
A Human Serum-Based Enzyme-Free Continuous Glucose Monitoring Technique Using a Needle-Type Bio-Layer Interference Sensor


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
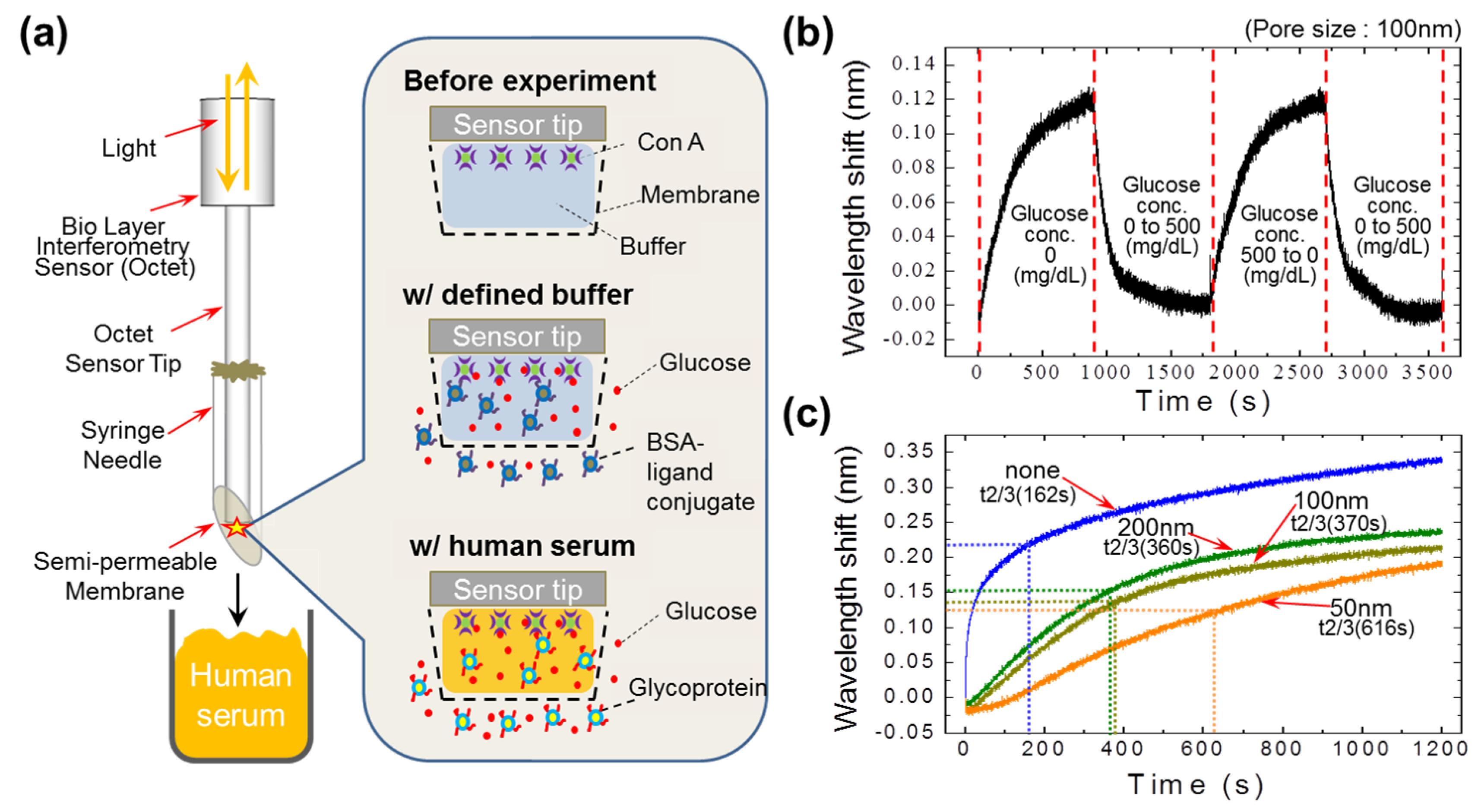
2.1. Fabrication of a Novel Needle-Type Sensor
2.2. Working Principle of a Newly-Developed Human Serum-Based Needle-Type Sensor
2.3. Sample Preparation
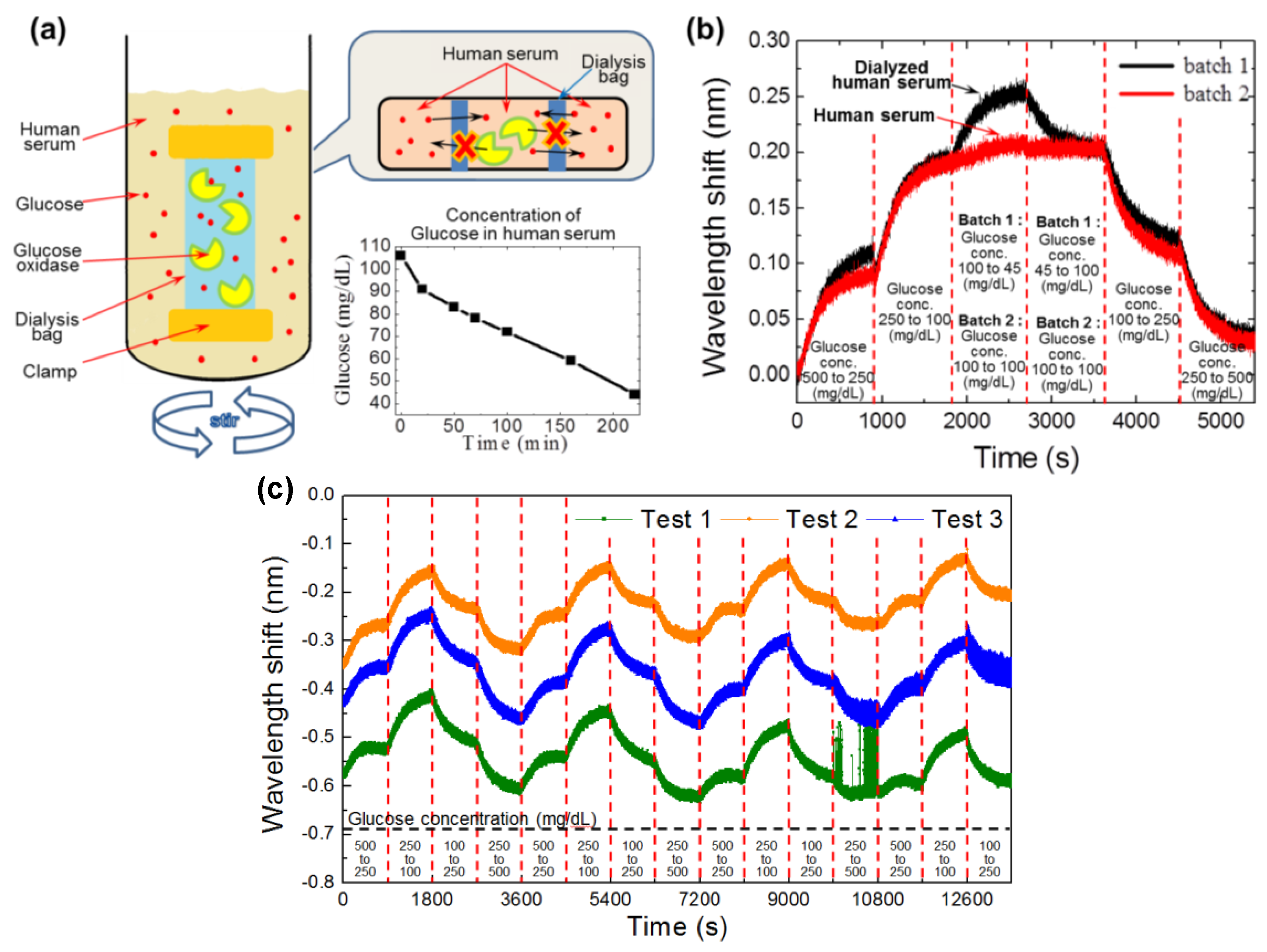
2.3.1. Selective Glucose Dialysis System Used to Obtain Hypoglycemic Samples
2.3.2. Preparation of Samples at Various Glucose Concentrations
2.4. Chemicals, Reagents, and Analytical Components Used
3. Results and Discussion
3.1. Performance of the Competitive Assay
3.2. Performance of the Semi-Permeable Membrane
3.3. Production and Screening of Hypoglycemic Samples
3.4. Comparison of the Needle-Type Sensor with the Ideal BLI Sensor
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- American Diabetes Association. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2014, 37, S81–S90. [Google Scholar]
- Dai, C.; Brissova, M.; Reinert, R.B.; Nyman, L.; Liu, E.H.; Thompson, C.; Shostak, A.; Shiota, M.; Takahashi, T.; Powers, A.C. Pancreatic Islet Vasculature Adapts to Insulin Resistance Through Dilation and Not Angiogenesis. Diabetes 2013, 62, 4144–4153. [Google Scholar] [CrossRef] [PubMed]
- Guariguata, L.; Whiting, D.R.; Hambleton, I.; Beagley, J.; Linnenkamp, U.; Shaw, J.E. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res. Clin. Pract. 2014, 103, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Cleland, C.R.; Burton, M.J.; Hall, C.; Hall, A.; Coutright, P.; Makupa, W.U.; Philippin, H. Diabetic retinopathy screening: Experiences from northern Tanzania. Lancet Diabetes Endocrinol. 2016, 4, 10–12. [Google Scholar] [CrossRef]
- Vachist, S.K. Continuous Glucose Monitoring Systems: A Review. Diagnostics 2013, 3, 385–412. [Google Scholar] [CrossRef] [PubMed]
- Ding, S.; Schumacher, M. Sensor Monitoring Physical Activity to Improve Glucose Management in Diabetic Patients: A Review. Sensors 2016, 16, 589. [Google Scholar] [CrossRef] [PubMed]
- Al-Halhouli, A.; Demming, S.; Alahmad, L.; Llobera, A.; Biittgenbach, S. An In-Line Photonic Biosensor for Monitoring of Glucose Concentrations. Sensors 2014, 14, 15749–15759. [Google Scholar] [CrossRef] [PubMed]
- Vaddiraju, S.; Burgess, D.J.; Tomazos, I.; Jain, F.C.; Papadimitrakopoulos, F. Technologies for Continuous Glucose Monitoring: Current Problems and Future Promises. J. Diabetes Sci. Technol. 2010, 4, 1540–1562. [Google Scholar] [CrossRef] [PubMed]
- Paek, S.-H.; Cho, I.-H.; Kim, D.-H.; Jeon, J.-W.; Lim, G.-S.; Paek, S.-H. Label-free, needle-type biosensor for continuous glucose monitoring based on competitive binding. Biosens. Bioelectron. 2013, 40, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Sone, H.; Shimano, H.; Ebinuma, H.; Takahashi, A.; Yano, Y.; Iida, K.T.; Suzuki, H.; Toyoshima, H.; Kawakami, Y.; Okuda, Y.; et al. Physiological Changes in Circulating Mannose Levels in Normal, Glucose-Intolerant, and Diabetic Subjects. Metabolism 2003, 52, 1019–1027. [Google Scholar] [CrossRef]
- Jonsson, A.; Wales, J.K. Blood glycoprotein levels in diabetes mellitus. Diabetologia 1976, 12, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Saleemuddin, M.; Husain, Q. Concanavalin A: A useful ligand for glycoenzyme immobilization—A review. Enzym. Microb. Technol. 1991, 13, 290–295. [Google Scholar] [CrossRef]
- Zhao, S.; Fernald, R.D. Comprehensive Algorithm for Quantitative Real-Time Polymerase Chain Reaction. J. Comput. Biol. 2005, 12, 1047–1064. [Google Scholar] [CrossRef] [PubMed]



© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seo, D.; Paek, S.-H.; Oh, S.; Seo, S.; Paek, S.-H. A Human Serum-Based Enzyme-Free Continuous Glucose Monitoring Technique Using a Needle-Type Bio-Layer Interference Sensor. Sensors 2016, 16, 1581. https://doi.org/10.3390/s16101581
Seo D, Paek S-H, Oh S, Seo S, Paek S-H. A Human Serum-Based Enzyme-Free Continuous Glucose Monitoring Technique Using a Needle-Type Bio-Layer Interference Sensor. Sensors. 2016; 16(10):1581. https://doi.org/10.3390/s16101581
Chicago/Turabian StyleSeo, Dongmin, Sung-Ho Paek, Sangwoo Oh, Sungkyu Seo, and Se-Hwan Paek. 2016. "A Human Serum-Based Enzyme-Free Continuous Glucose Monitoring Technique Using a Needle-Type Bio-Layer Interference Sensor" Sensors 16, no. 10: 1581. https://doi.org/10.3390/s16101581