
A Review of Classification Techniques of EMG Signals during Isotonic and Isometric Contractions


 , ,
, ,
Abstract
:1. Introduction
- signal-to-noise ratio
- noise signal
Noises in EMG Signals
Inherent Noise in Electronics Equipment
Ambient Noise
Motion Artifact
Inherent Instability of Signal
Electrocardiographic (ECG) Artifacts
Cross Talk
2. Motivation
2.1. Isotonic
2.1.1. Concentric Contractions
2.1.2. Eccentric Contractions
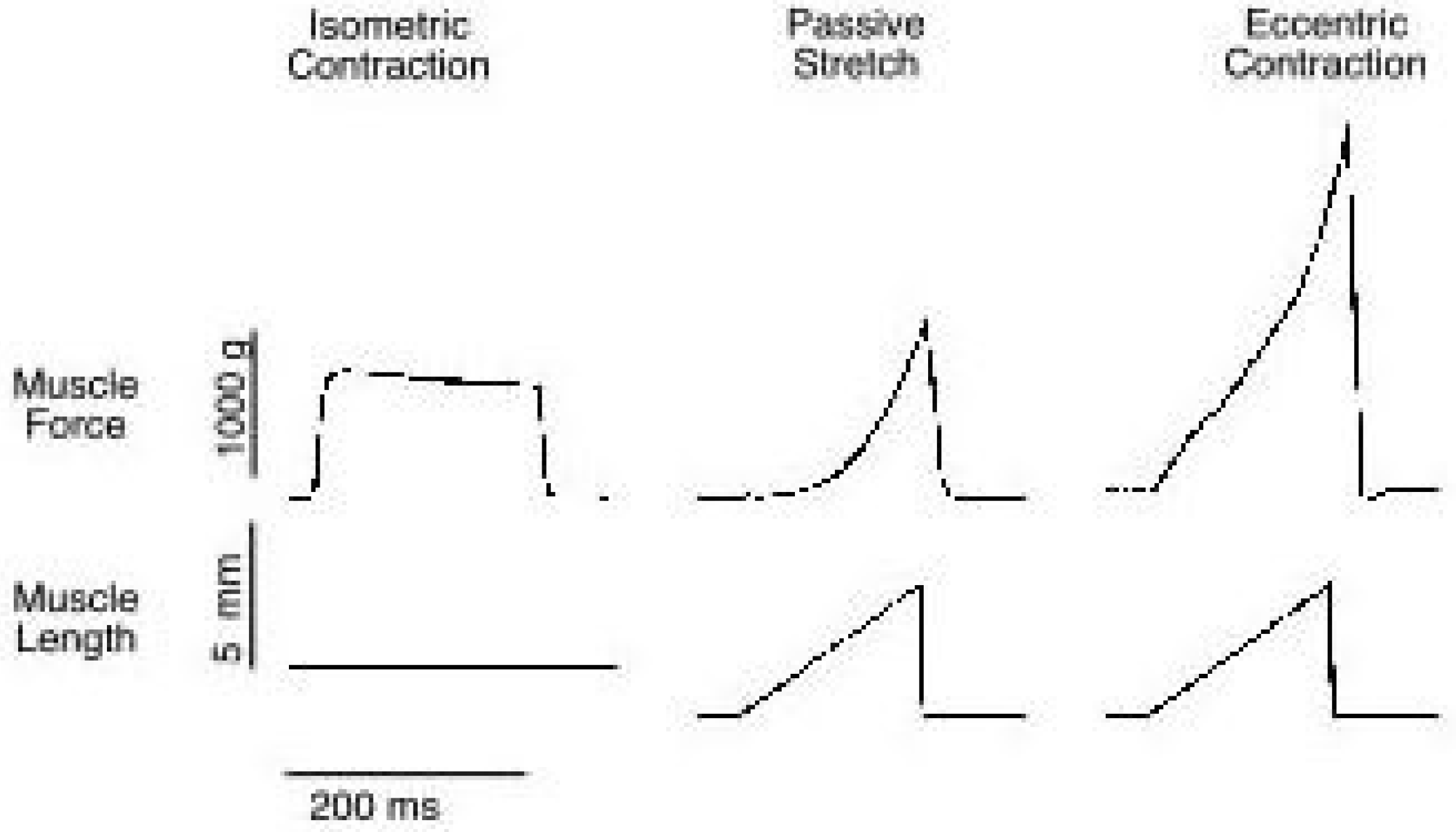
- Absolute tensions achieved are very high relative to the muscle’s maximum tetanic tension generating capacity.
- Absolute tension is relatively independent of lengthening velocity.
2.2. Isometric
3. Research Methodology
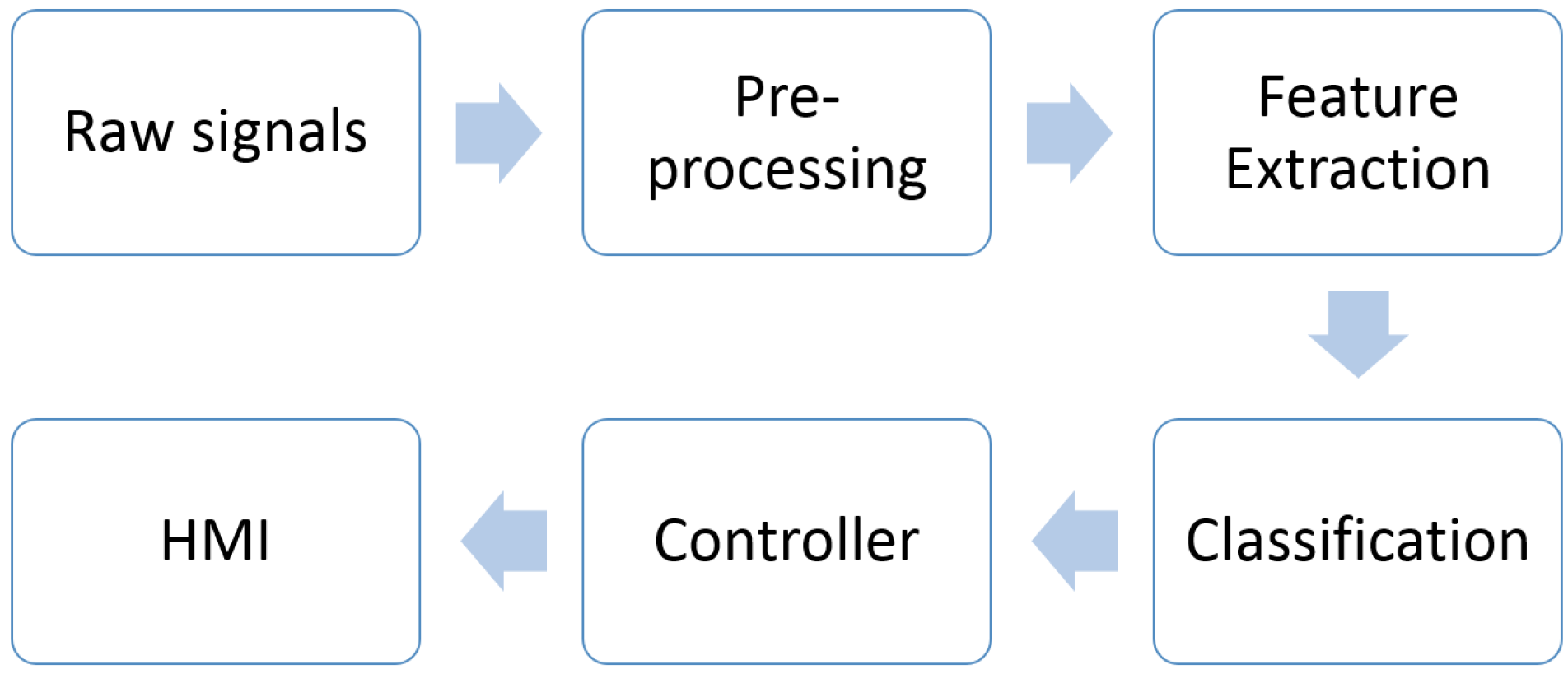
4. Automated EMG Analysis
4.1. EMG Signal Preprocessing
4.2. EMG Feature Extraction and Selection
- Feature projection
- Feature selection
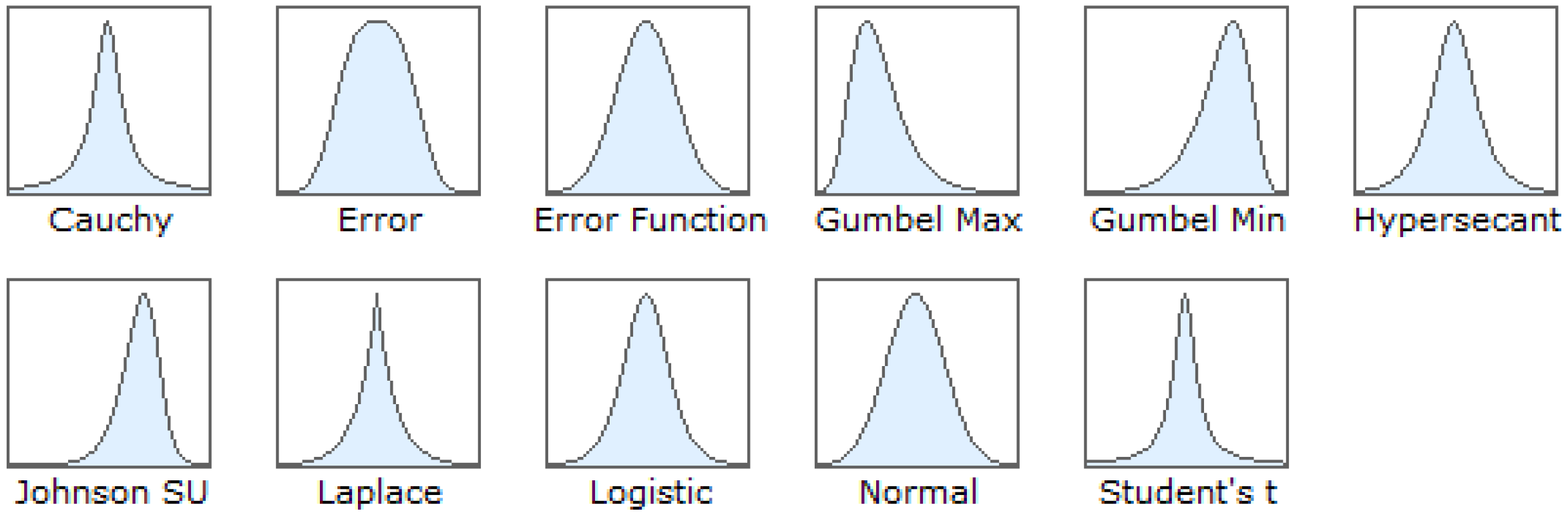
4.3. Probability Density Function
4.4. EMG Classification
4.5. EMG Evaluation Metrics
5. EMG Dataset
5.1. Placement of Electrodes
5.2. Muscle Conditions
6. Discussion
7. Future Trends
- Most studies do not critically highlight the pre-processing stage. To remove the artifacts in EMG signals, the cutoff frequency should be in the range between 20 Hz to 500 Hz and a Butterworth filter commonly applied. Meanwhile, the segmentation techniques used should depend upon its applications. However, the comparison performance between adjacent and overlapped windowing technique has not yet been identified.
- Feature extraction is the most difficult part in motion pattern recognition. In the literature, they compared the performance of TD, FD and TFD features of EMG signals during isometric contractions. The features of muscle contractions under isotonic has yet to be explored.
- Sample data of EMG signals has always been fitted with PDF under physical situations which correspond to non-fatiguing conditions, also called as isometric contractions. However, the PDF of isotonic contractions for EMG signals has never been investigated.
- To achieve better classification accuracy, significant features extracted is the main contribution. A classifier can be chosen depending on the number of features. Different classifiers result in different percentage error.
- Pattern recognition of EMG signals for upper limbs has been widely investigated compared to lower limbs especially in isometric contraction. The proper isotonic contractions behind the generation of the EMG signals is still unknown.
8. Conclusions
Acknowledgments
Conflicts of Interest
References
- Jiménez-Fabián, R.; Verlinden, O. Review of control algorithms for robotic ankle systems in lower-limb orthoses, prostheses, and exoskeletons. Med. Eng. Phys. 2012, 37, 505–511. [Google Scholar]
- Dzahir, M.A.M.; Nobutomo, T.; Yamamoto, S.I. Development of Gait Training System Powered by Antagonistic Monoand Bi-Articular Actuators using Contraction Model Control Scheme. Appl. Mech. Mater. 2013, 45393, 525–531. [Google Scholar] [CrossRef]
- Schweizer, K.; Brunner, R.; Romkes, J. Upper body movements in children with hemiplegic cerebral palsy walking with and without an ankle–foot orthosis. Clin. Biomech. 2014, 29, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.P.; Tan, A.W.; Tan, S.C. Gait recognition with Transient Binary Patterns. J. Vis. Commun. Image R 2015, 33, 69–77. [Google Scholar] [CrossRef]
- Ferris, D.P.; Gordon, K.E.; Sawicki, G.S.; Peethambaran, A. An improved powered ankle-foot orthosis using proportional myoelectric control. J. Gait Posture 2006, 23, 425–428. [Google Scholar] [CrossRef] [PubMed]
- Konrad, P. The ABC of EMG, A Practical Introduction to Kinesiological Electromyography; Noraxon Inc.: Scottsdale, AZ, USA, 2005. [Google Scholar]
- Wan Daud, W.M.B.; Yahya, A.B.; Horng, C.S.; Sulaima, M.F.; Sudirman, R. Features Extraction of Electromyography Signals in Time Domain on Biceps Brachii Muscle; International Journal of Modeling and Optimization: Bucharest, Romania, 2013; Volume 3. [Google Scholar]
- Reaz, M.B.I.; Hussain, M.S.; Mohd-Yasin, F. Techniques of EMG Signal Analysis: Detection, Processing, Classification and Applications; Biological Procedures Online: London, UK, 2006. [Google Scholar]
- Chowdhury, R.H.; Reaz, M.B.I.; Ali, M.A.M. Surface Electromyography Signal Processing and Classification Techniques. Sensors 2013, 13, 12431–12466. [Google Scholar] [CrossRef] [PubMed]
- Nadzri, A.A.A.; Ahmad, S.A.; Marhaban, M.H.; Haslina, J. Characterization of surface electromyography using time domain features for determining hand motion and stages of contraction. Australas. Phys. Eng. Sci. Med. 2014, 37, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Nardo, F.D.; Mengarelli, A.; Maranesi, E.; Burattini, L.; Fioretti, S. Assessment of the ankle muscle co-contraction during normal gait: A surface electromyography study. J. Electromyogr. Kinesiol. 2015, 25, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.A.; Chappel, P.H. Surface EMG pattern analysis of the wrist muscles at different speeds of contraction. J. Med. Eng. Technol. 2009, 33, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Balbinot, A.; Favieiro, G. A Neuro-Fuzzy System for Characterization of Arm Movements. Sensors 2013, 13, 2613–2630. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.V. The heat of shortening and the dynamic constants of muscle. Proc. R. Soc. Lond. Ser. B Biol. Sci. 1938, 126, 136–195. [Google Scholar] [CrossRef]
- Rosen, J.; Brand, M.; Fuchs, M.B.; Arcan, M. A myosignal-based powered exoskeleton system. IEEE Trans. Syst. Man Syst. Man Cybern. Part A Syst. Hum. 2001, 31, 210–222. [Google Scholar] [CrossRef]
- Fleischer, C.; Wege, A.; Kondak, K.; Hommel, G. Application of EMG signals for controlling exoskeleton robots. Conf. Biomed. Tech. 2006, 51, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Naeem, U.J. Human Arm’s Muscle Force Estimation Model Based on Fuzzy Theory. Appl. Mech. Mater. 2014, 551, 96–103. [Google Scholar] [CrossRef]
- Behrens, M.; Mau-Moeller, A.; Mueller, K.; Heise, S.; Gube, M.; Beuster, N.; Herlyn, P.K.; Fischer, D.C.; Bruhn, S. Plyometric training improves voluntary activation and strength during isometric, concentric and eccentric contractions. J. Sci. Med. Sport 2016, 19, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Al-Mulla, M.R.; Sepu, F.; Co, M. A Review of Non-Invasive Techniques to Detect and Predict Localised Muscle Fatigue. Sensors 2011, 11, 3545–3594. [Google Scholar] [CrossRef] [PubMed]
- Goslow, G.E.; Reinking, R.M.; Stuart, D.G. The cat step cycle: Hind limb joint angles and muscle lengths during unrestrained locomotion. J. Morphol. 1973, 141, 1–41. [Google Scholar] [CrossRef] [PubMed]
- Hoffer, J.; Caputi, A.; Pose, I.; Griffiths, R. Roles of muscle activity and load on the relationship between muscle spindle length and whole muscle length in the freely walking cat. Progr. Brain Res. 1989, 80, 75–85. [Google Scholar]
- Subasi, A. Classification of EMG signals using PSO optimized SVM for diagnosis of neuromuscular disorders. Comput. Biol. Med. 2013, 43, 576–586. [Google Scholar] [CrossRef] [PubMed]
- Rogers, D.R.; MacIsaac, D.T. A comparison of EMG-based muscle fatigue assessments during dynamic contractions. J. Electromyogr. Kinesiol. 2013, 23, 1004–1011. [Google Scholar] [CrossRef] [PubMed]
- Rechy-Ramirezn, E.J.; Huosheng, H. Bio-signal based control in assistive robots: A survey. Digit. Commun. Netw. 2015, 1, 85–101. [Google Scholar] [CrossRef]
- Yan, T.; Cempini, M.; Oddo, C.M.; Vitiello, N. Review of assistive strategies in powered lower-limb orthoses and exoskeletons. Robot. Auton. Syst. 2015, 64, 120–136. [Google Scholar] [CrossRef]
- Lorrain, T.; Jiang, N.; Farina, D. Influence of the training set on the accuracy of surface EMG classification in dynamic contractions for the control of multifunction prostheses. J. Neuroeng. Rehabil. 2011, 11, 8–25. [Google Scholar] [CrossRef] [PubMed]
- Phinyomark, A.; Qu, F.; Chrbonnier, S.; Serviere, C.; Tarpin-Benard, F.; Laurillau, Y. EMG feature evaluation for improving myoelectric pattern recognition robustness. Expert Syst. Appl. 2013, 40, 4832–4840. [Google Scholar] [CrossRef]
- Angkoon Phinyomark, P.P.; Limsakul, C. Feature reduction and selection for EMG signal classification. Expert Syst. Appl. 2012, 7, 7420–7431. [Google Scholar] [CrossRef]
- Tsai, A.C.; Hsieh, T.H.; Luh, J.J.; Lin, T.T. A comparison of upper-limb motion pattern recognition using EMG signals during dynamic and isometric muscle contractions. Biomed. Signal Process. Control 2014, 11, 17–26. [Google Scholar] [CrossRef]
- Thongpanja, S.; Phinyomark, A.; Limsakul, C.; Phukpattaranont, P. Analysis of Electromyography in Dynamic Hand Motions Using L-Kurtosis. Appl. Mech. Mater. 2015, 781, 604–607. [Google Scholar] [CrossRef]
- Nazarpour, K.; Al-Timemy, A.H.; Bugmann, G.; Jackson, A. A note on the probability distribution function of the surface electromyogram signal. Brain Res. Bull. 2013, 90, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Englehart, K.; Hudgins, B. A robust, real-time control scheme for multifunction myoelectric control. IEEE Trans. Biomed. Eng. 2003, 50, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Farina, D.; Merletti, R. Comparison of algorithms for estimation of EMG variables during voluntary isometric contractions. J. Electromyogr. Kinesiol. 2000, 10, 337–349. [Google Scholar] [CrossRef]
- Matsubara, T.; Morimoto, J. Bilinear Modeling of EMG Signals to Extract User-Independent Features for Multiuser Myoelectric Interface. IEEE Trans. Biomed. Eng. 2013, 6, 2205–2213. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.A. Moving Approximate Entropy and its Application to the Electromyographic Control of an Artificial Hand. Ph.D. Thesis, University of Southamptom, Southampton, UK, 2009. [Google Scholar]
- Englehart, K.; Hudgin, B.; Parker, P.A. A wavelet-based continuous classification scheme for multifunction myoelectric control. IEEE Trans. Biomed. Eng. 2001, 48, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Yeom, H.; Yoon, U. ECG Artifact Removal from Surface EMG Using Adaptive Filter Algorithm. Int. J. Multimed. Ubiquitous Eng. 2012, 1, 533–538. [Google Scholar]
- Lu, G.; Brittain, J.S.; Holland, P.; Yianni, J.; Green, A.L.; Stein, J.F.; Aziz, T.Z.; Wang, S. Removing ECG noise from surface EMG signals using adaptive filtering. Neurosci. Lett. 2009, 462, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Abbaspour, S.; Fallah, A. Removing ECG Artifact from the Surface EMG Signal Using Adaptive Subtraction Technique. J. Biomed. Phys. Eng. 2014, 4, 33–38. [Google Scholar] [PubMed]
- Benedetti, M.G.; Agostini, V.; Knaflitz, M.; Bonato, P. Applications of EMG in Clinical and Sports Medicine; InTech: Zagreb, Croatia, 2012; pp. 117–130. [Google Scholar]
- Kendell, C.; Lemaire, E.D.; Losier, Y.; Chan, A.; Hudgins, B. A novel approach to surface electromyography: An exploratory study of electrode-pair selection based on signal characteristics. J. Neuro Eng. Rehabil. 2012, 9. [Google Scholar] [CrossRef] [PubMed]
- Al-Angari, H.M.; Kanitz, G.; Tarantino, S.; Cipriani, C. Distance and mutual information methods for EMG feature and channel subset selection for classification of hand movements. Biomed. Signal Process. Control 2016, 27, 24–31. [Google Scholar] [CrossRef]
- Hogan, N.; Mann, R.W. Myoelectric Signal Processing: Optimal Estimation Applied to Electromyography—Part I: Derivation of the Optimal Myoprocessor. IEEE Trans. Biomed. Eng. 1980, BME-27, 382–395. [Google Scholar] [CrossRef]
- Englehart, K.; Hudgins, B.; Parker, P.A.; Stevenson, M. Classification of the myoelectric signal using time-frequency based representations. Med. Eng. Phys. 1999, 21, 431–438. [Google Scholar] [CrossRef]
- Oskoei, M.A.; Hu, H. Myoelectric control systems—A survey. Biomed. Signal Process. Control 2007, 2, 275–294. [Google Scholar] [CrossRef]
- Hudgins, B.; Parker, P.; Scott, R. A new strategy for multifunction myoelectric control. IEEE Trans. Biomed. Eng. 1993, 1, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Ahsan, M.R.; Ibrahimy, M.; Khalifa, O. Neural Network Classifier for Hand Motion Detection from EMG Signal; Springer Berlin Heidelberg: Kuala Lumpur, Malaysia, 2011; pp. 536–541. [Google Scholar]
- Sun, R.; Song, R.; Tong, K.Y. Complexity Analysis of EMG Signals for Patients After Stroke During Robot-Aided Rehabilitation Training Using Fuzzy Approximate Entropy. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Hamedi, M.; Salleh, S.H.; Noor, A.M.; Swee, T.T.; Afizam, I.K. Comparison of Different Time-Domain Feature Extraction Methods on Facial Gestures’ EMGs. Prog. Electromagn. Res. Symp. Proc. 2012, 12, 1897–1900. [Google Scholar]
- Tkach, D.; Huang, H.; Kuiken, T.A. Study of stability of time-domain features for electromyographic pattern recognition. J. Neuro Eng. Rehabil. 2010. [Google Scholar] [CrossRef] [PubMed]
- Oskoei, M.A.; Hu, H. Support vector machine-based classification scheme for myoelectric control applied to upper limb. IEEE Trans. Biomed. Eng. 2008, 55, 1956–1965. [Google Scholar] [CrossRef] [PubMed]
- Khushaba, R.N.; Al-Ani, A.; Al-Jumaily, A. Orthogonal fuzzy neighborhood discriminant analysis for multifunction myoelectric hand control. IEEE Trans. Biomed. Eng. 2010, 57, 1410–1419. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhou, P. Sample entropy analysis of surface EMG for improved muscle activity onset detection against spurious background spikes. J. Electromyogr. Kinesiol. 2012, 22, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Shin, H.; Zhou, P.; Niu, X.; Liu, J.; Rymer, W.Z. Power spectral analysis of surface electromyography (EMG) at matched contraction levels of the first dorsal interosseous muscle in stroke survivors. Clin. Neurophysiol. 2014, 125, 988–994. [Google Scholar] [CrossRef] [PubMed]
- Merletti, L.C. Surface EMG signal processing during isometric con- tractions. J. Electromyogr. Kinesiol. 1997, 7, 241–250. [Google Scholar] [CrossRef]
- Phinyomark, A.; Limsakul, C.; Phukpattaranont, P. Novel Feature Extraction for Robust EMG Pattern Recognition. J. Comput. 2009, 1, 71–80. [Google Scholar]
- Tsai, A.C.; Luh, J.J.; Lin, T.T. A novel STFT-ranking feature of multi-channel EMG for motion pattern recognition. Expert Syst. Appl. 2015, 42, 3327–3341. [Google Scholar] [CrossRef]
- Linnamo, V. Motor Unit Activation and Force Production during Eccentric, Concentric and Isometric Actions. Ph.D. Thesis, University of Jyvӓskylӓ, Jyvӓskylӓ, Finland, 2002. [Google Scholar]
- Kossev, A.; Christova, P. Discharge pattern ofhuman motor units during dynamic concentric and eccentric contractions. Electroencephalogr. Clin. Neurophysiol./Electromyogr. Motor Control 1998, 109, 245–255. [Google Scholar] [CrossRef]
- Oskoei, M.; Hu, H. GA-based feature subset selection for myoelectric classification. IEEE Int. Conf. Robot. Biomim. 2006, 1465–1470. [Google Scholar] [CrossRef]
- Basu, B.; Nagarajaiah, S.; Chakraborty, A. Online identification of linear time-varying stiffness of structural systems by wavelet analysis. Struct. Health Monit. 2008, 7, 21–36. [Google Scholar] [CrossRef]
- Guo, Y.; Kareem, A. Non-stationary frequency domain system identifi cation using time—Frequency representations. Mech. Syst. Signal Process. 2016, 72/73, 712–726. [Google Scholar] [CrossRef]
- Englehart, K. Signal Representation for Classification of the Transient Myoelectric Signal. Ph.D. Thesis, University of New Brunswick, Saint John, NB, Canada, 1998. [Google Scholar]
- Carrillo, R.E.; Aysal, T.C.; Barner, K.E. A Generalized Cauchy Distribution Framework for Problems Requiring Robust Behavior. EURASIP J. Adv. Signal. Process. 2010, 2010, 1–19. [Google Scholar] [CrossRef]
- Rosa, I.D.G.; Garcia, M.A.C.; Souza, M.N.D. Investigation of probability density functions in modeling sample distribution of surface electromyographic (sEMG) signals. Arch. Control Sci. 2013, 23, 381–393. [Google Scholar]
- Rasool, G.; Iqbal, K.; White, G. Myoelectric activity detection during a Sit-to-Stand movement using threshold methods. Comput. Math. Appl. 2012, 64, 1473–1483. [Google Scholar] [CrossRef]
- Micera, S.; Carpaneto, J.; Raspopovic, S. Control of Hand Prostheses Using Peripheral Information. IEEE Rev. Biomed. Eng. 2010, 3, 48–68. [Google Scholar] [CrossRef] [PubMed]
- Severini, G.; Conforto, S.; Chmid, M.S.; D’alessio, T. Novel Formulation of A Double Threshold Algorithm for the Estimation of Muscle Activation Intervals Designed for Variable Snr Environments. J. Electromyogr. Kinesiol. 2012, 22, 878–885. [Google Scholar] [CrossRef] [PubMed]
- Lenz, R. Generalized extreme value distributions, information geometry and sharpness functions for microscopy images. In Proceedings of the IEEE International Conference on Acoustics, Speech and Signal Processing, Florence, Italy, 4–9 May 2014; pp. 2848–2852.
- Nozari, H.; Karami, M.R. Design redundant Chebyshev dictionary with generalized extreme value distribution for sparse approximation and image denoising. Signal Image Video Process. 2014, 8, 327–338. [Google Scholar] [CrossRef]
- Rajan, J.; Den Dekker, A.J.; Sijbers, J. A new non-local maximum likelihood estimation method for Rician noise reduction in magnetic resonance images using the Kolmogorov-Smirnov test. Signal Process. 2014, 103, 16–23. [Google Scholar] [CrossRef]
- Shamshirband, S.; Iqbal, J.; Petković, D.; Mirhashemi, M.A. Survey of four models of probability density functions of wind speed and directions by adaptive neuro-fuzzy methodology. Adv. Eng. Softw. 2014, 76, 148–153. [Google Scholar] [CrossRef]
- Sang, H. Extreme Value Modeling for Space-Time Data with Meteorological Applications. Ph.D. Thesis, Duke University, Durham, NC, USA, 2008. [Google Scholar]
- Nazmi, N. Parameter Estimation for Generalized Extreme Value Distribution of Extreme Rainfall in Johor. Master’s Thesis, Universiti Teknologi Malaysia, Kuala Lumpur, Malaysia, 2014. [Google Scholar]
- López-rubio, E.; Muñoz pérez, J. Probability density function estimation with the frequency polygon transform. J. Inf. Sci. 2015, 298, 136–158. [Google Scholar] [CrossRef]
- Thongpanja, S.; Phinyomark, A.; Limsakul, C.; Phukpattaranont, P. Probability Density of Electromyography Signal for Different Levels of Contraction of Biceps Brachii. In Proceedings of the 10th International Conference on Electrical Engineering/Electronics, Computer, Telecommunications and Information Technology, Krabi, Thailand, 15–17 May 2013; pp. 1–5.
- Clancy, E.A.; Hogan, N. Probability Density of the Surface Electromyogram and Its Relation to Amplitude Detectors. IEEE Trans. Biomed. Eng. 1999, 46, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Hunter, I.W.; Kearney, R.E.; Jones, L.A. Estimation of the conduction velocity of muscle action potentials using phase and impulse response function techniques. Med. Biol. Eng. Comput. 1987, 25, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Ilodeau, M.B.; Cincera, M.; Arsenault, A.; Gravel, D. Normality and Stationarity of Emg Signals of Elbow Flexor Muscles during Ramp and Step Isometric Contractions. J. Electromyogr. Kinesiol. 1997, 7, 87–96. [Google Scholar] [CrossRef]
- Wang, Y.; Qi, Y.; Zhu, J.; Zhang, J.; Wang, Y.; Pan, G.; Zheng, X.; Wu, Z. A Cauchy-Based State-Space Model for Seizure Detection in EEG Monitoring Systems. IEEE Intell. Syst. 2015, 30, 1541–1672. [Google Scholar] [CrossRef]
- Nazmi, N.; Mazlan, S.A.; Zamzuri, H.; Rahman, M.A.A. Fitting Distribution for Electromyography and Electroencephalography Signals Based on Goodness-of-Fit Tests. Proced. Comput. Sci. 2015, 76, 468–473. [Google Scholar] [CrossRef]
- Markose, S.; Alentorn, A. The Generalized Extreme Value Distribution, Implied Tail Index, and Option Pricing. J. Deriv. 2011, 18, 35–60. [Google Scholar] [CrossRef]
- Luca, C.J.D. Physiological and Mathematical Basis of Myoelectric Signals. IEEE Trans. Biomed. Eng. 1980, 18, 313–325. [Google Scholar]
- Milner-Brown, H.; Stein, R. The Relation Between the Surface Elec- Tromyogram and Muscular Force. J. Physiol. 1975, 3, 549–569. [Google Scholar] [CrossRef]
- Parker, P.; Stuller, J.; Scott, R. Signal Processing for the Multi-State Myoelectric Channel. Proc. IEEE 1977, 65, 662–674. [Google Scholar] [CrossRef]
- Schittkowski, K. EASY-FIT: a software system for data fitting in dynamical systems. Struct. Multidiscip. Optim. 2002, 23, 153–169. [Google Scholar] [CrossRef]
- Jenkinson, A.F. The frequency distribution of the annual maximum (or minimum) values of meteorological elements. Q. J. R. Meteorol. Soc. 1955, 81, 158–171. [Google Scholar] [CrossRef]
- Coles, S. An Introduction to Statistical Modeling of Extreme Values; Springer-Verlag: London, UK, 2001. [Google Scholar]
- Rao, A.R.; Hamed, H.K. Flood Frequency Analysis; CRC Press: Boca Raton, FL, USA, 2000. [Google Scholar]
- Zhu, J.; Lin, X.; Blum, R.S.; Gu, Y. Parameter Estimation from Quantized Observations in Multiplicative Noise Environments. IEEE Trans. Signal Process. 2015, 63, 4037–4050. [Google Scholar] [CrossRef]
- Xu, X.; Lee, L.F. Maximum likelihood estimation of a spatial autoregressive Tobit model. J. Econom. 2015, 188, 264–280. [Google Scholar] [CrossRef]
- Khushaba, R.N.; Al-Jumaily, A. Fuzzy Wavelet Packet Based Feature Extraction Method for Multifunction Myoelectric Control. Int. J. Biomed. Sci. 2007, 3, 1–19. [Google Scholar]
- Xie, H.B.; Guo, T.; Bai, S.; Dokos, S. Hybrid soft computing systems for electromyographic signals analysis: A review. BioMed. Eng. Online 2014, 13, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Khezri, M.; Jahed, M. A Neuro–Fuzzy Inference System for sEMG-Based Identification of Hand Motion Commands. IEEE Trans. Ind. Electron. 2007, 58, 1952–1960. [Google Scholar] [CrossRef]
- Hussein, S.E.; Granat, M. Intention detection using a neuro-fuzzy EMG classifier. IEEE Eng. Med. Biol. 2002, 21, 123–129. [Google Scholar] [CrossRef]
- Vapnik, V. The Nature of Statistical Learning Theory; Springer: New York, NY, USA, 2000. [Google Scholar]
- Ogawa, T.; Sato, T.O.; Yamamoto, S.I.; Nakazawa, K.; Kawashima, N. Rhythmic arm swing enhances patterned locomotor-like muscle activity in passively moved lower extremities. IEEE Trans. Biomed. Eng. 2013, 6, 2205–2213. [Google Scholar] [CrossRef] [PubMed]
- Ibrahimy, M.I.; Ahsan, M.R.; Khalifa, O.O. Design and Optimization of Levenberg-Marquardt based Neural Network Classifier for EMG Signals to Identify Hand Motions. Meas. Sci. Rev. 2013, 13, 142–151. [Google Scholar] [CrossRef]
- Ayachi, F.S.; Boudaoud, S.; Marque, C. Evaluation of muscle force classifiation using shape analysis of the sEMG probability density function: A simulation study. Med. Biol. Eng. Comput. 2014, 52, 673–684. [Google Scholar] [CrossRef] [PubMed]
- Péter, A.; Hegyi, A.; Stenroth, L.; Finni, T.; Cronin, N.J. EMG and force production of the fl exor hallucis longus muscle in isometric plantarfl exion and the push-off phase of walking. J. Biomech. 2015, 48, 3413–3419. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Kouzaki, M.; Moritani, T. Newblock regional neuromuscular regulation within human rectus femoris muscle during gait in young and elderly men. J. Biomech. 2016, 49, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Marin, C.R.; Chang, A.; Cyhan, T.; Dinauer, P. EMG Signal Analysis for Identifying Walking Patterns of Normal Healthy Individuals. Indian J. Biomech. 2009, 12, 118–122. [Google Scholar]
- Stefano, A.D.; Burridge, J.H.; Yule, V.T.; Allen, R. Effect of gait cycle selection on EMG analysis during walking in adults and children with gait pathology. Gait Posture 2004, 20, 92–101. [Google Scholar] [CrossRef]
- Hussain, M.S.; Reaz, M.B.I.; Mohd-Yasin, F.; Ibrahimy, M.I. Electromyography signal analysis using wavelet transform and higher order statistics to determine muscle contraction. J. Knowl. Eng. Expert Syst. 2009, 26, 35–48. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | Abbreviation | References |
|---|---|---|
| Integrated EMG | IEMG | [28] |
| Mean Absolute Value | MAV | [7,28,42,47,50] |
| Modified mean absolute value 1 | MAV1 | [28,51] |
| Modified mean absolute value 2 | MAV2 | [28,51] |
| Root Mean Square | RMS | [7,13,28,47] |
| Variance | VAR | [28,47] |
| Waveform length | WL | [28,42,50] |
| Zero crossing | ZC | [28,42,50] |
| Slope sign change | SSC | [28,42,47] |
| Willison amplitude or Wilson amplitude | WAMP | [28,47] |
| Kurtosis | KURT | [31] |
| Skewness | SKEW | [52] |
| Moving Approximate Entropy | moving ApEn | [35] |
| Fuzzy approximate entropy | fApEn | [48] |
| Simple square integral | SSI | [28] |
| v-Order | V | [28,50] |
| Log detector | LOG | [28] |
| Average amplitude change | AAC | [28] |
| Difference absolute standard deviation value | DASDV | [28] |
| Mean absolute value slope | MAVSLP | [28] |
| Multiple hamming windows | MHW | [28] |
| Multiple trapezoidal windows | MTW | [28] |
| Histogram of EMG | HIST | [50] |
| Auto-regressive coefficients | AR | [50] |
| Cepstral coefficients | [28] | |
| Standard deviation | SD | [7,42,47] |
| Cepstral coefficients | CC | [28] |
| Sample entropy | SampEn | [53] |
| Integral absolute value | IAV | [50] |
| Variance | VAR | [50] |
| Maximum amplitude | MAX | [7] |
| Features | Abbreviation | References |
|---|---|---|
| Mean frequency | MNF | [28,41] |
| Median frequency | MDF | [28,41] |
| Mean power frequency | MNP | [51] |
| Peak frequency | PKF | [28] |
| Total power | TTP | [28] |
| Frequency ratio | FR | [28] |
| Power spectrum ratio | PSR | [28] |
| The power spectrum deformation | Ω | [41] |
| Variance of central frequency | VCF | [28] |
| Signal-to-motion artifact ratio | SMR | [41] |
| Signal-to-noise ratio | SNR | [41] |
| Spectral moment | SM | [28] |
| Energy | EN | [42] |
| Wavelet decomposition | WDC | [42] |
| Wavelet decomposition difference | WDCDIF | [42] |
| Modified mean frequency | MMNF | [56] |
| Modified median frequencies | MMDF | [56] |
| Short Time Fourier transform | STFT | [57] |
| Features | Abbreviation | References |
|---|---|---|
| Discrete Wavelet Transform | DWT | [44] |
| Continous Wavelet Transform | CWT | [9] |
| Empirical Mode Decomposition | EMD | [9] |
| Wavelet Packet Transform | WPT | [44] |
| Maximum Voluntary Contraction | |||||
|---|---|---|---|---|---|
| 20% | 40% | 60% | 80% | 100% | |
| Normal | 0.0036 | 0.0025 | 0.0024 | 0.0022 | 0.0028 |
| Laplace | 0.0081 | 0.0075 | 0.0076 | 0.0077 | 0.0071 |
| Cauchy | 0.0129 | 0.0123 | 0.0123 | 0.0124 | 0.0122 |
| Logistic | 0.0027 | 0.0012 | 0.0009 | 0.0011 | 0.0015 |
| Authors | |
|---|---|
| Gaussian | [43,76,77,78,85] |
| Cauchy | [65] |
| Laplace | [76,77] |
| Logistic | [65] |
| GEV | [81] |
| Training | Stop | Regression | Time | Classification Rate | Hidden | |||
|---|---|---|---|---|---|---|---|---|
| Function | Epochs | Elapsed | Training | Validation | Test | Overall | Neurons | |
| Levenberg marquardt | 15 | 0.8597 | 1.047 | 88.6 | 83.3 | 90 | 88 | 10 |
| 18 | 0.87251 | 0.921 | 94.3 | 66.7 | 80 | 88 | ||
| 16 | 0.87401 | 0.8721 | 88.7 | 90.3 | 90.3 | 89.2 | ||
| Average | 0.86874 | 0.947 | 90.533 | 80.1 | 86.767 | 88.4 | ||
| 33 | 0.85706 | 2.797 | 91.4 | 70 | 83.3 | 87 | 20 | |
| 14 | 0.85508 | 1.218 | 90 | 80 | 86.7 | 88 | ||
| 12 | 0.84772 | 1.094 | 92.9 | 76.7 | 83.3 | 89 | ||
| Average | 0.853287 | 1.703 | 91.433 | 75.567 | 84.433 | 88 | ||
| 16 | 0.86112 | 2.36 | 92.1 | 80 | 76.7 | 88 | 30 | |
| 11 | 0.85018 | 1.703 | 91.4 | 90 | 73.3 | 88.5 | ||
| 14 | 0.85192 | 2.125 | 89.3 | 76.7 | 83.3 | 86.5 | ||
| Average | 0.854107 | 2.0627 | 90.933 | 82.233 | 77.767 | 87.667 | ||
| Scaled Conjugate Gradient | 37 | 0.7819 | 0.703 | 80.7 | 83.3 | 83.3 | 82.43 | 10 |
| 27 | 0.7632 | 0.685 | 78.2 | 86 | 74.5 | 79.57 | ||
| 32 | 0.7904 | 0.823 | 82.4 | 71.9 | 79.4 | 77.9 | ||
| Average | 0.77917 | 0.737 | 80.433 | 80.4 | 79.067 | 79.9 | ||
| 31 | 0.802 | 0.797 | 78.6 | 90 | 82.7 | 83.77 | 20 | |
| 35 | 0.8153 | 1.252 | 79 | 87.3 | 78.1 | 81.47 | ||
| 34 | 0.79842 | 1.063 | 84.3 | 76.7 | 80 | 80.33 | ||
| Average | 0.80524 | 1.037 | 80.633 | 84.667 | 80.267 | 81.86 | ||
| 34 | 0.80767 | 2.457 | 83.6 | 83.3 | 86.7 | 84.53 | 30 | |
| 28 | 0.79215 | 1.073 | 81.2 | 72.1 | 69.5 | 74.27 | ||
| 31 | 0.82531 | 1.352 | 86.6 | 76.5 | 78.8 | 80.63 | ||
| Average | 0.80837 | 1.627 | 80.433 | 80.4 | 79.067 | 79.9 | ||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nazmi, N.; Abdul Rahman, M.A.; Yamamoto, S.-I.; Ahmad, S.A.; Zamzuri, H.; Mazlan, S.A. A Review of Classification Techniques of EMG Signals during Isotonic and Isometric Contractions. Sensors 2016, 16, 1304. https://doi.org/10.3390/s16081304
Nazmi N, Abdul Rahman MA, Yamamoto S-I, Ahmad SA, Zamzuri H, Mazlan SA. A Review of Classification Techniques of EMG Signals during Isotonic and Isometric Contractions. Sensors. 2016; 16(8):1304. https://doi.org/10.3390/s16081304
Chicago/Turabian StyleNazmi, Nurhazimah, Mohd Azizi Abdul Rahman, Shin-Ichiroh Yamamoto, Siti Anom Ahmad, Hairi Zamzuri, and Saiful Amri Mazlan. 2016. "A Review of Classification Techniques of EMG Signals during Isotonic and Isometric Contractions" Sensors 16, no. 8: 1304. https://doi.org/10.3390/s16081304