literacy Skills: Cybercitizen and E-Employee in the 21st Century. 2010. Available online: http://www.ibsa.org.au/Portals/ibsa.org.au/docs/Research%20&%20Discussion%20Papers/IBSA%20%20%20Identifying%20Digital%20Literacy%20Skills%2027%2004%2010%20v1.pdf (accessed on 10 October 2013).
- New Zealand Ministry of Education. Digital Information Literacy: Supported Development of Capability in Tertiary Environments. 2010. Available online: http://www.educationcounts.govt.nz/__data/assets/pdf_file/0006/80628/Digital-Information-Literacy-Research-Report-FINAL-pdf.pdf (accessed on 10 October 2013). [Google Scholar]
- Royal Pharmaceutical Society & Royal College of General Practitioners. Joint Statement: Breaking down the Barriers—How Community Pharmacists and GPs can Work together to Improve Patient Care; Royal Pharmaceutical Society & Royal College of General Practitioners (RPS & RCGP): London, England, 2011; Available online: www.rpharms.com/public-affairs-pdfs/RPSRCGPjointstatement.pdf (accessed on 1 October 2012).
- Royal Pharmaceutical Society. Empowering Pharmacists to Improve Pharmaceutical Care and Medicines Safety through Information Technology: Information Technology Strategic Principles; Royal Pharmaceutical Society: Edinburgh, Scotland, 2011; Available online: www.rpharms.com/...pharmacy-pdfs/imt---nov-2012---it-principles.pdf (accessed on 1 October 2012).
- e-Skills UK. National Occupational Standards for IT Users. 2011. Available online: https://www.e-skills.com/standards-and-qualifications/national-occupational-standards-nos/ (accessed on 20 January 2011).
- NHS Education for Scotland. ePharmacy Toolkit for Community Pharmacists. NHS Education for Scotland: Glasgow, Scotland, 2008. Available online: www.gov.scot/resource/doc/209438/0055428.pdf (accessed on 1 April 2010). [Google Scholar]
- General Pharmaceutical Council. Annual Report 2012/13. 2013. Available online: http://www.pharmacyregulation.org/sites/default/files/Annual%20Report%202013.pdf (accessed on 28 February 2013).
- Accreditation Council for Pharmacy Education. Available online: https://www.acpe-accredit.org/default.asp (accessed on 23 June 2012).
- Wilson, H.; Barber, N. Review of NHS Pharmaceutical Care of Patients in the Community in Scotland. 2013. Available online: http://www.scotland.gov.uk/Resource/0043/00430209.pdf (accessed on 15 August 2013). [Google Scholar]
- Scottish Government. Prescription for Excellence: A Vision and Action Plan for the Right Pharmaceutical Care through Integrated Partnerships and Innovation. 2013. Available online: http://www.scotland.gov.uk/Resource/0043/00434053.pdf (accessed on 11 November 2013). [Google Scholar]
- Scottish Government. Everyone Matters: 2020 Workforce Vision. 2013. Available online: http://www.scotland.gov.uk/Publications/2013/06/5943 (accessed on 11 November 2013). [Google Scholar]
- NHS Health Scotland. A Fairer Healthier Scotland: Our Strategy 2012–2017. 2012. Available online: http://www.healthscotland.com/uploads/documents/18922-CorporateStrategy.pdf (accessed on 11 November 2013).
- Scottish Government. Public Bodies (Joint Working) (Scotland) Bill. 2013. Available online: http://www.scottish.parliament.uk/parliamentarybusiness/Bills/63845.aspx (accessed on 14 August 2013). [Google Scholar]
- NHS Grampian. NHS Grampian Annual Review 2012/13. 2013. Available online: http://www.nhsgrampian.co.uk/nhsgrampian/gra_display.jsp;jsessionid=B56539D81BD0E705E5C988111E34A969?pContentID=6997&p_applic=CCC&p_service=Content.show& (accessed on 12 December 2013).
- Centre for Workforce Intelligence. Annual Review April 2010 to March 2011. 2011. Available online: www.cfwi.org.uk (accessed on 1 October 2011).
- Greenhalgh, T.; Robert, G.; MacFarlane, F.; Bate, P.; Kyriakidou, O.; Peacock, R. Storylines of Research in Diffusion of Innovation: A Meta-Narrative Approach to Systematic Review. Soc. Sci. Med. 2005, 61, 417–430. [Google Scholar] [CrossRef] [PubMed]
- Rogers, E.M. Diffusion of Innovations; Free Press: Glencoe, Scotland, 1995. [Google Scholar]
- Lewin, K. Field Theory in Social Science; Harper & Row: New York, NY, USA, 1947. [Google Scholar]
- Scottish Government. Better eHealth: Better Care—Citizen eHealth Survey. 2011. Available online: http://www.ehealth.scot.nhs.uk/?page_id=143 (accessed on 1 November 2011). [Google Scholar]
- Scottish Government. Achieving Sustainable Quality in Scotland’s Healthcare: A '20:20' Vision. 2011. Available online: http://www.knowledge.scot.nhs.uk/media/CLT/ResourceUploads/4002697/Achieving%20Sustainable%20Quality%20in%20Scotlands%20Healthcare%20-%20A%2020_.doc (accessed on 12 October 2015). [Google Scholar]
- Scottish Government. Route Map to the 2020 Vision for Health and Social Care. 2013. Available online: http://www.scotland.gov.uk/Topics/Health/Policy/Quality-Strategy/ routemap2020vision (accessed on 11 July 2013). [Google Scholar]
- Community Pharmacy Scotland. Policy Response from Chief Executive to Introduction of “Prescription for Excellence”. 2013. Available online: http://www.communitypharmacyscotland.org.uk/news,-policy-and-publications/policy/policy-responses-by-cps-%281%29/policy-responses-by-cps/ (accessed on 12 January 2013).
- National Health Service Knowledge and Skills Framework. NHS Knowledge and Skills Framework. 2013. Available online: http://www.ksf.scot.nhs.uk/ (accessed on 4 April 2013).
- British Computer Society. Preparing the NHS for an Information Revolution: BCS Report on the NHS Information Revolution Consultation Proposal; British Computer Society: London, England, 2013; Available online: https://www.bcs.org/upload/pdf/liberating-the-nhs.pdf (accessed on 1 December 2014).
- Adair, J.E. Action-Centred Leadership; McGraw-Hill: London, England, 1973. [Google Scholar]
- Muntyan, K.D.; Benne, B. Human Relations in Curriculum Change. Available online: http://www.channelingreality.com/Niwa/Documents/Social_Engineering/1951_HRCC_Benne_122710.pdf (accessed on 12 October 2015).
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implemen. Sci. 2011, 6, 42. Available online: http://www.implementationscience.com/content/6/1/42 (accessed on 5 July 2012). [Google Scholar] [CrossRef] [PubMed]
- Eason, K.; Waterson, P. The implications of e-health system delivery strategies for integrated healthcare: Lessons from England. Int. J. Med. Inform. 2012, 82, 96–106. Available online: www.ncbi.nlm.nih.gov/pubmed/23266062 (accessed on 5 July 2013). [Google Scholar] [CrossRef] [PubMed]
- Patterson, E.S. Technology support of the handover: Promoting observability, flexibility and efficiency. BMJ Qual. Saf. 2012, 21, i19–i21. Available online: www.ncbi.nlm.nih.gov/pubmed/23173184 (accessed on 12 October 2015). [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MacLure, K.; Stewart, D. Self-Reported Digital Literacy of the Pharmacy Workforce in North East Scotland. Pharmacy 2015, 3, 182-196. https://doi.org/10.3390/pharmacy3040182
MacLure K, Stewart D. Self-Reported Digital Literacy of the Pharmacy Workforce in North East Scotland. Pharmacy. 2015; 3(4):182-196. https://doi.org/10.3390/pharmacy3040182
Chicago/Turabian StyleMacLure, Katie, and Derek Stewart. 2015. "Self-Reported Digital Literacy of the Pharmacy Workforce in North East Scotland" Pharmacy 3, no. 4: 182-196. https://doi.org/10.3390/pharmacy3040182
APA StyleMacLure, K., & Stewart, D. (2015). Self-Reported Digital Literacy of the Pharmacy Workforce in North East Scotland. Pharmacy, 3(4), 182-196. https://doi.org/10.3390/pharmacy3040182