
Localized Electrical Impedance Myography of the Biceps Brachii Muscle during Different Levels of Isometric Contraction and Fatigue


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Experiment
2.3. Data Analysis and Statistics
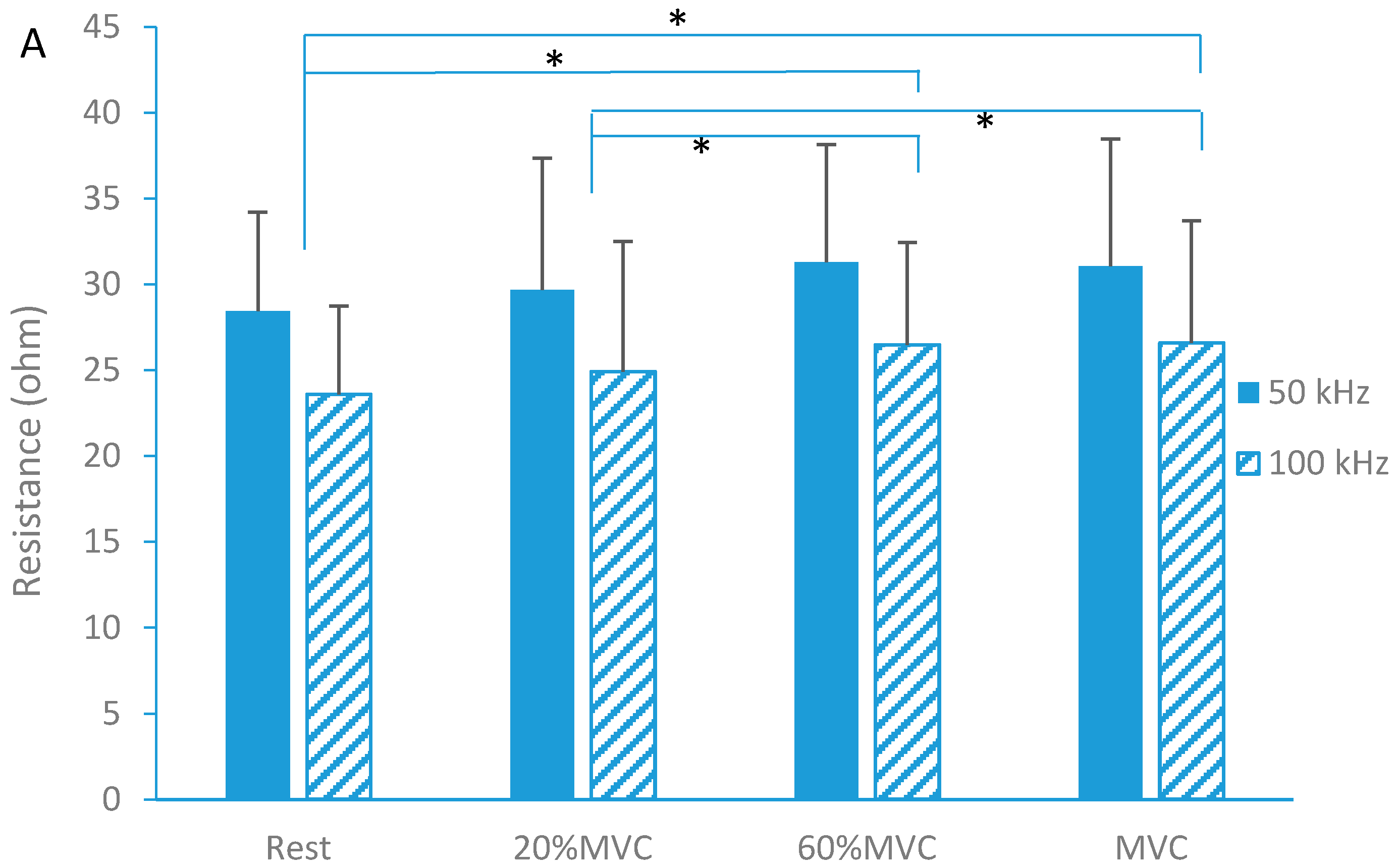
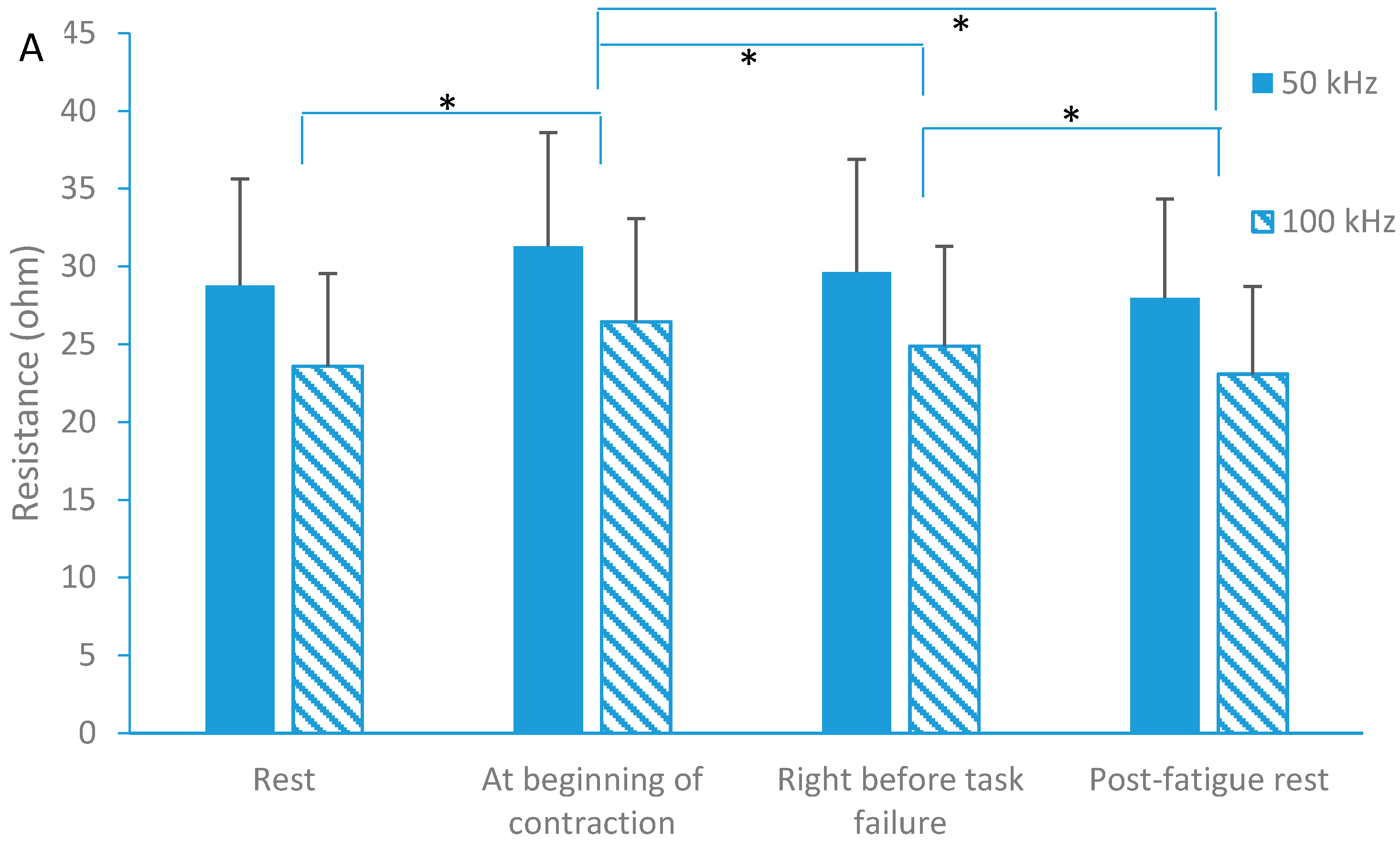
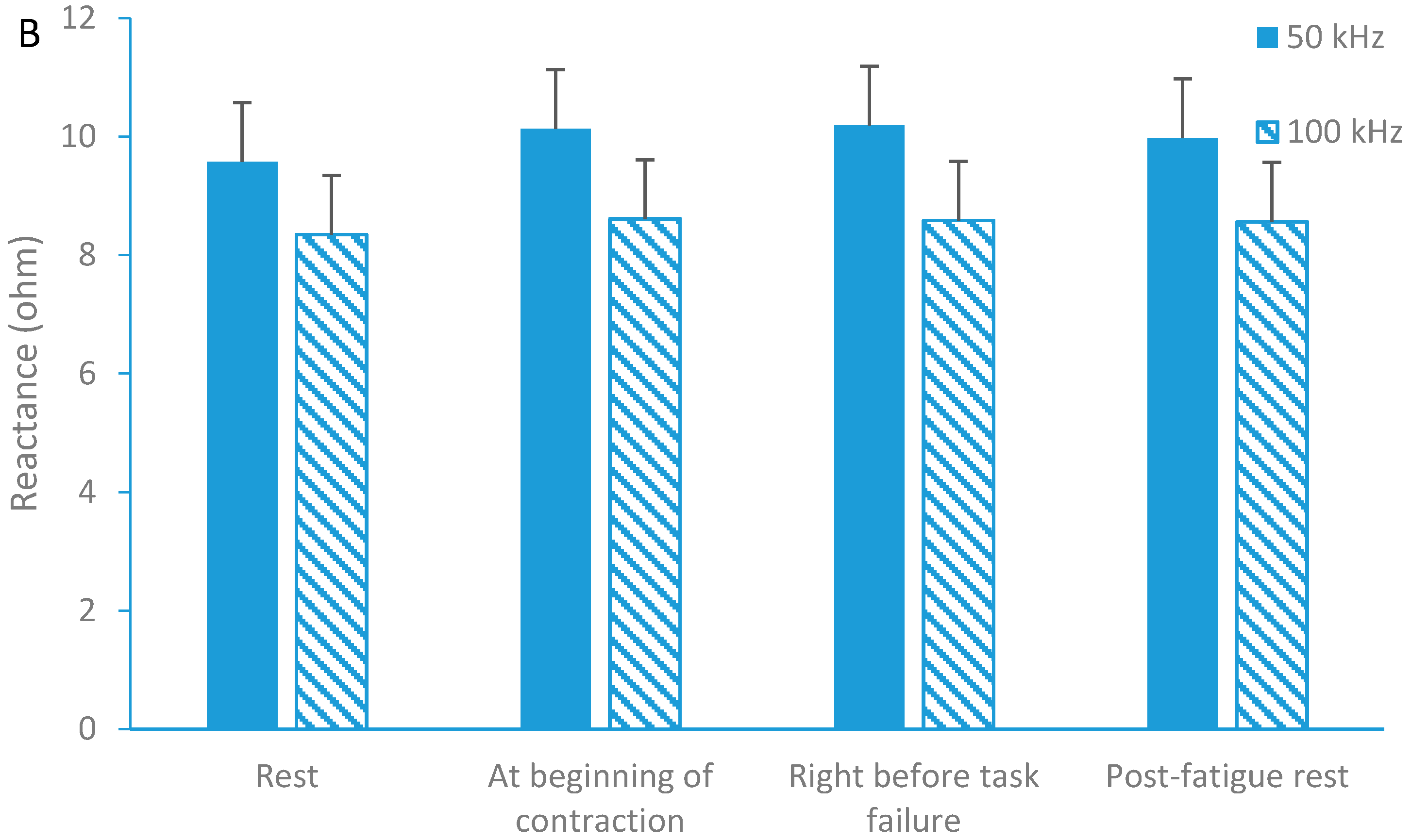
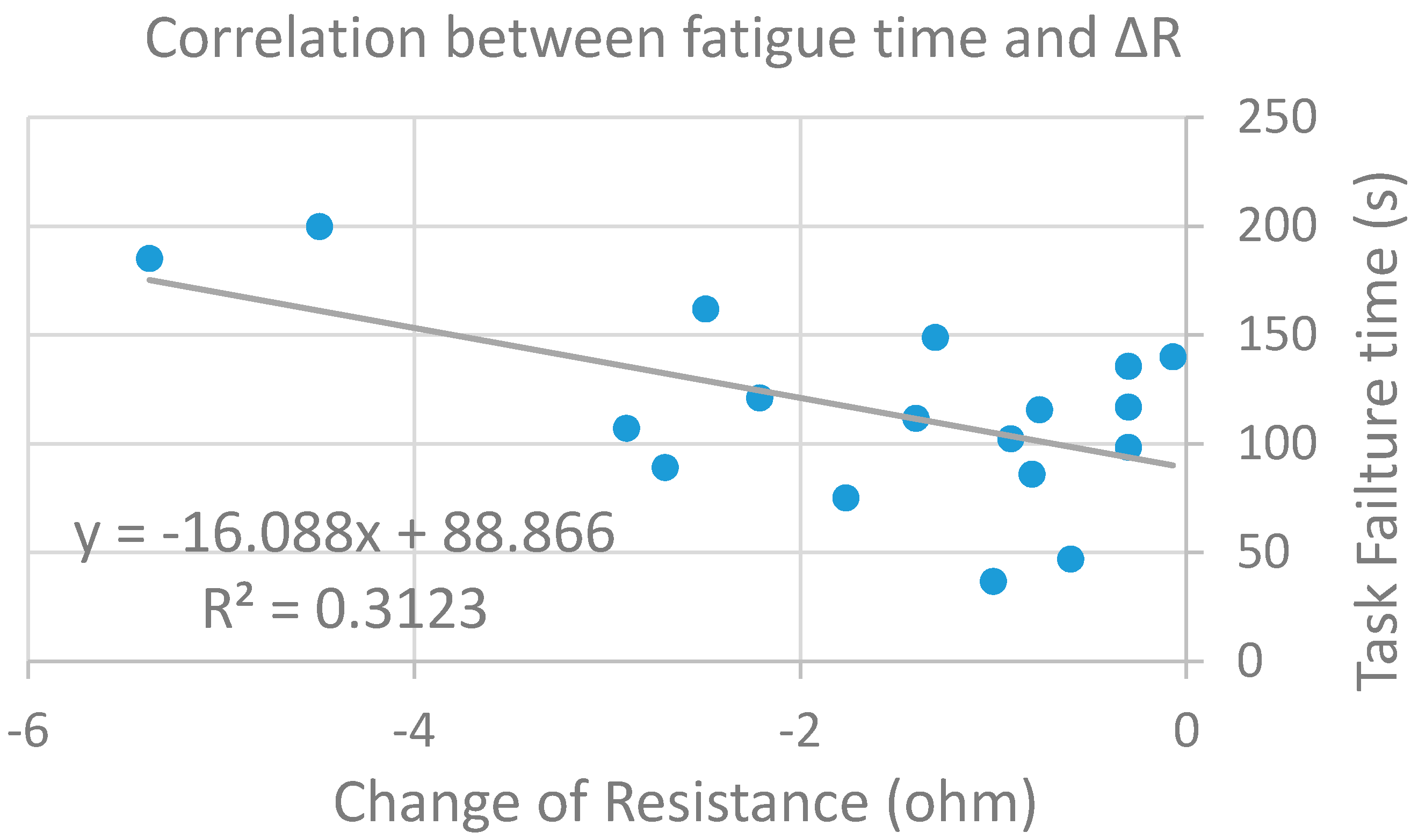
3. Results
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Rutkove, S.B. Electrical Impedance Myography: Background, Current State, and Future Directions. Muscle Nerve 2009, 40, 936–946. [Google Scholar] [CrossRef] [PubMed]
- Esper, G.J.; Shiffman, C.A.; Aaron, R.; Lee, K.S.; Rutkove, S.B. Assessing neuromuscular disease with multifrequency electrical impedance myography. Muscle Nerve 2006, 34, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Rutkove, S.B.; Aaron, R.; Shiffman, C.A. Localized bioimpedance analysis in the evaluation of neuromuscular disease. Muscle Nerve 2002, 25, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Chin, A.B.; Garmirian, L.P.; Nie, R.; Rutkove, S.B. Optimizing measurement of the electrical anisotropy of muscle. Muscle Nerve 2008, 37, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Tarulli, A.W.; Chin, A.B.; Partida, R.A.; Rutkove, S.B. Electrical impedance in bovine skeletal muscle as a model for the study of neuromuscular disease. Physiol Meas. 2006, 27, 1269–1279. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Spieker, A.J.; Rosen, G.D.; Rutkove, S.B. Electrical impedance alterations in the rat hind limb with unloading. J. Musculoskelet. Neuronal Interact. 2013, 13, 37–44. [Google Scholar] [PubMed]
- Aaron, R.; Huang, M.; Shiffman, C.A. Anisotropy of human muscle via non-invasive impedance measurements. Phys. Med. Biol. 1997, 42, 1245–1262. [Google Scholar] [CrossRef] [PubMed]
- Azizi, E.; Deslauriers, A.R. Regional heterogeneity in muscle fiber strain: The role of fiber architecture. Front. Physiol. 2014, 5. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Vargas, A.; Gonzalez-Sanchez, M. Correlation between architectural variables and torque in the erector spinae muscle during maximal isometric contraction. J. Sports Sci. 2014, 32, 1797–1804. [Google Scholar] [CrossRef] [PubMed]
- Maganaris, C.N.; Baltzopoulos, V. Predictability of in vivo changes in pennation angle of human tibialis anterior muscle from rest to maximum isometric dorsiflexion. Eur. J. Appl. Physiol. Occup. Physiol. 1999, 79, 294–297. [Google Scholar] [CrossRef] [PubMed]
- Walker, F.O.; Donofrio, P.D.; Harpold, G.J.; Ferrell, W.G. Sonographic imaging of muscle contraction and fasciculations: A correlation with electromyography. Muscle Nerve 1990, 13, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Aaron, R.; Shiffman, C.A. Localized muscle impedance measurements. In Skeletal Muscle Pathology, Diagnosis and Management of Disease; Preedy, V.R., Peters, T.J., Eds.; Greewich Medic: London, UK, 2002. [Google Scholar]
- Shiffman, C.A.; Aaron, R.; Rutkove, S.B. Electrical impedance of muscle during isometric contraction. Physiol. Meas. 2003, 24, 213–234. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, B.; Li, J.; Geisbush, T.; Bragos, R.; Rutkove, S. Impedance alterations in healthy and diseased mice during electrically-induced muscle contraction. IEEE Trans. Biomed. Eng. 2014. [Google Scholar] [CrossRef] [PubMed]
- Edwards, R.H.S. Human muscle function and fatigue. In Physiological Mechanisms; Pitman Medical: London, UK, 1981. [Google Scholar]
- Toffola, E.D.; Sparpaglione, D.; Pistorio, A.; Buonocore, M. Myoelectric manifestations of muscle changes in stroke patients. Arch. Phys. Med. Rehabil. 2001, 82, 661–665. [Google Scholar] [CrossRef] [PubMed]
- Angelini, C.; Tasca, E.; Nascimbeni, A.C.; Fanin, M. Muscle fatigue, nNOS and muscle fiber atrophy in limb girdle muscular dystrophy. Acta Myol. 2014, 33, 119–126. [Google Scholar] [PubMed]
- Neyroud, D.; Rüttimann, J.; Mannion, A.F.; Millet, G.Y.; Maffiuletti, N.A.; Kayser, B.; Place, N. Comparison of neuromuscular adjustments associated with sustained isometric contractions of four different muscle groups. J. Appl. Physiol. 2013, 114, 1426–1434. [Google Scholar] [CrossRef] [PubMed]
- Benson, C.; Docherty, D.; Brandenburg, J. Acute neuromuscular responses to resistance training performed at different loads. J. Sci. Med. Sport 2006, 9, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Bangsbo, J.; Graham, T.; Johansen, L.; Strange, S.; Christensen, C.; Saltin, B. Elevated muscle acidity and energy production during exhaustive exercise in humans. Am. J. Physiol. 1992, 263, R891–R899. [Google Scholar] [PubMed]
- Narayanaswami, P.; Spieker, A.J.; Mongiovi, P.; Keel, J.C.; Muzin, S.C.; Rutkove, S.B. Utilizing a handheld electrode array for localized muscle impedance measurements. Muscle Nerve 2012, 46, 257–63. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Liu, J.; Bhadane, M.; Zhou, P.; Rymer, W.Z. Activation deficit correlates with weakness in chronic stroke: Evidence from evoked and voluntary EMG recordings. Clin. Neurophysiol. 2014, 125, 2413–2417. [Google Scholar] [CrossRef] [PubMed]
- Jafarpoor, M.; Li, J.; White, J.K.; Rutkove, S.B. Optimizing electrode configuration for electrical impedance measurements of muscle via the finite element method. IEEE Trans. Biomed. Eng. 2013, 60, 1446–1452. [Google Scholar] [CrossRef] [PubMed]
- Booghs, C.; Baudry, S.; Enoka, R.; Duchateau, J. Influence of neural adjustments and muscle oxygenation on task failure during sustained isometric contractions with elbow flexor muscles. Exp. Physiol. 2012, 97, 918–929. [Google Scholar] [CrossRef] [PubMed]
- Beretta-Piccoli1, M.; D’Antona, G.; Barbero, M.; Fisher, B.; Dieli-Conwright, C.M.; Clijsen, R.; Cescon, C. Evaluation of central and peripheral fatigue in the quadriceps using fractal dimension and conduction velocity in young females. PLoS ONE 2015, 4, e0123921. [Google Scholar] [CrossRef] [PubMed]
- Garmirian, L.P.; Chin, A.B.; Rutkove, S.B. Discriminating neurogenic from myopathic disease via measurement of muscle anisotropy. Muscle Nerve 2009, 39, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Kashuri, H.; Aaron, R.; Shiffman, C.A. Frequency dependence of forearm muscle impedance during isometric gripping contractions. In 13th International Conference on Electrical Bioimpedance and the 8th Conference on Electrical Impedance Tomography; Scharfetter, H., Merwa, R., Eds.; Springer: Berlin, Germany; Heidelberg, Germany, 2007; Volume 17, pp. 651–654. [Google Scholar]
- Sung, M.; Spieker, A.J.; Narayanaswami, P.; Rutkove, S.B. The effect of subcutaneous fat on electrical impedance myography when using a handheld electrode array: The case for measuring reactance. Clin. Neurophysiol. 2013, 124, 400–404. [Google Scholar] [CrossRef] [PubMed]
- Romani, A. The treatment of fatigue. Neurol Sci. 2008, 29, S247–S249. [Google Scholar] [CrossRef] [PubMed]
- Allen, D.G.; Lamb, G.D.; Westerblad, H. Skeletal muscle fatigue: Cellular mechanisms. Physiol. Rev. 2008, 88, 287–332. [Google Scholar] [CrossRef] [PubMed]
- Sadamoto, T.; Bonde-Petersen, F.; Suzuki, Y. Skeletal muscle tension, flow, pressure, and EMG during sustained isometric contractions in humans. Eur. J. Appl. Physiol. Occup. Physiol. 1983, 51, 395–408. [Google Scholar] [CrossRef] [PubMed]
- Bigland-Ritchie, B.; Jones, D.A.; Woods, J.J. Excitation frequency and muscle fatigue: Electrical responses during human voluntary and stimulated contractions. Exp. Neurol. 1979, 64, 414–427. [Google Scholar] [CrossRef]
- Jones, D.A.; Bigland-Ritchie, B.; Edwards, R.H.T. Excitation frequency and muscle fatigue: Mechanical responses during voluntary and stimulated contractions. Exp. Neurol. 1979, 64, 401–413. [Google Scholar] [CrossRef]
- Taylor, J.L.; Gandevia, S.C. A comparison of central aspects of fatigue in submaximal and maximal voluntary contractions. J. Appl. Physiol. 2008, 104, 542–550. [Google Scholar] [CrossRef] [PubMed]
- Faes, T.J.; van der Meij, H.A.; de Munck, J.C.; Heethaar, R.M. The electric resistivity of human tissues (100 Hz–10 MHz): A meta-analysis of review studies. Physiol. Meas. 1999, 20, R1–R10. [Google Scholar] [CrossRef] [PubMed]
- Shiffman, C.A.; Kashuri, H.; Aaron, R. Electrical impedance myography at frequencies up to 2 MHz. Physiol. Meas. 2008, 29, S345–S363. [Google Scholar] [CrossRef] [PubMed]
- Rutkove, S.B.; Gregas, M.C.; Darras, B.T. Electrical impedance myography in spinal muscular atrophy: A longitudinal study. Muscle Nerve 2012, 45, 642–647. [Google Scholar] [CrossRef] [PubMed]
- Rutkove, S.B.; Caress, J.B.; Cartwright, M.S.; Burns, T.M.; Warder, J.; David, W.S.; Goyal, N.; Maragakis, N.J.; Benatar, M.; Sharma, K.R.; et al. Electrical impedance myography correlates with standard measures of ALS severity. Muscle Nerve 2014, 49, 441–443. [Google Scholar] [CrossRef] [PubMed]
- Shklyar, I.; Pasternak, A.; Kapur, K.; Darras, B.T.; Rutkove, S.B. Composite biomarkers for assessing duchenne muscular dystrophy: An initial assessment. Pediatr. Neurol. 2015, 52, 202–205. [Google Scholar] [CrossRef] [PubMed]
- Aaron, R.; Esper, G.J.; Shiffman, C.A.; Bradonjic, K.; Lee, K.S.; Rutkove, S.B. Effects of age on muscle as measured by electrical impedance myography. Physiol. Meas. 2006, 27, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Kortman, H.G.; Wilder, S.C.; Geisbush, T.R.; Narayanaswami, P.; Rutkove, S.B. Age- and gender-associated differences in electrical impedance values of skeletal muscle. Physiol. Meas. 2013, 34, 1611–1622. [Google Scholar] [CrossRef] [PubMed]






© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, L.; Shin, H.; Li, X.; Li, S.; Zhou, P. Localized Electrical Impedance Myography of the Biceps Brachii Muscle during Different Levels of Isometric Contraction and Fatigue. Sensors 2016, 16, 581. https://doi.org/10.3390/s16040581
Li L, Shin H, Li X, Li S, Zhou P. Localized Electrical Impedance Myography of the Biceps Brachii Muscle during Different Levels of Isometric Contraction and Fatigue. Sensors. 2016; 16(4):581. https://doi.org/10.3390/s16040581
Chicago/Turabian StyleLi, Le, Henry Shin, Xiaoyan Li, Sheng Li, and Ping Zhou. 2016. "Localized Electrical Impedance Myography of the Biceps Brachii Muscle during Different Levels of Isometric Contraction and Fatigue" Sensors 16, no. 4: 581. https://doi.org/10.3390/s16040581