
An Infrared Absorbance Sensor for the Detection of Melanoma in Skin Biopsies

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
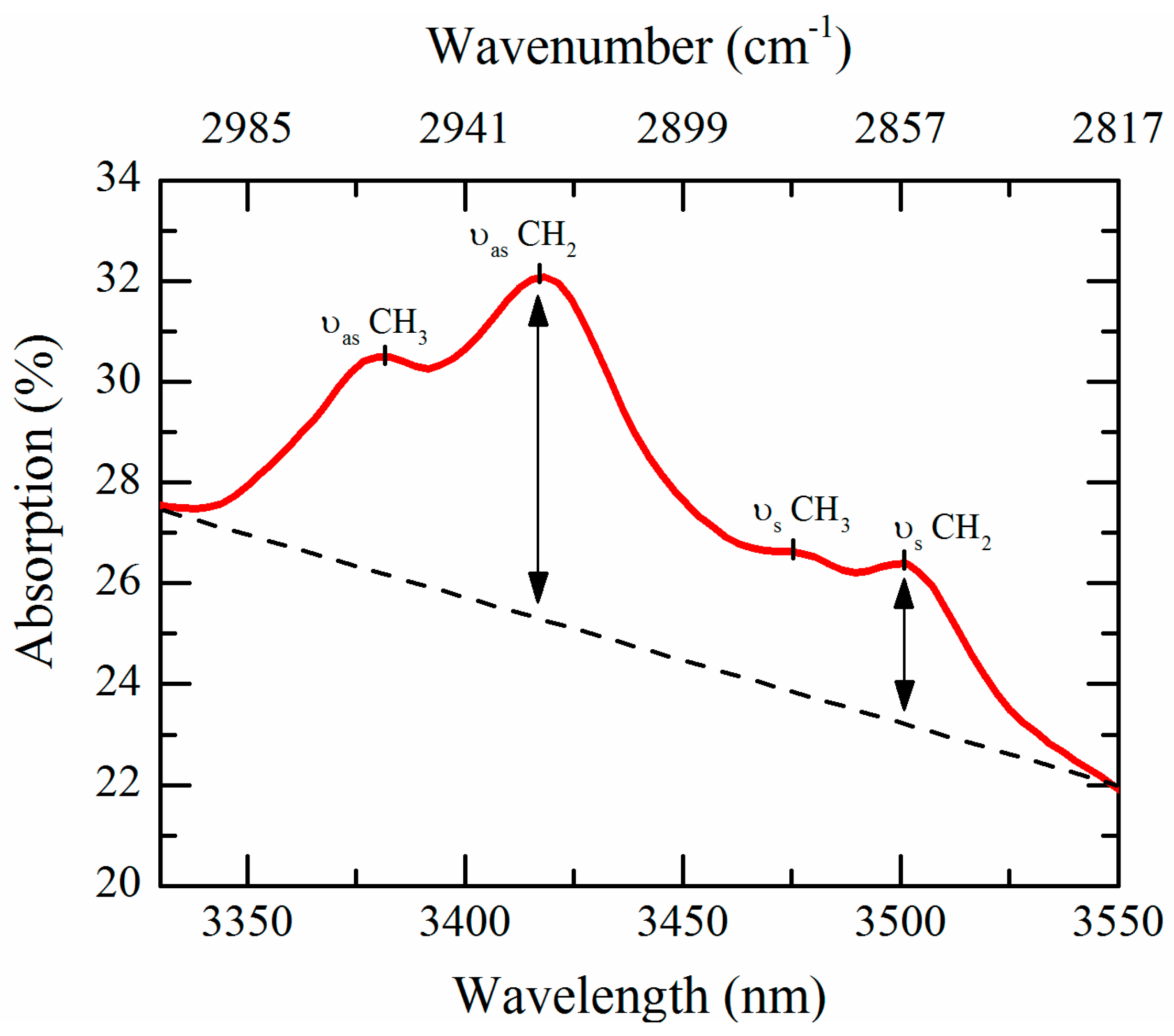
2.1. CH2 Stretch Ratio as a Cancer Indicator
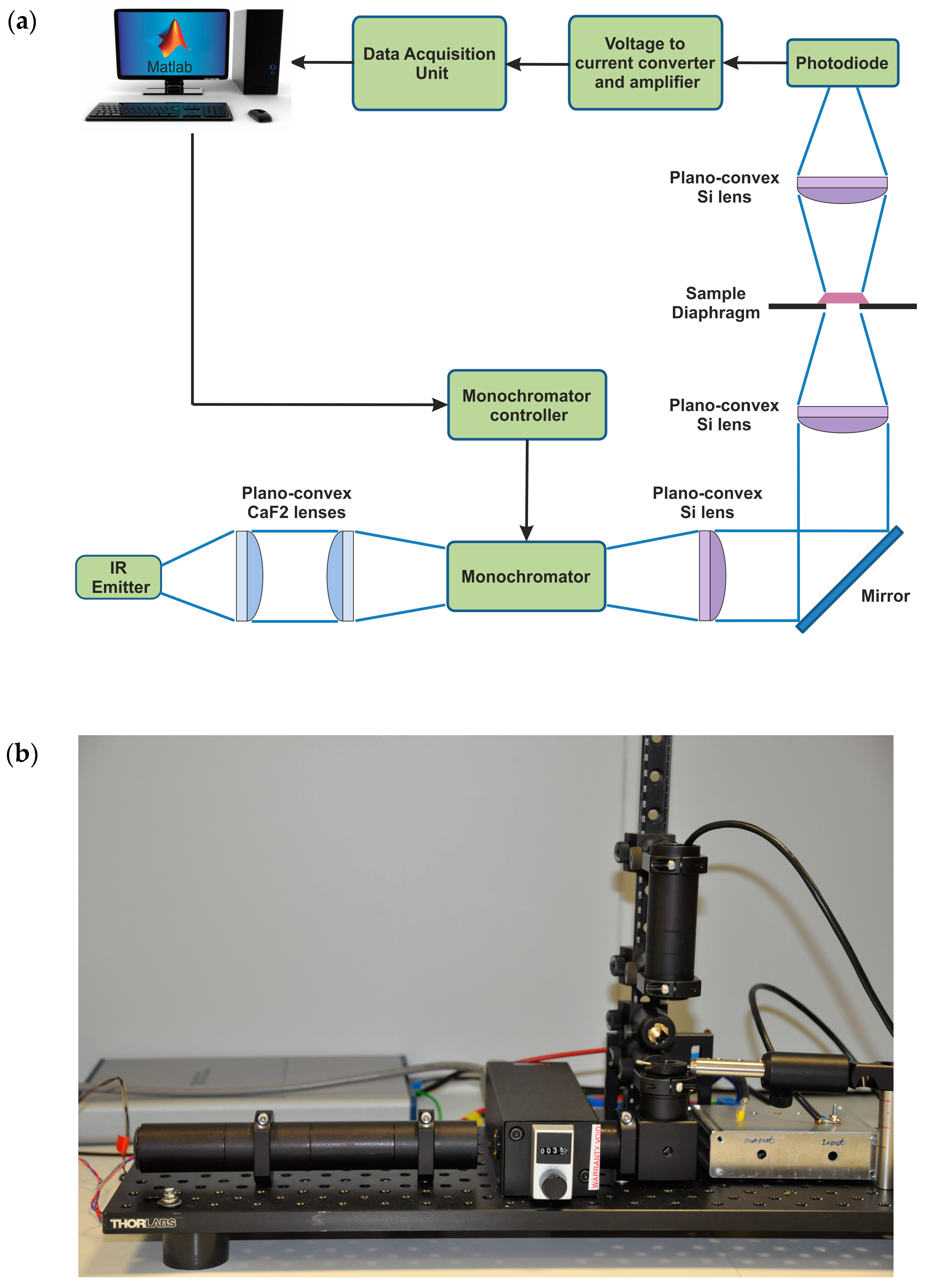
2.2. Infrared Absorbance Sensor
2.3. Skin Biopsy Preparation for IR Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A

References
- MacKie, R.M. Malignant melanoma: Clinical variants and prognostic indicators. Clin. Exp. Dermatol. 2000, 25, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Marks, R. Epidemiology of melanoma. Clin. Exp. Dermatol. 2000, 25, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Cichorek, M.; Wachulska, M.; Stasiewicz, A.; Tyminska, A. Skin melanocytes: Biology and development. Postep. Dermatol. Alergol. 2013, 30, 30–41. [Google Scholar] [CrossRef] [PubMed]
- MacKie, R.M.; Hauschild, A.; Eggermont, A.M. Epidemiology of invasive cutaneous melanoma. Ann. Oncol. 2009, 20, vi1–vi7. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Steliarova-Foucher, E.; Lortet-Tieulent, J.; Rosso, S.; Coebergh, J.W.; Comber, H.; Forman, D.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. Eur. J. Cancer. 2013, 49, 1374–1403. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, N.R.; Shaw, H.M.; Rigel, D.S.; Friedman, R.J.; McCarthy, W.H.; Osman, I.; Kopf, A.W.; Polsky, D. Early diagnosis of cutaneous melanoma: Revisiting the ABCD criteria. Jama 2004, 292, 2771–2776. [Google Scholar] [CrossRef] [PubMed]
- Urso, C.; Rongioletti, F.; Innocenzi, D.; Saieva, C.; Batolo, D.; Chimenti, S.; Filotico, R.; Gianotti, R.; Lentini, M.; Tomasini, C.; et al. Interobserver reproducibility of histological features in cutaneous malignant melanoma. J. Clin. Pathol. 2005, 58, 1194–1198. [Google Scholar] [CrossRef] [PubMed]
- Farmer, E.R.; Gonin, R.; Hanna, M.P. Discordance in the histopathologic diagnosis of melanoma and melanocytic nevi between expert pathologists. Hum. Pathol. 1996, 27, 528–531. [Google Scholar] [CrossRef]
- Herman, C. Emerging technologies for the detection of melanoma: Achieving better outcomes. Clin. Cosmet. Investig. Dermatol. 2012, 5, 195–212. [Google Scholar] [CrossRef] [PubMed]
- Mogensen, M.; Jemec, G.B. Diagnosis of nonmelanoma skin cancer/keratinocyte carcinoma: A review of diagnostic accuracy of nonmelanoma skin cancer diagnostic tests and technologies. Dermatol. Surg. 2007, 33, 1158–1174. [Google Scholar] [CrossRef] [PubMed]
- Andreassi, M.; Andreassi, L. Utility and limits of noninvasive methods in dermatology. Expert Rev. Dermatol. 2007, 2, 249–255. [Google Scholar] [CrossRef]
- Busam, K.J.; Hester, K.; Charles, C.; Sachs, D.L.; Antonescu, C.R.; Gonzalez, S.; Halpern, A.C. Detection of clinically amelanotic malignant melanoma and assessment of its margins by in vivo confocal scanning laser microscopy. Arch. Dermatol. 2001, 137, 923–929. [Google Scholar] [PubMed]
- Marghoob, A.A.; Charles, C.A.; Busam, K.J.; Rajadhyaksha, M.; Lee, G.; Clark-Loeser, L.; Halpern, A.C. In vivo confocal scanning laser microscopy of a series of congenital melanocytic nevi suggestive of having developed malignant melanoma. Arch. Dermatol. 2005, 141, 1401–1412. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, S.; Gilaberte-Calzada, Y. In vivo reflectance-mode confocal microscopy in clinical dermatology and cosmetology. Int. J. Cosmet. Sci. 2008, 30, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Gambichler, T.; Regeniter, P.; Bechara, F.G.; Orlikov, A.; Vasa, R.; Moussa, G.; Stücker, M.; Altmeyer, P.; Hoffmann, K. Characterization of benign and malignant melanocytic skin lesions using optical coherence tomography in vivo. J. Am. Acad. Dermatol. 2007, 57, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Goodson, A.G.; Grossman, D. Strategies for early melanoma detection: Approaches to the patient with nevi. J. Am. Acad. Dermatol. 2009, 60, 719–738. [Google Scholar] [CrossRef] [PubMed]
- Anbar, M. Assessment of physiologic and pathologic radiative heat dissipation using dynamic infrared imaging. Ann. N. Y. Acad. Sci. 2002, 972, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Pirtini, C.M.; Herman, C. Quantification of the thermal signature of a melanoma lesion. Int. J. Therm. Sci. 2011, 50, 421–431. [Google Scholar] [CrossRef]
- Herman, C. The role of dynamic infrared imaging in melanoma diagnosis. Expert Rev. Dermatol. 2013, 8, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Shada, A.L.; Dengel, L.T.; Petroni, G.R.; Smolkin, M.E.; Acton, S.; Slingluff, C.L. Infrared thermography of cutaneous melanoma metastases. J. Surg. Res. 2013, 182, e9–e14. [Google Scholar] [CrossRef] [PubMed]
- Aberg, P.; Birgersson, U.; Elsner, P.; Mohr, P.; Ollmar, S. Electrical impedance spectroscopy and the diagnostic accuracy for malignant melanoma. Exp. Dermatol. 2011, 20, 648–652. [Google Scholar] [CrossRef] [PubMed]
- Har-Shai, Y.; Glickman, Y.A.; Siller, G.; McLeod, R.; Topaz, M.; Howe, C.; Ginzburg, A.; Zamir, B.; Filo, O.; Kenan, G.; et al. Electrical impedance scanning for melanoma diagnosis: A validation study. Plast. Reconstr. Surg. 2005, 116, 782–790. [Google Scholar] [CrossRef] [PubMed]
- scibase.se. Available online: http://www.scibase.se (accessed on 24 August 2016).
- Malvehy, J.; Hauschild, A.; Curiel-Lewandrowski, C.; Mohr, P.; Hofmann-Wellenhof, R.; Motley, R.; Berking, C.; Grossman, D.; Paoli, J.; Loquai, C.; et al. Clinical performance of the Nevisense system in cutaneous melanoma detection: An international, multicenter, prospective and blinded clinical trial on efficacy and safety. Br. J. Dermatol. 2014, 171, 1099–1107. [Google Scholar] [CrossRef] [PubMed]
- Krafft, C.; Sergio, V. Biomedical applications of Raman and infrared spectroscopy to diagnose tissues. Spectroscopy 2006, 20, 195–218. [Google Scholar] [CrossRef]
- Kendall, C.; Isabelle, M.; Bazant-Hegemark, F.; Hutchings, J.; Orr, L.; Babrah, J.; Baker, R.; Stone, N. Vibrational spectroscopy: A clinical tool for cancer diagnostics. Analyst 2009, 134, 1029–1045. [Google Scholar] [CrossRef] [PubMed]
- Gniadecka, M.; Wulf, H.C.; Nielsen, O.F.; Christensen, D.H.; Hercogova, J. Distinctive molecular abnormalities in benign and malignant skin lesions: Studies by Raman spectroscopy. J. Photochem. Photobiol. 1997, 66, 418–423. [Google Scholar] [CrossRef]
- De Luca, A.C.; Dholakia, K.; Mazilu, M. Modulated Raman spectroscopy for enhanced cancer diagnosis at the cellular level. Sensors 2015, 15, 13680–13704. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, L.M.; Summers, R.; Jackson, M.; Mantsch, H.H.; Mansfield, J.R.; Howlett, M.; Crowson, A.N.; Toole, J.W. Towards non-invasive screening of skin lesions by near-infrared spectroscopy. J. Invest. Dermatol. 2001, 116, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Tfayli, A.; Piot, O.; Durlach, A.; Bernard, P.; Manfait, M. Discriminating nevus and melanoma on paraffin-embedded skin biopsies using FTIR microspectroscopy. Biochim. Biophys. Acta 2005, 1724, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Hammody, Z.; Argov, S.; Sahu, R.K.; Cagnano, E.; Moreha, R.; Mordechai, S. Distinction of malignant melanoma and epidermis using IR micro-spectroscopy and statistical methods. Analyst 2008, 133, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Ly, E.; Cardot-Leccia, N.; Ortonne, J.P.; Benchetrit, M.; Michiels, J.F.; Manfait, M.; Piot, O. Histopathological characterization of primary cutaneous melanoma using infrared microimaging: A proof-of-concept study. Br. J. Dermatol. 2010, 162, 1316–1323. [Google Scholar] [CrossRef] [PubMed]
- Tamm, L.K.; Tatulian, S.A. Infrared spectroscopy of proteins and peptides in lipid bilayers. Q. Rev. Biophys. 1997, 30, 365–429. [Google Scholar] [CrossRef] [PubMed]
- Farahi, R.H.; Passian, A.; Tetard, L.; Thundat, T. Pump-probe photothermal spectroscopy using quantum cascade lasers. J. Phys. D 2012, 45, 125101. [Google Scholar] [CrossRef]
- Rowlette, J.; Weide, M.; Bird, B.; Arnone, D.; Barre, M.; Day, T. High-confidence, highthroughput screening with high-def IR microspectroscopy. BioOptics World 2014, 7, 34–37. [Google Scholar]
- Kröger, N.; Egl, A.; Engel, M.; Gretz, N.; Haase, K.; Herpich, I.; Kränzlin, B.; Neudecker, S.; Pucci, A.; Schönhals, A.; et al. Quantum cascade laser–based hyperspectral imaging of biological tissue. J. Biomed. Opt. 2014, 19, 111607. [Google Scholar] [CrossRef] [PubMed]
- Curl, R.F.; Capasso, F.; Gmachl, C.; Kosterev, A.A.; McManus, B.; Lewicki, R.; Pusharsky, M.; Wysocki, G.; Tittel, F.K. Quantum cascade lasers in chemical physics. Chem. Phys. Lett. 2010, 487, 1–18. [Google Scholar] [CrossRef]
- Clemens, G.; Bird, B.; Weida, M.; Rowletteb, J.; Bakera, M.J. Quantum cascade laser-based mid-infrared spectrochemical imaging of tissues and biofluids. Spectrosc. Eur. 2014, 26, 14–19. [Google Scholar]
- Pilling, M.; Gardner, P. Fundamental developments in infrared spectroscopic imaging for biomedical applications. Chem. Soc. Rev. 2016, 45, 1935–1957. [Google Scholar] [CrossRef] [PubMed]
- Zeller, W.; Naehle, L.; Fuchs, P.; Gerschuetz, F.; Hildebrandt, L.; Koeth, J. DFB Lasers between 760 nm and 16 μm for Sensing Applications. Sensors 2010, 10, 2492–2510. [Google Scholar] [CrossRef] [PubMed]
- Rigas, B.; Morgello, S.; Goldman, I.S.; Wong, P.T. Human colorectal cancers display abnormal Fourier transform infrared spectra. Proc. Natl. Acad. Sci. USA 1990, 87, 8140–8144. [Google Scholar] [CrossRef] [PubMed]
- Maziak, D.E.; Do, M.T.; Shamji, F.M.; Sundaresan, S.R.; Perkins, D.G.; Wong, P.T.T. Fourier-transform infrared spectroscopic study of characteristic molecular structure in cancer cells of esophagus: An exploratory study. Cancer Detect. Prev. 2007, 31, 244–253. [Google Scholar] [CrossRef] [PubMed]
- Van den Driesche, S.; Witarski, W.; Pastorekova, S.; Vellekoop, M.J. A quadruple wavelength IR sensor system for label-free tumour screening. Meas. Sci. Technol. 2009, 20, 124015. [Google Scholar] [CrossRef]
- Van den Driesche, S.; Witarski, W.; Pastorekova, S.; Breiteneder, H.; Hafner, C.; Vellekoop, M.J. A label-free indicator for tumor cells based on the CH2-stretch ratio. Analyst 2011, 136, 2397–2402. [Google Scholar] [CrossRef] [PubMed]
- Quaroni, L.; Zlateva, T.; Sarafimov, B.; Kreuzer, H.W.; Wehbe, K.; Hegg, E.L.; Cinque, G. Synchrotron based infrared imaging and spectroscopy via focal plane array on live fibroblasts in D2O enriched medium. Biophys. Chem. 2014, 189, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Guyot-Sionnest, P.; Hunt, J.H.; Shen, Y.R. Sum-frequency vibrational spectroscopy of a Langmuir film: Study of molecular orientation of a two-dimensional system. Phys. Rev. Lett. 1987, 59, 1597–1600. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, F.; Gardiner, J.M. Membrane lipids and enzymes of cultured high- and low-metastatic B16 melanoma variants. Cancer Res. 1984, 44, 3262–3269. [Google Scholar] [PubMed]
- Ohe, C.; Sasaki, T.; Noi, M.; Goto, Y.; Itoh, K. Sum frequency generation spectroscopic study of the condensation effect of cholesterol on a lipid monolayer. Anal. Bioanal. Chem. 2007, 388, 73–79. [Google Scholar] [CrossRef] [PubMed]



© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fioravanti, V.; Brandhoff, L.; Van den Driesche, S.; Breiteneder, H.; Kitzwögerer, M.; Hafner, C.; Vellekoop, M.J. An Infrared Absorbance Sensor for the Detection of Melanoma in Skin Biopsies. Sensors 2016, 16, 1659. https://doi.org/10.3390/s16101659
Fioravanti V, Brandhoff L, Van den Driesche S, Breiteneder H, Kitzwögerer M, Hafner C, Vellekoop MJ. An Infrared Absorbance Sensor for the Detection of Melanoma in Skin Biopsies. Sensors. 2016; 16(10):1659. https://doi.org/10.3390/s16101659
Chicago/Turabian StyleFioravanti, Valeria, Lukas Brandhoff, Sander Van den Driesche, Heimo Breiteneder, Melitta Kitzwögerer, Christine Hafner, and Michael J. Vellekoop. 2016. "An Infrared Absorbance Sensor for the Detection of Melanoma in Skin Biopsies" Sensors 16, no. 10: 1659. https://doi.org/10.3390/s16101659
APA StyleFioravanti, V., Brandhoff, L., Van den Driesche, S., Breiteneder, H., Kitzwögerer, M., Hafner, C., & Vellekoop, M. J. (2016). An Infrared Absorbance Sensor for the Detection of Melanoma in Skin Biopsies. Sensors, 16(10), 1659. https://doi.org/10.3390/s16101659