
A New Trans-Tympanic Microphone Approach for Fully Implantable Hearing Devices

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
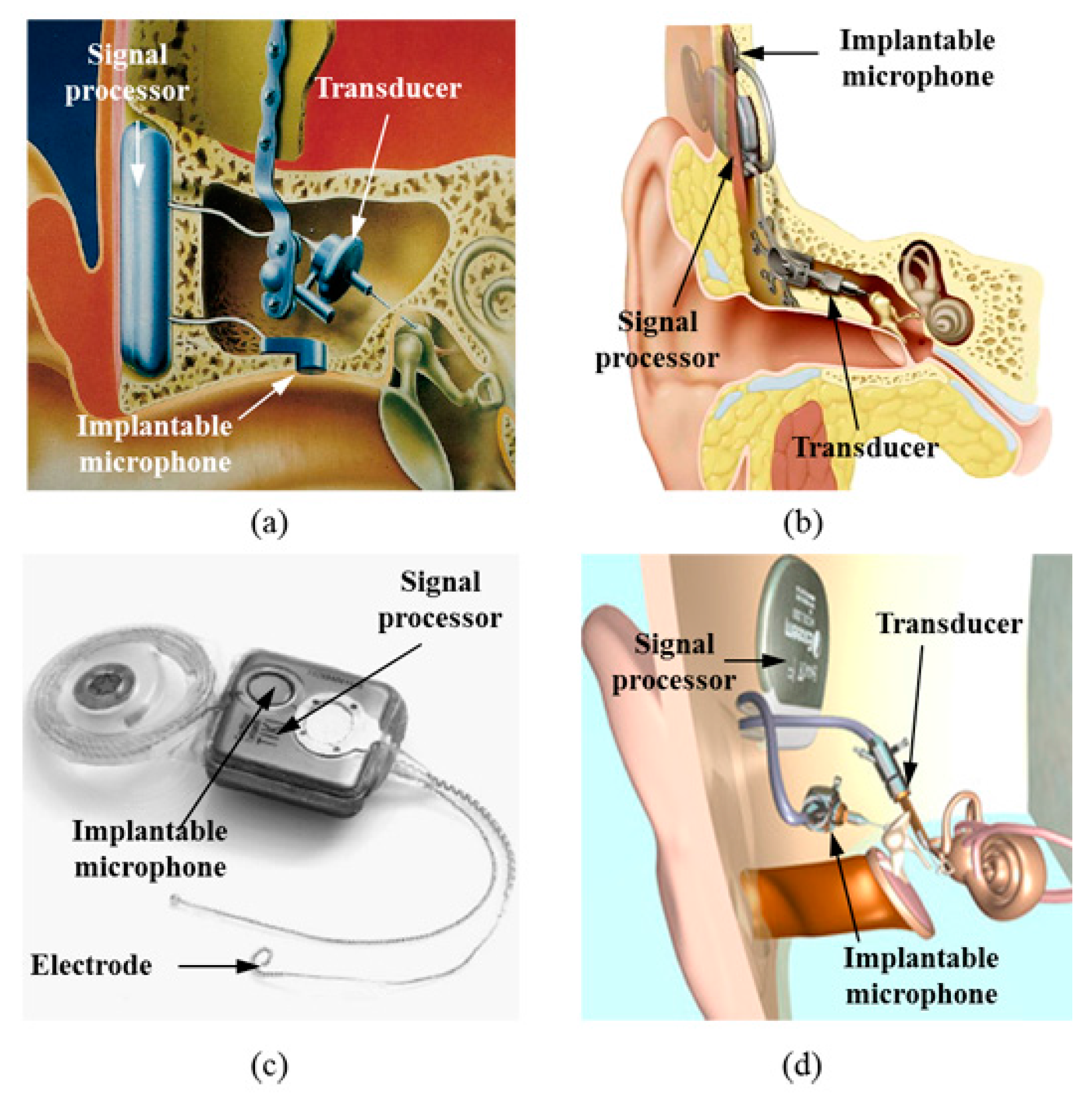
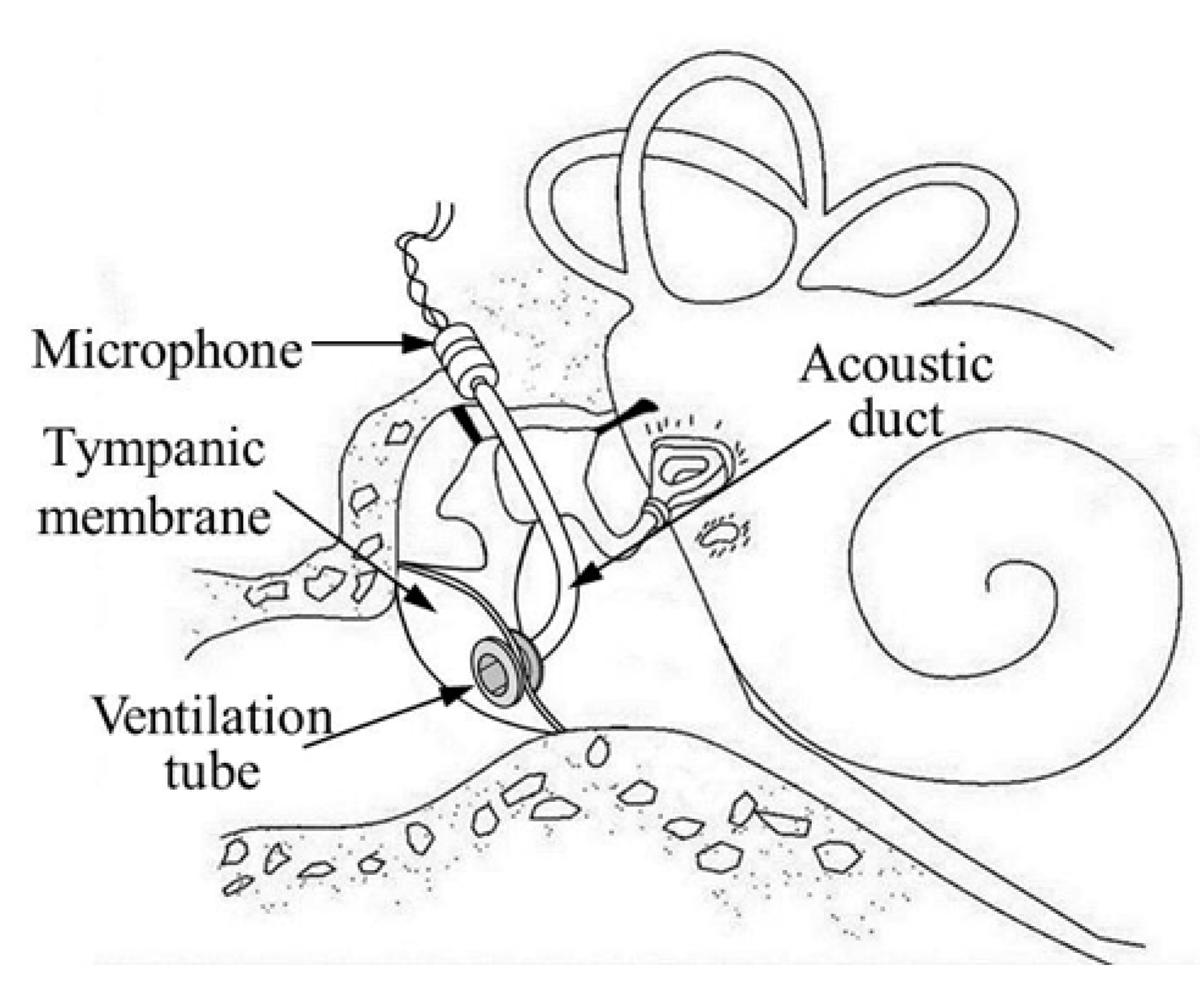
2. Conventional Implantable Microphones and the New Approach


3. Measurement Methods
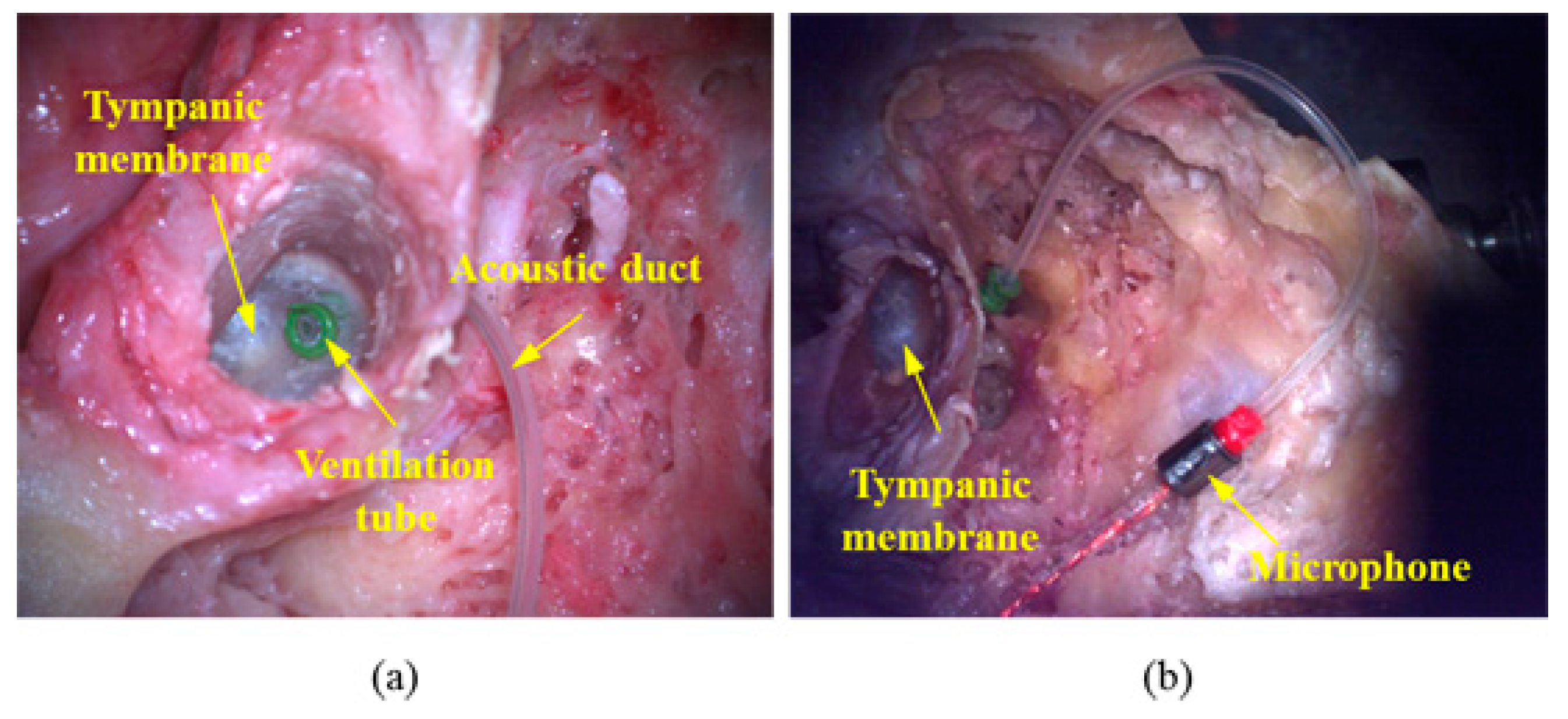
3.1. Temporal-Bone Preparation
3.2. Measurements and Data Acquisition

4. Results
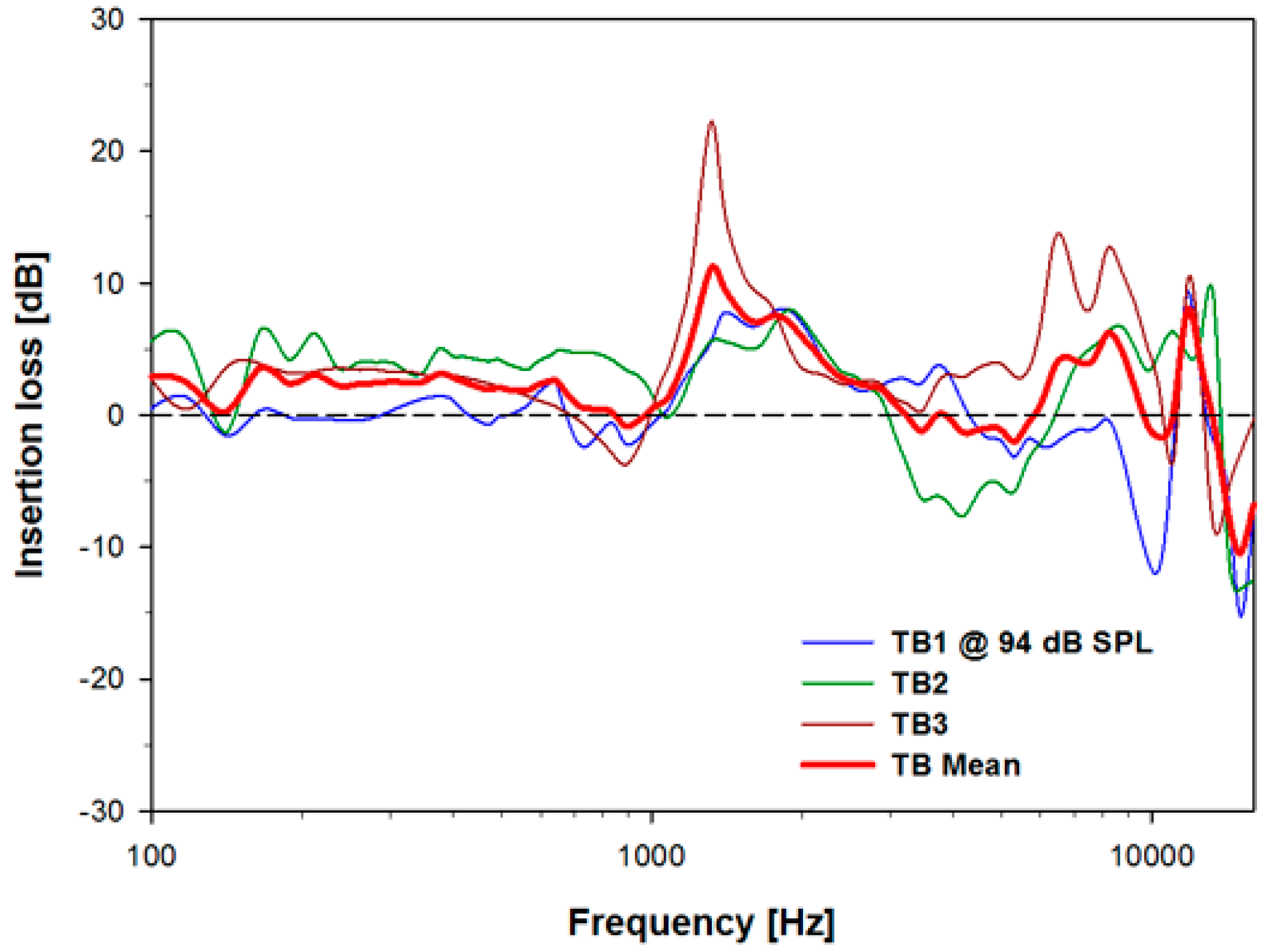
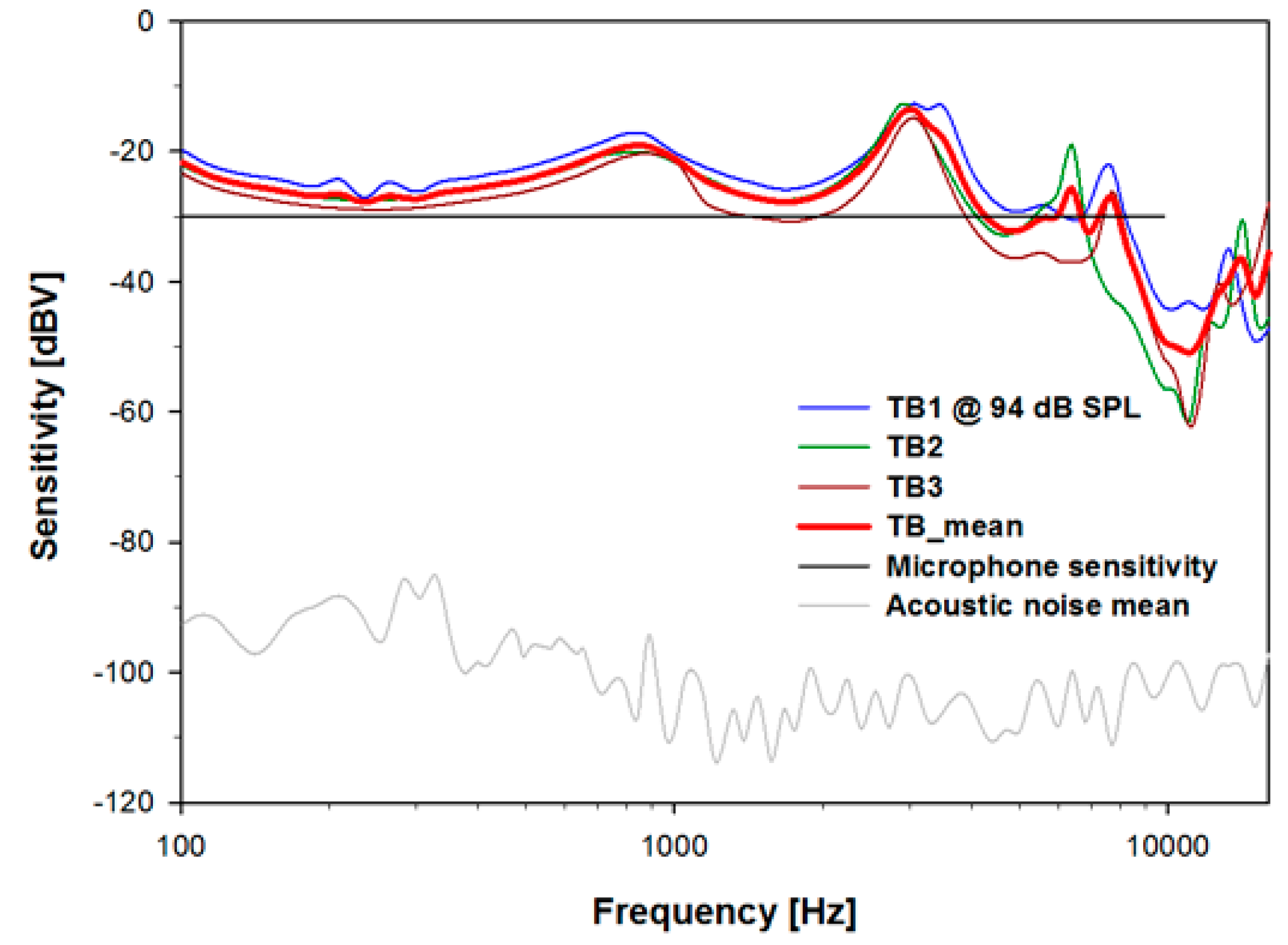
4.1. Results of the Trans-Tympanic Microphone Experiment




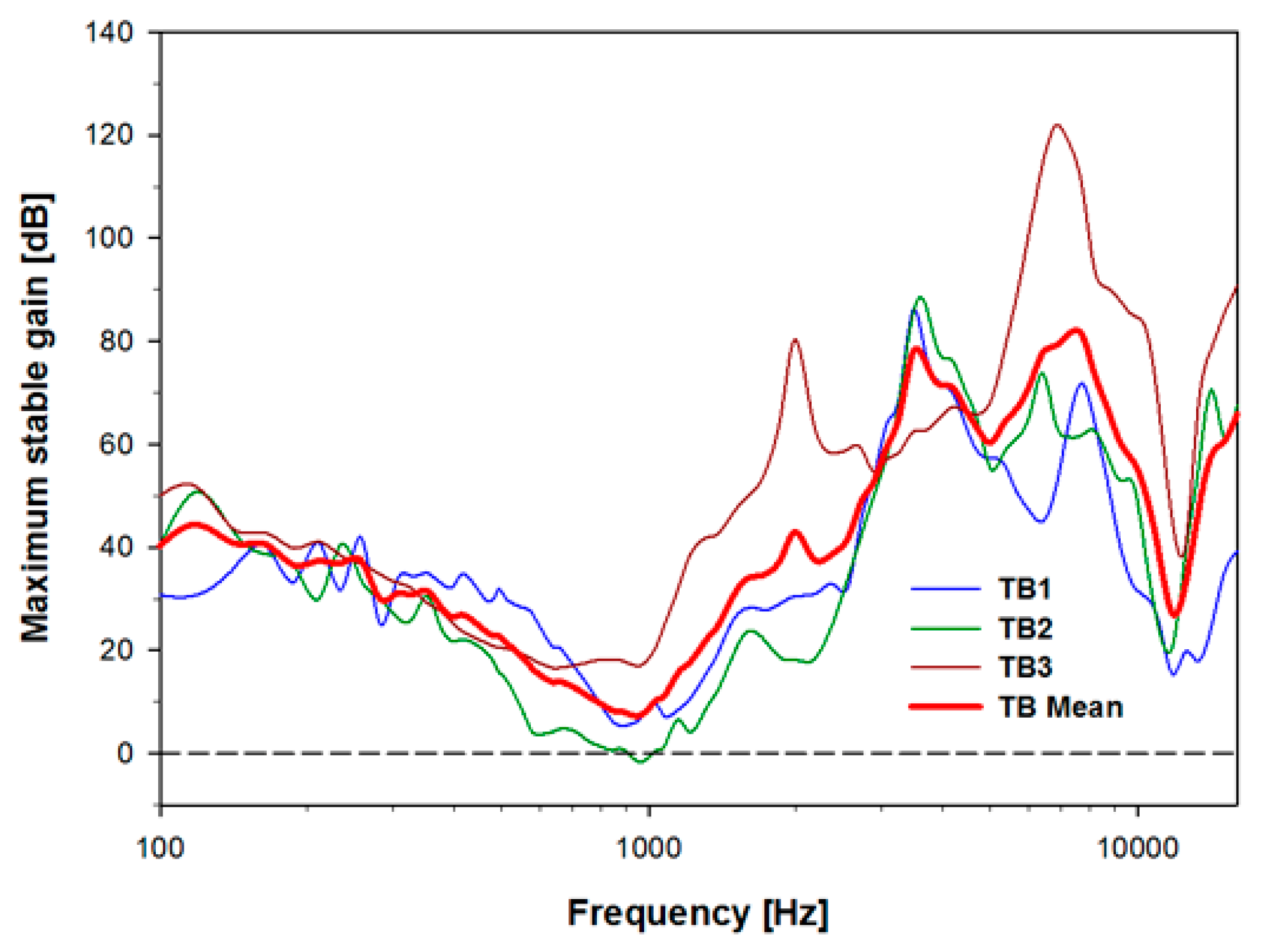
4.2. Acoustic Feedback for the Trans-Tympanic Microphone with Round-Window Drive

5. Discussion and Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Puria, S. Middle-ear hearing devices. In The Middle Ear: Science, Otosurgery, and Technology; Puria, S., Fay, R.R., Popper, A.N., Eds.; Springer New York: New York, NY, USA, 2013. [Google Scholar]
- Mathilde, D.; Evelyne, D.; Stephane, T.; Arnaud, D.; Thierry, M.; Vincent, D.; Eric, T. Evolution of the reliability of the fully implantable middle ear transducer over successive generations. Otol. Neurotol. 2015, 36, 625–630. [Google Scholar]
- Counter, P. Implantable hearing aids. J. Eng. Med. 2008, 222, 837–852. [Google Scholar] [CrossRef]
- Briggs, R.J.S.; Eder, H.C.; Seligman, P.M.; Cowan, R.S.C.; Plant, K.L.; Dalton, J.; Money, D.K.; Patrick, J.F. Initial clinical experience with a totally implantable cochlear implant research device. Otol. Neurotol. 2008, 29, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Haynes, D.S.; Young, J.A.; Wanna, G.B.; Glasscock, M.E., III. Middle ear implantable hearing devices: An overview. Trends Amplif. 2009, 13, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Kam, A.C.S.; Sung, J.K.K.; Yu, J.K.Y.; Tong, M.C.F. Clinical evaluation of a fully implantable hearing device in six patients with mixed and sensorineural hearing loss: Our experience. Clin. Otolaryngol. 2012, 37, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Pollack, M.C.; Carhart, R. Amplification for the Hearing Impaired; Grune & Stratton Inc.: Philadelphia, PA, USA, 1998; pp. 64–85. [Google Scholar]
- Zenner, H.P.; Leysieffer, H. Total implantation of the implex TICA hearing amplifier implant for high frequency sensorineural hearing loss: The Tubingen University experience. Otolaryngol. Clin. North Am. 2001, 34, 417–446. [Google Scholar] [CrossRef]
- Leysieffer, H.; Baumann, J.W.; Mayer, R.; Müller, D.; Müller, G.; Schön, T.; Volz, A.; Zenner, H.P. A totally implantable hearing aid for inner ear deafness: TICA LZ 3001. HNO 2003, 46, 853–863. [Google Scholar] [CrossRef]
- Bruschini, L.; Forli, F.; Santoro, A.; Bruschini, P.; Berrettini, S. Fully implantable otologics MET Carina™ device for the treatment of sensorineural hearing loss. Preliminary surgical and clinical results. Acta Otolaryngol. 2009, 29, 79–85. [Google Scholar]
- Pulcherio, J.O.B.; Bittencourt, A.G.; Burke, P.R.; Monsanto, R.D.C.; da Costa Monsanto, R.; de Brito, R.; Tsuji, R.K.; Bento, R.F. Carina® and Esteem®: A systematic review of fully implantable hearing devices. PLOS ONE 2014, 9, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Koch, M.; Essinger, T.M.; Bornitz, M.; Zahnert, T. Examination of a mechanical amplifier in the incudostapedial joint gap: FEM simulation and physical model. Sensors 2014, 14, 14356–14374. [Google Scholar] [CrossRef] [PubMed]
- Osberger, M.J.; Miyamoto, R.T.; Zimmerman-Phillips, S.; Kemink, J.L.; Stroer, B.S.; Firszt, J.S.; Novak, M.A. Independent evaluation of the speech perception abilities of children with the Nucleus 22-channel cochlear implant system. Ear Hear. 1991, 12, 66–80. [Google Scholar] [CrossRef]
- Cochlear Implants—Into a World of Sound. Available online: http://www.earassociates.com/services-cochlear-implants-san-jose-ca.html (accessed on 1 September 2015).
- Kraus, E.M.; Shohet, J.A.; Catalano, P.J. Envoy esteem totally implantable hearing system: Phase 2 trial, 1-year hearing results. Am. Acad. Otolaryngol. Head Neck Surg. 2011, 145, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Gerard, J.M.; Thill, M.P.; Chantrain, G.; Gersdorff, M.; Deggouj, N. Esteem 2 middle ear implant: Our experience. Audiol. Neurotol. 2012, 17, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Memari, F.; Asghari, A.; Daneshi, A.; Jalali, A. Safety and patient selection of totally implantable hearing aid surgery: Envoy system esteem. Eur. Arch. Oto-Rhino-Laryngol. 2011, 268, 1421–1425. [Google Scholar] [CrossRef] [PubMed]
- Deddens, A.E.; Wilson, E.P.; Fredrickson, J.M.; Deddens, A.E.; Wilson, E.P.; Lesser, T.H.J.; Fredrickson, J.M. Totally implantable hearing aids: The effects of skin thickness on microphone function. Am. J. Otolaryngol. 1990, 11, 1–4. [Google Scholar] [CrossRef]
- Jung, E.S.; Lim, H.G.; Cho, J.H.; Jung, E.S.; Seong, K.W.; Lim, H.G.; Lee, J.H.; Cho, J.H. Implantable microphone with acoustic tube for fully implantable hearing devices. IEICE Trans. Inf. Syst. 2011, 8, 215–219. [Google Scholar] [CrossRef]
- Jenkins, H.A.; Pergola, N.; Kasic, J. Anatomical vibrations that implantable microphones must overcome. Otol. Neurotol. 2007, 28, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Valente, M.; Hosford-Dunn, H.; Roeser, R.J. Audiology: Treatment; Thieme Medical Publisher: New York, NY, USA, 2007; pp. 331–332. [Google Scholar]
- Esteem Hearing Implant from Envoy Medical. Available online: http://www.audiologyonline.com/interviews/esteem-hearing-implant-from-envoy-12338 (accessed on 1 September 2015).
- Heerbeek, N.V.; de Saar, G.M.A.C.; Mulder, J.J.S. Long-term ventilation tubes: Results of 726 insertions. Clin. Otolaryngol. Allied Sci. 2002, 27, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Levy, S.C.; Freed, D.J.; Nilsson, M.; Moore, B.C.; Puria, S. Extended high-frequency bandwidth improves speech reception in the presence of spatially separated masking speech. Ear Hear. 2015, 36, e214–e224. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.; Guo, J.; Megerian, C.A.; Young, D.; Ko, W.H. A laboratory study on a capacitive displacement sensor as an implant microphone in totally implant cochlear hearing aid systems. In Proceedings of the 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS 2007, Lyon, France, 22–26 August 2007.
- Ko, W.H.; Zhang, R.; Huang, P.; Guo, J.; Ye, X.; Young, D.; Megerian, C.A. Studies of MEMS acoustic sensors as implantable microphones for totally implantable hearing-aid Systems. IEEE Trans. Biomed. Circuits Syst. 2009, 3, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Ko, W.H.; Huang, P.; Guo, J.; Zhang, R.; Young, D.; Megerian, C. MEMS acoustic sensors for totally implantable hearing aid systems. In Proceedings of the IEEE International Symposium on Circuits and Systems, ISCAS 2008, Seattle, WA, USA, 18–21 May 2008.
- Young, D.J.; Zurcher, M.A.; Semaan, M.; Megerian, C.A.; Ko, W.H. MEMS capacitive accelerometer-based middle ear microphone. IEEE Trans. Biomed. Eng. 2012, 59, 3283–3292. [Google Scholar] [CrossRef] [PubMed]
- Zurcher, D.; Young, J.; Semaan, M.; Megerian, C.; Ko, W.H. MEMS middle ear acoustic sensor for fully implantable cochlear prosthesis. In Proceedings of the IEEE 20th International Conference on Micro Electro Mechanical Systems, Hyogo, Japan, 21–25 January 2007.
- Yip, M.; Jin, R.; Nakajima, H.H.; Stankovic, K.H.; Chandrakasan, A.P. A fully-implantable cochlear implant SoC with piezoelectric middle-ear sensor and arbitrary waveform neural stimulation. IEEE J. Solid-State Circuits 2015, 50, 214–229. [Google Scholar] [CrossRef] [PubMed]
- Park, W.T.; O’Connor, K.N.; Chen, K.-L.; Mallon, J.R., Jr.; Maetani, T.; Dalal, P.; Candler, R.N.; Ayanoor-Vitikkate, V.; Roberson, J.B., Jr.; Puria, S.; et al. Ultraminiature encapsulated accelerometers as a fully implantable sensor for implantable hearing aids. Biomed. Microdevices 2007, 9, 939–949. [Google Scholar] [CrossRef] [PubMed]
- Marino, R.; Linton, N.; Eikelboom, R.H.; Statham, E.; Rajan, G.P. A comparative study of hearing aids and round window application of the vibrant sound bridge (VSB) for patients with mixed or conductive hearing loss. Int. J. Audiol. 2013, 52, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Adaptive Feedback Cancellation 3 from ON Semiconductor. Available online: http://www.onsemi.com/pub_link/Collateral/AND9020-D.PDF (accessed on 1 September 2015).
- Earwax and Care. Available online: http://www.entnet.org/content/earwax-and-care (accessed on 1 September 2015).
- McCarter, D.F.; Courtney, A.U.; Pollart, S.M. Cerumen impaction. Am. Fam. Physician 2007, 75, 1523–1528. [Google Scholar] [PubMed]
- Guest, J.F.; Greener, M.J.; Robinson, A.C; Smith, A.F. Impacted cerumen: Composition, production. Epidemiol. Manag. 2004, 97, 477–488. [Google Scholar]
- Roland, P.S.; Smith, T.L.; Schwartz, S.R.; Rosenfeld, R.M.; Ballachanda, B.; Earll, J.M.; Fayad, J.; Harlor, A.D., Jr.; Hirsch, B.E.; Jones, S.S.; et al. Clinical practice guideline: Cerumen impaction. Otolaryngol. Head Neck Surg. 2008, 139, S1–S21. [Google Scholar] [CrossRef] [PubMed]
- Mukerji, S. Medial migration of tympanostomy tubes: The why and what to do? Case report and review of literature. Austin J. Otolaryngol. 2015, 2, 1–2. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Woo, S.T.; Shin, D.H.; Lim, H.-G.; Seong, K.-W.; Gottlieb, P.; Puria, S.; Lee, K.-Y.; Cho, J.-H. A New Trans-Tympanic Microphone Approach for Fully Implantable Hearing Devices. Sensors 2015, 15, 22798-22810. https://doi.org/10.3390/s150922798
Woo ST, Shin DH, Lim H-G, Seong K-W, Gottlieb P, Puria S, Lee K-Y, Cho J-H. A New Trans-Tympanic Microphone Approach for Fully Implantable Hearing Devices. Sensors. 2015; 15(9):22798-22810. https://doi.org/10.3390/s150922798
Chicago/Turabian StyleWoo, Seong Tak, Dong Ho Shin, Hyung-Gyu Lim, Ki-Woong Seong, Peter Gottlieb, Sunil Puria, Kyu-Yup Lee, and Jin-Ho Cho. 2015. "A New Trans-Tympanic Microphone Approach for Fully Implantable Hearing Devices" Sensors 15, no. 9: 22798-22810. https://doi.org/10.3390/s150922798
APA StyleWoo, S. T., Shin, D. H., Lim, H.-G., Seong, K.-W., Gottlieb, P., Puria, S., Lee, K.-Y., & Cho, J.-H. (2015). A New Trans-Tympanic Microphone Approach for Fully Implantable Hearing Devices. Sensors, 15(9), 22798-22810. https://doi.org/10.3390/s150922798